
Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Analysis
3. Results
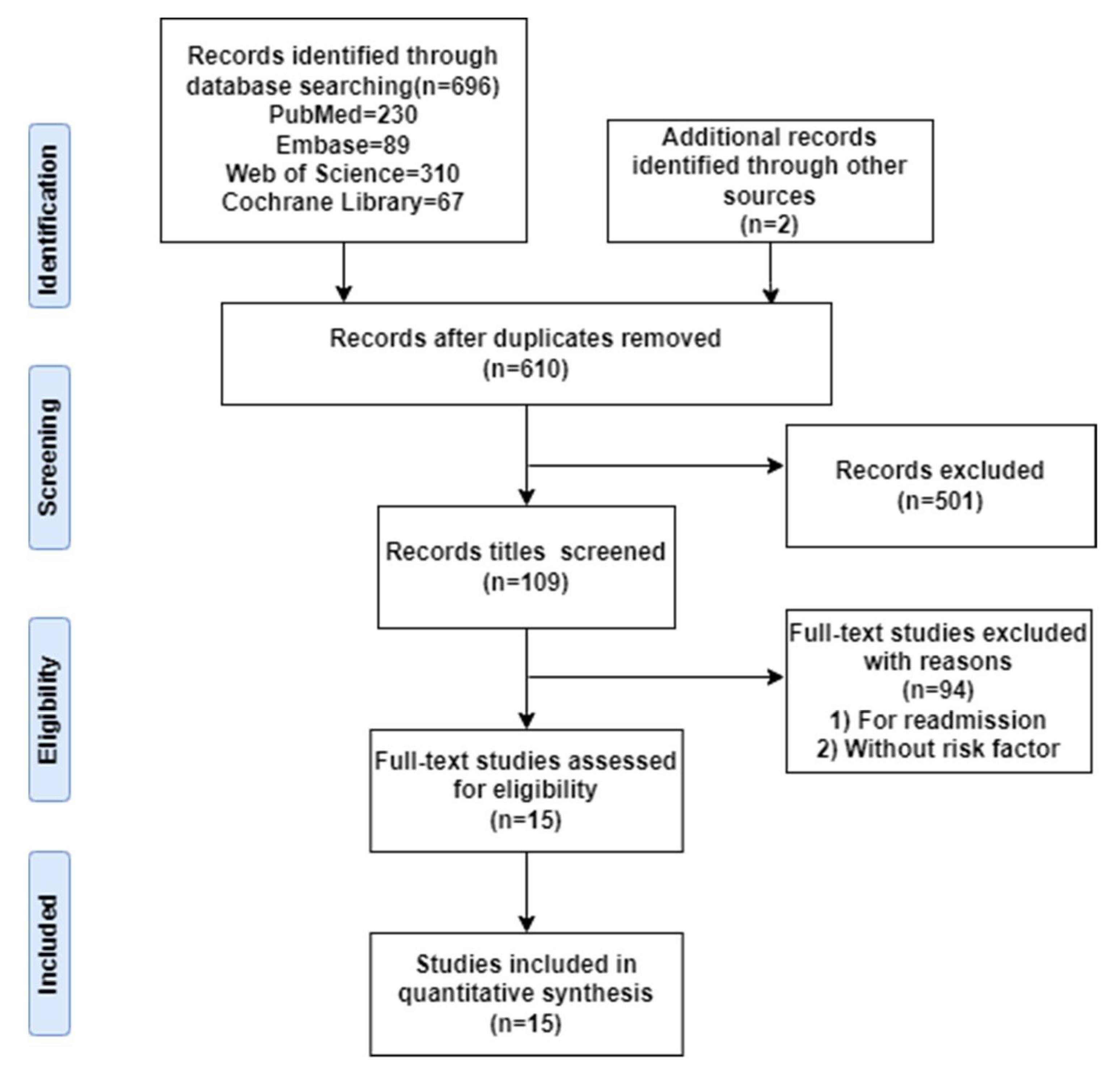
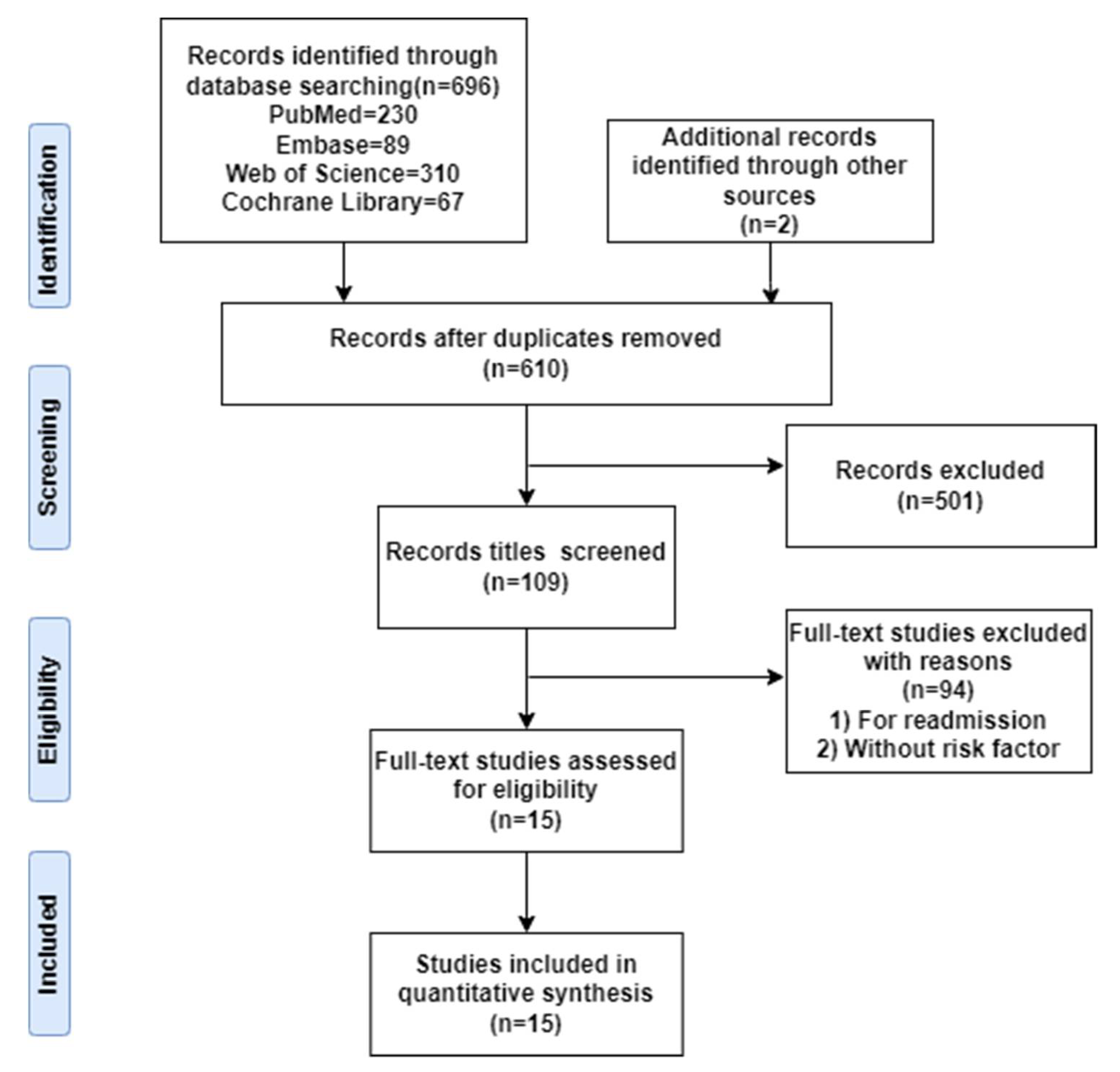
3.1. Search Results
3.2. Quality Assessment
3.3. Results of Meta-Analysis
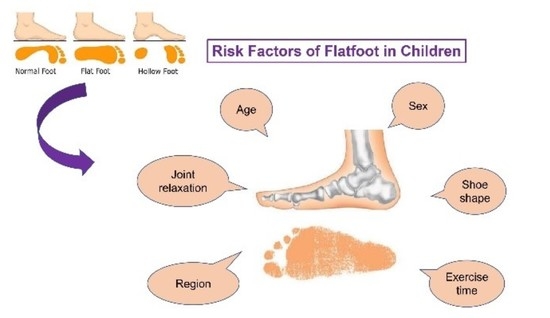
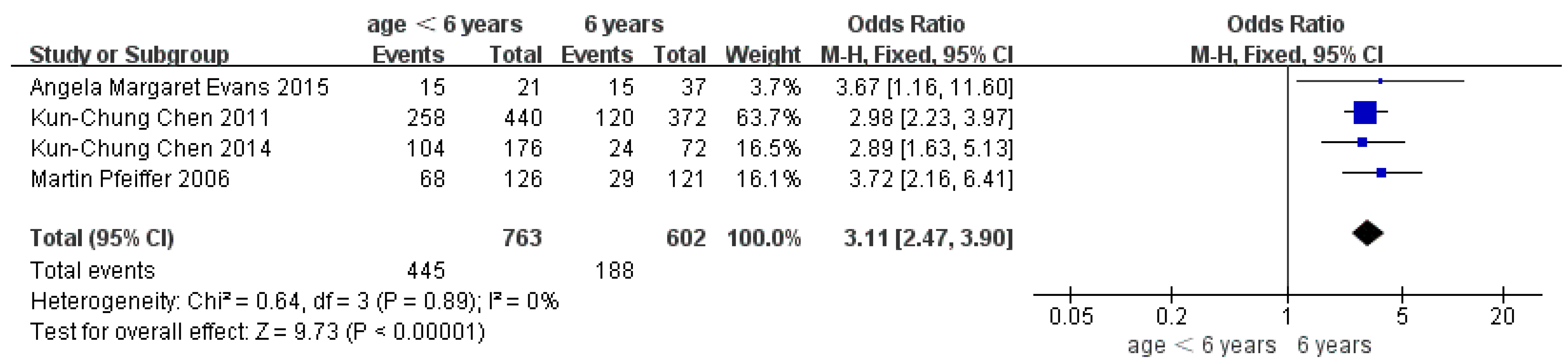
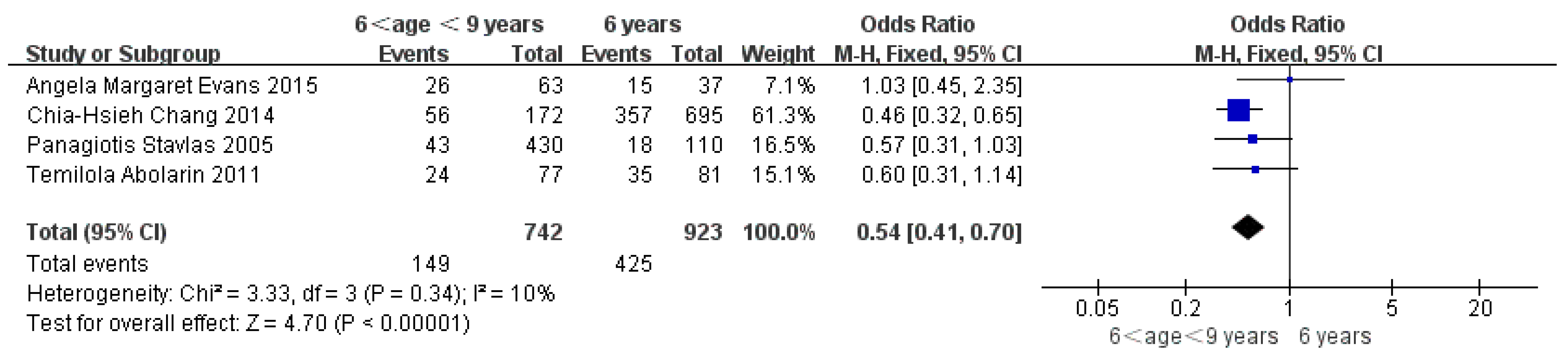
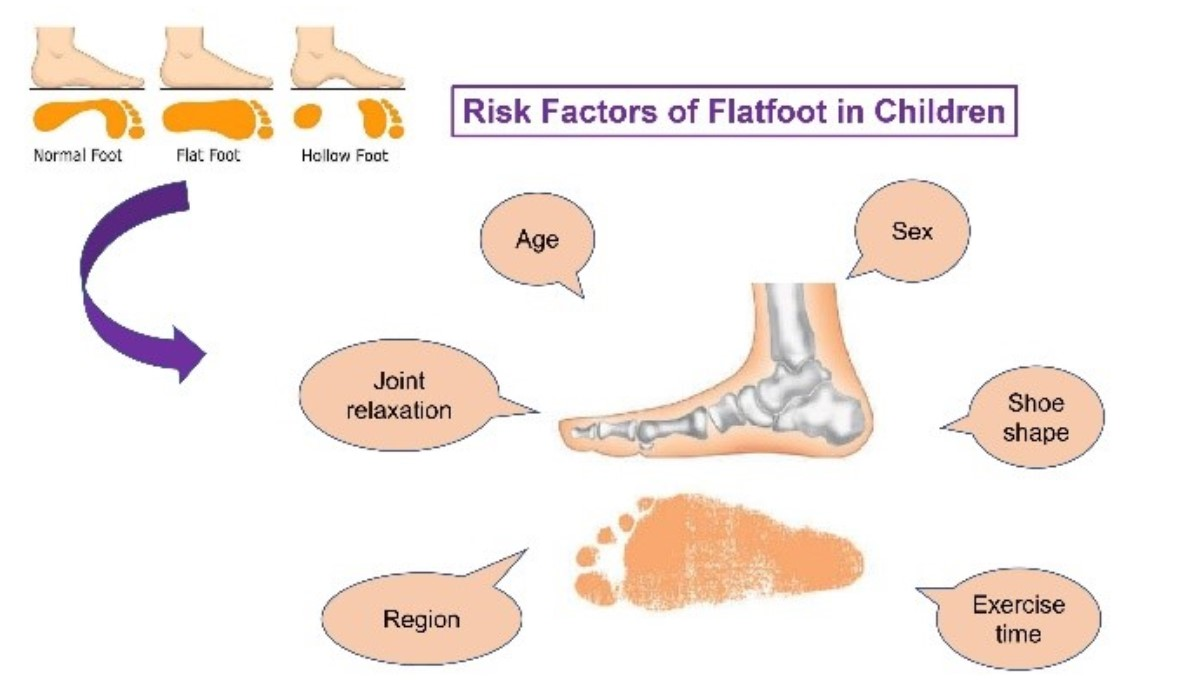
3.4. Risk Factors
3.5. Sensitivity Analysis
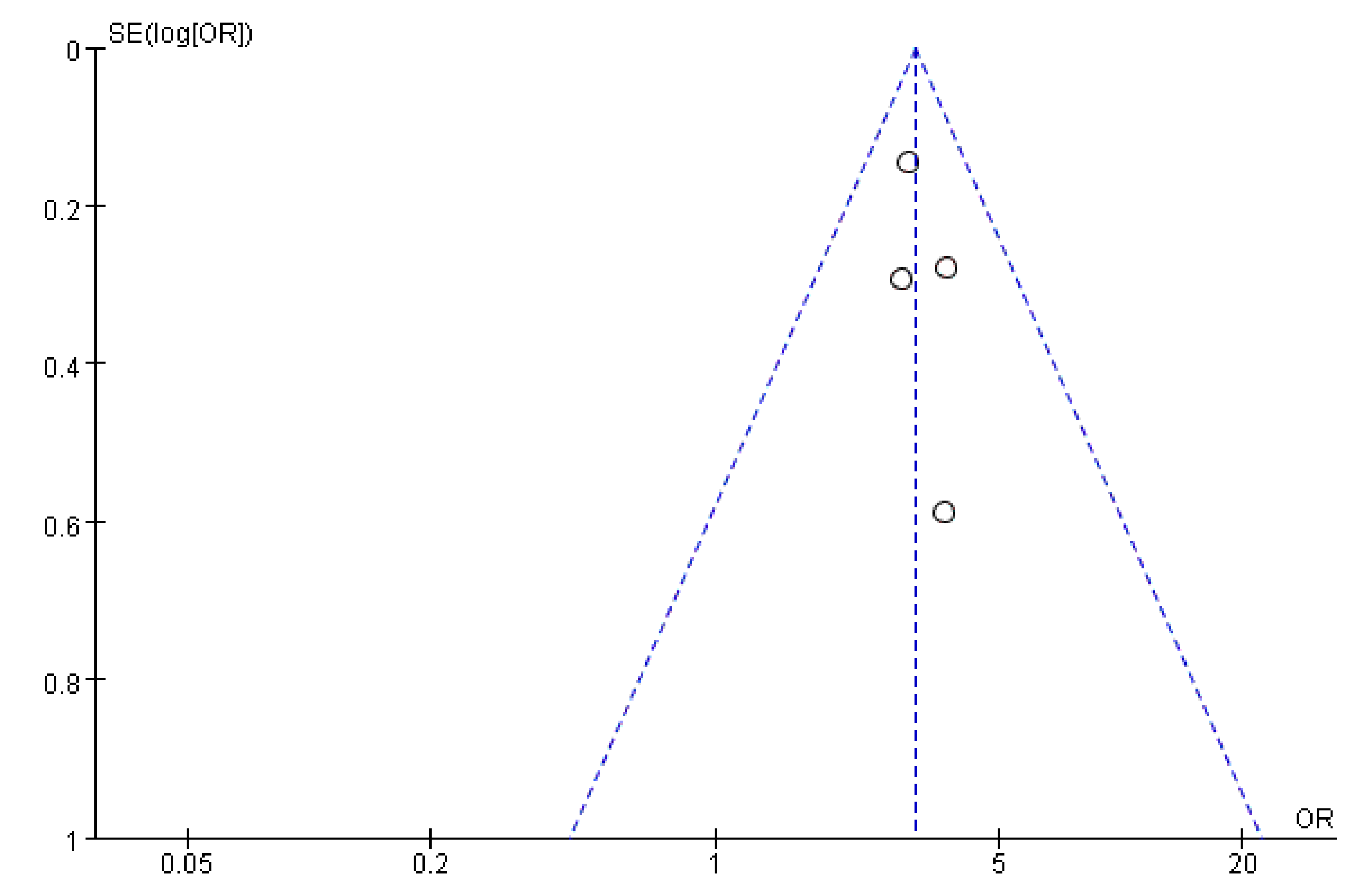
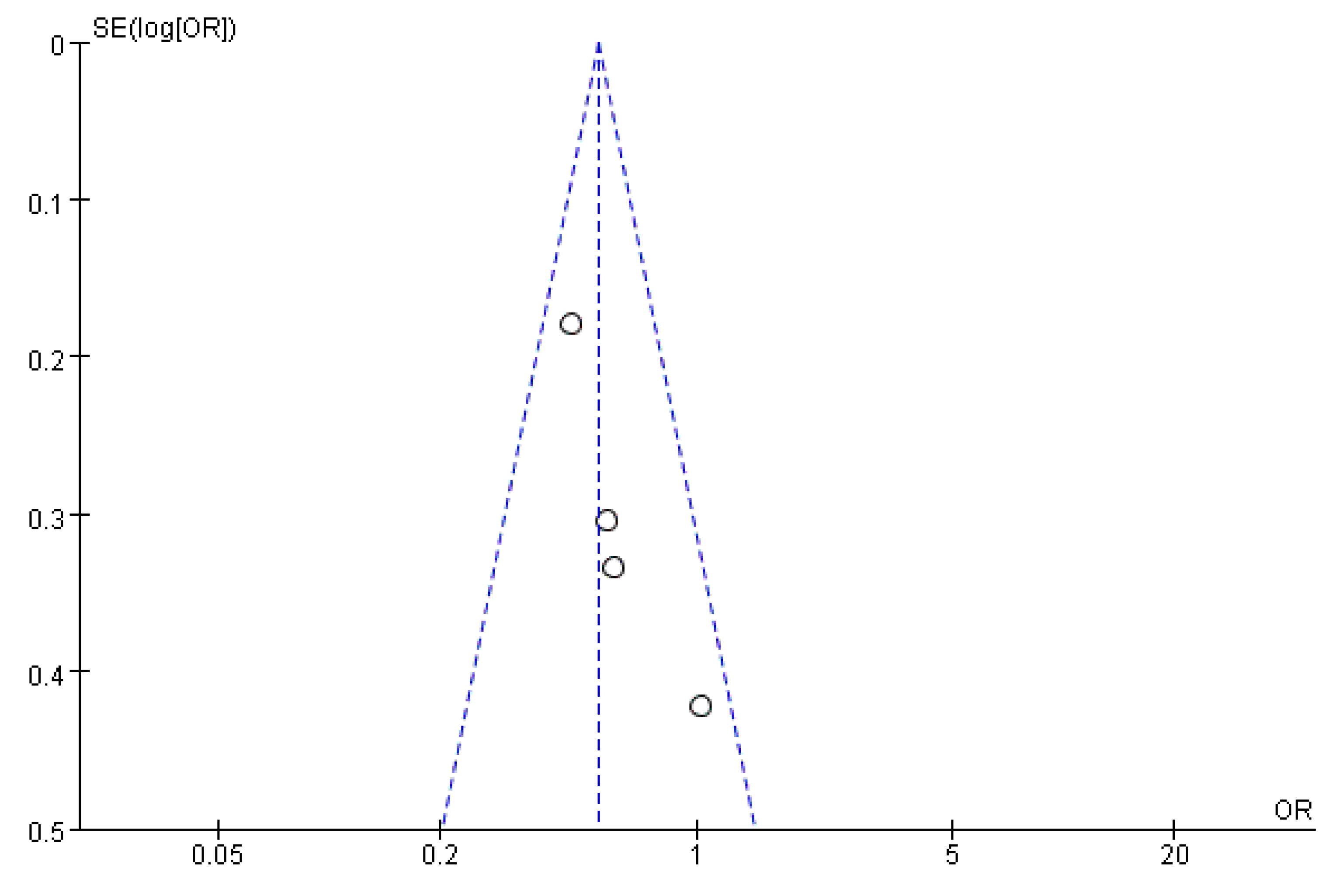
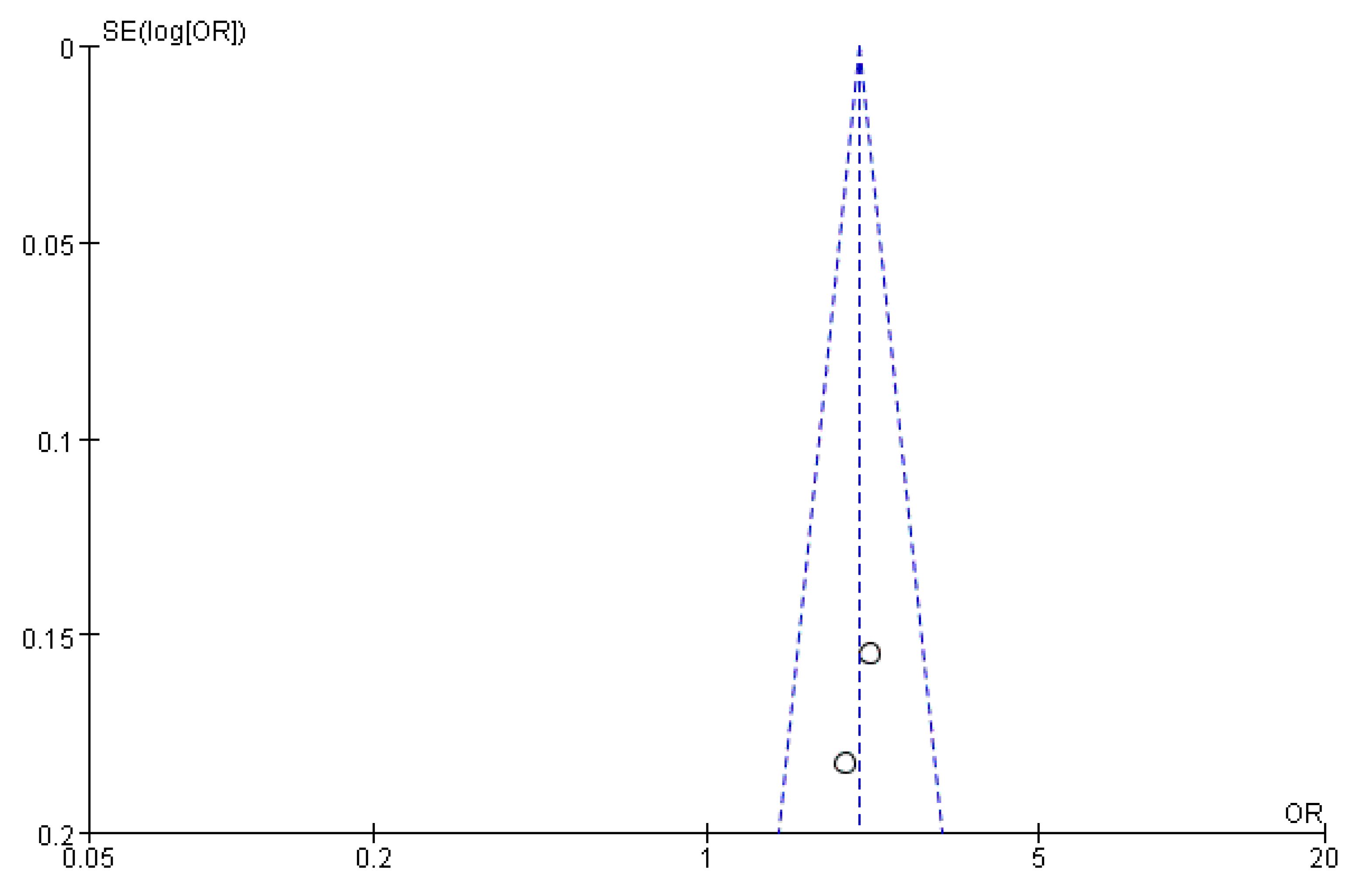
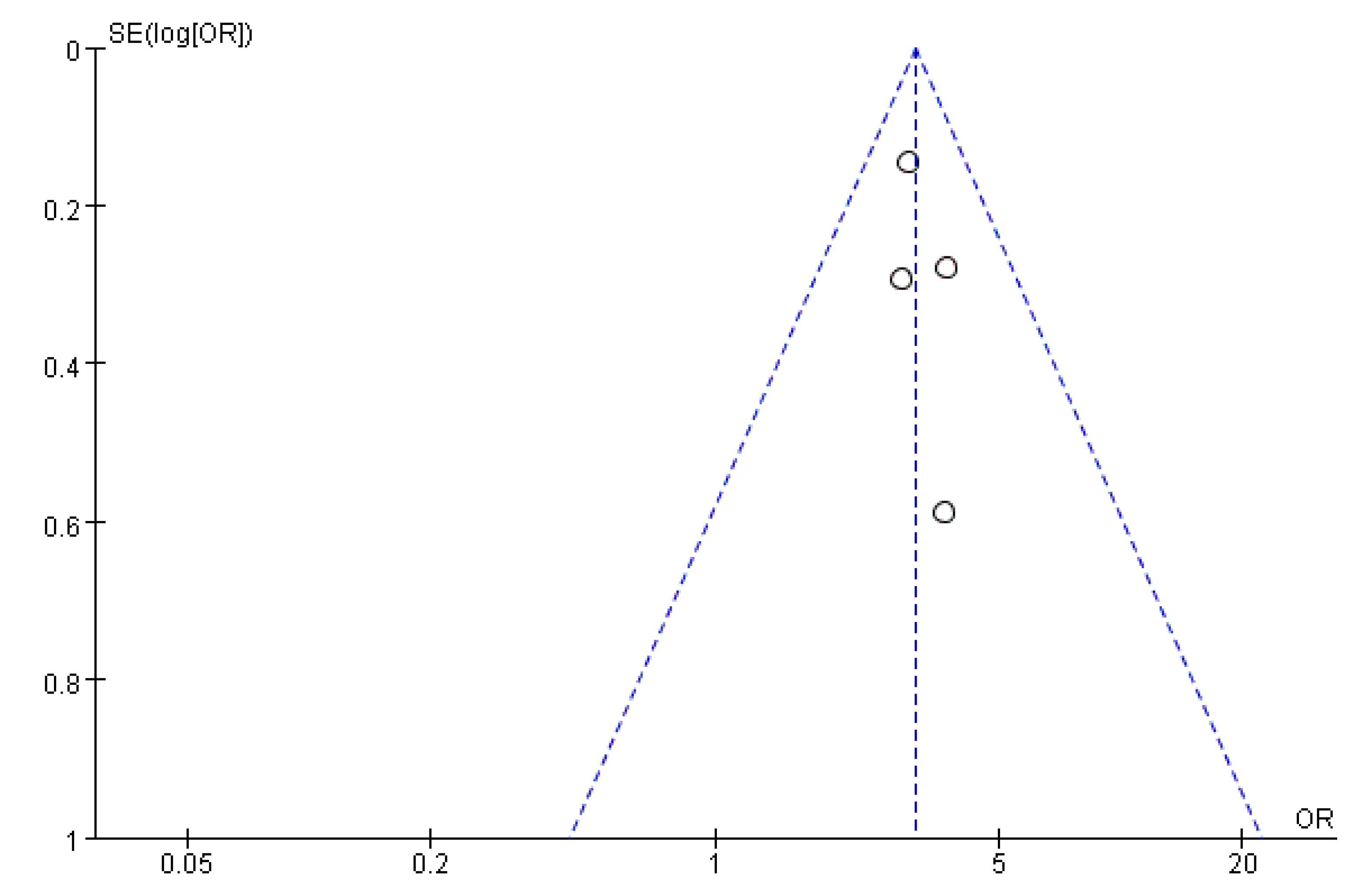
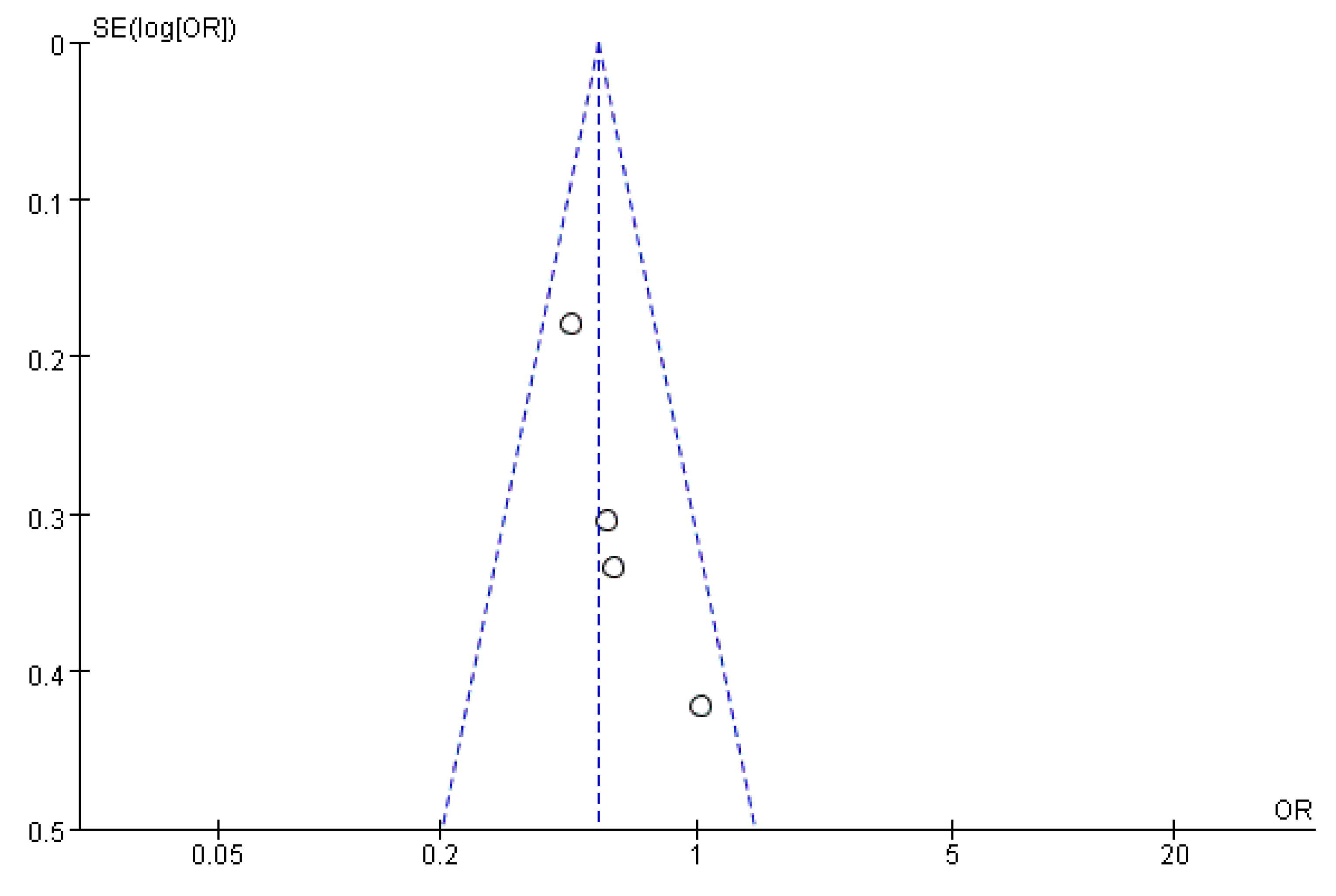
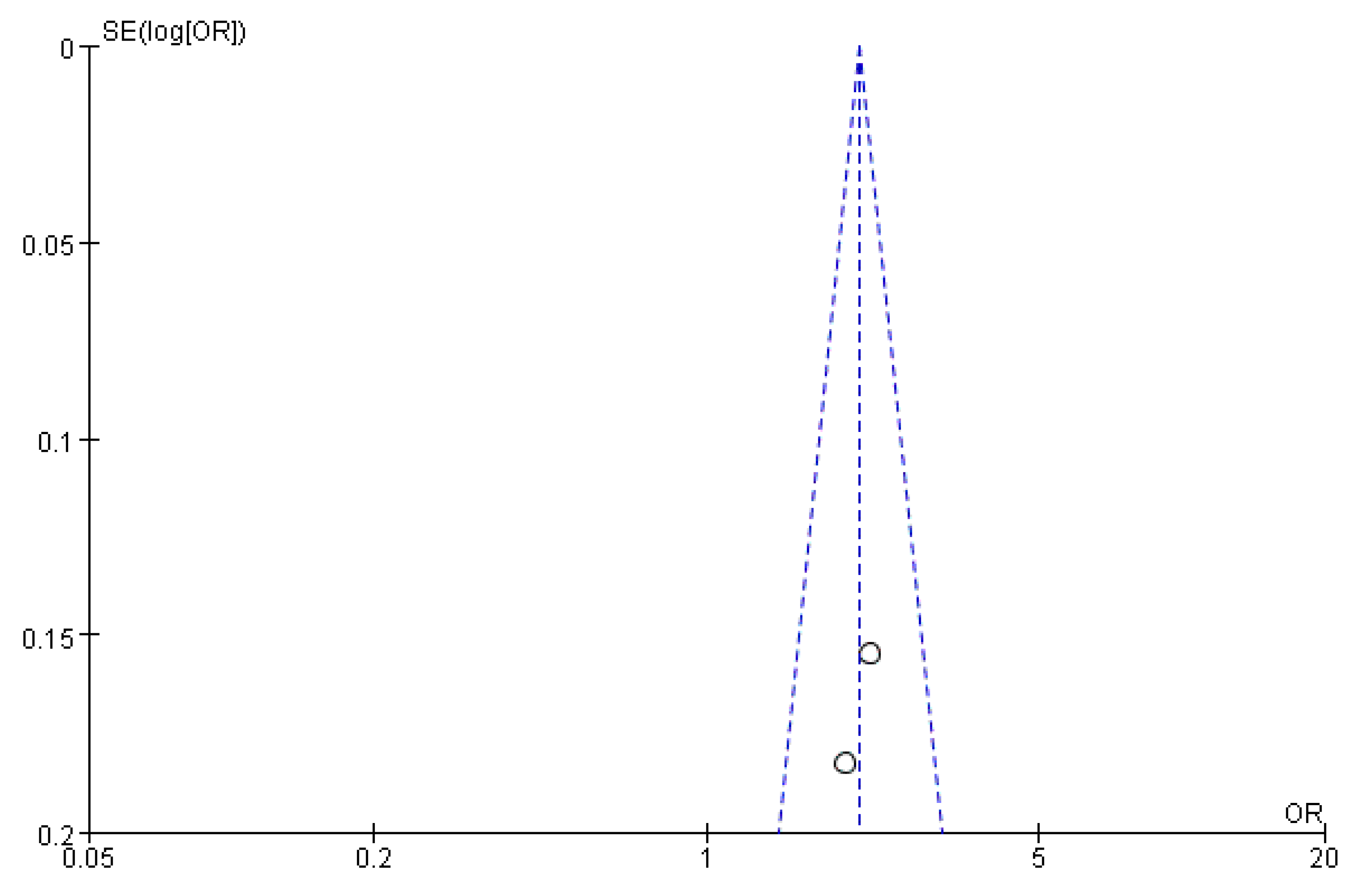
3.6. Publication Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, M.A. Flat feet in children. BMJ 1990, 301, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Villarroya, M.A.; Esquivel, J.M.; Tomás, C.; Moreno, L.A.; Buenafé, A.; Bueno, G. Assessment of the medial longitudinal arch in children and adolescents with obesity: Footprints and radiographic study. Eur. J. Pediatr. 2009, 168, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; Wang, S.H.; Kuo, C.L.; Shen, H.C.; Hong, Y.W.; Lin, L.C. Prevalence of flexible Flatfoot in Taiwanese school-aged children in relation to obesity, gender, and age. Eur. J. Pediatr. 2010, 169, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.M.; Rome, K. A Cochrane review of the evidence for non-surgical interventions for flexible pediatric flat feet. Eur. J. Phys. Rehabil. Med. 2011, 47, 69–89. [Google Scholar]
- Chen, K.C.; Tung, L.C.; Yeh, C.J.; Yang, J.F.; Kuo, J.F.; Wang, C.H. Change in Flatfoot of preschool-aged children: A 1-year follow-up study. Eur. J. Pediatr. 2013, 172, 255–260. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71–78. [Google Scholar] [CrossRef]
- Stavlas, P.; Grivas, T.B.; Michas, C.; Vasiliadis, E.; Polyzois, V. The evolution of foot morphology in children between 6 and 17 years of age: A cross-sectional study based on footprints in a Mediterranean population. J. Foot Ankle Surg. 2005, 44, 424–428. [Google Scholar] [CrossRef]
- Pfeiffer, M.; Kotz, R.; Ledl, T.; Hauser, G.; Sluga, M. Prevalence of flat foot in preschool-aged children. Pediatrics 2006, 118, 634–639. [Google Scholar] [CrossRef]
- Adoracion Villarroya, M.; Manuel Esquivel, J.; Tomás, C.; Buenafé, A.; Moreno, L. Foot structure in overweight and obese children. Int. J. Pediatr. Obes. 2008, 3, 39–45. [Google Scholar] [CrossRef]
- Twomey, D.; McIntosh, A.S.; Simon, J.; Lowe, K.; Wolf, S.I. Kinematic differences between normal and low arched feet in children using the Heidelberg foot measurement method. Gait Posture 2010, 32, 1–5. [Google Scholar] [CrossRef]
- Abolarin, T.; Aiyegbusi, A.; Tella, A.; Akinbo, S. Predictive factors for Flatfoot: The role of age and footwear in children in urban and rural communities in South West Nigeria. Foot 2011, 21, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.C.; Yeh, C.J.; Kuo, J.F.; Hsieh, C.L.; Yang, S.F.; Wang, C.H. Footprint analysis of Flatfoot in preschool-aged children. Eur. J. Pediatr. 2011, 170, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Chen, Y.C.; Yang, W.T.; Ho, P.C.; Hwang, A.W.; Chen, C.H.; Chang, J.H.; Change, L.W. Flatfoot diagnosis by a unique bimodal distribution of footprint index in children. PLoS ONE 2014, 9, e115808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.C.; Tung, L.C.; Tung, C.H.; Yeh, C.J.; Yang, J.F.; Wang, C.H. An investigation of the factors affecting Flatfoot in children with delayed motor development. Res. Dev. Disabil. 2014, 35, 639–645. [Google Scholar] [CrossRef]
- Galli, M.; Cimolin, V.; Rigoldi, C.; Pau, M.; Costici, P.; Albertini, G. The effects of low arched feet on foot rotation during gait in children with Down syndrome. J. Intellect. Disabil. Res. JIDR 2014, 58, 758–764. [Google Scholar] [CrossRef]
- Pauk, J.; Ihnatouski, M.; Najafi, B. Assessing plantar pressure distribution in children with flatfoot arch: Application of the Clarke angle. J. Am. Podiatr. Med. Assoc. 2014, 104, 622–632. [Google Scholar] [CrossRef]
- Evans, A.M.; Karimi, L. The relationship between paediatric foot posture and body mass index: Do heavier children really have flatter feet? J. Foot Ankle Res. 2015, 8, 46–52. [Google Scholar] [CrossRef] [Green Version]
- Tashiro, Y.; Fukumoto, T.; Uritani, D.; Matsumoto, D.; Nishiguchi, S.; Fukutani, N.; Adachi, D.; Hotta, T.; Morino, S.; Shirooka, H.; et al. Children with flat feet have weaker toe grip strength than those having a normal arch. J. Phys. Ther. Sci. 2015, 27, 3533–3536. [Google Scholar] [CrossRef]
- Drefus, L.C.; Kedem, P.; Mangan, S.M.; Scher, D.M.; Hillstrom, H.J. Reliability of the Arch Height Index as a Measure of Foot Structure in Children. Pediatr. Phys. Ther. 2017, 29, 83–88. [Google Scholar] [CrossRef]
- Abich, Y.; Mihiret, T.; Yihunie Akalu, T.; Gashaw, M.; Janakiraman, B. Flatfoot and associated factors among Ethiopian school children aged 11 to 15 years: A school-based study. PLoS ONE 2020, 15, e0238001. [Google Scholar] [CrossRef]
- Boryczka-Trefler, A.; Kalinowska, M.; Szczerbik, E.; Stępowska, J.; Łukaszewska, A.; Syczewska, M. How to Define Pediatric Flatfoot: Comparison of 2 Methods: Foot Posture in Static and Dynamic Conditions in Children 5 to 9 Years Old. Foot Ankle Spec. 2021, 5, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Carr, J.B., 2nd; Yang, S.; Lather, L.A. Pediatric Pes Planus: A State-of-the-Art Review. Pediatrics 2016, 137, 215–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueki, Y.; Sakuma, E.; Wada, I. Pathology and management of flexible flat foot in children. J. Orthop. Sci. 2019, 24, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Galafate, D.; Pournajaf, S.; Condoluci, C.; Goffredo, M.; Di Girolamo, G.; Manzia, C.M.; Pellicciari, L.; Franceschini, M.; Galli, M. Bilateral Foot Orthoses Elicit Changes in Gait Kinematics of Adolescents with Down Syndrome with Flatfoot. Int. J. Environ. Res. Public Health 2020, 17, 4994. [Google Scholar] [CrossRef]
- Peng, Y.; Wong DW, C.; Wang, Y.; Chen TL, W.; Tan, Q.; Chen, Z.; Jin, Z.; Zhang, M. Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 2226. [Google Scholar] [CrossRef] [Green Version]
- Yan, S.H.; Zhang, K.; Tan, G.Q.; Yang, J.; Liu, Z.C. Effects of obesity on dynamic plantar pressure distribution in Chinese prepubescent children during walking. Gait Posture 2013, 37, 37–42. [Google Scholar] [CrossRef]
- Hong, J.; Dai, G.; Weng, Q.; Liu, Y. Interference Screw for the Treatment of Pediatric Flexible Flatfoot. J. Foot Ankle Surg. 2020, 59, 1209–1214. [Google Scholar] [CrossRef]
- Tong, J.W.; Kong, P.W. Medial Longitudinal Arch Development of Children Aged 7 to 9 Years: Longitudinal Investigation. Phys. Ther. 2016, 96, 1216–1224. [Google Scholar] [CrossRef] [Green Version]
- Szczepanowska-Wołowiec, B.; Sztandera, P.; Kotela, I.; Zak, M. Assessment of the Foot′s Longitudinal Arch by Different Indicators and Their Correlation with the Foot Loading Paradigm in School-Aged Children: A Cross Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5196. [Google Scholar] [CrossRef]
- Dowling, A.M.; Steele, J.R.; Baur, L.A. What are the effects of obesity in children on plantar pressure distributions? Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2004, 28, 1514–1519. [Google Scholar] [CrossRef] [Green Version]
- Taylor, E.D.; Theim, K.R.; Mirch, M.C.; Ghorbani, S.; Tanofsky-Kraff, M.; Adler-Wailes, D.C.; Brady, S.; Reynolds, J.C.; Calis, K.A.; Yanovski, J.A. Orthopedic complications of overweight in children and adolescents. Pediatrics 2006, 117, 2167–2174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenger, D.R.; Mauldin, D.; Speck, G.; Morgan, D.; Lieber, R.L. Corrective shoes and inserts as treatment for flexible Flatfoot in infants and children. J. Bone Jt. Surg. Am. Vol. 1989, 71, 800–810. [Google Scholar] [CrossRef] [Green Version]
- Tahririan, M.A.; Ramtin, S.; Taheri, P. Functional and radiographic comparison of subtalar arthroereisis and lateral calcaneal lengthening in the surgical treatment of flexible Flatfoot in children. Int. Orthop. 2021, 45, 2291–2298. [Google Scholar] [CrossRef] [PubMed]
- Aharonson, Z.; Arcan, M.; Steinback, T.V. Foot-ground pressure pattern of flexible Flatfoot in children, with and without correction of calcaneovalgus. Clin. Orthop. Relat. Res. 1992, 278, 177–182. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Age (Year) | Sample Size | Detection Rate (%) | Research Factors | Measuring Method | AHRQ Score |
|---|---|---|---|---|---|---|---|
| Panagiotis 2005 [7] | Greece | 6–17 | 5866 | 4.4 | Sex, age, joint relaxation | the CSI, the AI | H |
| Martin 2006 [8] | Greece | 3–6 | 835 | 44 | Sex, age, BMI | the RA | H |
| Villarroya 2008 [9] | Spain | 9–17 | 245 | 30.6 | Sex, BMI, exercise level | the FPI | MD |
| Twomey 2010 [10] | Australia | 9–12 | 52 | 51.9 | Sex | the HFMM | MD |
| Temilola 2011 [11] | Nigeria | 6–12 | 560 | 24.7 | Sex, age, shoe type, region | the FPI | H |
| Chen 2011 [12] | China | 3–6 | 2638 | 44 | Age | the CA, the CSI, the AI | H |
| Chang 2014 [13] | China | 6–10 | 1228 | 45.3 | Sex, age, BMI | the FPI | H |
| Chen 2014 [14] | China | 3–6 | 484 | 48.5 | Sex, age, BMI, joint relaxation, and movement time | the CSI | H |
| Galli 2014 [15] | Italy | 9.6 | 140 | 88 | Joint relaxation | the AI | MD |
| Jolanta 2014 [16] | Poland | 9–16 | 75 | 56 | Sex, exercise time, school type | the CA | MD |
| Angela 2015 [17] | Australia | 3–15 | 728 | 40 | Age, BMI, region | the FPI | MD |
| Yuto 2015 [18] | Japan | 10–12 | 619 | 17.8 | Sex, age | the FPI, the TGS | H |
| Lisa 2017 [19] | America | 6–12 | 60 | 55 | Sex | the AHI | MD |
| Yohannes 2020 [20] | Ethiopia | 11–15 | 823 | 17.6 | Sex, age, school type, BMI, shoe type, exercise time | the FPI, the LLAS | H |
| Anna 2021 [21] | Mexico | 5–9 | 50 | 57.7 | Age, BMI | the CA | MD |
| Risk Factor | Studies | Statistically Methods | OR with 95% CI | I2 (%) | p-Value | |
|---|---|---|---|---|---|---|
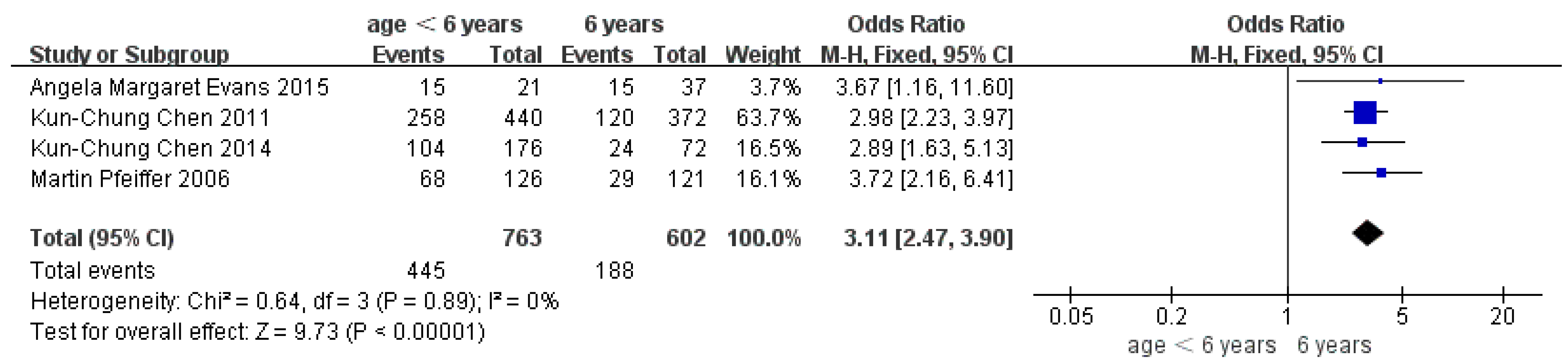
| Age | Age < 6 years | 4 | Fixed | 3.11 [2.47, 3.90] | 0 | p < 0.001 |
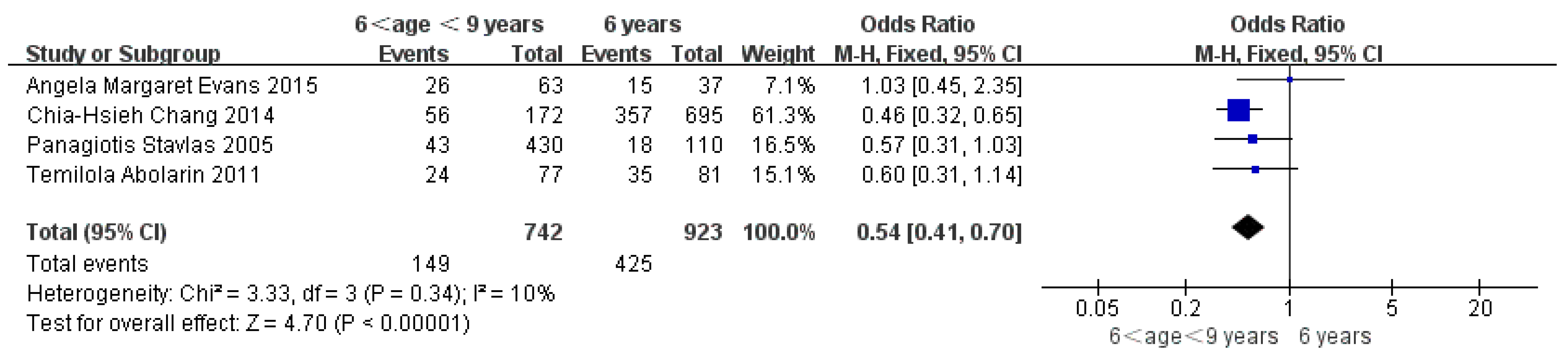
| age 6–9 years | 4 | Fixed | 0.54 [0.41, 0.70] | 10 | p < 0.001 | |
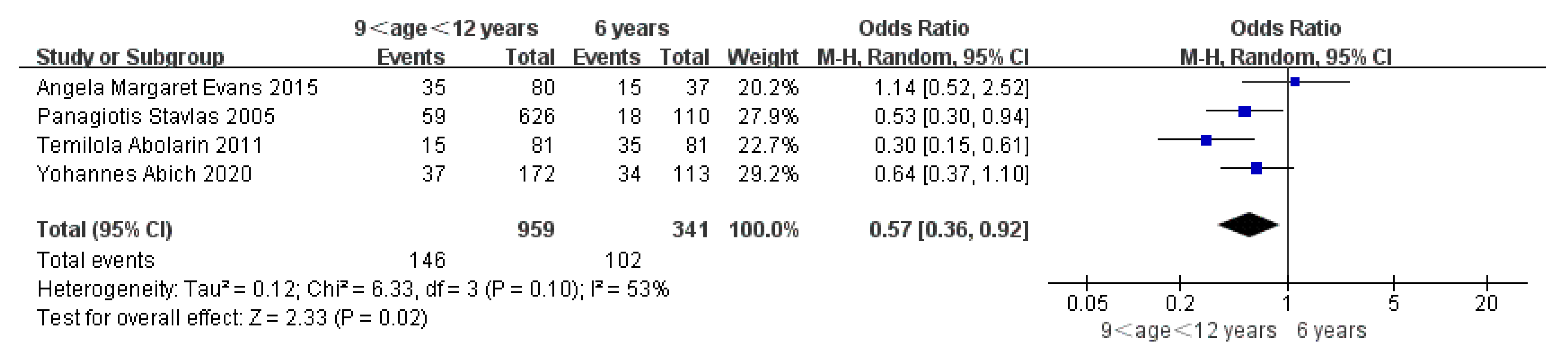
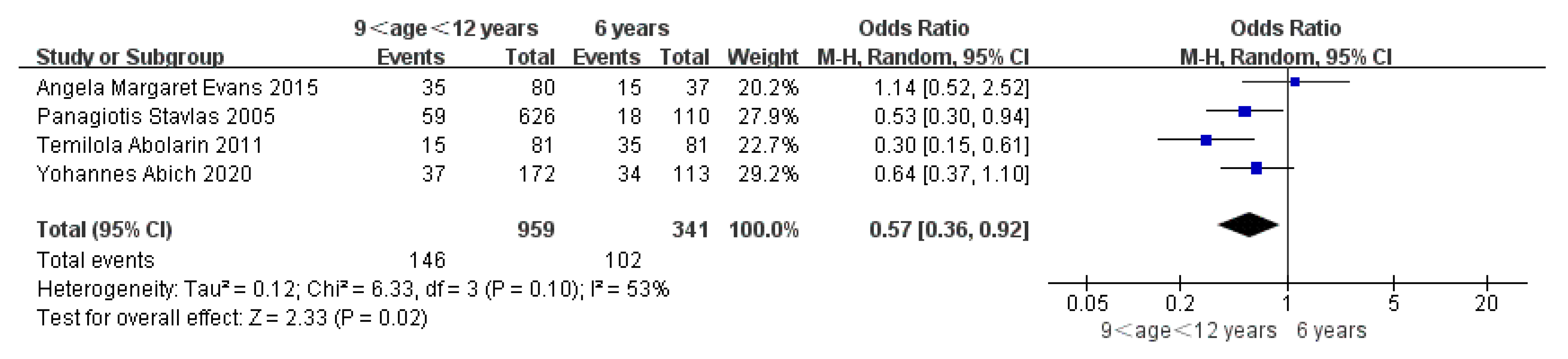
| age 9–12 years | 4 | Random | 0.57 [0.36, 0.92] | 53 | p = 0.02 | |
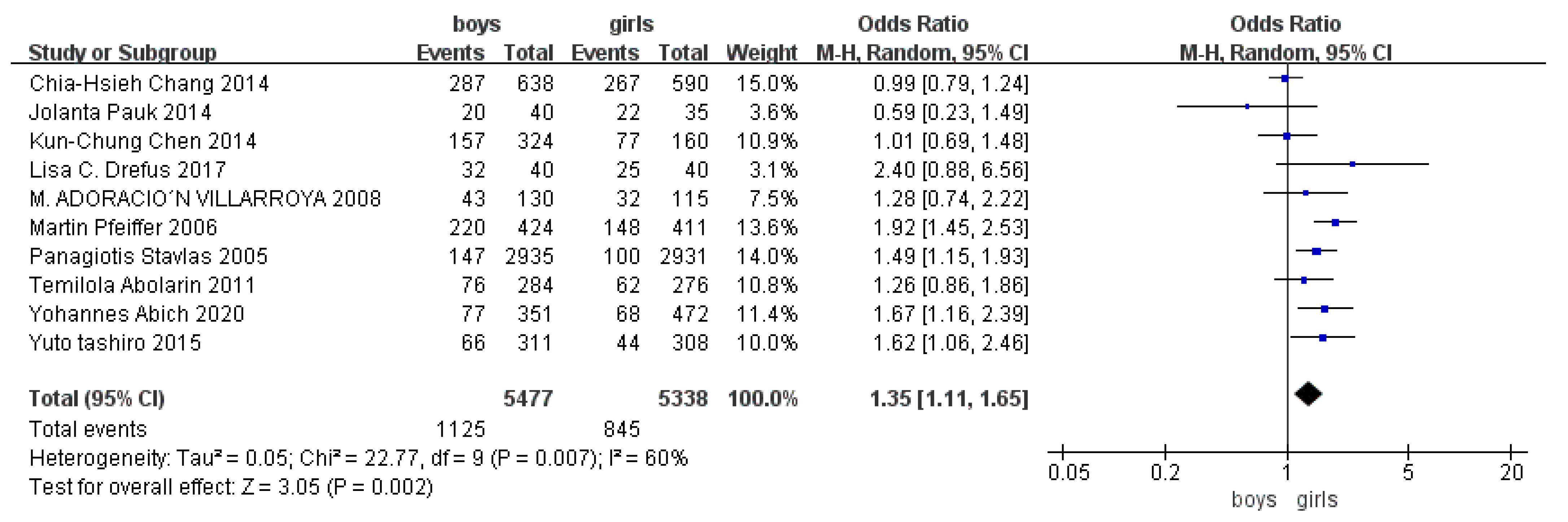
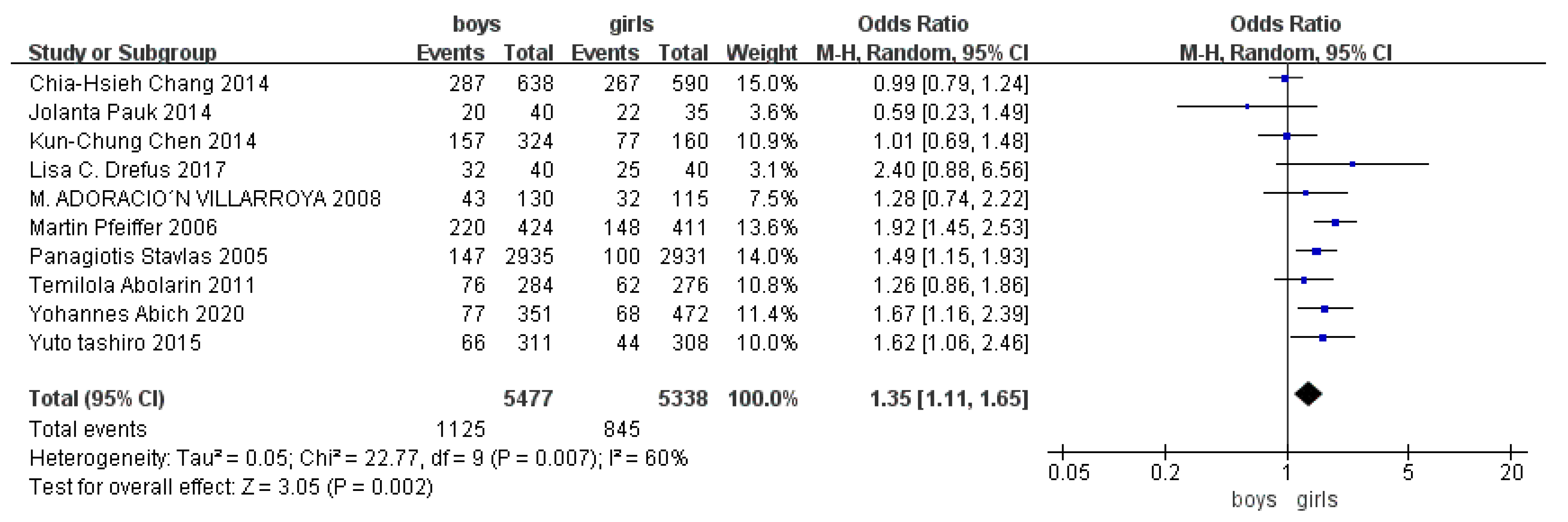
| Sex | Boy | 9 | Random | 1.35 [1.11, 1.65] | 60 | p = 0.002 |
| Girl | ||||||
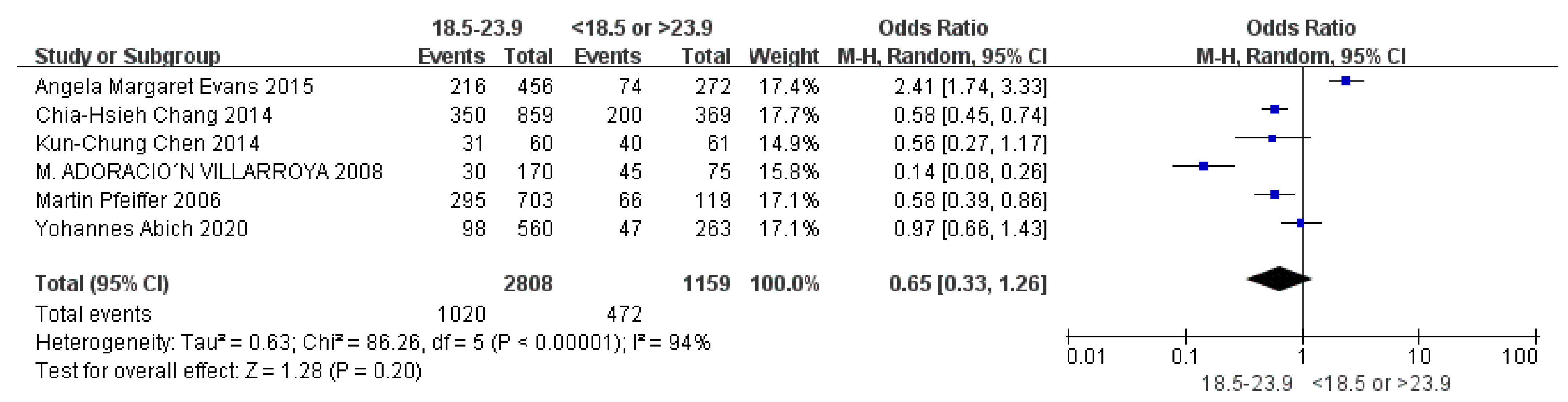
| BMI | 18.5–23.9 | 6 | Random | 0.65 [0.33, 1.26] | 94 | p = 0.20 |
| <18.5 or >23.9 | ||||||
| Joint relaxation | Positive | 2 | Random | 4.82 [1.19, 19.41] | 89 | p = 0.03 |
| Negative | ||||||
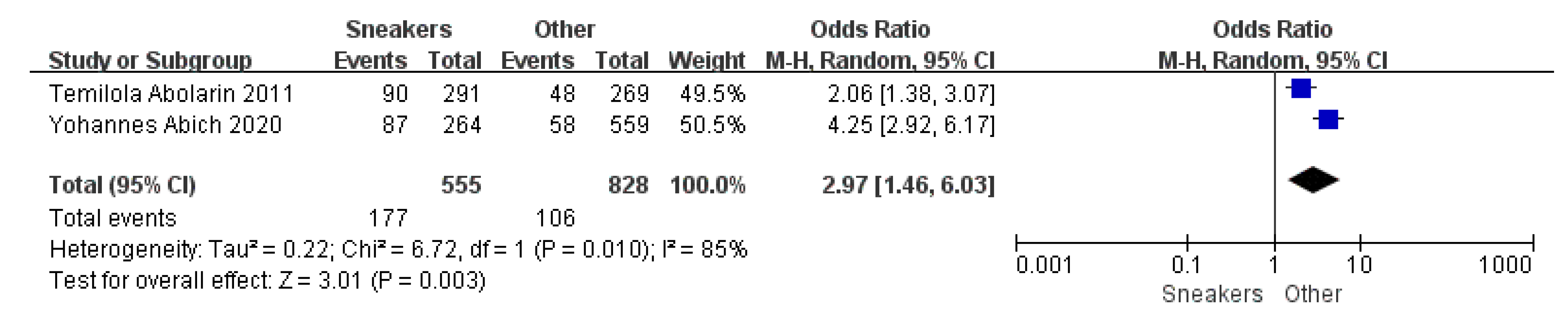
| Shoe shape | Sneakers | 2 | Random | 2.97 [1.46, 6.03] | 85 | p = 0.003 |
| Other | ||||||
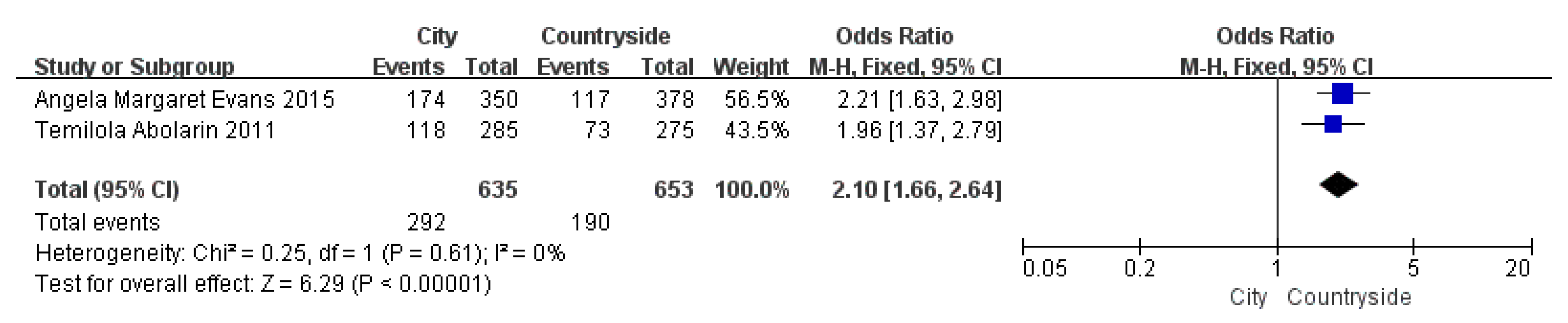
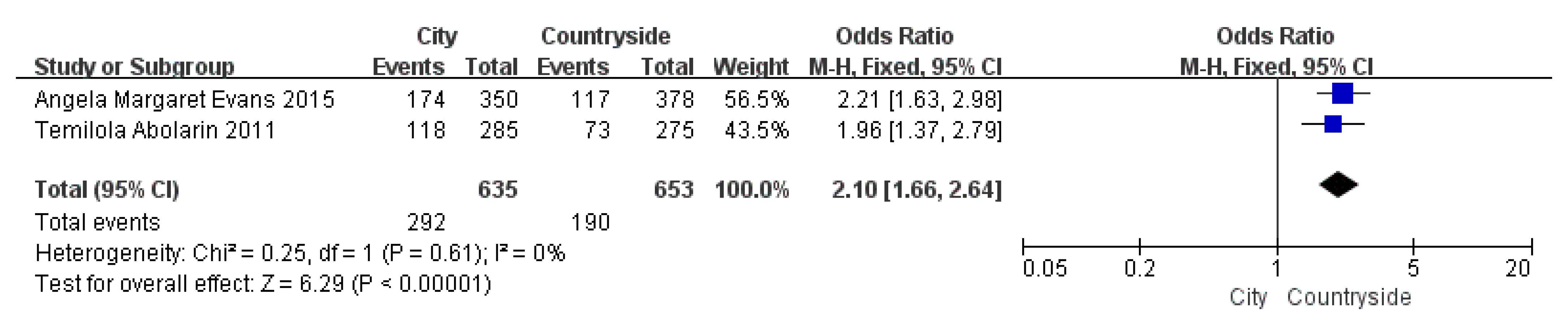
| Region | City | 2 | Fixed | 2.10 [1.66, 2.64] | 0 | p < 0.001 |
| Countryside | ||||||
| School type | Public | 2 | Random | 0.27 [0.06, 1.37] | 87 | p = 0.11 |
| Private | ||||||
| Exercise time | Long exercise time (>180 min/week) | 3 | Random | 0.25 [0.08, 0.80] | 81 | p = 0.02 |
| Short exercise time (<180 min/week) | ||||||
| Related Factors | Fixed-Effects Model | Random-Effects Model | ||
|---|---|---|---|---|
| I2 | OR (95% CI) | I2 | OR (95% CI) | |
| Age < 6 years | 0 | 3.11 [2.47, 3.90] | 0 | 3.11 [2.47, 3.90] |
| age 6–9 years | 10 | 0.54 [0.41, 0.70] | 10 | 0.55 [0.41, 0.73] |
| age 9–12 years | 53 | 0.57 [0.42, 0.78] | 53 | 0.57 [0.36, 0.92] |
| Sex | 63 | 1.34 [1.20, 1.50] | 63 | 1.35 [1.11, 1.65] |
| BMI | 94 | 0.80 [0.69, 0.92] | 94 | 0.65 [0.33, 1.26] |
| Joint relaxation | 89 | 7.84 [6.05, 10.16] | 89 | 4.82 [1.19, 19.41] |
| Shoe shape | 85 | 2.98 [2.27, 3.91] | 85 | 2.97 [1.46, 6.03] |
| Region | 0 | 2.10 [1.66, 2.64] | 0 | 2.10 [1.67, 2.64] |
| Exercise time | 81 | 0.34 [0.21, 0.55] | 81 | 0.25 [0.08, 0.80] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, L.; Gu, H.; Zhang, Y.; Sun, T.; Yu, J. Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8247. https://doi.org/10.3390/ijerph19148247
Xu L, Gu H, Zhang Y, Sun T, Yu J. Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(14):8247. https://doi.org/10.3390/ijerph19148247
Chicago/Turabian StyleXu, Liya, Hongyi Gu, Yimin Zhang, Tingting Sun, and Jingjing Yu. 2022. "Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 14: 8247. https://doi.org/10.3390/ijerph19148247
APA StyleXu, L., Gu, H., Zhang, Y., Sun, T., & Yu, J. (2022). Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(14), 8247. https://doi.org/10.3390/ijerph19148247