Abstract
Little is known about the association of sleep duration with hyperuricemia. Especially lacking is evidence from longitudinal studies. Based on the MJ Health Examination Database in Beijing, China, a prospective study was designed. Participants were classed into short, normal, and long groups by sleep duration. The Cox regression model was used to estimate the hazard risk of hyperuricemia for short or long sleep duration compared with the normal group after adjusting for potential confounders. During a median 3.08 years follow-up, 4868 (14.31%) incident hyperuricemia events were documented among 34,025 participants with a crude incidence rate of 39.49 per 1000 persons. Years after adjusting for potential confounders, a 7% higher risk of hyperuricemia in the short sleep duration group (<7 h, 95% confidence interval: 1.01–1.14) and a 15% lower risk in the long sleep duration group (≥8 h, 95%CI: 0.74–0.97) were found compared with the normal group (7–8 h) (p for trend < 0.001). Nevertheless, the association of the short sleep duration group was marginally significant after further adjustment of the count of white blood cells (hazard ratio: 1.07, 95%CI: 1.00–1.13). Sleep duration was inversely associated with hyperuricemia, which highlights the public health significance of sufficient sleep duration for preventing hyperuricemia.
1. Introduction
Hyperuricemia is considered to be the primary step in the occurrence and development of gout and uric acid calculi, and is strongly correlated with various chronic metabolic diseases, such as gout, hypertension, type 2 diabetes, lipid metabolism disorders, chronic kidney disease, heart failure, and stroke [1,2,3,4,5,6,7,8]. As an inflammatory metabolite, uric acid (UA) is involved in the inflammatory response and activation of the innate immune, and induces the development of diseases [6,9,10]. However, the prevalence of hyperuricemia varies across countries, from 20% in the United States [11] to 6.4% in China [12]. At the same time, the incidence and prevalence of gout and hyperuricemia are constantly increasing around the world, causing a heavier burden and health loss [13]. Therefore, the discovery and control of risk factors for hyperuricemia has become a critical public health issue.
Sleep duration reflects sleep situations and plays an important role in health. Sleep that is both too short and too long sleep has been demonstrated to be related to various diseases and mortality [14,15,16,17]. However, with the current socio-economic development, about one-third of people sleep less than 7 h, one-tenth less than 5 h, and 8% sleep more than 9 h [18].
Existing evidence has shown sleep duration was related to inflammatory molecules [19,20,21] and metabolic diseases. However, there is still a lack of research on the relationship between sleep duration and uric acid levels. A recent cross-sectional study showed a U-shaped relationship between sleep duration and uric acid levels in Korean women [22]. The risk for higher serum UA increased 54% in the short sleep duration group and 94% in long group, compared with that in participants who slept for 7–8 h. Moreover, evidence from an elderly Mediterranean population showed an inverse association between sleep duration and serum UA concentrations [23]. Nevertheless, no longitudinal studies with a large sample size have been reported so far in this field to confirm the association. Our study is a prospective longitudinal study with a large sample to assess the association between sleep duration and hyperuricemia in Chinese adults. It would fill the gap in this field and contribute to public health research on the prevention of hyperuricemia.
2. Materials and Methods
2.1. Study Population
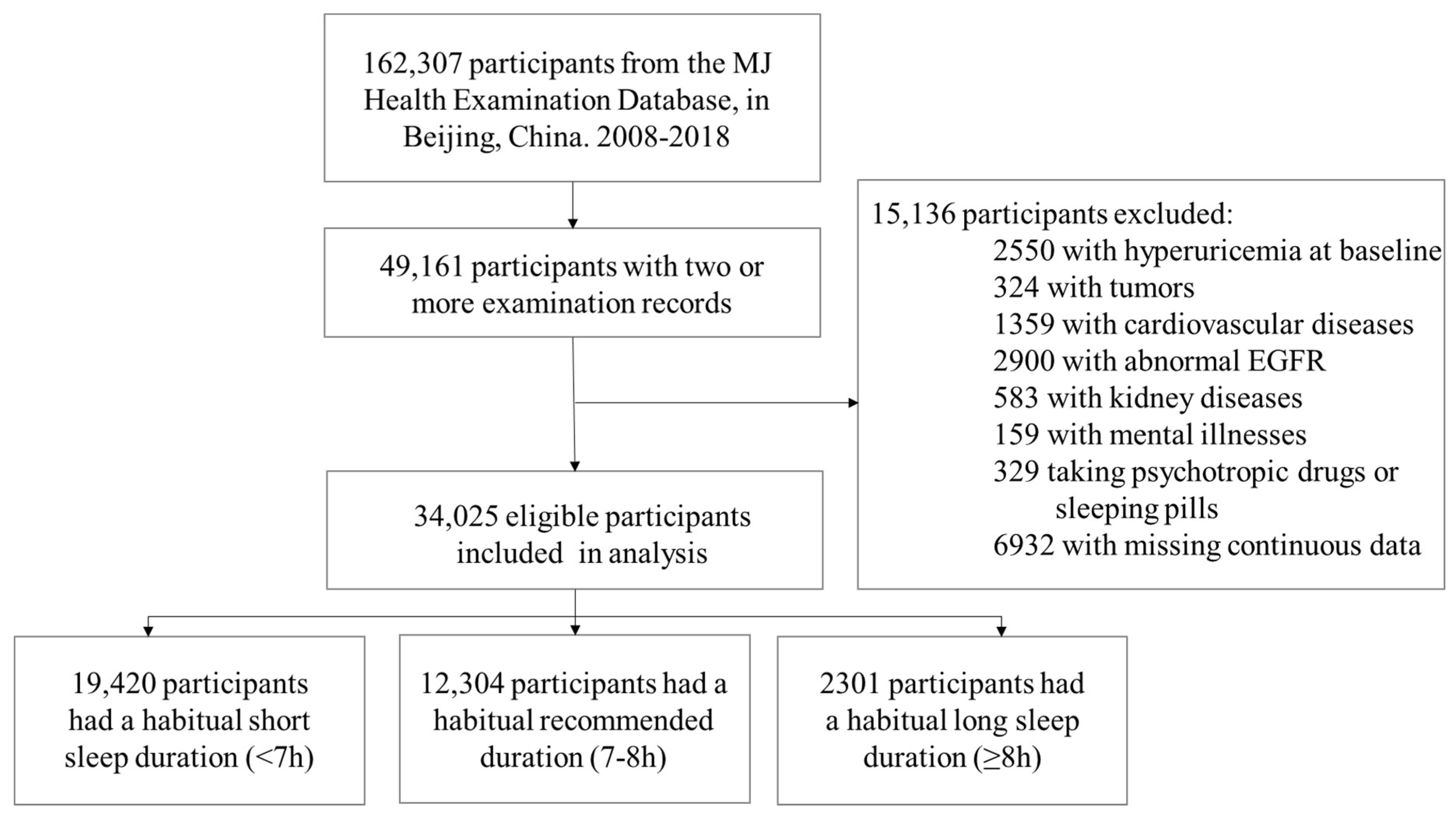
This longitudinal study aimed to explore the association of sleep duration with hyperuricemia among Chinese adults. This study was based on the MJ Health Examination Database in Beijing, China. The details of the database can be found online [24]. We included participants over 18 without prevalent hyperuricemia at baseline that had two or more examinations from 1 January 2008 to 31 December 2018. We excluded subjects with tumors, cardiovascular diseases, kidney diseases, mental illness, or those taking psychotropic drugs or sleeping pills. In addition, we also excluded participants with missing key covariables, including sleep duration, Serum UA, age, sex, and Body Mass Index (BMI). Finally, 34,025 participants remained in the study (Figure 1).
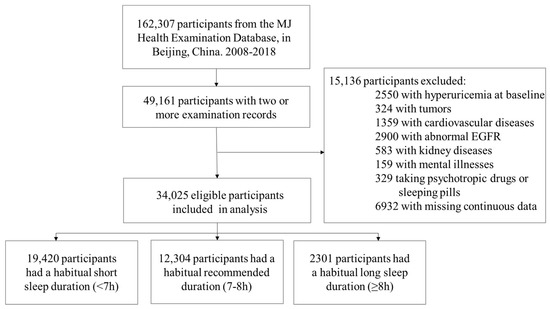
Figure 1.
Flow chart for inclusion and exclusion criteria. EGFR indicates estimated glomerular filtration rate.
All participants completed a standardized self-administered questionnaire at each visit to collect their demographic information, lifestyle habits, medication status, and disease history. The physical and laboratory examinations were performed at the MJ Medical Examination Center with medical diagnostic qualifications. The project was approved by the Peking University biological and medical ethics committee (IRB0001052-19077), with written informed consent obtained from each participant.
2.2. Assessment of Sleep Duration and Hyperuricemia
The sleep duration was obtained through a unified self-administrated questionnaire. All participants were asked the following question about sleep duration: “On average, how many hours do you sleep per day”. There were five options for the question: (1) <6 h; (2) 6–7 h; (3) 7–8 h; (4) 8–9 h; and (5) ≥9 h. Participants were categorized into three groups: 7–8 h as the reference group, <7 h as the short sleep duration group, and ≥8 h as the long sleep duration group, which was consistent with previous studies [21]. Serum UA was measured using Roche Cobas C 501 biochemical analyzer. Hyperuricemia was defined as UA ≥ 420 μmol/L in males or UA ≥ 360 μmol/L in females [25,26].
2.3. Covariates
The questionnaire collected demographic characteristics (i.e., age, sex, marital status, income, education status), lifestyle behavior (i.e., alcohol drinking, cigarette smoking, leisure-time physical activity), and medical conditions. Marital status was classified into two groups: married and the others (including never married, divorced, and widowed). Personal annual income was identified as three levels: CNY < 0.1 million (Chinese Yuan), CNY 0.1–0.2 million, CNY > 0.2 million per year. The education attainment was divided into three categories: bachelor’s degree or lower, master’s degree, and doctoral degree. Smoking status, drinking status, and leisure-time physical activity status were dichotomized into yes or no.
All biochemical markers, including serum creatinine (SCR), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), blood glucose, and amount of white blood cells (WBC), were measured using a Roche Cobas C 501 biochemical analyzer. Physical examinations, such as height, weight, abdominal circumference, and blood pressure (BP), were performed by trained physicians. BMI was calculated as weight in kilograms divided by height squared in meters, and then dichotomized as a binary variable with a cut point of 24 kg/m2 [27]. Abdominal obesity was defined as abdominal circumference >90 cm in males or >85 cm in females [28]. BP was measured with a regular mercury sphygmomanometer on the right arm after resting for at least five minutes. Hypertension was determined as systolic blood pressure ≥140 or diastolic blood pressure ≥90, including the use of anti-hypertension medication or self-reported history of hypertension [29]. Fasting serum HDL-C ≤ 1.04 mmol/L indicated low high-density lipoprotein, and fasting serum TG ≥ 1.70 mmol/L was classified as high triglycerides [28]. Diabetes was determined when fasting serum glucose ≥ 7.0 mmol/L or glycosylated hemoglobin ≥ 6.5%, including use of hypoglycemic drugs and self-reported history of diabetes [30]. WBC classification was described as a binary variable including a low (<7 × 109/L) and high level (≥7 × 109/L).
2.4. Statistical Analysis
The distribution of continuous variables was tested using the Shapiro–Wilk normality test. Continuous variables with normal distribution were described as means and standard deviations (SD). Other continuous variables used medians and interquartile ranges. Categorical variables were described as frequencies and percentages. The characteristics at baseline were compared in groups according to sleep duration by the chi-square test for categorical variables, analysis of variance (ANOVA) test for continuous variables with homogeneous variance, and the Kruskal–Wallis test for continuous variables without homogeneous variance. We assigned a separate group for the missing values in categorical variables.
The Cox proportional hazard regression model was used to calculate the hazard ratio (HR) and 95% confidence interval (CI). Survival time was defined as the time difference from the first visit to the examination which documented hyperuricemia or taking UA-lowering drugs for the first time, or the last visit, whenever came first. The incidence of hyperuricemia (per 1000 person-years) was calculated according to the sleep duration category. Four models were estimated: Model 1: Only adjusted for sex and age; Model 2: Additionally adjusted for education level, personal annual income, marital status, smoking status, drinking status, and leisure-time physical activity status based on Model 1; Model 3: was the fully adjusted model in this research, which additionally adjusted for BMI, abdominal circumference, hypertension, diabetes, triglycerides, and high-density lipoprotein cholesterol based on Model (2) and (4); and Model 4: To test potential intermediate factors by inflammation, we further adjusted the amount of white blood cells based on Model 3. To access the linear trend between sleep and hyperuricemia, we also fitted restricted cubic splines with 5 knots to flexibly model the association. To further explore the modification effects by different covariates, subgroup analysis was also conducted.
In addition, sensitivity analyses based on the fully adjusted model were performed as follows: (1) Re-run the cox proportional risk regression analysis by excluding participants with missing data; (2) Use the five-category sleep duration to test the dose–response relationship between sleep duration and hyperuricemia. Two-sides p < 0.05 were considered as statistically significant, and all analyses were completed using SAS statistical software version 9.4.
3. Results
3.1. Baseline Characteristics
At baseline, the mean age was 38.31 ± 9.59 years old and 54.38% of participants were women. A total of 19420 (57.08%) participants reported short sleep duration, and 2301 (6.76%) participants were in the long sleep group. The baseline characteristics were shown by different sleep duration groups in Table 1. Compared with other groups, long sleepers were most likely to be women, younger, to report the lowest education attainment and annual income, and they had the lowest proportion in drinking, leisure-time physical activity, overweight or obesity, abdominal obesity, and low HDL-C (p for difference < 0.05 for each) (Table 1).

Table 1.
Baseline characteristics of participants by sleep duration.
3.2. Association between Sleep Duration and Hyperuricemia
With the follow-up of a median 3.08 (interquartile range: 1.92–5.17) years, 4868 incident hyperuricemia were documented, with a total crude incidence 39.49 per 1000 person-years.
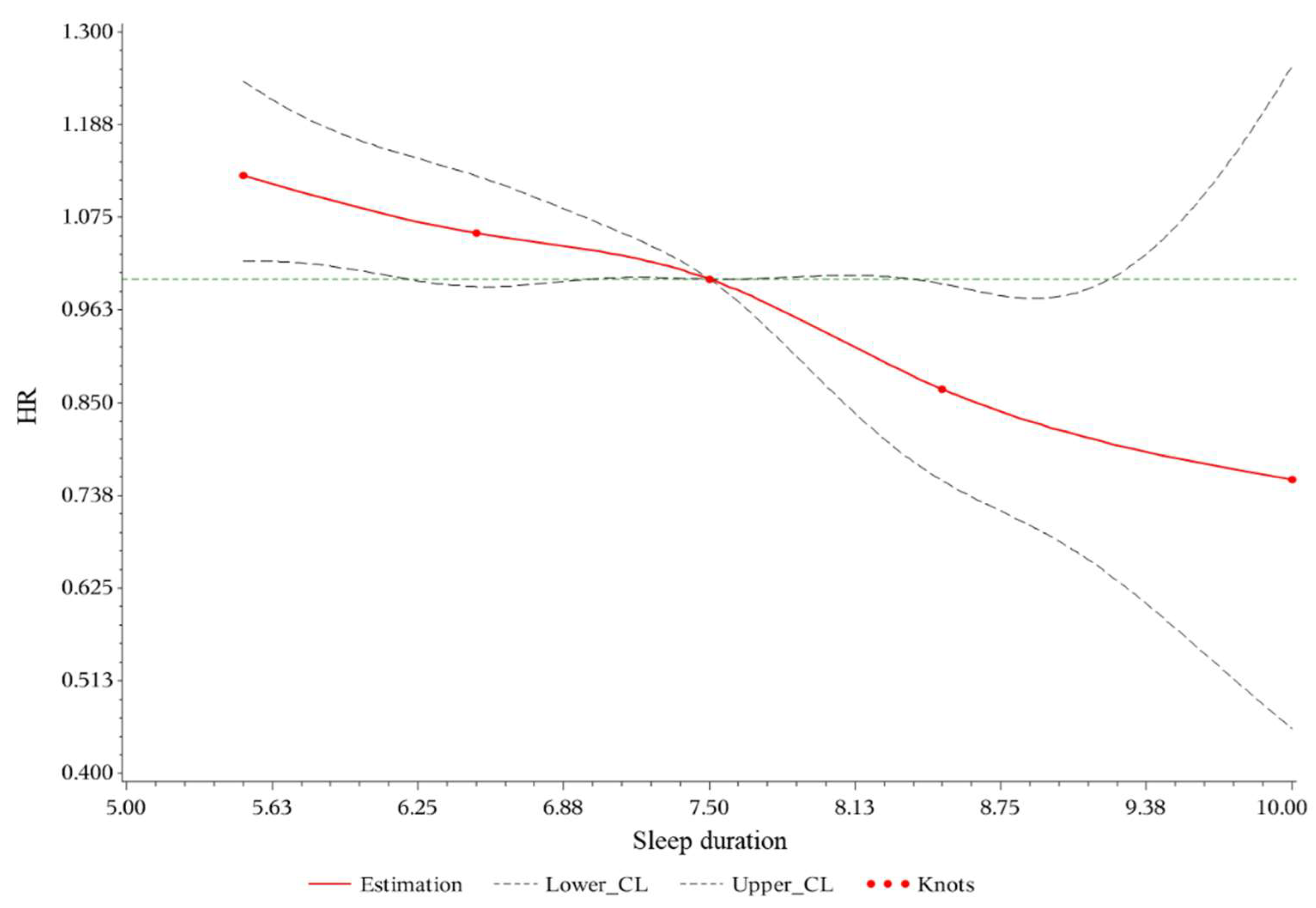
After adjusting for demographic factors, habits, and metabolism-related covariates (Model 3), HR was 1.07 (95%CI: 1.01–1.14) for short sleep duration and 0.85 (95%CI: 0.74–0.97) for long sleep duration. Adding adjustment of white blood cell amount, HR was 1.07 (95%CI: 1.00–1.13) for short sleep duration with marginal significance and 0.84 (95%CI: 0.74–0.97) for long sleep duration in Model 4. All four models showed a significant inverse trend (p for trend < 0.001) (Table 2). No significant nonlinearity was detected based on restricted cubic spline (Figure 2, p for nonlinearity > 0.05) In the additional sensitivity analyses, the results remained unchanged (shown in Table A1). In the five-category sleep duration analysis, a significant inverse trend (p for trend < 0.001) was also observed in all four models (shown in Table A2).
Table 2.
Association of sleep duration with risk of hyperuricemia in different model.
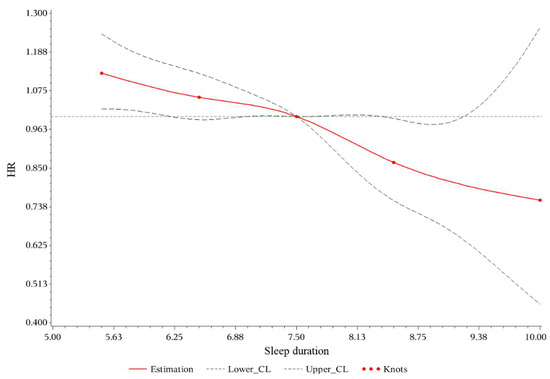
Figure 2.
Restricted cubic spline plots for hyperuricemia by sleep duration. HR indicates hazard ratio; CL, confidence limit. Multivariable Cox regression models with restricted cubic splines show the hazard ratio for the incidence of hyperuricemia adjusted for sex, age, education level, personal income, marital status, smoking status, drinking status, exercise status, Body Mass Index, abdominal circumference, hypertension, diabetes, triglycerides, high-density lipoprotein cholesterol, and amount of white blood cells. The dotted lines indicate 95% CL. The x-axis represents the sleep duration. The y axis represents the HR of hyperuricemia.
The associations were similar across different levels of covariates. Only the interaction between sleep duration and BMI was significant (p for interaction = 0.035) (Table 3). A 16.3% higher risk of hyperuricemia for short sleep individuals with normal weight. A 19.9% lower risk of hyperuricemia for those who reported long sleep duration and overweight or obesity was found.
Table 3.
Association of sleep duration with risk of hyperuricemia in different subgroups and interactions.
4. Discussion
In this prospective study, a dose–response effect of sleep duration was observed on hyperuricemia in Chinese adults. Short sleep duration was associated with a 7% higher risk of hyperuricemia, while a long sleep duration showed a 15% lower risk. The findings highlighted that extending sleep duration might be a potential public health strategy to prevent hyperuricemia.
Sleep loss is still a global problem, and there is still a lack of corresponding policies worldwide. In this study, only 36.16% of participants had a recommended sleep duration, and over one-half of participants slept less than 7 h. Our results are in line with several previous studies that estimated the association of sleep duration with hyperuricemia. Consistent with previous cross-sectional studies [22,23,31], short sleep duration was considered as a risk factor for hyperuricemia in this study. Appropriate public health actions should be taken to increase the sleep time of the population to reduce the damage to health caused by sleep that is too short, especially among subgroups with a low HDL-C, a high TG, or those who are not overweight.
This study provides further evidence that sleep duration is independently associated with hyperuricemia after adjusting for known risk factors and potential confounders. Unlike a U-shaped curve reported in Korean women [22], our findings indicated that longer sleep (>8 h) could also reduce the incidence of hyperuricemia significantly, which was consistent with previous studies [23,32]. In this prospective longitudinal study, sufficient samples and prospective study design avoided reverse causality by chronological order. Interestingly, although we found that the participants who had a longer sleep duration had a lower risk of hyperuricemia, previous studies showed that long sleep was detrimental to health [33,34,35]. In addition, studies have shown that a low level of uric acid was a risk factor for Parkinson’s disease [32] and Alzheimer’s disease [36]. Thus, the choice of sleep duration needs to comprehensively consider the other problems caused by a long sleep duration.
Two underlying mechanisms could explain our findings of the inverse association of sleep duration with hyperuricemia. One possible way for sleep duration to alter metabolism might be by affecting levels of catecholamine. Catecholamine is an essential neuroactive transmitter, facilitating the breakdown of nucleotides, leading to more production of endogenous uric acid [37]. The activity of locus coeruleus catecholamine was reported to decrease during sleeping, which would reduce the level of uric acid [38]. Moreover, animal models have proved that catecholamines play an important role in the occurrence of hyperuricemia [39]. The other pathway might be related to inflammatory reactions. Studies have shown that sleep duration substantially affected inflammatory mediators, inducing a series of chronic inflammatory diseases [21,40,41]. As an activator of the immune system [10], uric acid enrolls in the body’s inflammatory response. Previous studies showed that the number of white blood cells was a potential intermediate factor between sleep duration and hyperuricemia [23,42]. After adjusting the amount of white blood cells in this study, the association between short sleep duration and hyperuricemia was no longer significant, which supported the hypothesis. Moreover, interactions among metabolites should be noticed. Cicero et al. found that a high serum uric acid level and a high serum LDL-C level would have an interaction on incidence of hypertension [43], which further proves the complexity of interactions among metabolites. In the subgroup analysis, BMI was found to have an interaction between sleep duration and hyperuricemia. This might be related to the different metabolic status of individuals with different BMI level [44]. Notably, short sleep duration is associated with a 16% increase in risk for hyperuricemia in the participants with a BMI < 24, which provides insights into screening high-risk populations and protection of susceptible people.
To the best of our knowledge, the present study is the first population-based prospective study which included a large sample size to study the relationship between sleep duration and hyperuricemia. We conducted a comprehensive analysis by adjusting potential risk factors and confounders, including comprehensive laboratory markers, which enabled us with to examine the possible mechanism of the association.
However, some limitations should be mentioned. First, the participants enrolled in the present study were from Beijing, with higher education attainment and annual income, but a relatively lower percentage of long sleepers as compared to the other studies, which limited the extrapolation of our findings. Second, the follow-up time was calculated from each health check-up visit, hence diagnosis time could be delayed, leading to underestimation of the association. Third, some covariates were missing. However, the sensitivity analysis showed the robustness of our findings using a simple imputation. In addition, although the sleep duration related questions were similar to those in previous studies [18,45], our questionnaires were not validated. Further validation of the questionnaires is needed in future research.
5. Conclusions
Sleep duration was inversely associated with hyperuricemia, which indicated that short sleep duration might cause hyperuricemia. In contrast, long sleep duration might be a protective factor. The findings suggest that maintaining healthy sleep habits would be a potential intervention to prevent hyperuricemia, which highlights the public health significance of sufficient sleep duration.
Author Contributions
Conceptualization, H.Y. (Huan Yu), J.L., B.W., C.Y. and L.L.; Data curation, S.M., J.Y. and B.W.; Formal analysis, H.Y. (Huan Yu), K.S. and H.Y. (Haiming Yang); Funding acquisition, J.L., C.Y. and L.L.; Methodology, K.S., H.Y. (Haiming Yang), D.S. and C.Y.; Project administration, H.Y. (Huan Yu); Resources, J.Y., B.W., C.Y. and L.L.; Software, H.Y. (Huan Yu), K.S., H.Y. (Haiming Yang) and Y.M.; Supervision, D.S., J.L., B.W., C.Y. and L.L.; Validation, Y.M.; Visualization, S.M.; Writing—original draft, H.Y. (Huan Yu) and C.Y.; Writing—review and editing, H.Y. (Huan Yu), K.S., H.Y. (Haiming Yang), D.S., J.L., Y.M., S.M., J.Y., B.W., C.Y. and L.L. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (91846303). The funders had no role in the study design, data collection, data analysis and interpretation, writing of the report, or the decision to submit the article for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the project has been approved by the Peking University biological and medical ethics committee (IRB0001052-19077).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets analyzed during the current study are not publicly available due to the protection of privacy considering the ethics but are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A
Table A1.
Association of sleep duration with risk of hyperuricemia after excluding missing data (n = 17,325, events = 2561).
Table A1.
Association of sleep duration with risk of hyperuricemia after excluding missing data (n = 17,325, events = 2561).
| Models | HR (95%CI) | ||
|---|---|---|---|
| <7 h | 7–8 h | ≥8 h | |
| Events | 1598 | 837 | 126 |
| Person year | 37,809.5 | 22,176.08 | 4411.167 |
| Incidence Rate (/1000 py) | 42.27 | 37.74 | 28.56 |
| Model 1 | 1.055 (0.970, 1.148) | ref | 0.804 (0.667, 0.970) |
| Model 2 | 1.055 (0.969, 1.148) | ref | 0.798 (0.662, 0.963) |
| Model 3 | 1.018 (0.935, 1.108) | ref | 0.788 (0.653, 0.950) |
| Model 4 | 1.014 (0.931, 1.104) | ref | 0.785 (0.651, 0.947) |
Abbreviation: HR indicates hazard ratio; CI, confidence interval; py, person-year. Model 1: Only adjusted for sex and age; Model 2: education level, personal income, marital status, smoking status, drinking status, and exercise status were additionally adjusted based on Model 1; Model 3: BMI, abdominal circumference, hypertension, diabetes, triglycerides, and high-density lipoprotein cholesterol, were further adjusted based on Model 2; Model 4: further adjusted amount of white blood cells based on Model 3.
Table A2.
Sensitivity analysis in association of five sleep duration groups with risk of hyperuricemia.
Table A2.
Sensitivity analysis in association of five sleep duration groups with risk of hyperuricemia.
| Models | HR (95%CI) | p for Trend | ||||
|---|---|---|---|---|---|---|
| <6 h | 6–7 h | 7–8 h | 8–9 h | ≥9 h | ||
| Events | 571 | 2382 | 1668 | 232 | 15 | |
| Person year | 12,943.17 | 56,837.42 | 44,966.25 | 7913.58 | 598.33 | |
| Incidence Rate (/1000 py) | 44.12 | 41.91 | 37.09 | 29.32 | 25.07 | |
| Model 1 | 1.200 (1.089, 1.322) | 1.090 (1.023, 1.160) | ref | 0.865 (0.754, 0.992) | 0.836 (0.503, 1.389) | <0.001 |
| Model 2 | 1.176 (1.067, 1.296) | 1.084 (1.017, 1.155) | ref | 0.855 (0.745, 0.981) | 0.795 (0.478, 1.322) | <0.001 |
| Model 3 | 1.128 (1.023, 1.243) | 1.058 (0.993, 1.128) | ref | 0.854 (0.744, 0.980) | 0.752 (0.452, 1.251) | <0.001 |
| Model 4 | 1.116 (1.012, 1.230) | 1.055 (0.990, 1.125) | ref | 0.852 (0.743, 0.978) | 0.734 (0.441, 1.221) | <0.001 |
Abbreviation: HR indicates hazard ratio; CI, confidence interval; py, person-year. Model 1: Only adjusted for sex and age; Model 2: education level, personal income, marital status, smoking status, drinking status, and exercise status were additionally adjusted based on Model 1; Model 3: BMI, abdominal circumference, hypertension, diabetes, triglycerides, and high-density lipoprotein cholesterol, were further adjusted based on Model 2; Model 4: further adjusted amount of white blood cells based on Model 3.
References
- Li, X.; Meng, X.; Timofeeva, M.; Tzoulaki, I.; Tsilidis, K.K.; Ioannidis, J.P.; Campbell, H.; Theodoratou, E. Serum uric acid levels and multiple health outcomes: Umbrella review of evidence from observational studies, randomised controlled trials, and Mendelian randomisation studies. BMJ 2017, 357, j2376. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, M.; Hisatome, I.; Niwa, K.; Hara, S.; Roncal-Jimenez, C.A.; Bjornstad, P.; Nakagawa, T.; Andres-Hernando, A.; Sato, Y.; Jensen, T.; et al. Uric Acid Is a Strong Risk Marker for Developing Hypertension From Prehypertension: A 5-Year Japanese Cohort Study. Hypertension 2018, 71, 78–86. [Google Scholar] [CrossRef]
- Kuwabara, M.; Niwa, K.; Hisatome, I.; Nakagawa, T.; Roncal-Jimenez, C.A.; Andres-Hernando, A.; Bjornstad, P.; Jensen, T.; Sato, Y.; Milagres, T.; et al. Asymptomatic Hyperuricemia Without Comorbidities Predicts Cardiometabolic Diseases: Five-Year Japanese Cohort Study. Hypertension 2017, 69, 1036–1044. [Google Scholar] [CrossRef]
- Han, T.; Meng, X.; Shan, R.; Zi, T.; Li, Y.; Ma, H.; Zhao, Y.; Shi, D.; Qu, R.; Guo, X.; et al. Temporal relationship between hyperuricemia and obesity, and its association with future risk of type 2 diabetes. Int. J. Obes. 2018, 42, 1336–1344. [Google Scholar] [CrossRef]
- Jayachandran, M.; Qu, S. Harnessing hyperuricemia to atherosclerosis and understanding its mechanistic dependence. Med. Res. Rev. 2021, 41, 616–629. [Google Scholar] [CrossRef]
- Ponticelli, C.; Podestà, M.A.; Moroni, G. Hyperuricemia as a trigger of immune response in hypertension and chronic kidney disease. Kidney Int. 2020, 98, 1149–1159. [Google Scholar] [CrossRef]
- Borghi, C.; Palazzuoli, A.; Landolfo, M.; Cosentino, E. Hyperuricemia: A novel old disorder-relationship and potential mechanisms in heart failure. Heart Fail. Rev. 2020, 25, 43–51. [Google Scholar] [CrossRef]
- Chaudhary, N.S.; Bridges, S.L., Jr.; Saag, K.G.; Rahn, E.J.; Curtis, J.R.; Gaffo, A.; Limdi, N.A.; Levitan, E.B.; Singh, J.A.; Colantonio, L.D.; et al. Severity of Hypertension Mediates the Association of Hyperuricemia With Stroke in the REGARDS Case Cohort Study. Hypertension 2020, 75, 246–256. [Google Scholar] [CrossRef]
- Cabău, G.; Crișan, T.O.; Klück, V.; Popp, R.A.; Joosten, L.A.B. Urate-induced immune programming: Consequences for gouty arthritis and hyperuricemia. Immunol. Rev. 2020, 294, 92–105. [Google Scholar] [CrossRef] [Green Version]
- Joosten, L.A.B.; Crişan, T.O.; Bjornstad, P.; Johnson, R.J. Asymptomatic hyperuricaemia: A silent activator of the innate immune system. Nat. Rev. Rheumatol. 2020, 16, 75–86. [Google Scholar] [CrossRef]
- Chen-Xu, M.; Yokose, C.; Rai, S.K.; Pillinger, M.H.; Choi, H.K. Contemporary Prevalence of Gout and Hyperuricemia in the United States and Decadal Trends: The National Health and Nutrition Examination Survey, 2007–2016. Arthritis Rheumatol. 2019, 71, 991–999. [Google Scholar] [CrossRef]
- Song, P.; Wang, H.; Xia, W.; Chang, X.; Wang, M.; An, L. Prevalence and correlates of hyperuricemia in the middle-aged and older adults in China. Sci. Rep. 2018, 8, 4314. [Google Scholar] [CrossRef]
- Dehlin, M.; Jacobsson, L.; Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 2020, 16, 380–390. [Google Scholar] [CrossRef]
- Zhou, L.; Yu, K.; Yang, L.; Wang, H.; Xiao, Y.; Qiu, G.; Liu, X.; Yuan, Y.; Bai, Y.; Li, X.; et al. Sleep duration, midday napping, and sleep quality and incident stroke: The Dongfeng-Tongji cohort. Neurology 2020, 94, e345–e356. [Google Scholar] [CrossRef]
- Smiley, A.; King, D.; Bidulescu, A. The Association between Sleep Duration and Metabolic Syndrome: The NHANES 2013/2014. Nutrients 2019, 11, 2582. [Google Scholar] [CrossRef] [Green Version]
- Prather, A.A.; Janicki-Deverts, D.; Hall, M.H.; Cohen, S. Behaviorally Assessed Sleep and Susceptibility to the Common Cold. Sleep 2015, 38, 1353–1359. [Google Scholar] [CrossRef]
- Wang, C.; Bangdiwala, S.I.; Rangarajan, S.; Lear, S.A.; AlHabib, K.F.; Mohan, V.; Teo, K.; Poirier, P.; Tse, L.A.; Liu, Z.; et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: A study of 116,632 people from 21 countries. Eur. Heart J. 2019, 40, 1620–1629. [Google Scholar] [CrossRef]
- Liu, Y.; Wheaton, A.G.; Chapman, D.P.; Cunningham, T.J.; Lu, H.; Croft, J.B. Prevalence of Healthy Sleep Duration among Adults—United States, 2014. Morb. Mortal Wkly. Rep. 2016, 65, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Bakour, C.; Schwartz, S.; O’Rourke, K.; Wang, W.; Sappenfield, W.; Couluris, M.; Chen, H. Sleep Duration Trajectories and Systemic Inflammation in Young Adults: Results From the National Longitudinal Study of Adolescent to Adult Health (Add Health). Sleep 2017, 40, zsx156. [Google Scholar] [CrossRef]
- Holingue, C.; Owusu, J.T.; Feder, K.A.; Spira, A.P. Sleep duration and C-reactive protein: Associations among pregnant and non-pregnant women. J. Reprod. Immunol. 2018, 128, 9–15. [Google Scholar] [CrossRef]
- Irwin, M.R.; Olmstead, R.; Carroll, J.E. Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation. Biol. Psychiatry 2016, 80, 40–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.C.; Son, D.H.; Kwon, Y.J. U-Shaped Association between Sleep Duration, C-Reactive Protein, and Uric Acid in Korean Women. Int. J. Environ. Res. Public Health 2020, 17, 2657. [Google Scholar] [CrossRef] [PubMed]
- Papandreou, C.; Babio, N.; Díaz-López, A.; Martínez-González, M.; Becerra-Tomas, N.; Corella, D.; Schröder, H.; Romaguera, D.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Sleep Duration is Inversely Associated with Serum Uric Acid Concentrations and Uric Acid to Creatinine Ratio in an Elderly Mediterranean Population at High Cardiovascular Risk. Nutrients 2019, 11, 761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MJ Health Care. Available online: https://www.mjlife.com.cn/ (accessed on 17 May 2022).
- Lin, K.C.; Lin, H.Y.; Chou, P. Community based epidemiological study on hyperuricemia and gout in Kin-Hu, Kinmen. J. Rheumatol. 2000, 27, 1045–1050. [Google Scholar]
- Bardin, T.; Richette, P. Definition of hyperuricemia and gouty conditions. Curr. Opin. Rheumatol. 2014, 26, 186–191. [Google Scholar] [CrossRef]
- Chen, C.; Lu, F.C. The guidelines for prevention and control of overweight and obesity in Chinese adults. Biomed. Environ. Sci. BES 2004, 17, 1–36. [Google Scholar]
- Joint Committee for Developing Chinese Guidelines on Prevention and Treatment of Dyslipidemia in Adults. Chinese guidelines on prevention and treatment of dyslipidemia in adults. Zhonghua Xin Xue Guan Bing Za Zhi 2007, 35, 390–419. [Google Scholar]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Executive summary: Standards of medical care in diabetes—2012. Diabetes Care 2012, 35 (Suppl. S1), S4–S10. [CrossRef] [Green Version]
- Chou, Y.T.; Li, C.H.; Shen, W.C.; Yang, Y.C.; Lu, F.H.; Wu, J.S.; Chang, C.J. Association of sleep quality and sleep duration with serum uric acid levels in adults. PLoS ONE 2020, 15, e0239185. [Google Scholar] [CrossRef]
- van Wamelen, D.J.; Taddei, R.N.; Calvano, A.; Titova, N.; Leta, V.; Shtuchniy, I.; Jenner, P.; Martinez-Martin, P.; Katunina, E.; Chaudhuri, K.R. Serum Uric Acid Levels and Non-Motor Symptoms in Parkinson’s Disease. J. Parkinsons Dis. 2020, 10, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Floras, J.S. Sleep Apnea and Cardiovascular Disease: An Enigmatic Risk Factor. Circ. Res. 2018, 122, 1741–1764. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Zhou, Z.; McEvoy, R.D.; Anderson, C.S.; Rodgers, A.; Perkovic, V.; Neal, B. Association of Positive Airway Pressure With Cardiovascular Events and Death in Adults With Sleep Apnea: A Systematic Review and Meta-analysis. JAMA 2017, 318, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Kwon, Y.; Koene, R.J.; Johnson, A.R.; Lin, G.M.; Ferguson, J.D. Sleep, sleep apnea and atrial fibrillation: Questions and answers. Sleep Med. Rev. 2018, 39, 134–142. [Google Scholar] [CrossRef]
- Du, N.; Xu, D.; Hou, X.; Song, X.; Liu, C.; Chen, Y.; Wang, Y.; Li, X. Inverse Association Between Serum Uric Acid Levels and Alzheimer’s Disease Risk. Mol. Neurobiol. 2016, 53, 2594–2599. [Google Scholar] [CrossRef]
- Glantzounis, G.K.; Tsimoyiannis, E.C.; Kappas, A.M.; Galaris, D.A. Uric acid and oxidative stress. Curr. Pharm. Des. 2005, 11, 4145–4151. [Google Scholar] [CrossRef]
- Hayat, H.; Regev, N.; Matosevich, N.; Sales, A.; Paredes-Rodriguez, E.; Krom, A.J.; Bergman, L.; Li, Y.; Lavigne, M.; Kremer, E.J.; et al. Locus coeruleus norepinephrine activity mediates sensory-evoked awakenings from sleep. Sci. Adv. 2020, 6, eaaz4232. [Google Scholar] [CrossRef] [Green Version]
- Sumi, T.; Umeda, Y. Adrenergic regulation of the plasma levels of purine metabolites in the rat. Eur. J. Pharmacol. 1977, 46, 243–247. [Google Scholar] [CrossRef]
- Besedovsky, L.; Lange, T.; Haack, M. The Sleep-Immune Crosstalk in Health and Disease. Physiol. Rev. 2019, 99, 1325–1380. [Google Scholar] [CrossRef] [Green Version]
- Tobaldini, E.; Fiorelli, E.M.; Solbiati, M.; Costantino, G.; Nobili, L.; Montano, N. Short sleep duration and cardiometabolic risk: From pathophysiology to clinical evidence. Nat. Rev. Cardiol. 2019, 16, 213–224. [Google Scholar] [CrossRef]
- Boudjeltia, K.Z.; Faraut, B.; Stenuit, P.; Esposito, M.J.; Dyzma, M.; Brohée, D.; Ducobu, J.; Vanhaeverbeek, M.; Kerkhofs, M. Sleep restriction increases white blood cells, mainly neutrophil count, in young healthy men: A pilot study. Vasc. Health Risk Manag. 2008, 4, 1467–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cicero, A.F.G.; Fogacci, F.; Giovannini, M.; Grandi, E.; D’Addato, S.; Borghi, C. Interaction between low-density lipoprotein-cholesterolaemia, serum uric level and incident hypertension: Data from the Brisighella Heart Study. J. Hypertens. 2019, 37, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Kuwabara, R.; Niwa, K.; Hisatome, I.; Smits, G.; Roncal-Jimenez, C.A.; MacLean, P.S.; Yracheta, J.M.; Ohno, M.; Lanaspa, M.A.; et al. Different Risk for Hypertension, Diabetes, Dyslipidemia, and Hyperuricemia According to Level of Body Mass Index in Japanese and American Subjects. Nutrients 2018, 10, 1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leng, Y.; Cappuccio, F.P.; Wainwright, N.W.; Surtees, P.G.; Luben, R.; Brayne, C.; Khaw, K.T. Sleep duration and risk of fatal and nonfatal stroke: A prospective study and meta-analysis. Neurology 2015, 84, 1072–1079. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).