
Real-World Evidence for the Association between Heat-Related Illness and the Risk of Psychiatric Disorders in Taiwan

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Design
2.3. Variable Measures
2.4. Statistical Analyses
3. Results
3.1. Description of Study Cohorts with and without HRI at the Baseline
3.2. Heat-Related Illness and the Risk of Psychiatric Disorders
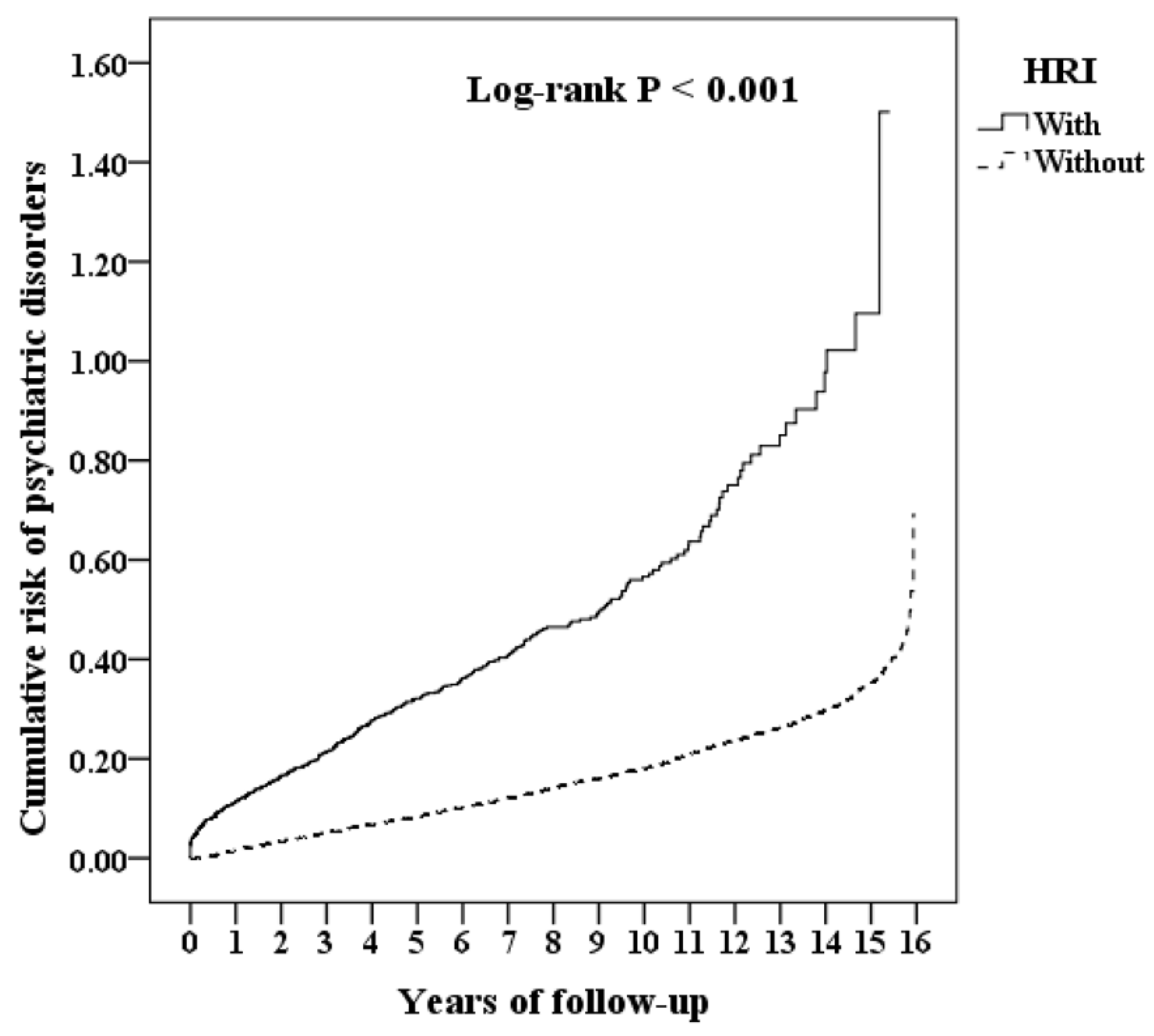
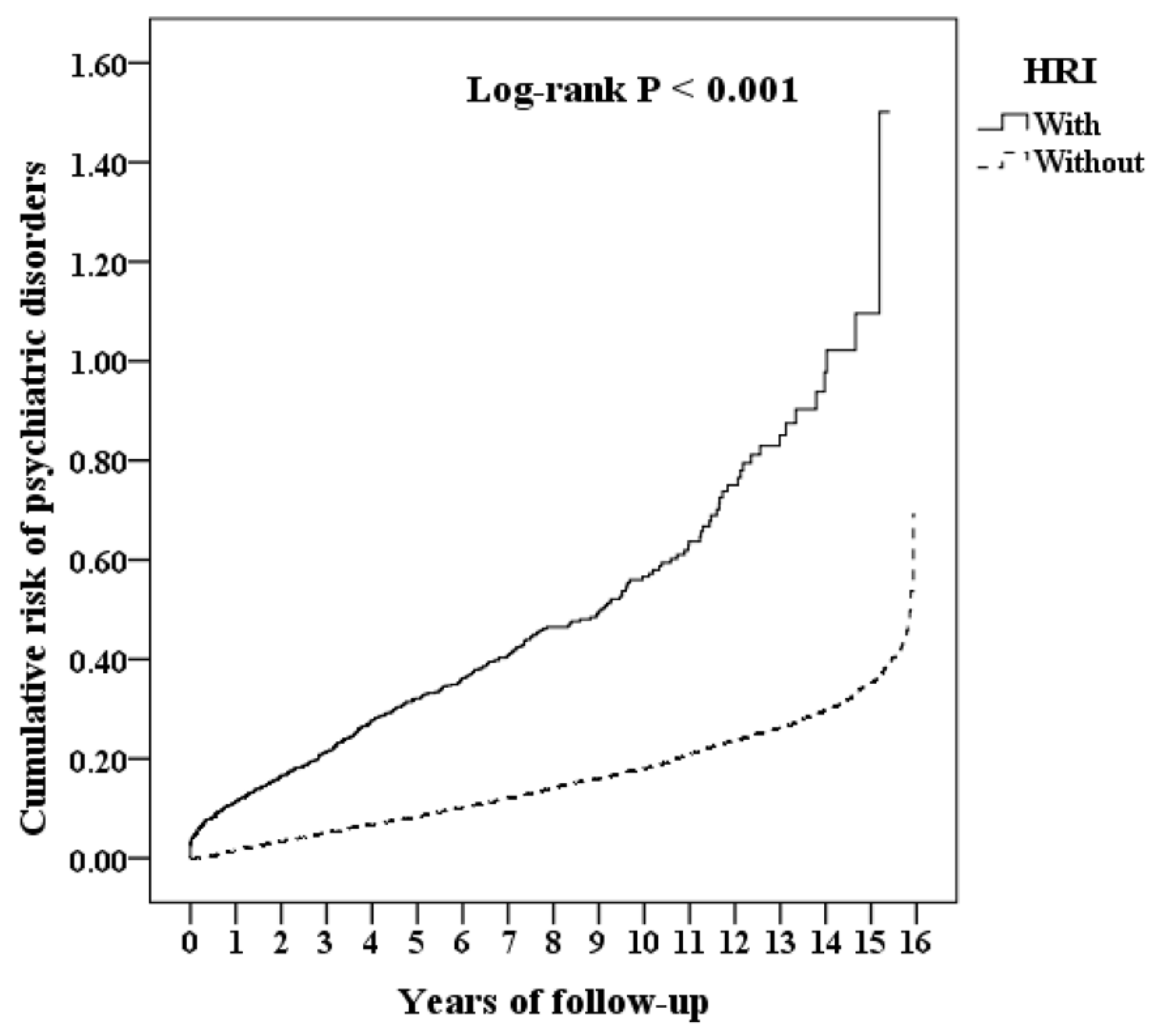
3.3. Kaplan–Meier Model for the Cumulative Incidence of Psychiatric Disorders
3.4. Subgroup Analysis Stratified by the Different Characteristics
3.5. Heat-Related Illnesses, the Situations, and the Association with Psychiatric Disorders
3.6. Sensitivity Analysis
4. Discussion
4.1. Potential Underlying Mechanisms
4.2. Strengths
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lin, R.T.; Chan, C.C. Effects of heat on workers’ health and productivity in Taiwan. Glob. Health Action 2009, 2, 2024. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, F.G.; Grissom, C.K. Cooling methods in heat stroke. J. Emerg. Med. 2016, 50, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Kakamu, T.; Endo, S.; Hidaka, T.; Masuishi, Y.; Kasuga, H.; Fukushima, T. Heat-related illness risk and associated personal and environmental factors of construction workers during work in summer. Sci. Rep. 2021, 11, 1119. [Google Scholar] [CrossRef]
- Lu, K.C.; Wang, T.L. Heat stroke. Ann. Disaster Med. 2004, 2 (Suppl. 2), s97–s109. [Google Scholar]
- Gauer, R.; Meyers, B.K. Heat-Related Illnesses. Am. Fam. Physician 2019, 99, 482–489. [Google Scholar]
- O’connor, F.G.; Williams, A.D.; Blivin, S.; Heled, Y.; Deuster, P.; Flinn, S.D. Guidelines for return to duty (play) after heat illness: A military perspective. J. Sport Rehabil. 2007, 16, 227–237. [Google Scholar] [CrossRef]
- Becker, J.A.; Stewart, L.K. Heat-related illness. Am. Fam. Physician 2011, 83, 1325–1330. [Google Scholar]
- Dematte, J.E.; O’Mara, K.; Buescher, J.; Whitney, C.G.; Forsythe, S.; McNamee, T.; Adiga, R.B.; Ndukwu, I.M. Near-fatal heat stroke during the 1995 heat wave in Chicago. Ann. Intern. Med. 1998, 129, 173–181. [Google Scholar] [CrossRef]
- Wang, J.C.; Chien, W.C.; Chu, P.; Chung, C.H.; Lin, C.Y.; Tsai, S.H. The association between heat stroke and subsequent cardiovascular diseases. PLoS ONE 2019, 14, e0211386. [Google Scholar] [CrossRef]
- Tseng, M.F.; Chou, C.L.; Chung, C.H.; Chen, Y.K.; Chien, W.C.; Feng, C.H.; Chu, P. Risk of chronic kidney disease in patients with heat injury: A nationwide longitudinal cohort study in Taiwan. PLoS ONE 2020, 15, e0235607. [Google Scholar] [CrossRef]
- Szold, O.; Reider-Groswasser, I.I.; Abraham, R.B.; Aviram, G.; Segev, Y.; Biderman, P.; Sorkine, P. Gray–white matter discrimination—A possible marker for brain damage in heat stroke? Eur. J. Radiol. 2002, 43, 1–5. [Google Scholar] [CrossRef]
- Kalaiselvan, M.; Renuka, M.; Arunkumar, A. A retrospective study of clinical profile and outcomes of critically ill patients with heat-related illness. Indian J. Anaesth. 2015, 59, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Sun, G.; Qian, S.; Jiang, Q.; Liu, K.; Li, B.; Li, M.; Zhao, L.; Zhou, Z.; von Deneen, K.M.; Liu, Y. Hyperthermia-induced disruption of functional connectivity in the human brain network. PLoS ONE 2013, 8, e61157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, E.M.; Pearce, H.; Gabb, G.M. Review article: Environmental heatstroke and long-term clinical neurological outcomes: A literature review of case reports and case series 2000–2016. Emerg. Med. Australas. 2019, 31, 163–173. [Google Scholar] [CrossRef]
- Yang, Y.; Wang, C.; Xiang, Y.; Lu, J.; Penzel, T. Editorial: Mental disorders associated with neurological diseases. Front. Psychiatry 2020, 11, 196. [Google Scholar] [CrossRef] [Green Version]
- Ho Chan, W.S. Taiwan’s healthcare report 2010. EPMA J. 2010, 1, 563–585. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.Y.; Su, C.C.; Shao, S.C.; Sung, S.F.; Lin, S.J.; Yang, Y.H.K.; Lai, E.C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Hsing, S.C.; Jin, Y.T.; Tzeng, N.S.; Chung, C.H.; Chen, T.Y.; Chang, H.A.; Kao, Y.C.; Chien, W.C. Is agomelatine associated with less sedative-hypnotic usage in patients with major depressive disorder? A nationwide, population-based study. Neuropsychiatr. Dis. Treat. 2020, 16, 1727–1736. [Google Scholar] [CrossRef]
- Hsu, W.F.; Chien, W.C.; Chung, C.H.; Lee, P.C.; Wang, D.S.; Huang, S.W.; Chang, H.A.; Kao, Y.C.; Yang, S.S.; Tzeng, N.S. Association between tetralogy of fallot and psychiatric disorders: A nationwide cohort study. J. Clin. Psychiatry 2021, 82, 28323. [Google Scholar] [CrossRef]
- Li, L.Y.; Chien, W.C.; Wang, J.C.; Tzeng, N.S.; Chung, C.H.; Lin, C.Y.; Tsai, S.H. Association between abdominal aortic aneurysms and alcohol-related diseases. Medicine 2020, 99, e22968. [Google Scholar] [CrossRef]
- Lin, I.J.; Tzeng, N.S.; Chung, C.H.; Chien, W.C. Psychiatric disorders in female psychosexual disorders-a nationwide, cohort study in Taiwan: Psychiatric disorders and female psychosexual disorders. BMC Psychiatry 2021, 21, 63. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.C.; Chen, T.Y.; Chien, W.C.; Chung, C.H.; Chang, H.A.; Kao, Y.C.; Tsai, C.S.; Lin, C.S.; Tzeng, N.S. Stimulants associated with reduced risk of hospitalization for motor vehicle accident injury in patients with obstructive sleep apnea-a nationwide cohort study. BMC Pulm. Med. 2020, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.P.; Chien, W.C.; Chung, C.H.; Chang, H.A.; Kao, Y.C.; Tzeng, N.S. Are anticholinergic medications associated with increased risk of dementia and behavioral and psychological symptoms of dementia? A nationwide 15-year follow-up cohort study in Taiwan. Front. Pharmacol. 2020, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinese Hospital Association. ICD-9-CM English-Chinese Dictionary; Chinese Hospital Association Press: San Francisco, CA, USA, 2000. [Google Scholar]
- Ministry of Justice. National Health Insurance Reimbursement Regulations. 2014. Available online: http://law.moj.gov.tw/LawClass/LawAllIf.aspx?PCode=L0060006 (accessed on 7 March 2018).
- Chen, H.L.; Lea, Y.P.; Young, S.C.; Wu, C.Y. A summary report of concurrent peer review of inpatient medical records in a medical center. Taiwan J. Public Health 1995, 14, 103–110. [Google Scholar]
- Chiu, M.L.; Cheng, C.F.; Liang, W.M.; Lin, P.T.; Wu, T.N.; Chen, C.Y. The temporal relationship between selected mental disorders and substance-related disorders: A nationwide population-based cohort study. Psychiatry J. 2018, 2018, 5697103. [Google Scholar] [CrossRef] [Green Version]
- Lin, S.L.; Wu, S.L.; Ko, S.Y.; Lu, C.H.; Wang, D.W.; Ben, R.J.; Horng, C.T.; Yang, J.W. Dysthymia increases the risk of temporomandibular disorder: A population-based cohort study (A STROBE-Compliant Article). Medicine 2016, 95, e4271. [Google Scholar] [CrossRef]
- Needham, D.M.; Scales, D.C.; Laupacis, A.; Pronovost, P.J. A systematic review of the Charlson comorbidity index using Canadian administrative databases: A perspective on risk adjustment in critical care research. J. Crit. Care 2005, 20, 12–19. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Hansen, A.; Bi, P.; Nitschke, M.; Ryan, P.; Pisaniello, D.; Tucker, G. The effect of heat waves on mental health in a temperate Australian city. Environ. Health Perspect. 2008, 116, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Cianconi, P.; Betro, S.; Janiri, L. The impact of climate change on mental health: A systematic descriptive review. Front. Psychiatry 2020, 11, 74. [Google Scholar] [CrossRef]
- Tzeng, N.S.; Chung, C.H.; Chang, C.C.; Chang, H.A.; Kao, Y.C.; Chang, S.Y.; Chien, W.C. What could we learn from SARS when facing the mental health issues related to the COVID-19 outbreak? A nationwide cohort study in Taiwan. Transl. Psychiatry 2020, 10, 339. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.J.; Chien, W.C.; Chung, C.H.; Yang, Y.J.; Tzeng, N.S. Association between traumatic spinal cord injury and affective and other psychiatric disorders—A nationwide cohort study and effects of rehabilitation therapies. J. Affect. Disord. 2020, 265, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.S.; Chung, C.H.; Chang, H.A.; Kao, Y.C.; Chu, D.M.; Wang, C.C.; Chen, S.J.; Tzeng, N.S.; Chien, W.C. Association between child abuse exposure and the risk of psychiatric disorders: A nationwide cohort study in Taiwan. Child Abuse Negl. 2020, 101, 104362. [Google Scholar] [CrossRef] [PubMed]
- Yeh, T.C.; Chien, W.C.; Chung, C.H.; Liang, C.S.; Chang, H.A.; Kao, Y.C.; Yeh, H.W.; Yang, Y.J.; Tzeng, N.S. Psychiatric disorders after traumatic brain injury: A nationwide population-based cohort study and the effects of rehabilitation therapies. Arch. Phys. Med. Rehabil. 2020, 101, 822–831. [Google Scholar] [CrossRef]
- Lippmann, S.J.; Fuhrmann, C.M.; Waller, A.E.; Richardson, D.B. Ambient temperature and emergency department visits for heat-related illness in North Carolina, 2007–2008. Environ. Res. 2013, 124, 35–42. [Google Scholar] [CrossRef]
- Sugg, M.M.; Konrad, C.E.; Fuhrmann, C.M. Relationships between maximum temperature and heat-related illness across North Carolina, USA. Int. J. Biometeorol. 2016, 60, 663–675. [Google Scholar] [CrossRef]
- Na, W.; Jang, J.Y.; Lee, K.E.; Kim, H.; Jun, B.; Kwon, J.W.; Jo, S.N. The effects of temperature on heat-related illness according to the characteristics of patients during the summer of 2012 in the Republic of Korea. J. Prev. Med. Public Health 2013, 46, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Pflanz, S. Occupational stress and psychiatric illness in the military: Investigation of the relationship between occupational stress and mental illness among military mental health patients. Mil. Med. 2001, 166, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Saraceno, B.; Barbui, C. Poverty and mental illness. Can. J. Psychiatry 1997, 42, 285–290. [Google Scholar] [CrossRef]
- Sharma, H.S. Methods to produce hyperthermia-induced brain dysfunction. Prog. Brain Res. 2007, 162, 173–199. [Google Scholar]
- VanItallie, T.B. Stress: A risk factor for serious illness. Metabolism 2002, 51 (Suppl. 1), 40–45. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total (n = 34,386) n (%) | With HRI (n = 3126) n (%) | Without HRI (n = 31,260) n (%) | p Value |
|---|---|---|---|---|
| Gender | 0.999 | |||
| Male | 27,687 (80.52) | 2517 (80.52) | 25,170 (80.52) | |
| Female | 6699 (19.48) | 609 (19.48) | 6090 (19.48) | |
| Age (years) | 45.95 ± 17.20 | 45.57 ± 16.68 | 45.99 ± 17.25 | 0.193 |
| Age groups (years) | 0.999 | |||
| 20–49 | 20,548 (59.76) | 1868 (59.76) | 18,680 (59.76) | |
| 50–64 | 6413 (18.65) | 583 (18.65) | 5830 (18.65) | |
| ≥65 | 7425 (21.59) | 675 (21.59) | 6750 (21.59) | |
| Insured premium (TWD) | 0.084 | |||
| <8000 | 33,753 (98.16) | 3065 (98.05) | 30,688 (98.17) | |
| 18,000–34,999 | 456 (1.33) | 51 (1.63) | 405 (1.30) | |
| ≥35,000 | 177 (0.51) | 10 (0.32) | 167 (0.53) | |
| CCI_R | 0.70 ± 1.67 | 0.52 ± 1.42 | 0.71 ± 1.69 | <0.001 |
| CCI_R groups | <0.001 | |||
| 0 | 23,884 (69.46) | 2297 (73.48) | 21,587 (69.06) | |
| 1 | 5475 (15.92) | 494 (15.80) | 4981 (15.93) | |
| 2 | 2026 (5.89) | 177 (5.66) | 1849 (5.91) | |
| 3 | 1534 (4.46) | 87 (2.78) | 1447 (4.63) | |
| ≥4 | 1467 (4.27) | 71 (2.27) | 1396 (4.47) | |
| Season | 0.999 | |||
| Spring (March–May) | 5412 (15.74) | 492 (15.74) | 4920 (15.74) | |
| Summer (June–August) | 21,758 (63.28) | 1978 (63.28) | 19,780 (63.28) | |
| Autumn (September–November) | 5159 (15.00) | 469 (15.00) | 4690 (15.00) | |
| Winter (December–February) | 2057 (5.98) | 187 (5.98) | 1870 (5.98) | |
| Location | <0.001 | |||
| Northern Taiwan | 13,045 (37.94) | 692 (22.14) | 12,353 (39.52) | |
| Middle Taiwan | 9919 (28.85) | 1175 (37.59) | 8744 (27.97) | |
| Southern Taiwan | 8915 (25.93) | 773 (24.73) | 8142 (26.05) | |
| Eastern Taiwan | 2319 (6.74) | 443 (14.17) | 1876 (6.00) | |
| Outlets islands | 188 (0.55) | 43 (1.38) | 145 (0.46) | |
| Urbanization level | <0.001 | |||
| 1 (The highest) | 11,149 (32.42) | 481 (15.39) | 10,668 (34.13) | |
| 2 | 14,205 (41.31) | 1361 (43.54) | 12,844 (41.09) | |
| 3 | 3111 (9.05) | 413 (13.21) | 2698 (8.63) | |
| 4 (The lowest) | 5921 (17.22) | 871 (27.86) | 5050 (16.15) | |
| Level of care | <0.001 | |||
| Hospital center | 9978 (29.02) | 394 (12.60) | 9584 (30.66) | |
| Regional hospital | 10,668 (31.02) | 1274 (40.75) | 9394 (30.05) | |
| Local hospital | 13,740 (39.96) | 1458 (46.64) | 12,282 (39.29) |
| Variables | No Competing Risk in the Model | Competing Risk in the Model | ||||
|---|---|---|---|---|---|---|
| Adjusted HR | 95% CI | p Value | Adjusted HR | 95% CI | p Value | |
| HRI | ||||||
| Without | Reference | Reference | ||||
| With | 3.748 | 3.412–4.117 | <0.001 | 3.849 | 3.522–4.206 | <0.001 |
| Gender | ||||||
| Male | 1.101 | 1.017–1.192 | 0.017 | 1.128 | 1.043–1.221 | 0.003 |
| Female | Reference | Reference | ||||
| Age groups (years) | ||||||
| 20–49 | Reference | |||||
| 50–64 | 1.506 | 1.465–1.551 | <0.001 | 1.517 | 1.475–1.563 | <0.001 |
| ≥65 | 1.649 | 1.602–1.701 | <0.001 | 1.733 | 1.680–1.791 | <0.001 |
| Insured premium (TWD) | ||||||
| <18,000 | Reference | Reference | ||||
| 18,000–34,999 | 0.827 | 0.641–1.067 | 0.145 | 0.799 | 0.619–1.031 | 0.085 |
| ≥35,000 | 0.212 | 0.079–0.565 | 0.002 | 0.209 | 0.078–0.556 | 0.002 |
| CCI_R groups | ||||||
| 0 | Reference | Reference | ||||
| 1 | 1.474 | 1.365–1.593 | <0.001 | 1.520 | 1.407–1.642 | <0.001 |
| 2 | 1.633 | 1.474–1.808 | <0.001 | 1.756 | 1.585–1.945 | <0.001 |
| 3 | 1.223 | 1.069–1.399 | 0.003 | 1.391 | 1.216–1.592 | <0.001 |
| ≥4 | 1.002 | 0.889–1.130 | 0.973 | 1.331 | 1.180–1.503 | <0.001 |
| Season | ||||||
| Spring (March–May) | Reference | Reference | ||||
| Summer (June–August) | 0.998 | 0.816–1.088 | 0.970 | 0.998 | 0.916–1.087 | 0.959 |
| Autumn (September–November) | 0.873 | 0.800–0.952 | 0.002 | 0.865 | 0.793–0.944 | 0.001 |
| Winter (December–February) | 0.976 | 0.894–1.065 | 0.584 | 0.982 | 0.899–1.071 | 0.679 |
| Urbanization level | ||||||
| 1 (The highest) | 1.221 | 1.107–1.347 | <0.001 | 1.179 | 1.069–1.301 | <0.001 |
| 2 | 1.036 | 0.914–1.184 | 0.903 | 1.023 | 0.903–1.160 | 0.721 |
| 3 | 1.005 | 0.929–1.097 | 0.704 | 1.004 | 0.927–1.088 | 0.923 |
| 4 (The lowest) | Reference | Reference | ||||
| Level of care | ||||||
| Hospital center | 1.713 | 1.557–1.885 | <0.001 | 1.752 | 1.592–1.929 | <0.001 |
| Regional hospital | 1.222 | 1.124–1.329 | <0.001 | 1.225 | 1.126–1.332 | <0.001 |
| Local hospital | Reference | Reference | <0.001 | |||
| Stratified Variables | With HRI | Without HRI (Reference) | Competing Risk in the Model | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Events | PYs | Rate (Per 105 PYs) | Events | PYs | Rate (Per 105 PYs) | Adjusted sHR | 95% CI | p Value | |
| Total | 523 | 29,478.47 | 1774.18 | 3619 | 303,153.95 | 1193.78 | 3.849 | 3.522–4.206 | <0.001 |
| Gender | |||||||||
| Male | 398 | 21,718.98 | 1832.50 | 2845 | 240,747.97 | 1181.73 | 4.016 | 3.675–4.389 | <0.001 |
| Female | 125 | 7759.48 | 1610.93 | 774 | 62,405.99 | 1240.27 | 3.364 | 3.078–3.676 | <0.001 |
| Age groups (years) | |||||||||
| 20–49 | 205 | 10,686.70 | 1918.27 | 1457 | 93,914.94 | 1551.40 | 3.202 | 2.930–3.499 | <0.001 |
| 50–64 | 117 | 6407.14 | 1826.09 | 1046 | 89,618.76 | 1167.17 | 4.052 | 3.708–4.428 | <0.001 |
| ≥65 | 201 | 12,384.63 | 1622.98 | 1116 | 119,620.24 | 932.95 | 4.505 | 4.123–4.923 | <0.001 |
| Insured premium (TWD) | |||||||||
| <18,000 | 517 | 28,817.05 | 1794.08 | 3568 | 296,634.58 | 1202.83 | 3.863 | 3.535–4.221 | <0.001 |
| 18,000–34,999 | 6 | 627.18 | 956.66 | 48 | 4950.82 | 969.54 | 2.555 | 2.338–2.792 | <0.001 |
| ≥35,000 | 0 | 34.24 | 0.00 | 3 | 1568.56 | 191.26 | - | - | 0.995 |
| CCI_R groups | |||||||||
| 0 | 190 | 15,559.82 | 1221.09 | 1660 | 153,252.94 | 1083.18 | 2.920 | 2.672–3.190 | <0.001 |
| 1 | 158 | 6051.41 | 2610.96 | 997 | 66,703.94 | 1494.66 | 4.524 | 4.140–4.944 | <0.001 |
| 2 | 101 | 2920.17 | 3458.70 | 457 | 29,081.72 | 1571.43 | 5.700 | 5.216–6.229 | <0.001 |
| 3 | 25 | 1679.63 | 1488.42 | 186 | 20,875.25 | 891.01 | 4.326 | 3.959–4.728 | <0.001 |
| ≥4 | 49 | 3267.44 | 1499.65 | 319 | 33,240.11 | 959.68 | 4.047 | 3.703–4.422 | <0.001 |
| Season | |||||||||
| Spring (March–May) | 155 | 6795.83 | 2280.81 | 901 | 72,017.75 | 1251.08 | 4.722 | 4.320–5.159 | <0.001 |
| Summer (June–August) | 142 | 6900.78 | 2057.74 | 931 | 77,668.50 | 1198.68 | 4.446 | 4.068–4.858 | <0.001 |
| Autumn (September–November) | 103 | 8563.55 | 1202.77 | 907 | 81,760.81 | 1109.33 | 2.808 | 2.569–3.068 | <0.001 |
| Winter (December–February) | 123 | 7218.31 | 1704.00 | 880 | 71,706.88 | 1227.22 | 3.596 | 3.291–3.930 | <0.001 |
| Urbanization level | |||||||||
| 1 (The highest) | 112 | 6610.42 | 1694.30 | 924 | 91,033.70 | 1015.01 | 4.323 | 3.956–4.724 | <0.001 |
| 2 | 222 | 14,550.52 | 1525.72 | 1329 | 134,057.66 | 991.36 | 3.986 | 3.647–4.356 | <0.001 |
| 3 | 50 | 2772.35 | 1803.53 | 331 | 24,698.28 | 1340.17 | 3.485 | 3.189–3.809 | <0.001 |
| 4 (The lowest) | 139 | 5545.18 | 2506.68 | 1035 | 53,364.31 | 1939.50 | 3.347 | 3.063–3.658 | <0.001 |
| Level of care | |||||||||
| Hospital center | 102 | 7590.10 | 1343.86 | 894 | 101,204.83 | 883.36 | 3.940 | 3.605–4.305 | <0.001 |
| Regional hospital | 238 | 14,836.84 | 1604.12 | 1511 | 138,305.48 | 1092.51 | 3.803 | 3.480–4.155 | <0.001 |
| Local hospital | 183 | 7051.53 | 2595.18 | 1214 | 63,643.64 | 1907.50 | 3.524 | 3.224–3.850 | <0.001 |
| Sensitivity Test | Psychiatric Disorders Subgroup | With HRI | Without HRI (Reference) | Competing Risk in the Model | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Events | PYs | Rate (Per 105 PYs) | Events | PYs | Rate (Per 105 PYs) | Adjusted sHR | 95% CI | p Value | ||
| Overall | Overall | 523 | 29,478.47 | 1774.18 | 3619 | 303,153.95 | 1193.78 | 3.849 | 3.522–4.206 | <0.001 |
| Dementia | 87 | 29,478.47 | 295.13 | 729 | 303,153.95 | 240.47 | 3.179 | 2.908–3.473 | <0.001 | |
| Anxiety | 81 | 29,478.47 | 274.78 | 498 | 303,153.95 | 164.27 | 4.332 | 3.964–4.734 | <0.001 | |
| Depression | 88 | 29,478.47 | 298.52 | 535 | 303,153.95 | 176.48 | 4.381 | 4.009–4.787 | <0.001 | |
| Bipolar | 16 | 29,478.47 | 54.28 | 78 | 303,153.95 | 25.73 | 5.463 | 4.999–5.970 | <0.001 | |
| Sleep disorders | 114 | 29,478.47 | 386.72 | 806 | 303,153.95 | 265.87 | 3.767 | 3.447–4.116 | <0.001 | |
| PTSD/ASD | 8 | 29,478.47 | 27.14 | 10 | 303,153.95 | 3.30 | 21.307 | 19.497–23.283 | <0.001 | |
| Psychotic disorders | 57 | 29,478.47 | 193.36 | 419 | 303,153.95 | 138.21 | 3.623 | 3.315–3.959 | <0.001 | |
| Schizophrenia | 35 | 29,478.47 | 118.73 | 234 | 303,153.95 | 77.19 | 3.984 | 3.645–4.353 | <0.001 | |
| Schizophreniform | 3 | 29,478.47 | 10.18 | 3 | 303,153.95 | 0.99 | 26.634 | 24.371–29.104 | <0.001 | |
| Other psychotic disorders | 17 | 29,478.47 | 57.67 | 122 | 303,153.95 | 40.24 | 3.711 | 3.396–4.056 | <0.001 | |
| SRD | 143 | 29,478.47 | 485.10 | 904 | 303,153.95 | 298.20 | 4.213 | 3.855–4.604 | <0.001 | |
| AUD | 123 | 29,478.47 | 417.25 | 818 | 303,153.95 | 269.83 | 4.005 | 3.665–4.376 | <0.001 | |
| IDUD | 22 | 29,478.47 | 74.63 | 97 | 303,153.95 | 32.00 | 6.041 | 5.527–6.601 | <0.001 | |
| In the first 1 years excluded | Overall | 303 | 25,760.55 | 1176.22 | 3270 | 301,005.38 | 1086.36 | 2.804 | 2.566–3.064 | <0.001 |
| Dementia | 62 | 25,760.55 | 240.68 | 697 | 301,005.38 | 231.56 | 2.692 | 2.463–2.942 | <0.001 | |
| Anxiety | 43 | 25,760.55 | 166.92 | 456 | 301,005.38 | 151.49 | 2.854 | 2.611–3.118 | <0.001 | |
| Depression | 44 | 25,760.55 | 170.80 | 495 | 301,005.38 | 164.45 | 2.690 | 2.461–2.939 | <0.001 | |
| Bipolar | 8 | 25,760.55 | 31.06 | 69 | 301,005.38 | 22.92 | 3.509 | 3.211–3.834 | <0.001 | |
| Sleep disorders | 55 | 25,760.55 | 213.50 | 765 | 301,005.38 | 254.15 | 2.176 | 1.991–2.377 | <0.001 | |
| PTSD/ASD | 2 | 25,760.55 | 7.76 | 9 | 301,005.38 | 2.99 | 6.725 | 6.154–7.349 | <0.001 | |
| Psychotic disorders | 31 | 25,760.55 | 120.34 | 325 | 301,005.38 | 107.97 | 2.887 | 2.641–3.154 | <0.001 | |
| Schizophrenia | 20 | 25,760.55 | 77.64 | 218 | 301,005.38 | 72.42 | 2.776 | 2.540–3.034 | <0.001 | |
| Schizophreniform | 1 | 25,760.55 | 3.88 | 3 | 301,005.38 | 1.00 | 10.087 | 9.230–11.023 | <0.001 | |
| Other psychotic disorders | 8 | 25,760.55 | 31.06 | 106 | 301,005.38 | 35.22 | 2.284 | 2.090–2.496 | <0.001 | |
| SRD | 96 | 25,760.55 | 372.66 | 781 | 301,005.38 | 259.46 | 3.720 | 3.404–4.065 | <0.001 | |
| AUD | 81 | 25,760.55 | 314.43 | 706 | 301,005.38 | 234.55 | 3.472 | 3.177–3.794 | <0.001 | |
| IDUD | 17 | 25,760.55 | 65.99 | 85 | 301,005.38 | 28.24 | 6.052 | 5.538–6.614 | <0.001 | |
| In the first 5 years excluded | Overall | 113 | 11,982.97 | 943.00 | 2052 | 271,841.51 | 754.85 | 3.235 | 2.961–3.535 | <0.001 |
| Dementia | 19 | 11,982.97 | 158.56 | 507 | 271,841.51 | 186.51 | 2.202 | 2.015–2.406 | <0.001 | |
| Anxiety | 17 | 11,982.97 | 141.87 | 250 | 271,841.51 | 91.97 | 3.995 | 3.656–4.366 | <0.001 | |
| Depression | 16 | 11,982.97 | 133.52 | 321 | 271,841.51 | 118.08 | 2.928 | 2.680–3.200 | <0.001 | |
| Bipolar | 2 | 11,982.97 | 16.69 | 44 | 271,841.51 | 16.19 | 2.671 | 2.444–2.918 | <0.001 | |
| Sleep disorders | 27 | 11,982.97 | 225.32 | 503 | 271,841.51 | 185.03 | 3.154 | 2.886–3.446 | <0.001 | |
| PTSD/ASD | 0 | 11,982.97 | 0.00 | 8 | 271,841.51 | 2.94 | 0.000 | - | 0.993 | |
| Psychotic disorders | 7 | 11,982.97 | 58.42 | 198 | 271,841.51 | 72.84 | 2.077 | 1.901–2.270 | <0.001 | |
| Schizophrenia | 4 | 11,982.97 | 33.38 | 142 | 271,841.51 | 52.24 | 1.655 | 1.514–1.809 | <0.001 | |
| Schizophreniform | 0 | 11,982.97 | 0.00 | 2 | 271,841.51 | 0.74 | 0.000 | - | 0.995 | |
| Other psychotic disorders | 2 | 11,982.97 | 16.69 | 56 | 271,841.51 | 20.60 | 2.098 | 1.920–2.293 | <0.001 | |
| SRD | 38 | 11,982.97 | 317.12 | 423 | 271,841.51 | 155.61 | 5.278 | 4.830–5.768 | <0.001 | |
| AUD | 31 | 11,982.97 | 258.70 | 373 | 271,841.51 | 137.21 | 4.883 | 4.468–5.336 | <0.001 | |
| IDUD | 8 | 11,982.97 | 66.76 | 56 | 271,841.51 | 20.60 | 8.393 | 7.680–9.172 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, F.-L.; Chien, W.-C.; Chung, C.-H.; Lai, C.-Y.; Tzeng, N.-S. Real-World Evidence for the Association between Heat-Related Illness and the Risk of Psychiatric Disorders in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 8087. https://doi.org/10.3390/ijerph19138087
Li F-L, Chien W-C, Chung C-H, Lai C-Y, Tzeng N-S. Real-World Evidence for the Association between Heat-Related Illness and the Risk of Psychiatric Disorders in Taiwan. International Journal of Environmental Research and Public Health. 2022; 19(13):8087. https://doi.org/10.3390/ijerph19138087
Chicago/Turabian StyleLi, Fang-Ling, Wu-Chien Chien, Chi-Hsiang Chung, Chung-Yu Lai, and Nian-Sheng Tzeng. 2022. "Real-World Evidence for the Association between Heat-Related Illness and the Risk of Psychiatric Disorders in Taiwan" International Journal of Environmental Research and Public Health 19, no. 13: 8087. https://doi.org/10.3390/ijerph19138087
APA StyleLi, F.-L., Chien, W.-C., Chung, C.-H., Lai, C.-Y., & Tzeng, N.-S. (2022). Real-World Evidence for the Association between Heat-Related Illness and the Risk of Psychiatric Disorders in Taiwan. International Journal of Environmental Research and Public Health, 19(13), 8087. https://doi.org/10.3390/ijerph19138087