
Polycythemia-Related Proliferative Ischemic Retinopathy Managed with Smoking Cessation: A Case Report


Abstract
:1. Introduction
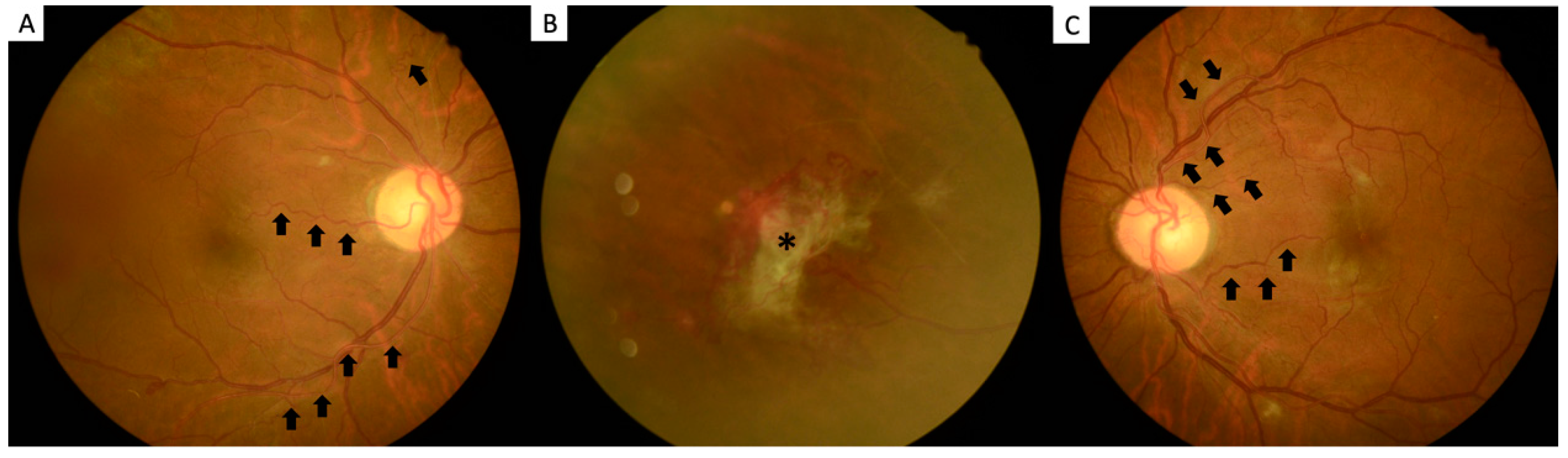
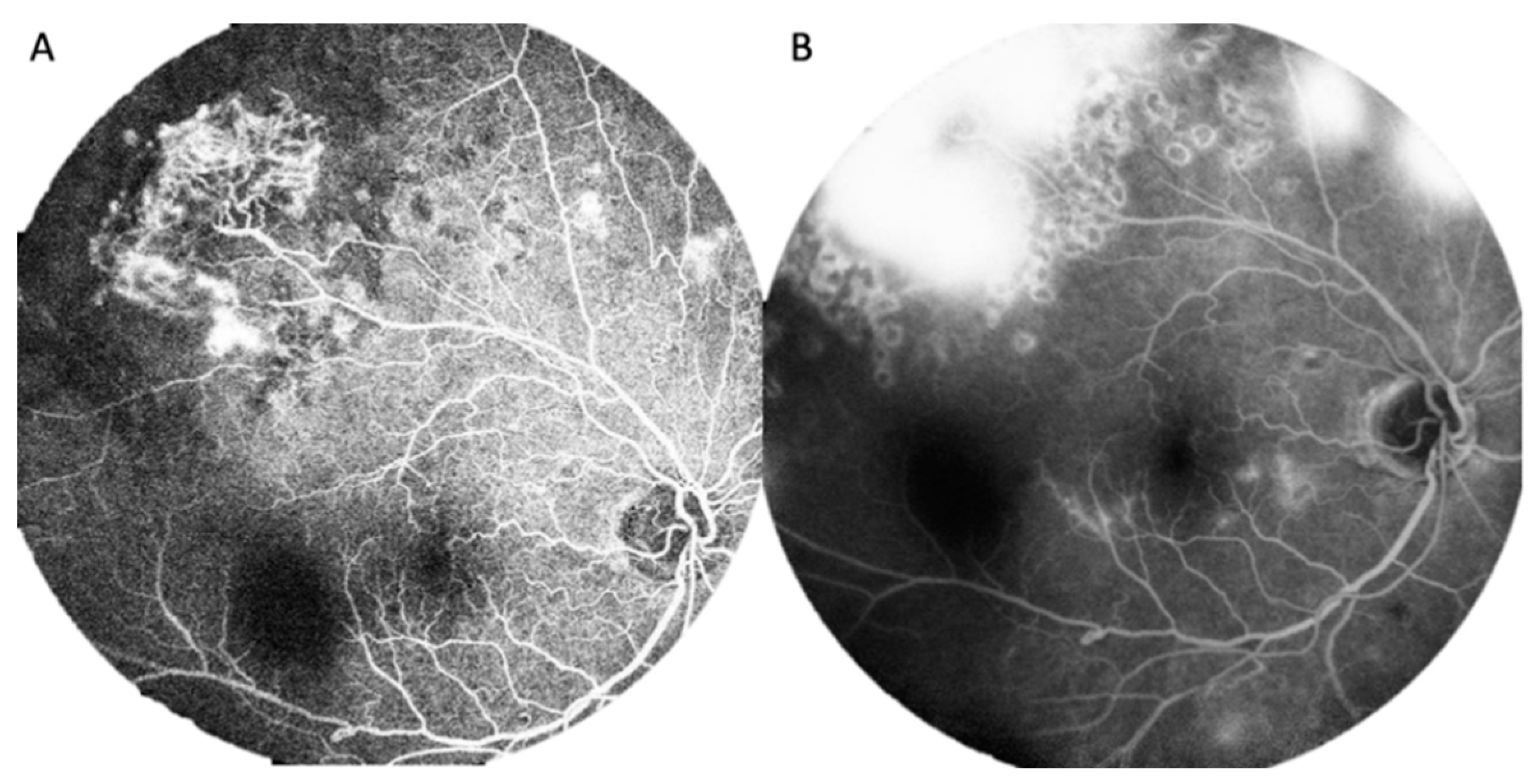
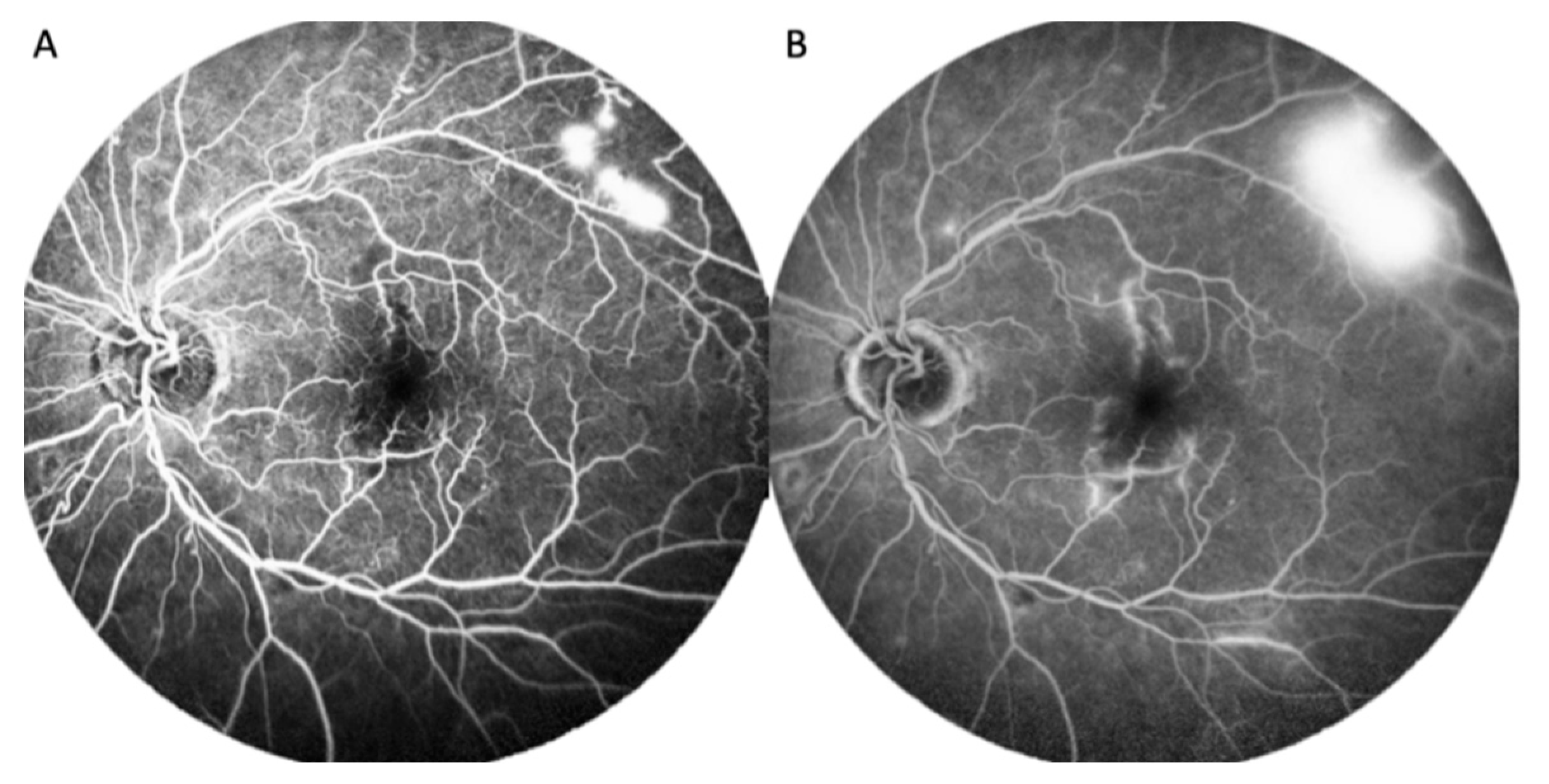
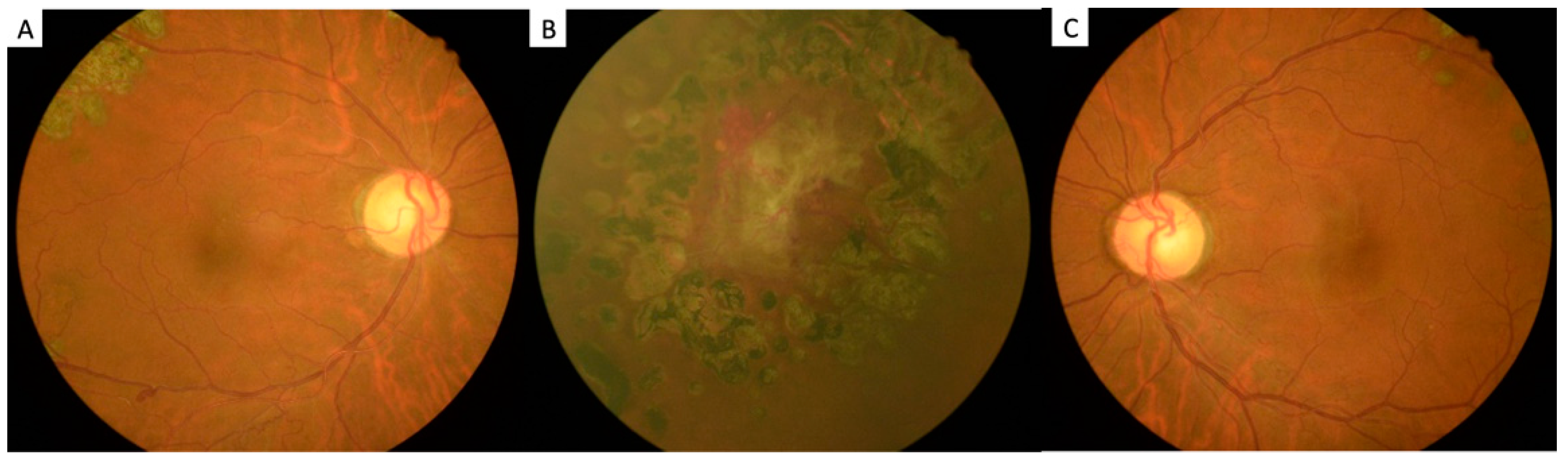
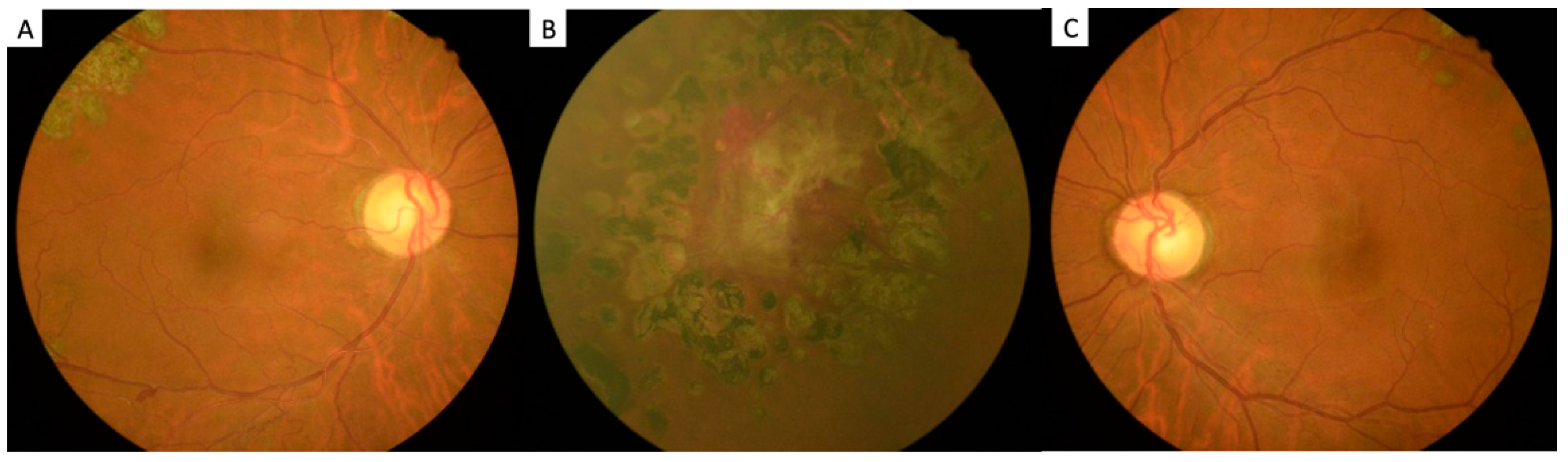
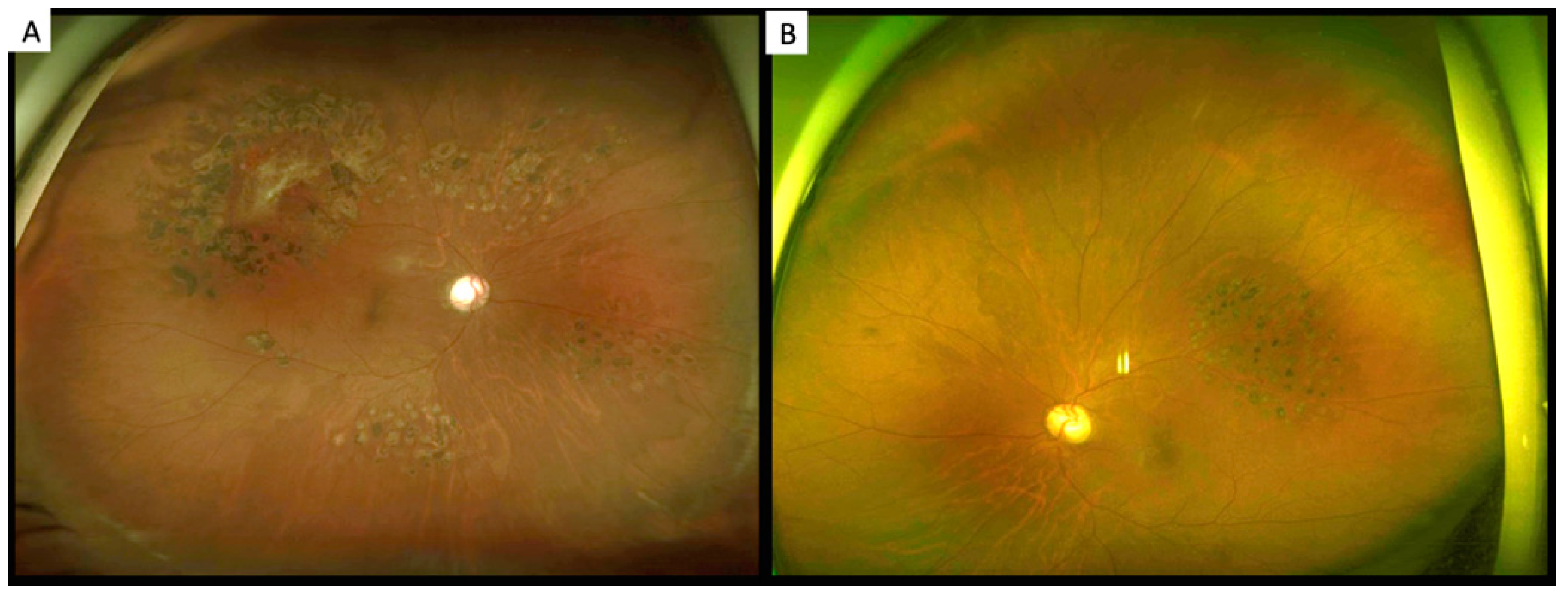
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Current Cigarette Smoking among Adults in the United States; CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- Xu, X.; Shrestha, S.S.; Trivers, K.F.; Neff, L.; Armour, B.S.; King, B.A. U.S. healthcare spending attributable to cigarette smoking in 2014. Prev. Med. 2021, 150, 106529. [Google Scholar] [CrossRef] [PubMed]
- Office of the Surgeon General; Office on Smoking and Health. Reports of the Surgeon General. In The Health Consequences of Smoking: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2004. [Google Scholar]
- Hocking, W.G.; Golde, D.W. Polycythemia: Evaluation and management. Blood Rev. 1989, 3, 59–65. [Google Scholar] [CrossRef]
- Blood, A.M.; Lowenthal, E.A.; Nowakowski, R.W. Retinopathy secondary to anemia from myeloid metaplasia in polycythemia vera. J. Am. Optom. Assoc. 1997, 68, 734–738. [Google Scholar] [PubMed]
- Tefferi, A.; Barbui, T. Polycythemia vera and essential thrombocythemia: 2021 update on diagnosis, risk-stratification and management. Am. J. Hematol. 2020, 95, 1599–1613. [Google Scholar] [CrossRef]
- Mithoowani, S.; Laureano, M.; Crowther, M.A.; Hillis, C.M. Investigation and management of erythrocytosis. CMAJ 2020, 192, E913–E918. [Google Scholar] [CrossRef]
- Mossuz, P.; Girodon, F.; Donnard, M.; Latger-Cannard, V.; Dobo, I.; Boiret, N.; Lecron, J.C.; Binquet, C.; Barro, C.; Hermouet, S.; et al. Diagnostic value of serum erythropoietin level in patients with absolute erythrocytosis. Haematologica 2004, 89, 1194–1198. [Google Scholar]
- Fricker, M.; Goggins, B.J.; Mateer, S.; Jones, B.; Kim, R.Y.; Gellatly, S.L.; Jarnicki, A.G.; Powell, N.; Oliver, B.G.; Radford-Smith, G.; et al. Chronic cigarette smoke exposure induces systemic hypoxia that drives intestinal dysfunction. JCI Insight 2018, 3, 94040. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.A.; Goodson, W.H.; Hopf, H.W.; Hunt, T.K. Cigarette smoking decreases tissue oxygen. Arch. Surg. 1991, 126, 1131–1134. [Google Scholar] [CrossRef]
- Alkhedaide, A.Q. Tobacco smoking causes secondary polycythemia and a mild leukocytosis among heavy smokers in Taif City in Saudi Arabia. Saudi J. Biol. Sci. 2020, 27, 407–411. [Google Scholar] [CrossRef]
- Moodley, T.; Mannaru, K.T.; Hugo, A.; Lines, J.A.; Van der Merwe, J.M.; Ramparsad, N.; Holland, N.S. Secondary polycythaemia with elevated carbon monoxide levels due to hookah pipe smoking: A public health concern. S. Afr. Med. J. 2021, 111, 938–941. [Google Scholar] [CrossRef]
- Malenica, M.; Prnjavorac, B.; Bego, T.; Dujic, T.; Semiz, S.; Skrbo, S.; Gusic, A.; Hadzic, A.; Causevic, A. Effect of Cigarette Smoking on Haematological Parameters in Healthy Population. Med. Arch. 2017, 71, 132–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlQahtany, F.S.; Algahtani, F.H.; Alshebly, M.M.; Madkhaly, F.M.; Ghandour, M.K.; Almalki, J.H.; AlOtaibi, W.S.; Salim, A.; Mendoza, F.C. Association between cigarette & shisha smoking and the severity of polycythemia: A cross sectional study. Saudi J. Biol. Sci. 2020, 27, 460–464. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, K.M.; Çolak, Y.; Ellervik, C.; Hasselbalch, H.C.; Bojesen, S.E.; Nordestgaard, B.G. Smoking and Increased White and Red Blood Cells. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 965–977. [Google Scholar] [CrossRef] [PubMed]
- Kondo, T.; Nakano, Y.; Adachi, S.; Murohara, T. Effects of Tobacco Smoking on Cardiovascular Disease. Circ. J. 2019, 83, 1980–1985. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, V.R. Secondary polycythemia and the risk of venous thromboembolism. J. Clin. Med. Res. 2014, 6, 395–397. [Google Scholar] [CrossRef] [Green Version]
- Schwarcz, T.H.; Hogan, L.A.; Endean, E.D.; Roitman, I.T.; Kazmers, A.; Hyde, G.L. Thromboembolic complications of polycythemia: Polycythemia vera versus smokers’ polycythemia. J. Vasc. Surg. 1993, 17, 518–522; discussion 522–523. [Google Scholar] [CrossRef] [Green Version]
- Nadeem, O.; Gui, J.; Ornstein, D.L. Prevalence of venous thromboembolism in patients with secondary polycythemia. Clin. Appl. Thromb. Hemost. 2013, 19, 363–366. [Google Scholar] [CrossRef]
- Yang, H.S.; Joe, S.G.; Kim, J.G.; Park, S.H.; Ko, H.S. Delayed choroidal and retinal blood flow in polycythaemia vera patients with transient ocular blindness: A preliminary study with fluorescein angiography. Br. J. Haematol. 2013, 161, 745–747. [Google Scholar] [CrossRef]
- Tönz, M.S.; Rigamonti, V.; Iliev, M.E. Simultaneous, bilateral anterior ischemic optic neuropathy (AION) in polycythemia vera: A case report. Klin. Mon. Augenheilkd. 2008, 225, 504–506. [Google Scholar] [CrossRef]
- Rao, K.; Shenoy, S.B.; Kamath, Y.; Kapoor, S. Central retinal artery occlusion as a presenting manifestation of polycythaemia vera. BMJ Case Rep. 2016, 2016, bcr2016216417. [Google Scholar] [CrossRef]
- Ganesan, S.; Raman, R.; Sharma, T. Polycythemia causing posterior segment vascular occlusions. Oman J. Ophthalmol. 2017, 10, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Ahn, B.Y.; Choi, K.D.; Choi, Y.J.; Jea, S.Y.; Lee, J.E. Isolated monocular visual loss as an initial manifestation of polycythemia vera. J. Neurol. Sci. 2007, 258, 151–153. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R. Peripheral retinal neovascularization associated with polycythemia rubra vera. Jpn. J. Ophthalmol. 2009, 53, 188–189. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tobacco: Health Benefits of Smoking Cessation Q&A; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Gallucci, G.; Tartarone, A.; Lerose, R.; Lalinga, A.V.; Capobianco, A.M. Cardiovascular risk of smoking and benefits of smoking cessation. J. Thorac. Dis. 2020, 12, 3866–3876. [Google Scholar] [CrossRef]
- Bain, B.J.; Rothwell, M.; Feher, M.D.; Robinson, R.; Brown, J.; Sever, P.S. Acute changes in haematological parameters on cessation of smoking. J. R. Soc. Med. 1992, 85, 80–82. [Google Scholar] [PubMed]
- Van Tiel, E.; Peeters, P.H.; Smit, H.A.; Nagelkerke, N.J.; Van Loon, A.J.; Grobbee, D.E.; Bueno-de-Mesquita, H.B. Quitting smoking may restore hematological characteristics within five years. Ann. Epidemiol. 2002, 12, 378–388. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Data | At Diagnosis | After Recovery |
|---|---|---|
| WBC (/μL) | 8500 | 10,520 |
| RBC (×106/μL) | 5.73 | 5.16 |
| Platelet (×103/μL) | 201 | 179 |
| Hb (g/dL) | 17.7 | 16.2 |
| Hct (%) | 51.6 | 47.6 |
| MCV (fL) | 90.1 | 96.3 |
| RDW (%) | 13.3 | 13.3 |
| ESR (mm/h) | 25 | 15 |
| HbA (%) | 5.0 | 5.5 |
| CHOL(T) (mg/dL) | 239 | 221 |
| TG (mg/dL) | 101 | |
| HDL (mg/dL) | 62.1 | 51 |
| LDL (mg/dL) | 141.7 | 126.7 |
| PT (second) | 9.7 | |
| aPTT (second) | 31.3 | |
| lupus anticoagulant | negative | |
| Anti-cardiolipin antibody | negative | |
| Anti-β2 glycoprotein-I antibody | negative | |
| ANA | negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, S.-Y.; Chang, Y.-C.; Wu, H.-J.; Lai, H.-C. Polycythemia-Related Proliferative Ischemic Retinopathy Managed with Smoking Cessation: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 8072. https://doi.org/10.3390/ijerph19138072
Sung S-Y, Chang Y-C, Wu H-J, Lai H-C. Polycythemia-Related Proliferative Ischemic Retinopathy Managed with Smoking Cessation: A Case Report. International Journal of Environmental Research and Public Health. 2022; 19(13):8072. https://doi.org/10.3390/ijerph19138072
Chicago/Turabian StyleSung, Shao-Yu, Yo-Chen Chang, Horng-Jiun Wu, and Hung-Chi Lai. 2022. "Polycythemia-Related Proliferative Ischemic Retinopathy Managed with Smoking Cessation: A Case Report" International Journal of Environmental Research and Public Health 19, no. 13: 8072. https://doi.org/10.3390/ijerph19138072
APA StyleSung, S.-Y., Chang, Y.-C., Wu, H.-J., & Lai, H.-C. (2022). Polycythemia-Related Proliferative Ischemic Retinopathy Managed with Smoking Cessation: A Case Report. International Journal of Environmental Research and Public Health, 19(13), 8072. https://doi.org/10.3390/ijerph19138072