
Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Index COVID-19 Cases
2.4. Participant Household Contacts and Data Collection
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 18 May 2022).
- World Health Organization. Weekly Epidemiological Update on COVID-19—25 January 2022, Edition 76. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---25-january-2022 (accessed on 18 May 2022).
- World Health Organization. Weekly Epidemiological Update on COVID-19—8 March 2022, Edition 82. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---8-march-2022 (accessed on 18 May 2022).
- Ministry of Health, Labor and Welfare, Japan. Visualizing the Data: Information on COVID-19 Infections. Available online: https://covid19.mhlw.go.jp/en/ (accessed on 21 June 2022).
- COVID-19 Advisory Board of the Ministry of Health, Labor and Welfare, Japan. Current Situation of Infection and Others. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00333.html (accessed on 21 June 2022). (In Japanese)
- Ministry of Health, Labor and Welfare, Japan. Situation of Domestic Occurrence of Omicron Variant. Available online: https://www.mhlw.go.jp/stf/newpage_23133.html (accessed on 21 June 2022). (In Japanese)
- Madewell, Z.J.; Yang, Y.; Longini, I.M.; Halloran, M.E.; Dean, N.E. Household transmission of SARS-CoV-2: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2031756. [Google Scholar] [CrossRef]
- Jørgensen, S.B.; Nygård, K.; Kacelnik, O.; Telle, K. Secondary attack rates for Omicron and Delta variants of SARS-CoV-2 in Norwegian households. JAMA 2022, 327, 1610–1611. [Google Scholar] [CrossRef]
- Del Águila-Mejía, J.; Wallmann, R.; Calvo-Montes, J.; Rodríguez-Lozano, J.; Valle-Madrazo, T.; Aginagalde-Llorente, A. Secondary attack rate, transmission and incubation periods, and serial interval of SARS-CoV-2 Omicron variant, Spain. Emerg. Infect. Dis. 2022, 28, 1224. [Google Scholar] [CrossRef]
- Baker, J.M.; Nakayama, J.Y.; O’Hegarty, M.; McGowan, A.; Teran, R.A.; Bart, S.M.; Mosack, K.; Roberts, N.; Campos, B.; Paegle, A.; et al. SARS-CoV-2 B.1.1.529 (Omicron) variant transmission within households—Four U.S. jurisdictions, November 2021–February 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 341–346. [Google Scholar] [CrossRef]
- Song, J.S.; Lee, J.; Kim, M.; Jeong, H.S.; Kim, M.S.; Kim, S.G.; Yoo, H.N.; Lee, J.J.; Lee, H.Y.; Lee, S.E.; et al. Serial intervals and household transmission of SARS-CoV-2 Omicron variant, South Korea, 2021. Emerg. Infect. Dis. 2022, 28, 756–759. [Google Scholar] [CrossRef]
- Madewell, Z.J.; Yang, Y.; Longini, I.M.J.; Halloran, M.E.; Dean, N.E. Household Secondary Attack Rates of SARS-CoV-2 by Variant and Vaccination Status: An Updated Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e229317. [Google Scholar] [CrossRef]
- Liu, Y.; Rocklöv, J. The effective reproduction number for the omicron SARS-CoV-2 variant of concern is several times higher than Delta. J. Travel Med. 2022, 29, taac037. [Google Scholar] [CrossRef]
- Nishiura, H.; Ito, K.; Anzai, A.; Kobayashi, T.; Piantham, C.; Rodríguez-Morales, A.J. Relative reproduction number of SARS-CoV-2 Omicron (B.1.1.529) compared with Delta variant in South Africa. J. Clin. Med. 2021, 11, 30. [Google Scholar] [CrossRef]
- Ito, K.; Piantham, C.; Nishiura, H. Relative instantaneous reproduction number of Omicron SARS-CoV-2 variant with respect to the Delta variant in Denmark. J. Med. Virol. 2022, 94, 2265–2268. [Google Scholar] [CrossRef]
- Madewell, Z.J.; Yang, Y.; Longini, I.M.; Halloran, M.E.; Dean, N.E. Factors associated with household transmission of SARS-CoV-2: An updated systematic review and meta-analysis. JAMA Netw. Open 2021, 4, e2122240. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Tseng, H.F.; Ackerson, B.K.; Luo, Y.; Sy, L.S.; Talarico, C.A.; Tian, Y.; Bruxvoort, K.J.; Tubert, J.E.; Florea, A.; Ku, J.H.; et al. Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. Nat. Med. 2022, 28, 1063–1071. [Google Scholar] [CrossRef]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association between 3 doses of mRNA COVID-19 vaccine and symptomatic infection caused by the SARS-CoV-2 Omicron and Delta variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases, Infectious Disease Epidemiology Center. Manual Conducting for Active Epidemiological Surveillance of Patients with Novel Coronavirus Infection (Provisional Version on May 29). May 2020. Available online: https://www.niid.go.jp/niid/ja/diseases/ka/corona-virus/2019-ncov/2484-idsc/9357-2019-ncov-02.html (accessed on 21 June 2022). (In Japanese)
- Ogata, T.; Irie, F.; Ogawa, E.; Ujiie, S.; Seki, A.; Wada, K.; Tanaka, H. Secondary Attack Rate among Non-Spousal Household Contacts of Coronavirus Disease 2019 in Tsuchiura, Japan, August 2020–February 2021. Int. J. Environ. Res. Public Health 2021, 18, 8921. [Google Scholar] [CrossRef]
- Ogata, T.; Tanaka, H.; Nozawa, Y.; Mukouyama, K.; Tanaka, E.; Osaki, N.; Noguchi, E.; Seo, K.; Wada, K. Increased Secondary Attack Rate among Unvaccinated Household Contacts of Coronavirus Disease 2019 Patients with Delta Variant in Japan. Int. J. Environ. Res. Public Health 2022, 19, 3889. [Google Scholar] [CrossRef]
- Institute of Health of Ibaraki Prefectural Government. Situation of Tests on Variant Virus of SARS-CoV-2. Available online: https://www.pref.ibaraki.jp/hokenfukushi/eiken/kikaku/covid-19_ibarakieiken_kensa.html (accessed on 21 June 2022). (In Japanese)
- Prime Minister’s Office of Japan. Total Number of Vaccination and Supply of Vaccine So Far. Available online: https://www.kantei.go.jp/jp/content/kenbetsu-vaccination_data2.pdf (accessed on 18 May 2022). (In Japanese)
- Ibaraki Prefectural Government. Vaccination Status. Available online: https://ibaraki.stopcovid19.jp/cards/vaccination-2nd/ (accessed on 21 June 2022). (In Japanese)
- Allen, H.; Vusirikala, A.; Flannagan, J.; Twohig, K.A.; Zaidi, A.; Chudasama, D.; Lamagni, T.; Groves, N.; Turner, C.; Rawlinson, C.; et al. Household transmission of COVID-19 cases associated with SARS-CoV-2 delta variant (B.1.617.2): National case-control study. Lancet Reg. Health Eur. 2022, 12, 100252. [Google Scholar] [CrossRef]
- Tanaka, H.; Ogata, T.; Shibata, T.; Nagai, H.; Takahashi, Y.; Kinoshita, M.; Matsubayashi, K.; Hattori, S.; Taniguchi, C. Shorter Incubation Period among COVID-19 Cases with the BA.1 Omicron Variant. Int. J. Environ. Res. Public Health 2022, 19, 6330. [Google Scholar] [CrossRef]
- Du, Z.; Liu, C.; Wang, L.; Bai, Y.; Lau, E.H.Y.; Wu, P.; Cowling, B.J. Shorter serial intervals and incubation periods in SARS-CoV-2 variants than the SARS-CoV-2 ancestral strain. J. Travel Med. 2022, taac052. [Google Scholar] [CrossRef]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef]
- Hayek, S.; Shaham, G.; Ben-Shlomo, Y.; Kepten, E.; Dagan, N.; Nevo, D.; Lipsitch, M.; Reis, B.Y.; Balicer, R.D.; Barda, N. Indirect protection of children from SARS-CoV-2 infection through parental vaccination. Science 2022, 375, 1155–1159. [Google Scholar] [CrossRef]
- Jung, J.; Kim, J.Y.; Park, H.; Park, S.; Lim, J.S.; Lim, S.Y.; Bae, S.; Lim, Y.J.; Kim, E.O.; Kim, J.; et al. Transmission and Infectious SARS-CoV-2 Shedding Kinetics in Vaccinated and Unvaccinated Individuals. JAMA Netw. Open 2022, 5, e2213606. [Google Scholar] [CrossRef] [PubMed]
- Shinjo, Y.; Arima, Y.; Suzuki, M.L. Interim Report of a Case-Control Study Examining Effect of COVID-19 Vaccine (the Third Report). Available online: https://www.niid.go.jp/niid/ja/2019-ncov/2484-idsc/10966-covid19-71.html (accessed on 21 June 2022). (In Japanese)
- Maeda, H.; Morimoto, K.; Saito, N.; Igarashi, A. Vaccine Effectiveness Real-Time Surveillance SARS-CoV-2 (VERSUS) Study (Fourth Report). Available online: https://www.mhlw.go.jp/content/10900000/000922127.pdf (accessed on 21 June 2022). (In Japanese)
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e15. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, K.; Tjan, L.H.; Kurahashi, Y.; Sutandhio, S.; Nishimura, M.; Arii, J.; Mori, Y. Assessment of Neutralizing Antibody Response Against SARS-CoV-2 Variants After 2 to 3 Doses of the BNT162b2 mRNA COVID-19 Vaccine. JAMA Netw. Open 2022, 5, e2210780. [Google Scholar] [CrossRef]
- De Marco, L.; D’Orso, S.; Pirronello, M.; Verdiani, A.; Termine, A.; Fabrizio, C.; Capone, A.; Sabatini, A.; Guerrera, G.; Placido, R.; et al. Assessment of T-cell Reactivity to the SARS-CoV-2 Omicron Variant by Immunized Individuals. JAMA Netw. Open 2022, 5, e2210871. [Google Scholar] [CrossRef] [PubMed]
- GeurtsvanKessel, C.H.; Geers, D.; Schmitz, K.S.; Mykytyn, A.Z.; Lamers, M.M.; Bogers, S.; Scherbeijn, S.; Gommers, L.; Sablerolles, R.S.G.; Nieuwkoop, N.N.; et al. Divergent SARS-CoV-2 Omicron-reactive T and B cell responses in COVID-19 vaccine recipients. Sci. Immunol. 2022, 7, eabo2202. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Labor, Health, and Welfare; National Institute of Infectious Disease. Report of Serum Epidemiology on COVID-19 in 2022 Fiscal Year. Available online: https://www.niid.go.jp/niid/images/epi/corona/79/covid19-79.pdf (accessed on 21 June 2022).


{kind=link}
| Dominant Variant during the Outbreak | Total | ||
|---|---|---|---|
| Omicron | Delta | ||
| Date | 4 January to 20 January 2022 | 21 August to 7 November 2021 | |
| Pandemic wave in Japan | 6th | 5th | |
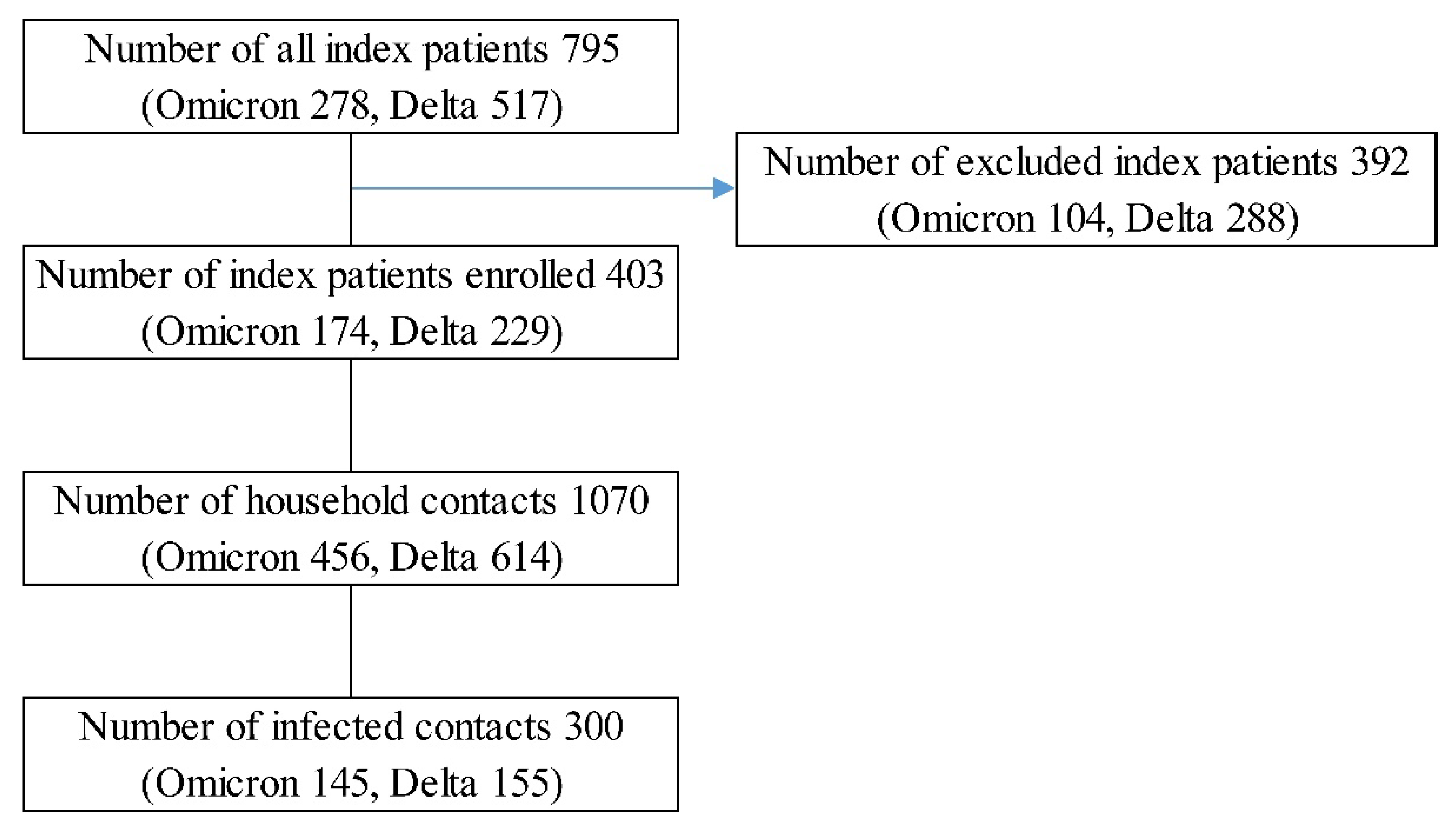
| No. of all index patients | 278 | 517 | 795 |
| Number of index patients enrolled | 174 | 229 | 403 |
| Proportion of index patients enrolled | 62.6% | 44.3% | |
| Test for confirmation of index patients | |||
| Polymerase chain reaction | 112 | 169 | 281 |
| Antigen test | 56 | 52 | 108 |
| Loop-mediated isothermal amplification test | 1 | 7 | 8 |
| Nicking enzyme amplification reaction | 1 | 0 | 1 |
| Unknown | 4 | 1 | 5 |
| Number of household contacts | 456 | 614 | 1070 |
| Variables | Household Contacts | Infected Contacts | Secondary Attack Rate | Multivariate Analysis |
|---|---|---|---|---|
| % (95% CI) | aRR (95% CI) | |||
| N = 456 | N = 145 | 28.0% (25.4–30.8) | ||
| Dominant viral type during the period | ||||
| Delta | 614 | 155 | 25.2% (22.0–28.8) | 1 |
| Omicron | 456 | 145 | 31.8% (27.7–36.2) | 1.61 (1.13–2.28) |
| Risk factors in household contacts | ||||
| Vaccination | ||||
| 0–1* | 602 | 193 | 32.1% (28.5–35.9) | 1 |
| 2†–3 | 468 | 107 | 22.9% (19.3–26.9) | 0.86 (0.69–1.07) |
| Sex | ||||
| Male | 490 | 121 | 24.7% (21.1–28.7) | 1 |
| Female | 580 | 1*79 | 30.9% (27.2–34.7) | 1.26 (1.07–1.48) |
| Age, years | ||||
| ≤19 | 330 | 123 | 37.3% (32.2–42.6) | 1.46 (1.18–1.81) |
| 20–59 | 572 | 135 | 23.6% (20.3–27.3) | 1 |
| ≥60 | 168 | 42 | 25.0% (19.1–32.1) | 1.13 (0.84–1.53) |
| Relationship to index patient | ||||
| Spouse | 155 | 53 | 34.2% (27.2–42.0) | 1.49 (1.12–1.97) |
| Other | 915 | 247 | 31.8% (24.2–30.0) | 1 |
| The size of household | ||||
| 2 | 86 | 25 | 29.1% (20.5–39.4) | 1.04 (0.70–1.54) |
| 3 | 204 | 58 | 28.4% (22.7–35.0) | 1.10 (0.80–1.50) |
| ≥4 | 780 | 217 | 27.8% (24.8–31.1) | 1 |
| Risk factors in index COVID-19 patient | ||||
| Vaccination | ||||
| 0–1* | 704 | 203 | 28.8% (25.6–32.3) | 1 |
| 2†–3 | 366 | 97 | 26.5% (22.2–31.3) | 0.67 (0.46–0.96) |
| Diagnostic delay from onset | ||||
| ≤1 days | 595 | 155 | 26.1% (22.7–29.7) | 1 |
| ≥2 days | 436 | 138 | 31.7% (27.5–36.2) | 1.30 (1.00–1.68) |
| Asymptomatic | 39 | 7 | 17.9% (8.8–33.1) | 1.03 (0.44–2.4) |
| Sex | ||||
| Male | 533 | 164 | 30.8% (27.0–34.8) | 0.82 (0.63–1.07) |
| Female | 537 | 136 | 25.3% (21.8–29.2) | 1 |
| Age, years | ||||
| ≤19 | 394 | 116 | 29.4% (25.2–34.1) | 1.10 (0.81–1.50) |
| 20–59 | 612 | 170 | 27.8% (24.4–31.5) | 1 |
| ≥60 | 64 | 14 | 21.9% (13.4–33.6) | 1.01 (0.58–1.76) |
| Variables | Household Contacts | Infected Contacts | Secondary Attack Rate | Multivariate Analysis |
|---|---|---|---|---|
| % (95% CI) | aRR (95% CI) | |||
| N = 456 | N = 145 | 31.8% (27.7–36.2) | ||
| Risk factors in household contacts | ||||
| Vaccination | ||||
| 0–1* | 143 | 57 | 39.9% (32.2–48.1) | 1 |
| 2†–3 | 313 | 88 | 28.1% (23.4–33.4) | 0.95 (0.68–1.32) |
| Sex | ||||
| Male | 199 | 52 | 26.1% (20.5–32.7) | 1 |
| Female | 257 | 93 | 36.2% (30.6–42.2) | 1.29 (1.01–1.65) |
| Age, years | ||||
| ≤19 | 133 | 51 | 38.3% (30.5–46.8) | 1.23 (0.93–1.64) |
| 20–59 | 267 | 73 | 27.3% (22.3–33.0) | 1 |
| ≥60 | 56 | 21 | 37.5% (26.0–50.6) | 1.18 (0.74–1.90) |
| Relationship to index patient | ||||
| Spouse | 72 | 25 | 34.7% (24.8–46.3) | 1.34 (0.93–1.93) |
| Other | 384 | 120 | 31.3% (26.8–36.1) | 1 |
| The size of household | ||||
| 2 | 36 | 8 | 22.2% (11.6–38.4) | 0.70 (0.37–1.32) |
| 3 | 86 | 31 | 36.0% (26.7–46.6) | 1.25 (0.83–1.89) |
| ≥4 | 334 | 106 | 31.7% (27.0–36.9) | 1 |
| Risk factors in index COVID-19 patient | ||||
| Vaccination | ||||
| 0–1* | 148 | 61 | 41.2% (33.6–49.3) | 1 |
| 2†–3 | 308 | 84 | 27.3% (22.6–32.5) | 0.57 (0.38–0.84) |
| Diagnostic delay from onset | ||||
| ≤1 days | 282 | 84 | 29.8% (24.8–35.4) | 1 |
| ≥2 days | 150 | 57 | 38.0% (30.6–46.0) | 1.38 (0.97–1.97) |
| Asymptomatic | 24 | 4 | 16.7% (6.2–36.6) | 1.01 (0.32–3.3) |
| Sex | ||||
| Male | 233 | 82 | 35.2% (29.4–41.5) | 1 |
| Female | 223 | 63 | 28.3% (22.8–34.5) | 0.72 (0.48–1.07) |
| Age, years | ||||
| ≤19 | 208 | 69 | 33.2% (27.1–39.8) | 1.03 (0.67–1.56) |
| 20–59 | 215 | 68 | 31.6% (25.8–38.1) | 1 |
| ≥60 | 33 | 8 | 24.2% (12.7–41.3) | 0.92 (0.48–1.77) |
| Vaccination of Household Contacts | Vaccination of Index COVID-19 Patients | Household Contacts | Infected Contacts | Secondary Attack Rate |
|---|---|---|---|---|
| 0–1* | 0–1* | 71 | 33 | 46% |
| 0–1* | 2†–3 | 72 | 24 | 33% |
| 2†–3 | 0–1* | 77 | 28 | 36% |
| 2†–3 | 2†–3 | 236 | 60 | 25% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogata, T.; Tanaka, H.; Tanaka, E.; Osaki, N.; Noguchi, E.; Osaki, Y.; Tono, A.; Wada, K. Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan. Int. J. Environ. Res. Public Health 2022, 19, 8068. https://doi.org/10.3390/ijerph19138068
Ogata T, Tanaka H, Tanaka E, Osaki N, Noguchi E, Osaki Y, Tono A, Wada K. Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan. International Journal of Environmental Research and Public Health. 2022; 19(13):8068. https://doi.org/10.3390/ijerph19138068
Chicago/Turabian StyleOgata, Tsuyoshi, Hideo Tanaka, Emiko Tanaka, Natsumi Osaki, Etsuko Noguchi, Yukino Osaki, Ayane Tono, and Koji Wada. 2022. "Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan" International Journal of Environmental Research and Public Health 19, no. 13: 8068. https://doi.org/10.3390/ijerph19138068
APA StyleOgata, T., Tanaka, H., Tanaka, E., Osaki, N., Noguchi, E., Osaki, Y., Tono, A., & Wada, K. (2022). Increased Secondary Attack Rates among the Household Contacts of Patients with the Omicron Variant of the Coronavirus Disease 2019 in Japan. International Journal of Environmental Research and Public Health, 19(13), 8068. https://doi.org/10.3390/ijerph19138068