
A Parent-Focused Creative Approach as a Treatment for a High-Functioning Child with Autism Spectrum Disorder (ASD) in Korea: A Case Study


Abstract
:1. Introduction
2. Literature Review
3. Case Description
3.1. Clinical Profile
3.2. Diagnostic Formulation
4. Materials and Methods
4.1. Art-Based Assessments
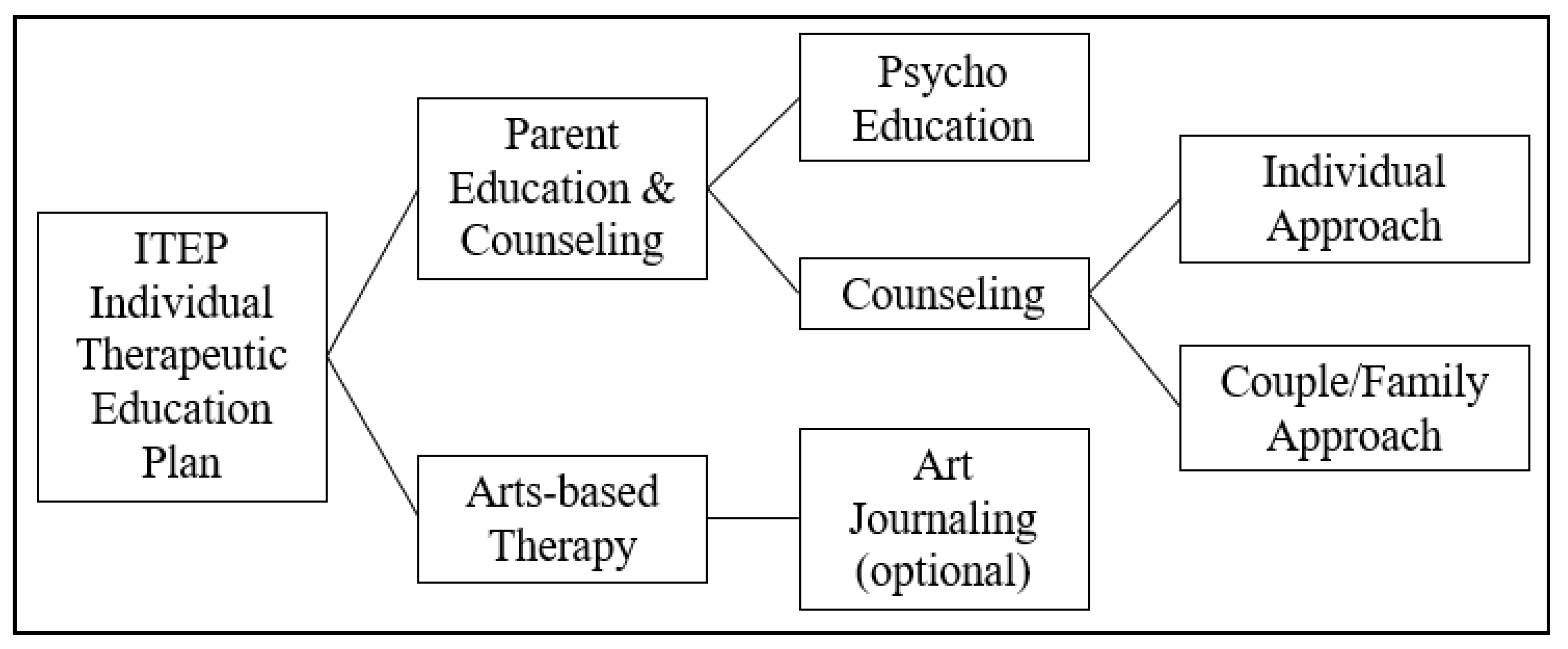
4.2. April’s Individual Therapeutic Education Plan (ITEP)
4.2.1. Parental Education and Counseling Plan
4.2.2. Art therapy with April
5. Results
5.1. Progress
5.1.1. Sessions 1–6: Initial Stage
5.1.2. Sessions 7–17: Active Stage 1
5.1.3. Sessions 18–31: Active Stage 2
5.1.4. Sessions 31–37: Termination Stage
5.2. Treatment Outcome
5.3. Follow-Up Monitoring
6. Discussion
6.1. Two-Way Approach: Parent Involvement in Therapies with Children with ASD
6.2. Emotional Development: Connecting Affect and Cognition with Art
6.3. Art and Creativity: Natural Behavior for Human Development
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Issue | Long-Term Goal | Immediate Short-Term Goal | Objectives | Interventions |
|---|---|---|---|---|---|
| 1 | Language Delay | Communication | (a) Build verbal expression including understanding of meaning of words (b) Practice intonation and pronunciation (c) Build confidence in making sounds | (a) Make verbal responses (b) Use words (c) Build self-confidence | (a) Drawing while singing (b) Making a talking book (c) Parent education on using books, stories in play and using pictures for communication |
| 2 | Lack of expressive language | Emotions Expression | (a) Decrease anxiety with strangers (people other than parents) (b) Build self-confidence with others | (a) Build a foundation for expressive language, starting from emotional safety with others and confidence | (a) Expressing “self” in art play with chosen art materials (b) Interacting with diverse art materials (c) Expressing feelings and emotions through art |
| 3 | Problematic Behaviors | Emotions Regularization | (a) Change (behavioral) responses based on learning of emotions (b) Build self-regularization pattern | (a) Initiate behavioral change based on behavioral analysis assisted by parental observation and record (Appendix B) | (a) Parental observation and analysis of behavior patterns and life schedule (b) Parent education on reshaping behaviors |
| 4 | Lack of Interaction | Emotions Interactions | (a) Meet and make contact with new figures (strangers) in life (b) Initiate with others | (a) Build comfortable/safe feeling with others (b) Learn self-emotional status when being with others (c) Build responses with others | (a) Making a self-representation (doll-making) and theatrical play with the doll in various situations (b) Learning boundaries through art play with paints and other art materials (c) Building a safety zone with art |
| 5 | Lack of Socialization including peer relationship | Sharing Socialization Regularization Adaptation | (a) Adapt/learn to adjust in new social spaces and environments other than the home (b) Trying social activities and extracurricular activities (e.g., group music therapy program) | (a) Learn social cues, manners, and behaviors (b) Understand own feelings with others (c) Build self-confidence in social situations with others in strange/unfamiliar places (d) Understand different roles and others’ (e.g., friends) points of view | (a) Playing with self-representation figure (i.e., doll) by placing the figure in various situations and drawing feelings (b) Making a safe mask for pretend play with masks in social situations (c) Scripting and acting (stage playing) with animal friends (d) Parent education on outside and extracurricular activities to expand social boundaries, e.g., regular visits to places such as the playground and theme parks |
| 6 | Sleeping Disturbance | Anxiety | (a) Change sleep pattern (b) Ease anxiety in nighttime | (a) Build new sleep pattern based on sleep schedule analysis by parents’ observation (b) Build sleep rituals and self-habits at nighttime (c) Learn relaxation skills | (a) Talking about and drawing dreams (b) Decorating and building a safe sleep zone (c) Making a worry doll (d) Parent education on ritual-building before sleep |
Appendix B
| Week | Psychoeducation | Art-Based Counseling Topic |
|---|---|---|
| 1, 2 | General information about ASD and April’s issues and treatment goals | Anxiety and worries |
| 3, 4 | Importance of emotional development in children with ASD | Helen’s fears and need of help (including sleeping problems and caring for April) |
| 5, 6 | Importance of parent support to change for development in children with ASD | Couples’ counseling |
| 7, 8 | Use of art for communication, expression, interaction, and socialization in children with ASD (learn basics about home art therapy) | Changes for the home environment |
| 9, 10 | Build safety, boundaries, and attachment through art and play with children | Initiating the changes |
| 11, 12 | Express emotions and build relationships (learn the importance of and ways to build the parent–child relationship) | Learning to relax, communicate, and express (art journaling for the personal process) |
References
- Kasari, C.; Gulsrud, A.; Wong, C.; Kwon, S.; Locke, J. Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. J. Autism Dev. Disord. 2010, 40, 1045–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schertz, H.H.; Horn, K.; Lee, M.; Mitchell, S. Supporting parents to help toddlers with autism risk make social connections. Young Except. Child. 2017, 20, 16–29. [Google Scholar] [CrossRef]
- Matson, M.; Mahan, S.; Matson, J. Parent training: A review of methods for children with autism spectrum disorders. Res. Autism Spectr. Disord. 2009, 3, 868–875. [Google Scholar] [CrossRef]
- Zaghlawan, H.Y.; Ostrosky, M.M. A parent-implemented intervention to improve imitation skills by children with autism: A pilot study. Early Child. Educ. J. 2016, 44, 671–680. [Google Scholar] [CrossRef]
- Barna, I.; Androne, M. The language of literary texts: Between artistic philosophy and cognitive-behavioral therapy. Procedia-Soc. Behav. Sci. 2012, 51, 268–271. [Google Scholar] [CrossRef] [Green Version]
- Green, J.; Basis The BASIS Team; Wan, M.W.; Guiraud, J.; Holsgrove, S.; McNally, J.; Slonims, V.; Elsabbagh, M.; Charman, T.; Pickles, A.; et al. Intervention for Infants at Risk of Developing Autism: A Case Series. J. Autism Dev. Disord. 2013, 43, 2502–2514. [Google Scholar] [CrossRef]
- Schweizer, C.; Knorth, E.J.; Spreen, M. Art therapy with children with Autism Spectrum Disorders: A review of clinical case descriptions on ‘what works’. Arts Psychother. 2014, 41, 577–593. [Google Scholar] [CrossRef]
- Lu, L.; Petersen, F.; Lacroix, L.; Rousseau, C. Stimulating creative play in children with autism through sandplay. Arts Psychother. 2010, 37, 56–64. [Google Scholar] [CrossRef]
- Martin, N. Art therapy and autism: Overview and recommendations. Art Ther. J. Am. Art Ther. Assoc. 2009, 26, 187–190. [Google Scholar] [CrossRef]
- Martin, N. Art as an Early Intervention Tool for Children With Autism; Jessica Kingsley: London, UK, 2009. [Google Scholar]
- Thayer, F.C. Evaluation of a Developmental Individualized Relationship (DIR®) and Creative Arts Therapies Program for Children with Autism. Ph.D. Thesis, Expressive Therapies Division, Lesley University, Cambridge, MA, USA, 2016. Retrieved from ProQuest. (10036375). [Google Scholar]
- Kuo, N.-C.; Plavnick, J.B. Using an Antecedent Art Intervention to Improve the Behavior of a Child with Autism. Art Ther. 2015, 32, 54–59. [Google Scholar] [CrossRef]
- Lee, J.H. Effectiveness of group art therapy for mothers of children with disabilities. Arts Psychother. 2020, 73, 101754. [Google Scholar] [CrossRef]
- Lee, G.K. Parents of children with high functioning autism: How well do they cope and adjust? J. Dev. Phys. Disabil. 2009, 21, 93. [Google Scholar] [CrossRef]
- Hodge, D.; Hoffman, C.D.; Sweeney, D.P. Increased psychopathology in parents of children with autism: Genetic liability or burden of caregiving? J. Dev. Phys. Disabil. 2011, 23, 227–239. [Google Scholar] [CrossRef]
- Keenan, B.M.; Newman, L.K.; Gray, K.M.; Rinehart, N.J. Parents of Children with ASD Experience More Psychological Distress, Parenting Stress, and Attachment-Related Anxiety. J. Autism Dev. Disord. 2016, 46, 2979–2991. [Google Scholar] [CrossRef] [PubMed]
- Krakovich, T.M.; McGrew, J.H.; Yu, Y.; Ruble, L.A. Stress in parents of children with autism spectrum disorder: An fexploration of demands and resources. J. Autism Dev. Disord. 2016, 46, 2042–2053. [Google Scholar] [CrossRef]
- Adib, N.; Ibrahim, M.; Rahman, A.; Bakar, R.; Yahaya, N.; Hussin, S.; Mansor, W. Perceived Stress among Caregivers of Children with Autism Spectrum Disorder: A State-Side Study. Int. J. Environ. Res. Public Health 2019, 16, 1468. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.J.; Kim, Y.H. Establishment of community-based integrated model for early detection and early intervention of young children with disabilities. J. Korean Assoc. Pers. Autism 2018, 18, 29–59. [Google Scholar] [CrossRef]
- Ingersoll, B.; Wainer, A.L.; Berger, N.I.; Pickard, K.E.; Bonter, N. Comparison of a self-directed and therapist-assisted telehealth parent-mediated intervention for children with ASD: A pilot RCT. J. Autism Dev. Disord. 2016, 46, 2275–2284. [Google Scholar] [CrossRef]
- Park, J.E. Effectiveness of creative arts-based parent training for parents with children with Autism Spectrum Disorder. Arts Psychother. 2021, 76, 101837. [Google Scholar] [CrossRef]
- Leong, D. Art in a hidden world: Creative process and invisible anomaly. Int. J. Arts Soc. Annu. Rev. 2013, 7, 29. [Google Scholar]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Wetherby, A.M.; Woods, J.; Allen, L.; Cleary, J.; Dickinson, H.; Lord, C. Early Indicators of Autism Spectrum Disorders in the Second Year of Life. J. Autism Dev. Disord. 2004, 34, 473–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeBarton, E.S.; Iverson, J.M. Gesture development in toddlers with an older sibling with autism. Int. J. Lang. Commun. Disord. 2015, 51, 18–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Autism Speaks. “Real world” Autism Interventions for Home and School. Available online: http://www.autismspeaks.org/blog/2017/03/28/%E2%80%98real-world%E2%80%99-autism-interventions-home-and-school (accessed on 8 February 2017).
- Berkovits, L.; Eisenhower, A.; Blacher, J. Emotion Regulation in Young Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2017, 47, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Daou, N.; Hady, R.T. Teaching children with autism spectrum disorder to recognize and express emotion: A review of the literature. Int. Electron. J. Elem. Educ. 2016, 9, 419–432. [Google Scholar]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Achenback, T.M. Manual for the Child Behavior Checklist; Univ. Vermont/Dept. Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Gresham, F.M.; Elliott, S.N. Social Skills Improvement System-Rating Scales; Pearson Assessments: Minneapolis, MN, USA, 2008. [Google Scholar]
- Wechsler, D. Wechsler Preschool and Primary Scale of Intelligence–III: Technical and Interpretative Manual; Psychological Corporation: San Antonio, TX, USA, 2002. [Google Scholar]
- Carrow-Woolfolk, E. CASL: Comprehensive Assessment of SPOKEN Language; American Guidance Services: Circle Pines, MN, USA, 1999. [Google Scholar]
- Constantino, J.N.; Gruber, C.P. Social Responsiveness Scale (SRS) Manual; Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.C.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule, Second Edition (ADOS-2); Western Psychological Services: Torrance, CA, USA, 2012. [Google Scholar]
- Baron-Cohen, S.; Leslie, A.M.; Frith, U. Does the autistic child have a “theory of mind”? Cognition 1985, 21, 37–46. [Google Scholar] [CrossRef]
- Mazza, M.; Mariano, M.; Peretto, S.; Masedu, F.; Pino, M.C.; Valenti, M. The role of theory of mind on social information processing in children with autism spectrum disorders: A mediation analysis. J. Autism Dev. Disord. 2017, 47, 1369. [Google Scholar] [CrossRef]
- Scambler, D.J.; Hepburn, S.; Rutherford, M.D.; Wehner, E.A.; Roger, S.J. Emotional responsibility in children with autism, children with other developmental disabilities, and children with typical development. J. Autism Dev. Disord. 2007, 37, 553–563. [Google Scholar] [CrossRef]
- Grossman, J.B.; Klin, A.; Carter, A.S.; Volkmar, F.R. Verbal bias in recognition of facial emotions in children with Asperger syndrome. J. Child Psychol. Psychiatry 2000, 41, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Lindner, J.L.; Rosen, L.A. Decoding of emotion through facial expression, prosody and verbal content in children and adolescents with Asperger’s syndrome. J. Autism Dev. Disord. 2006, 36, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Richard, D.A.; More, W.; Joy, S.P. Recognizing emotions: Testing an intervention for children with autism spectrum disorders. Art Ther. J. Am. Art Ther. Assoc. 2015, 32, 13–19. [Google Scholar] [CrossRef]
- Daou, N.; Vener, S.M.; Poulson, C.L. Analysis of three components of affective behavior in children with autism. Res. Autism Spectr. Disord. 2014, 8, 480–501. [Google Scholar] [CrossRef]
- Gena, A.; Krantz, P.J.; McClannahan, L.E.; Poulson, C.L. Training and generalization of affective behavior displayed by youth with autism. J. Appl. Behav. Anal. 1996, 29, 291–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argott, P.; Townsend, D.B.; Sturmey, P.; Poulson, C.L. Increasing the use of empathic statements in the presence of a non-verbal affective stimulus in adolescents with autism. Res. Autism Spectr. Disord. 2008, 2, 341–352. [Google Scholar] [CrossRef]
- Daou, N. Conducting Behavioral Research with Children Attending Nonbehavioral Intervention Programs for Autism: The Case of Lebanon. Behav. Anal. Pract. 2014, 7, 78–90. [Google Scholar] [CrossRef] [Green Version]
- DeQuinzio, J.A.; Townsend, D.B.; Sturmey, P.; Poulson, C.L. Generalized imitation of facial models by children with autism. J. Appl. Behav. Anal. 2007, 40, 755–759. [Google Scholar] [CrossRef] [Green Version]
- Hobson, R.P.; Ouston, J.; Lee, A. What’s in face? Case Autism. Br. J. Psychol. 1998, 79, 441–453. [Google Scholar] [CrossRef]
- Klin, A.; Jones, W.; Schultz, R.; Volkmar, F.; Cohen, D. Visual fixation patterns during viewing of naturalistic social situations as predictors of social competence in individuals with autism. Arch. Gen. Psychiatry 2002, 59, 809–816. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Wigram, T.; Gold, C. Emotional, motivational and interpersonal responsiveness of children with autism in improvisational music therapy. Autism 2009, 13, 389–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Betts, D.J. Developing a Projective Drawing Test: Experiences with the Face Stimulus Assessment (FSA). Art Ther. 2003, 20, 77–82. [Google Scholar] [CrossRef]
- Gardner, H. The Arts and Human Development; Basic Books: New York, NY, USA, 1994. [Google Scholar]
- Allgood, N. Parent’s perceptions of family-based group music therapy for children with autism spectrum disorders. Music. Ther. Perspect. 2005, 23, 92–99. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.L.; DiLavore, P.C.; Risi, S. Autism Diagnostic Observation Schedule—WPS; WPS, Ed.; Western Psychological Services: Los Angeles, CA, USA, 1999. [Google Scholar]
- Yoo, H.J.; Kwak, Y.S. Autism Diagnostic Observation Schedule; Hak-ji-sa: Seoul, Korea, 2007. [Google Scholar]
- Chopler, E.; Reichler, R.J.; DeVellis, R.F.; Daly, K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 1980, 10, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Park, R. The childhood Autism Rating Scale (CARS): For Diagnostic Screening and Classification of Autism; Special Education Publisher: Seoul, Korea, 1996. [Google Scholar]
- Kim, Y.; Seong, T.; Lee, Y. Preschool Receptive Expressive Language Scale (PRES); Hansol Education: Seoul, Korea, 2003. [Google Scholar]
- Kim, Y.T.; Hong, G.H.; Kim, K.H.; Jang, H.S.; Lee, J.Y. Receptive & Expressive Vocabulary Test (REVT); Seoul Community Rehabilitation Center: Seoul, Korea, 2009. [Google Scholar]
- Shin, M.; Kim, J.; Lee, S.; Lee, S. Speech Mechanism Screening Test (SMST); Hakjisa: Seoul, Korea, 2009. [Google Scholar]
- Pénzes, I.; van Hooren, S.; Dokter, D.; Smeijsters, H.; Hutschemaekers, G. Material interaction in art therapy assessment. Arts Psychother. 2014, 41, 484–492. [Google Scholar] [CrossRef]
- Lusebrink, V.B. Assessment and Therapeutic Application of the Expressive Therapies Continuum: Implications for Brain Structures and Functions. Art Ther. 2010, 27, 168–177. [Google Scholar] [CrossRef]
- Lusebrink, V.B. Art Therapy and the Brain: An Attempt to Understand the Underlying Processes of Art Expression in Therapy. Art Ther. 2011, 21, 125–135. [Google Scholar] [CrossRef]
- Hinz, L. Expressive Therapies Continuum: A Framework for Using Art in Therapy; Routledge: New York, NY, USA, 2009. [Google Scholar]
- Beery, K.E. Revised Administration, Scoring and Teaching Manual for the Developmental Test of Visual-motor Integration; Modern Curriculum Press: Cleveland, OH, USA, 1982. [Google Scholar]
- Kaplan, E.F.; Goodglass, H.; Weintraub, S. The Boston Naming Test; Lea & Febiger: Philadelphia, PA, USA, 1983. [Google Scholar]
- Bracken, B.A.; Boatwright, B.S. CAT-C: Clinical Assessment of Attention Deficit-Child; Psychological Assessment Resources, Incorporated: Lutz, FL, USA, 2005. [Google Scholar]
- Oh, K.J.; Lee, H.L.; Hong, K.E.; Ha, E.H. Korean Version of Child Behavior Checklist (K-CBCL); ChungAng Aptitude Publishing: Seoul, Korea, 1997. [Google Scholar]
- Doll, E.A. Vineland Social Maturity Scale: Condensed Manual of Directions; American Guidance Service: Circle Pines, MN, USA, 1965. [Google Scholar]
- Kaufman, A.S.; Kaufman, N.L. Kaufman Assessment Battery for Children Interpretive Manual; American Guidance Service: Circle Pines, MN, USA, 1983. [Google Scholar]
- Moon, S.B.; Byun, C.J. Interpretation Manual for the Kaufman Assessment Battery for Children-Korean; Hakjisa: Seoul, Korea, 1997. [Google Scholar]
- Rutter, M.; Bailey, A.; Lord, C. Social Communication Questionnaire (SCQ); Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Bottema-Beutel, K.; Yoder, P.J.; Hochman, J.M.; Watson, L.R. The role of supported joint engagement and parent utterances in language and social communication development in children with autism spectrum disorder. J. Autism Dev. Disord. 2014, 44, 2162–2174. [Google Scholar] [CrossRef] [Green Version]
- Kallael, A. Autism and Our Community: Feedback From Early Intervention Providers. Master’s Thesis, Southern Illinois University, Carbondale, IL, USA, 2014. [Google Scholar]
- Ingersoll, B. The social role of imitation in autism: Implications for the treatment of imitation deficits. Infants Young Child. 2008, 21, 107–119. [Google Scholar] [CrossRef] [Green Version]
- Lusebrink, V.B.; Hinz, L.D. Cognitive and symbolic aspects of art therapy and similarities with large scale brain networks. Art Ther. J. Am. Art Ther. Assoc. 2020, 37, 113–122. [Google Scholar] [CrossRef]
- Dissanayake, E. What Is Art For? University of Washington Press: Seattle, WA, USA, 1988. [Google Scholar]
- Stern, D.N. Forms of Vitality: Exploring Dynamic Experience in Psychology, the Arts, Psychotherapy, and Development; Oxford University Press: Oxford, UK, 2010. [Google Scholar]
- Schweizer, C.; Knorth, E.; Yperen, T.; Spreen, M. Evaluation of ‘image of self,’ an art therapy program for children diagnosed with autism spectrum disorder (ASD). Child. Youth Serv. Rev. 2020, 116, 105207. [Google Scholar] [CrossRef]
- Osborne, J. Art and the child with autism: Therapy or education? Early Child Dev. Care 2010, 173, 411–423. [Google Scholar] [CrossRef]
- Evans, K. Sharping experience and sharing meaning art therapy for children with autism. Inscape 1998, 3, 17–25. [Google Scholar] [CrossRef]
- D’Amico, M.; Lalonde, C. The effectiveness of art therapy for teaching social skills to children with autism spectrum disorder. Art Ther. 2017, 34, 176–182. [Google Scholar] [CrossRef]
- Lesner, W.J.; Hillman, D. A Developmental Schema of Creativity. J. Creative Behav. 1983, 17, 103–114. [Google Scholar] [CrossRef]
- Goldstein, J.; Kornfield, J. Seeking the Heart of Wisdom: The Path of Insight Meditation; Shambhala: Boson, MA, USA; London, UK, 2001. [Google Scholar]
- Hass-Cohen, N.; Carr, R. Art Therapy and Clinical Neuroscience; Jessica Kingsley Publisher: London, UK, 2008. [Google Scholar]
- Sternberg, R. The Nature of Creativity: Contemporary Psychological Perspectives; Cambridge University Press: Cambridge, UK, 1988. [Google Scholar]
- Stuckey, H.; Nobel, J. The connection between art, healing, and public health: A review of current literature. Am. J. Public Health 2010, 100, 254–263. [Google Scholar] [CrossRef]
- Runco, M.; Jaeger, G. The standard definition of creativity. Creat. Res. J. 2012, 24, 92–96. [Google Scholar] [CrossRef]
- Dissanayake, E. Art and Intimacy. University of Washington Press: Seattle, WA, USA, 2012. [Google Scholar]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.E.J. A Parent-Focused Creative Approach as a Treatment for a High-Functioning Child with Autism Spectrum Disorder (ASD) in Korea: A Case Study. Int. J. Environ. Res. Public Health 2022, 19, 7836. https://doi.org/10.3390/ijerph19137836
Park JEJ. A Parent-Focused Creative Approach as a Treatment for a High-Functioning Child with Autism Spectrum Disorder (ASD) in Korea: A Case Study. International Journal of Environmental Research and Public Health. 2022; 19(13):7836. https://doi.org/10.3390/ijerph19137836
Chicago/Turabian StylePark, Jung Eun Jeanne. 2022. "A Parent-Focused Creative Approach as a Treatment for a High-Functioning Child with Autism Spectrum Disorder (ASD) in Korea: A Case Study" International Journal of Environmental Research and Public Health 19, no. 13: 7836. https://doi.org/10.3390/ijerph19137836
APA StylePark, J. E. J. (2022). A Parent-Focused Creative Approach as a Treatment for a High-Functioning Child with Autism Spectrum Disorder (ASD) in Korea: A Case Study. International Journal of Environmental Research and Public Health, 19(13), 7836. https://doi.org/10.3390/ijerph19137836