
Is There a Direct Link between Sexual Satisfaction and Restrictions during the Second Wave of the COVID-19 Pandemic?



Abstract

1. Introduction
2. Materials and Methods
2.1. Procedure and Participants
2.2. Measures
2.2.1. Sexual Satisfaction
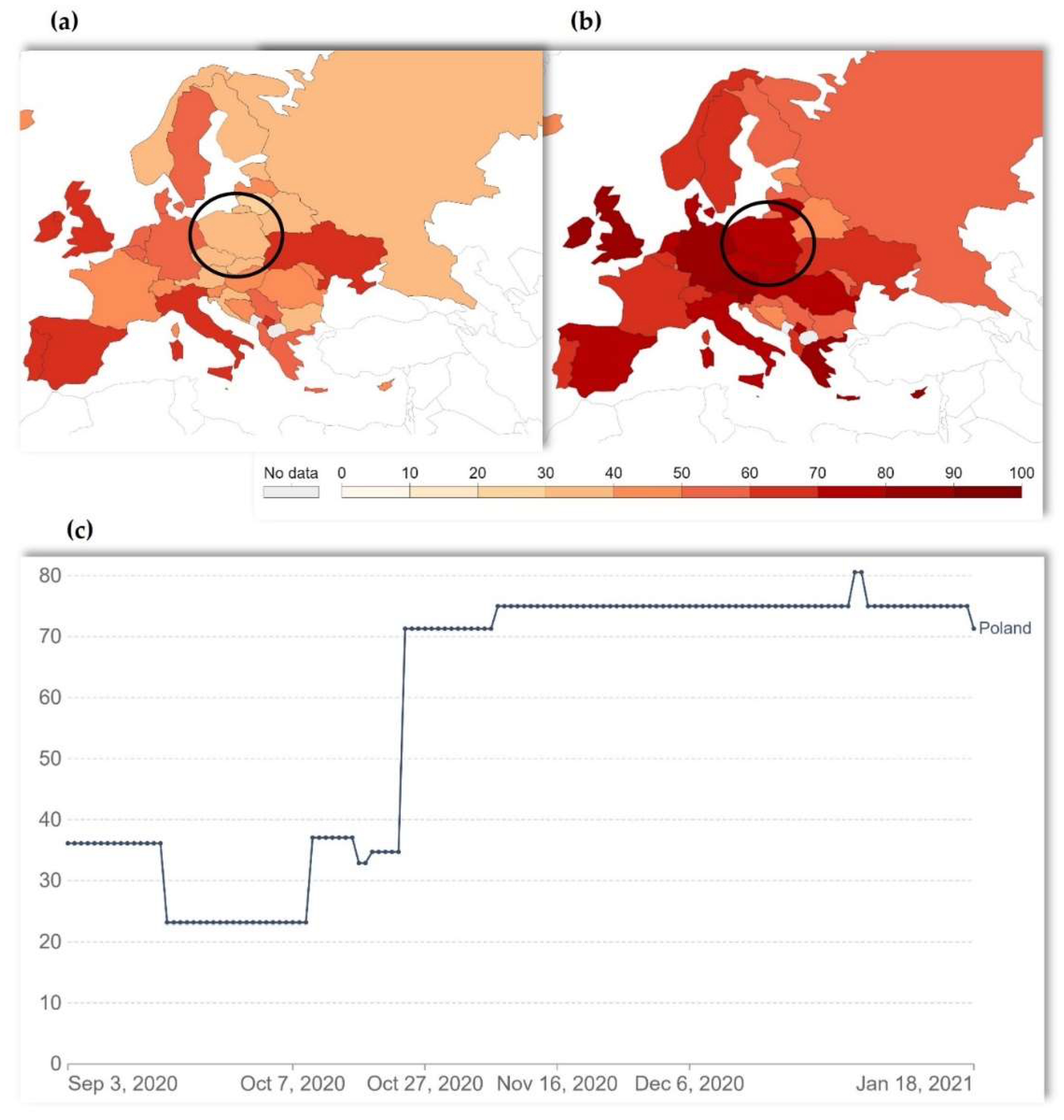
2.2.2. Stringency Index
2.3. Statistical Analysis
3. Results
3.1. Stringency Index
3.2. Sexual Satisfaction
3.3. Differences in Sexual Satisfaction Dependent on Stringency Level during the Data Collection
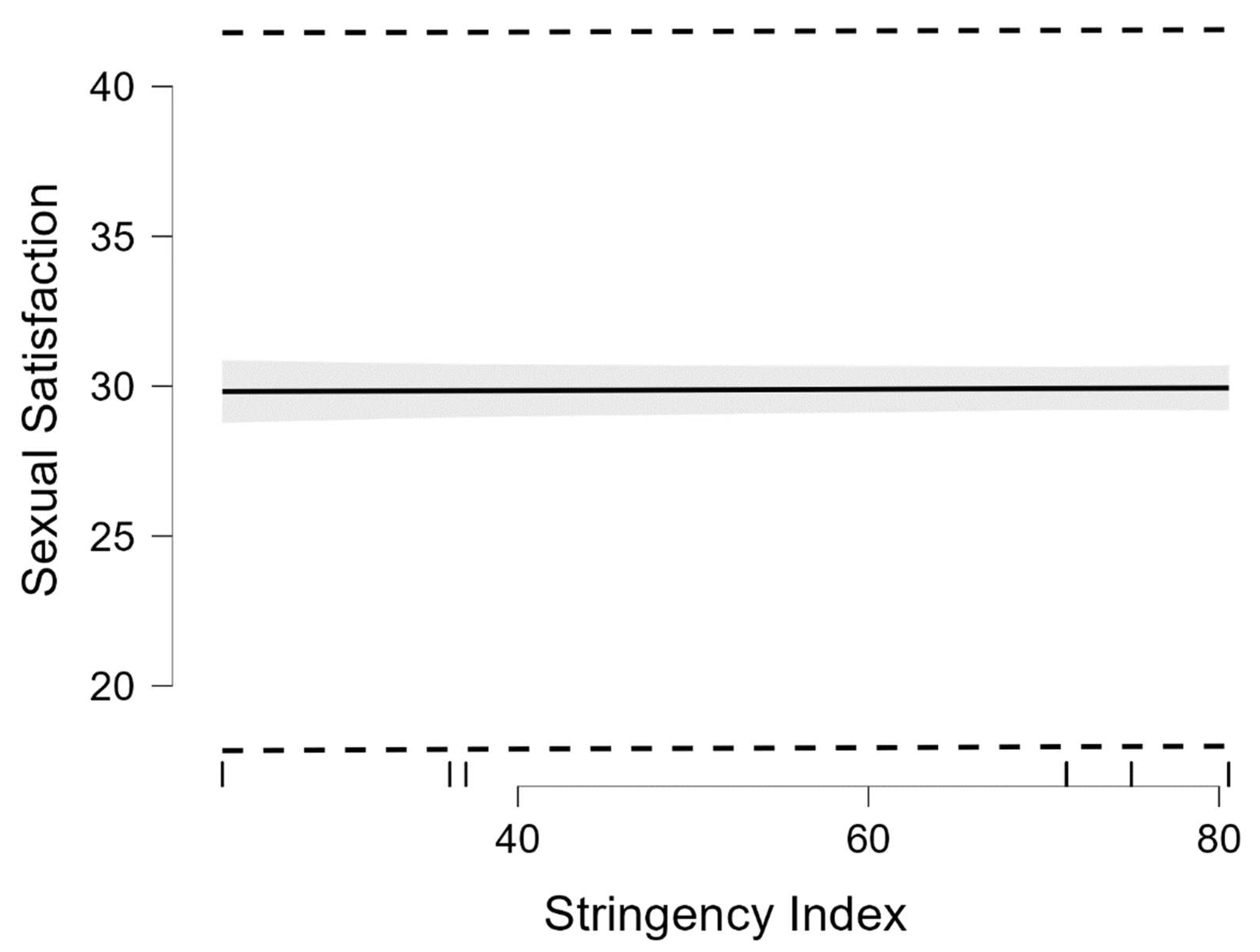
3.4. Association between Sexual Satisfaction and Stringency Level during the Second Wave of the COVID-19 Pandemic
4. Discussion
Limitation of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat. Hum. Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Aknin, L.B.; de Neve, J.-E.; Dunn, E.W.; Fancourt, D.E.; Goldberg, E.; Helliwell, J.F.; Jones, S.P.; Karam, E.; Layard, R.; Lyubomirsky, S.; et al. Mental health during the first year of the COVID-19 pandemic: A review and recommendations for moving forward. Perspect. Psychol. Sci. 2022. [Google Scholar] [CrossRef] [PubMed]
- Manchia, M.; Gathier, A.W.; Yapici-Eser, H.; Schmidt, M.V.; de Quervain, D.; van Amelsvoort, T.; Bisson, J.I.; Cryan, J.F.; Howes, O.D.; Pinto, L.; et al. The impact of the prolonged COVID-19 pandemic on stress resilience and mental health: A critical review across waves. Eur. Neuropsychopharmacol. 2022, 55, 22–83. [Google Scholar] [CrossRef]
- de Sousa, G.M., Jr.; de Oliveira Tavares, V.D.; de Meiroz Grilo, M.L.P.; Coelho, M.L.G.; de Lima-Araújo, G.L.; Schuch, F.B.; Galvão-Coelho, N.L. Mental Health in COVID-19 Pandemic: A Meta-Review of Prevalence Meta-Analyses. Front. Psychol. 2021, 12, 703838. [Google Scholar] [CrossRef] [PubMed]
- Gray, B.; van Ommeren, M.; Lewis, S.; Akhtar, A.; Hanna, F.; Fleischmann, A.; Chisholm, D.; Kestel, D. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief, 2 March 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 1 June 2022).
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.; Shrestha, A.D.; Stojanac, D.; Miller, L.J. The impact of the COVID-19 pandemic on women’s mental health. Arch. Women Ment. Health 2020, 23, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Elharake, J.A.; Akbar, F.; Malik, A.A.; Gilliam, W.; Omer, S.B. Mental health impact of COVID-19 among children and college students: A systematic review. Child. Psychiatry Hum. Dev. 2022. [Google Scholar] [CrossRef]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Research 2020, 9, 636. [Google Scholar] [CrossRef]
- Rogowska, A.M.; Ochnik, D.; Kuśnierz, C.; Chilicka, K.; Jakubiak, M.; Paradowska, M.; Głazowska, L.; Bojarski, D.; Fijołek, J.; Podolak, M.; et al. Changes in mental health during three waves of the COVID-19 pandemic: A repeated cross-sectional study among polish university students. BMC Psychiatry 2021, 21, 627. [Google Scholar] [CrossRef]
- Ochnik, D.; Rogowska, A.M.; Kuśnierz, C.; Jakubiak, M.; Wierzbik-Strońska, M.; Schütz, A.; Held, M.J.; Arzenšek, A.; Pavlova, I.; Korchagina, E.V.; et al. Exposure to COVID-19 during the First and the Second Wave of the Pandemic and Coronavirus-Related PTSD Risk among University Students from Six Countries—A Repeated Cross-Sectional Study. J. Clin. Med. 2021, 10, 5564. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Defining Sexual Health. Available online: https://www.who.int/reproductivehealth/topics/sexual_health/sh_definitions/en/ (accessed on 15 August 2020).
- Mitchell, K.R.; Lewis, R.; O’Sullivan, L.F.; Fortenberry, J.D. What is sexual wellbeing and why does it matter for public health? Lancet 2021, 6, e608–e613. [Google Scholar] [CrossRef]
- Nomejko, A.; Dolińska-Zygmunt, G. The Sexual Satisfaction Questionnaire psychometric properties. Pol. J. Appl. Psychol. 2014, 12, 105–112. [Google Scholar] [CrossRef]
- Nomejko, A.; Dolińska-Zygmunt, G.; Zdrojewicz, Z. The sense of the quality of life and satisfaction with sex life-own research. Seksuol. Pol. 2012, 10, 54–60. Available online: https://journals.viamedica.pl/seksuologia_polska/article/view/33536/24579 (accessed on 1 June 2022). (In Polish).
- Neto, R.P.; Nascimento, B.; Carvalho Dos Anjos Silva, G.; Barbosa, J.; Júnior, J.B.; Teixeira, T.A.; Srougi, M.; Nahas, W.C.; Hallak, J.; Cury, J. Impact of COVID-19 pandemic on the sexual function of health professionals from an epicenter in Brazil. Sex. Med. 2021, 9, 100408. [Google Scholar] [CrossRef]
- Gauvin, S.; Mulroy, M.E.; McInnis, M.K.; Jackowich, R.A.; Levang, S.L.; Coyle, S.M.; Pukall, C.F. An investigation of sexual and relationship adjustment during COVID-19. Arch. Sex. Behav. 2022, 51, 273–285. [Google Scholar] [CrossRef]
- Dong, M.; Tao, Y.; Wu, S.; Kong, L.; Zhou, F.; Tan, J. Changes in sexual behaviour, anxiety symptoms, and quality of couple relationship of patients with infertility during the COVID-19 lockdown. J. Assist. Reprod. Genet. 2022, 39, 493–504. [Google Scholar] [CrossRef]
- Fang, D.; Peng, J.; Liao, S.; Tang, Y.; Cui, W.; Yuan, Y.; Wu, D.; Hu, B.; Wang, R.; Song, W.; et al. An online questionnaire survey on the sexual life and sexual function of Chinese adult men during the coronavirus disease 2019 epidemic. Sex Med. 2021, 9, 100293. [Google Scholar] [CrossRef]
- Feng, Y.J.; Fan, Y.J.; Su, Z.Z.; Li, B.B.; Li, B.; Liu, N.; Wang, P.X. Correlation of sexual behavior change, family function, and male-female intimacy among adults aged 18–44 years during COVID-19 epidemic. Sex Med. 2021, 9, 100301. [Google Scholar] [CrossRef]
- Li, G.; Tang, D.; Song, B.; Wang, C.; Qunshan, S.; Xu, C.; Geng, H.; Wu, H.; He, X.; Cao, Y. Impact of the COVID-19 pandemic on partner relationships and sexual and reproductive health: Cross-sectional, online survey study. J. Med. Internet Res. 2020, 22, e20961. [Google Scholar] [CrossRef]
- Li, W.; Li, G.; Xin, C.; Wang, Y.; Yang, S. Challenges in the Practice of Sexual Medicine in the Time of COVID-19 in China. J. Sex. Med. 2020, 17, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.S.; Dawood, W.; Eid, N.; Eldeeb, D.; Munir, A.; Arafat, W. Psychological and Sexual Health During the COVID-19 Pandemic in Egypt: Are Women Suffering More? Sex. Med. 2021, 9, 100295. [Google Scholar] [CrossRef] [PubMed]
- Gouvernet, B.; Bonierbale, M. COVID-19 lockdown impact on cognitions and emotions experienced during sexual intercourse. Sexologies 2021, 30, e9–e21. [Google Scholar] [CrossRef]
- Batz, F.; Lermer, E.; Hatzler, L.L.; Vilsmaier, T.; Schröder, L.; Chelariu-Raicu, A.; Behr, J.; Mahner, S.; Buspavanich, P.; Thaler, C.J. The impact of the COVID-19 pandemic on sexual health in cis women living in Germany. J. Sex. Med. 2022, 6, 907–922. [Google Scholar] [CrossRef]
- Hille, Z.; Oezdemir, U.C.; Beier, K.M.; Hatzler, L. The disruptive impact of the COVID-19 pandemic on sexual behavior of a German-speaking population. Sexologies 2021, 30, e23–e33. [Google Scholar] [CrossRef]
- Räuchle, J.; Briken, P.; Schröder, J.; Ivanova, O. Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany. Int. J. Environ. Res. Public Health 2022, 19, 1428. [Google Scholar] [CrossRef]
- Kusuma, A.; Brodjonegoro, S.R.; Soerohardjo, I.; Hendri, A.Z.; Yuri, P. Sexual activities during the COVID-19 pandemic in Indonesia. Afr. J. Urol. 2021, 27, 116. [Google Scholar] [CrossRef]
- Schiavi, M.C.; Spina, V.; Zullo, M.A.; Colagiovanni, V.; Luffarelli, P.; Rago, R.; Palazzetti, P. Love in the Time of COVID-19: Sexual Function and Quality of Life Analysis During the Social Distancing Measures in a Group of Italian Reproductive-Age Women. J. Sex. Med. 2020, 17, 1407–1413. [Google Scholar] [CrossRef]
- Fuchs, A.; Szul, M.; Dulska, A.; Bodziony, J.; Matonóg, A.; Pilarska, J.; Sieradzka, P.; Stojko, R.; Drosdzol-Cop, A. The impact of COVID-19 pandemic on female sexual function. Int. J. Environ. Res. Public Health 2022, 19, 3349. [Google Scholar] [CrossRef]
- Szuster, E.; Kostrzewska, P.; Pawlikowska, A.; Mandera, A.; Biernikiewicz, M.; Kałka, D. Mental and sexual health of Polish women of reproductive age during the COVID-19 pandemic—An online survey. Sex. Med. 2021, 9, 100367. [Google Scholar] [CrossRef]
- Tan, R.; O’Hara, C.A.; Kumar, N. Partnership status, living arrangements, and changes in sexual behaviour and satisfaction during the COVID-19 lockdown: Insights from an observational, cross-sectional online survey in Singapore. Sex. Health 2021, 18, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Cascalheira, C.J.; McCormack, M.; Portch, E.; Wignall, L. Changes in Sexual Fantasy and Solitary Sexual Practice During Social Lockdown Among Young Adults in the UK. Sex. Med. 2021, 9, 100342. [Google Scholar] [CrossRef] [PubMed]
- Bhambhvani, H.P.; Chen, T.; Kasman, A.M.; Wilson-King, G.; Enemchukwu, E.; Eisenberg, M.L. Female sexual function during the COVID-19 pandemic in the United States. Sex. Med. 2021, 9, 100355. [Google Scholar] [CrossRef] [PubMed]
- Gleason, N.; Banik, S.; Braverman, J.; Coleman, E. The Impact of the COVID-19 pandemic on sexual behaviors: Findings from a national survey in the United States. J. Sex. Med. 2021, 18, 1851–1862. [Google Scholar] [CrossRef] [PubMed]
- Osur, J.; Ireri, E.M.; Esho, T. The effect of COVID-19 and its control measures on sexual satisfaction among married couples in Kenya. Sex. Med. 2021, 9, 100354. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Alradie-Mohamed, A.; Kar, S.K.; Sharma, P.; Kabir, R. Does COVID-19 pandemic affect sexual behaviour? A cross-sectional, cross-national online survey. Psychiatry Res. 2020, 289, 113050. [Google Scholar] [CrossRef]
- Zhang, Y.; Wen, C.; Zhang, Y.; Luo, X.; Ma, Z.F. The Impact of Mental Health and Stress Concerns on Relationship and Sexuality Amidst the COVID-19 Lockdown. J. Sex. Med. 2021, 18, 1843–1850. [Google Scholar] [CrossRef]
- Tan, P.L. Changes in frequency and patterns of marital sexual activity during COVID-19: Evidence from longitudinal data prior to, during and after lockdown in Singapore. J. Sex. Med. 2022, 19, 188–200. [Google Scholar] [CrossRef]
- Štulhofer, A.; Mehulić, J.; Briken, P.; Klapilová, K.; de Graaf, H.; Carvalheira, A.A.; Löfgren-Mårtenson, C.; Nobre, P.; Chollier, M.; Köse, Ö.; et al. Perceived changes in sexual interest and distress about discrepant sexual interest during the first phase of COVID-19 pandemic: A multi-country assessment in cohabiting partnered individuals. Arch. Sex. Behav. 2022, 51, 231–246. [Google Scholar] [CrossRef]
- Mumm, J.N.; Vilsmaier, T.; Schuetz, J.M.; Rodler, S.; Zati Zehni, A.; Bauer, R.M.; Staehler, M.; Stief, C.G.; Batz, F. How the COVID-19 Pandemic Affects Sexual Behavior of Hetero-, Homo-, and Bisexual Males in Germany. Sex. Med. 2021, 9, 100380. [Google Scholar] [CrossRef]
- Chen, T.; Bhambhvani, H.P.; Kasman, A.M.; Eisenberg, M.L. The association of the COVID-19 pandemic on male sexual function in the United States: A survey study of male cannabis users. Sex. Med. 2021, 9, 100340. [Google Scholar] [CrossRef] [PubMed]
- Izdebski, Z.; Słowikowska-Hilczer, J.; Mazur, J. The Effect of the COVID-19 Pandemic on the Assessment of Sexual Life—Repeated Cross-Sectional Surveys among Polish Adults in 2017, 2020 and 2021. Int. J. Environ. Res. Public Health 2022, 19, 4110. [Google Scholar] [CrossRef] [PubMed]
- Pennanen-Iire, C.; Prereira-Lourenço, M.; Padoa, A.; Ribeirinho, A.; Samico, A.; Gressler, M.; Jatoi, N.-A.; Mehrad, M.; Girard, A. Sexual Health Implications of COVID-19 Pandemic. Sex. Med. Rev. 2021, 9, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Eleuteri, S.; Alessi, F.; Petruccelli, F.; Saladino, V. The global impact of the COVID-19 pandemic on individuals’ and couples’ sexuality. Front. Psychol. 2022, 12, 798260. [Google Scholar] [CrossRef]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). OurWorldInData.org. 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 1 June 2022).
- George, D.; Mallery, P. IBM SPSS Statistics 26 Step by Step, 16th ed.; Taylor & Francis: New York, NY, USA, 2020. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- JASP Team. 2020 JASP; Version 0.16.0.0; Windows; University of Amsterdam: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Fischer, V.J.; Andersson, G.; Billieux, J.; Vögele, C. The relationship between emotion regulation and sexual function and satisfaction: A scoping review. Sex. Med. Rev. 2022, 10, 195–208. [Google Scholar] [CrossRef]
- McKay, T.; Henne, J.; Gonzales, G.; Gavulic, K.A.; Quarles, R.; Gallegos, S.G. Sexual behavior change among gay and bisexual men during the first COVID-19 pandemic wave in the United States. Sex. Res. Soc. Policy 2021, 2021, 1–15. [Google Scholar] [CrossRef]
- Delcea, C.; Chirilă, V.I.; Săuchea, A.M. Effects of COVID-19 on sexual life—A meta-analysis. Sexologies 2021, 30, e49–e54. [Google Scholar] [CrossRef]
- de Oliveira, L.; Carvalho, J. Women’s sexual health during the pandemic of COVID-19: Declines in sexual function and sexual pleasure. Curr. Sex. Health Rep. 2021, 13, 76–88. [Google Scholar] [CrossRef]
- Masoudi, M.; Maasoumi, R.; Bragazzi, N.L. Effects of the COVID-19 pandemic on sexual functioning and activity: A systematic review and meta-analysis. BMC Public Health 2022, 22, 189. [Google Scholar] [CrossRef]
- Arrington, R.; Cofrancesco, J.; Wu, A.W. Questionnaires to measure sexual quality of life. Qual. Life Res. 2004, 13, 1643–1658. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, D.A.; Dewitte, M. Individual, relational, and sociocultural determinants of sexual function and sexual satisfaction in Ecuador. Sex. Med. 2021, 9, 100307. [Google Scholar] [CrossRef] [PubMed]
- Pollard, A.E.; Rogge, R.D. Love in the Time of COVID-19: A Multi-Wave Study Examining the Salience of Sexual and Relationship Health During the COVID-19 Pandemic. Arch. Sex. Behav. 2022, 51, 247–271. [Google Scholar] [CrossRef] [PubMed]
- Neto, F.; da Conceição Pinto, M. The satisfaction with sex life across the adult life span. Soc. Indic. Res. 2013, 114, 767–784. [Google Scholar] [CrossRef]
- Lorentz, M.S.; Chagas, L.B.; Perez, A.V.; da Silva Cassol, P.A.; Vettorazzi, J.; Lubianca, J.N. Correlation between depressive symptoms and sexual dysfunction in postpartum women during the COVID-19 pandemic. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 258, 162–167. [Google Scholar] [CrossRef]
- Rogowska, A.; Wójcik, N.; Janik, A.; Klimala, P. Sexual satisfaction during the COVID-19 pandemic in Poland. Mendeley Data 2022. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Month | n | Range | M | SD |
|---|---|---|---|---|
| September 2020 | 604 | 11–40 | 31.46 | 6.55 |
| October 2020 | 128 | 17–40 | 31.94 | 4.98 |
| November 2020 | 245 | 13–40 | 31.07 | 5.69 |
| December 2020 | 312 | 12–40 | 31.22 | 6.01 |
| January 2021 | 75 | 13–40 | 30.07 | 6.66 |
| 95% BCaCIB | ||||||||
|---|---|---|---|---|---|---|---|---|
| Model | Variable | B | SEB | LL | UL | β | t | p |
| H0 | Intercept | 31.304 | 0.167 | 30.962 | 31.631 | 187.916 | <0.001 | |
| H1 | Intercept | 28.848 | 0.967 | 26.858 | 30.784 | 29.821 | <0.001 | |
| Stringency Index | 0.002 | 0.009 | −0.016 | 0.021 | 0.007 | 0.242 | 0.809 | |
| Age | 0.037 | 0.026 | −0.012 | 0.083 | 0.038 | 1.422 | 0.155 | |
| Gender (1) | −0.641 | 0.376 | −1.344 | 0.062 | −1.704 | 0.089 | ||
| Relationships (1) | 2.364 | 0.420 | 1.605 | 3.186 | 5.630 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogowska, A.M.; Wójcik, N.; Janik, A.; Klimala, P. Is There a Direct Link between Sexual Satisfaction and Restrictions during the Second Wave of the COVID-19 Pandemic? Int. J. Environ. Res. Public Health 2022, 19, 7769. https://doi.org/10.3390/ijerph19137769
Rogowska AM, Wójcik N, Janik A, Klimala P. Is There a Direct Link between Sexual Satisfaction and Restrictions during the Second Wave of the COVID-19 Pandemic? International Journal of Environmental Research and Public Health. 2022; 19(13):7769. https://doi.org/10.3390/ijerph19137769
Chicago/Turabian StyleRogowska, Aleksandra M., Natalia Wójcik, Aleksandra Janik, and Paulina Klimala. 2022. "Is There a Direct Link between Sexual Satisfaction and Restrictions during the Second Wave of the COVID-19 Pandemic?" International Journal of Environmental Research and Public Health 19, no. 13: 7769. https://doi.org/10.3390/ijerph19137769
APA StyleRogowska, A. M., Wójcik, N., Janik, A., & Klimala, P. (2022). Is There a Direct Link between Sexual Satisfaction and Restrictions during the Second Wave of the COVID-19 Pandemic? International Journal of Environmental Research and Public Health, 19(13), 7769. https://doi.org/10.3390/ijerph19137769