1. Introduction
Neurodevelopmental disorders such as Developmental Coordination Disorder (DCD) are under recognized in developing countries [
1,
2]. Current understanding about the causes of various neurodevelopmental disorders has largely relied on samples from European ancestry, creating concern about the relevance of the science for African populations and global health equity. To objectively measure motor competence, the child’s motor abilities need to be measured with a reliable and valid tool.
The most widely used motor tests to assist in the diagnosis of developmental motor delays are the Movement Assessment Battery for Children, second edition (MABC-2) and the Bruininks–Oseretsky Test of Motor Proficiency, second edition (BOT-2) [
3,
4] as recommended by the international guideline [
5]. Both tests are norm-referenced, reliable and valid in diagnosing developmental motor delays [
5,
6]. As most developmental scales, the MABC and BOT were created in Western European (MABC-2) and North American countries (BOT-2), and item choice, population norms and cut-off scores may be limited to those regions. This raises the issue of whether these assessments would be valid in other countries [
1]. Indeed, several studies have highlighted the importance of validating these assessments given the knowledge that the performance of daily life tasks may be influenced by cultural context [
7]. Furthermore, the results based on the MABC in China, Czech Republic, Italy, Japan and the Netherlands suggest that there may be significant cross-regional differences in motor competence among children, and the results highlight the importance of validating these motor assessments when they are introduced to new regions [
8,
9,
10,
11,
12,
13].
In African countries there is a lack of motor assessments that have been validated for use in children with possible motor delays. We know of no studies that evaluated if the international age-normative values are applicable to school-aged children from African countries. In low resourced areas, for instance, having qualified physical education (PE) teachers and structured PE classes is not common [
14,
15,
16]. Breaks are mostly used for active play and games played usually do not require (special) equipment (small shells, a rope, a piece of chalk, a ball made of plastic bags). Children with coordination difficulties have reduced levels of active play participation, which places them at risk for secondary health problems (i.e., low cardiorespiratory fitness and overweight) [
17,
18]. On the other hand, many children must use active transportation to school and are used to helping out parents with chores that may involve carrying and walking. Moreover, part of the children in African countries are treated for HIV with Antiretroviral Therapy, which is known to influence motor skill development, especially gross motor skills [
19,
20,
21]. North-West province has an estimated of 26,790 children under the age of 15 living with HIV as of midyear 2016 [
22], 45.4% of these children received ART. Given these child and environment related factors the children in various African countries will have developed different motor skills.
Since the psychometric properties of any measure are not universal, but rather specific to the population being reported on [
23], they deserve attention when standardized tests are introduced to new world regions. Especially, establishing cross-cultural validity is of utmost importance as it may hamper the case finding of children with motor problems in different cultures, if found insufficient. As African children are likely to have developed other skills than those being originally assessed with the MABC and BOT, paying attention to and addressing these concerns about content validity [
24], and reference norms is needed in order to determine whether these tests could serve as measurement tools for identifying motor problems in African children. Content validity represents the degree to which an assessment tool measures the construct it intends to measure. The items of a motor test are thought to be related to the skills children will use (and need) in their daily life (content validity) [
25]. The equipment and recreational opportunities available, the educational systems (fine and gross motor training) and beliefs in the society play an important role in what skills children need in everyday activities and will acquire through natural exposure [
26,
27,
28]. Being able to put pegs in tiny holes may be as distant a task to some children as is carrying a basket of vegetables on the head or eating with chop stick to others. Hence, motor development is largely dependent upon the experience-based learning and will therefore be context specific [
29,
30,
31,
32].
Both the MABC-2 and BOT-2 are norm-referenced, reliable and valid in evaluating motor competence and identifying motor developmental delays [
5,
6] and are therefore hypothesized to be related. Since psychometric properties of any measure are not universal but specific to the population, we want to explore the degree to which these two measures yield similar results (convergent validity) [
33]. By determining convergent validity between the two most widely used motor skill assessments, insights are gained into whether these motor skill tests are measuring similar motor skill constructs in children raised under different environmental constraints compared to the countries where the tests were originally developed. Agreement between tests is explored when pre-established cut-points are used to identify cases at risk of motor performance development impairments such as in DCD.
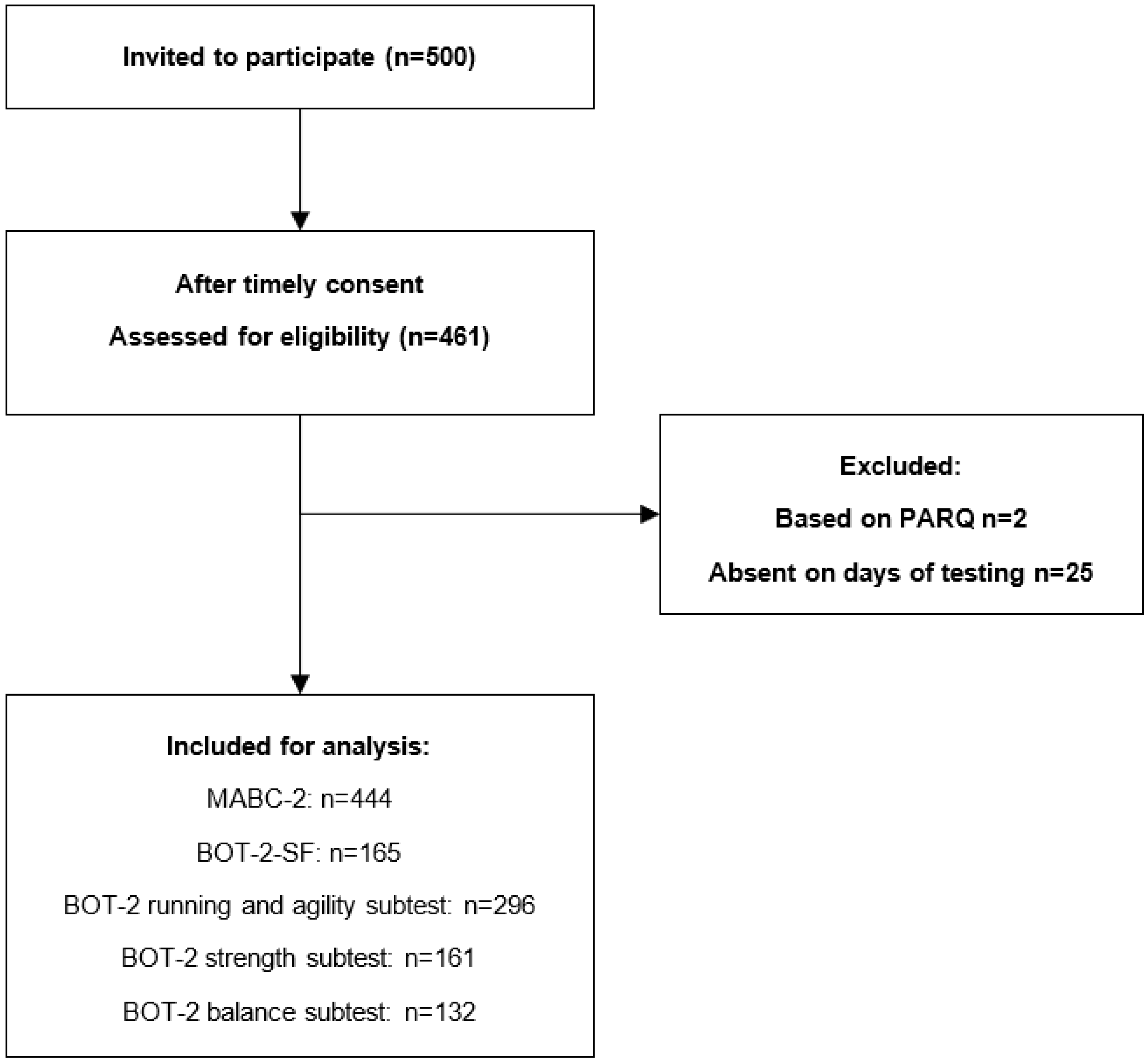
The first aim in establishing cross-cultural validity of the MABC-2 and BOT-2 was to describe the classification on both tests of randomly selected school-aged South African children aged 6–10 years.
Two sub-questions were posed:
- (1)
What are the percentages of the MABC-2 and BOT-2 classification of “at risk” and “impaired categories” for the total test and component scores in a large group of randomly selected school-aged South African children aged 6–10 years?
- (2)
Which items cause classification into the at risk and impaired categories.
The second aim in establishing cross-cultural validity of the MABC-2 and BOT-2 was to investigate the convergent validity between both tests when completed by randomly selected school-aged children aged 6–10 years.
Five sub-questions were posed:
- (1)
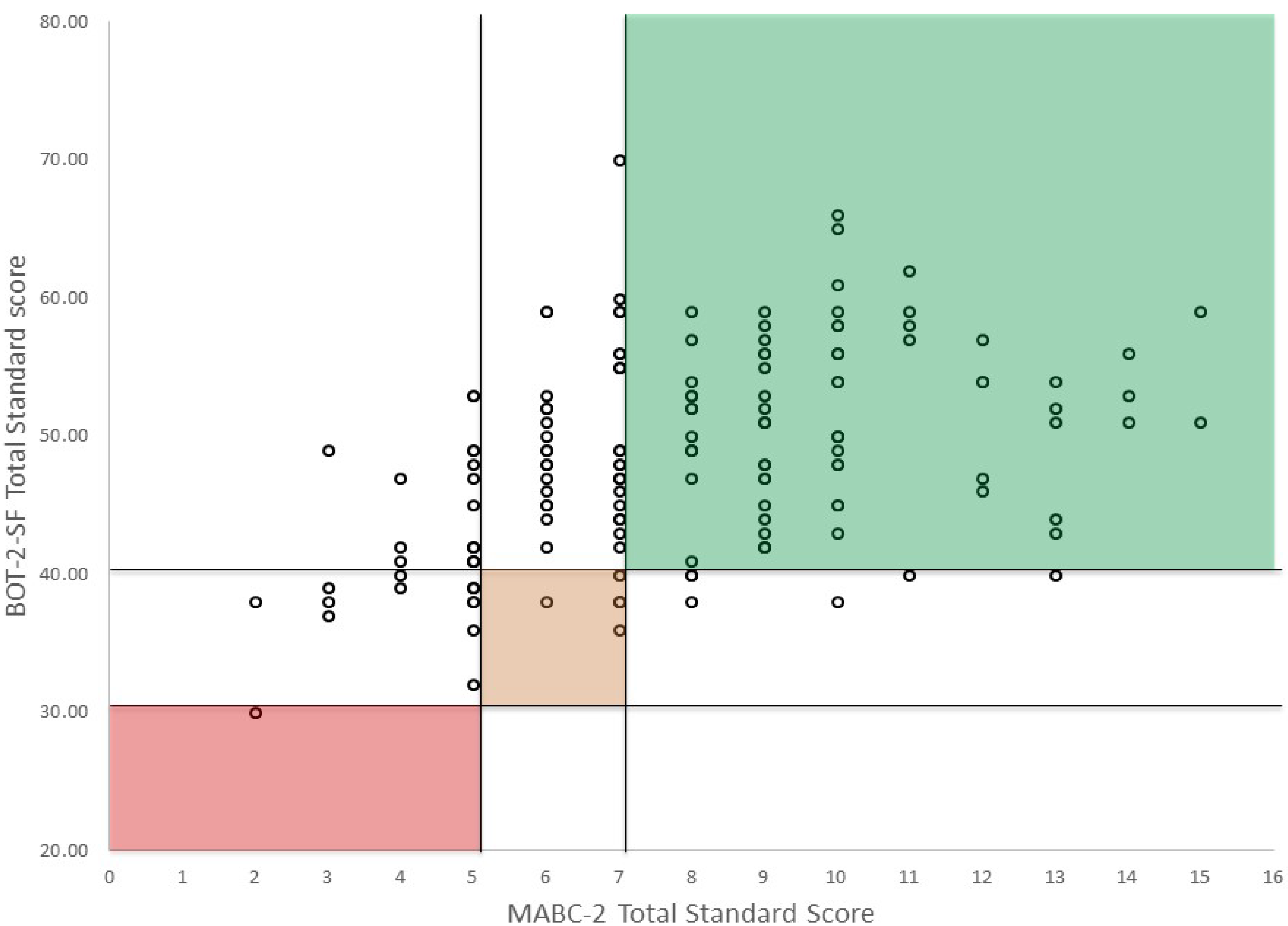
Does the BOT-2-SF standard score significantly correlate with the MABC-2 total test score when completed by children aged 6–10 years?
- (2)
Which proportion of children are classified as having motor problems on both tests and on which percentage of children do they disagree (sensitivity/specificity)?
- (3)
Do the BOT-2 subtest scales Running and Agility, Balance, and Strength significantly correlate with the MABC-2 total score and component scores?
- (4)
What are the overall skill levels on sub tests of the BOT-2 of children designated as at risk for motor problems and definite motor impairments based on the MABC-2 classification.
- (5)
Are there differences in demographics (age, sex, BMI) between children identified by both tests to have typical development, those identified by one test only, and those who do meet criteria for possible motor deficits based on both tests.
4. Discussion
This study examined cross-cultural validity of the MABC-2 and BOT-2 in a randomly selected sample of school-aged South African children. Based on the outcomes of the MABC-2 a prevalence of 36% was found for children at risk for motor problems. Almost 20% of the children obtained scores in the impaired category for the component Manual dexterity. Based on BOT-SF outcomes the percentages of children suspected of poor motor performance was about 17%. The subtest of the BOT-2 with the lowest scores was Strength, with 22% of the children in the at-risk category. The BOT-2-SF total standard score and MABC-2 total test score showed a moderate correlation (r = 0.44) and a fair Kappa of 0.21. Since we used a random group of sufficient sample size, we were able to examine important measures of agreement such as sensitivity and specificity. The specificity of 0.90 tells us how likely it is for the BOT-2 to be negative (no motor difficulties) in case someone does not have motor difficulties. The sensitivity of 0.21 tells us that many children who should have tested positive for motor difficulties based on MABC-2 outcome did not do so on the BOT-2. Lastly there were differences in demographics between motor performance classification groups; children who scored positive (at risk or impaired) on both tests were more often obese than children with other combinations.
The fact that 36% of the children without known disorders scored at or below the 16th percentile of the MABC-2 could mean two things: (1) one third of the children in the current sample has poor motor skills, or (2) the international age-normative mean values are not likely to be applicable to children from African countries. MABC-2 is an easy instrument for screening children over a short period of time and the manual has been translated into numerous languages. However, two points are important to consider. First, generalization of the validity findings is limited to populations with similar attributes, and in similar contexts, as those in whom the instrument was tested for validity. If that is not checked, these instruments may lack to provide information relevant to a specific population living under specific/different circumstances and may be more sensitive to exploration (experience) differences than to motor impairment. Second, even if the instrument is valid, it could still be that norms (and cut-off values) from the original population are not suited for children living in the different context. On the other hand, using the same tool and cut-off scores for research has advantages to compare data across demographic or clinical populations.
4.1. Prevalence of Poor Motor Skills
The percentage of children scoring in the “at risk for motor problems” range was 36% which is much higher than the current estimated prevalence in school-aged children [
37]. Children in different countries will perform different daily tasks, each with different facilitators and barriers in their environments [
28,
38,
39]. DCD has been reported to be more prevalent in low-resourced areas, therefore, differences in percentage are to be expected [
40]. Children in the current sample live in the settings where they often experience limitations with equipment, coaching and space as barriers to participate in physical activities, such as sports. This in turn limits their development of coordinated motor skills [
40]. In particular, art and crafts, and handwriting training is less rigorous due to space (more children in one bench with rough surface or floor seating) and material limitations. Although this information was not sampled, part of the children in the current sample were treated for HIV with Antiretroviral Therapy which might also have influenced their motor skill development. In summary there are reasons to belief that the level of skills on the items included in the MABC-2 might indeed be lower in the random South African sample than in the UK sample.
4.2. BOT-2 MABC-2 Comparison
Although at first sight there are many similarities between MABC-2 and BOT-SF in that they are both focusing on functional motor skills (e.g., fine motor and gross motor skills and balance) and yield a quantitative measure that indicates performance level (norm-referenced values), correlations between the scores (r = 0.44) indicate that they partly measure different constructs or required levels of the motor skills. Thus, these two tests do not meet the criterion for testing similar constructs: (r > 0.5) but of related constructs (0.30–0.50) [
25].
Due to the different nature of motor performance assessment tools, it is not uncommon that different tests identify different children. The number of gross and fine motor items vary between the two tools. Even comparable items have small differences that may lead to different results. For instance, the BOT-2 balance items only last 10 s while the MABC-2 have a maximum time of 30 s. On the other hand, the BOT-2 subtest Balance also includes three items with eyes closed. The time difference may select children with different underlying problems, 30 s is harder but also more prone to pick up distractibility, while the eyes closed items may be more sensitive to poor proprioception. The MABC-2 categorizes jumping or hopping as balance while the BOT-2 orders these items under the construct Running and Agility. Moreover, no items for Bilateral coordination and Strength are included in the MABC-2.
So far, we found only two studies comparing the BOT-2 and MABC-2 in this age range [
41,
42]. Other studies either used an earlier version of the tests [
43,
44] or looked at specific groups (intellectual disabilities: [
45]). The correlation between the first version of the MABC and BOT was also moderate (r = 0.50,
p < 0.01). Kappa’s were also low (k = 0.19 at the 5th percentile; k = 0.29 at 15th percentile cut-points), so comparable to our study [
46]. Spironello and colleagues suggested that the BOT rather than the M-ABC may be preferable in school-based studies where large numbers of children need to be assessed at the same time and where cost prohibits the administration of motor tests by health professionals [
46].
Of the studies comparing second edition of both tests, one study was performed as part of the validation for the Dutch version of the MABC-2. In this study, we compared the full-scale BOT-2 to MABC-2 and a correlation of 0.58 (
p < 0.01) was found [
42]. Although we commonly speak about “the” MABC-2, this test in fact constitutes 3 different test sets, which measure different constructs per age group. This was confirmed when Lane and Brown [
41] examined the convergent validity of the MABC-2 and BOT-2 in 25 children in age band 2 and 25 in age band 3. Importantly, no significant correlation was found between the BOT-2 Total Motor Composite and Total Test Score of the MABC-2 in the age band 2. However, a positive strong correlation was found between the BOT-2 Total Motor Composite and MABC-2 Total Test Score in the age band 3 (rho = 0.80,
p < 0.01).
While we cannot rule out the option that the international age-normative values of the MABC-2 (age band 2) are not applicable to children from African countries, after comparing the results in our study to the outcomes of the BOT-2, it seems the less obvious explanation. Thus far, the prevalence in the current sample of the children seems within the estimated for motor problems on the BOT-2, around 17 percent. The BOT-2 subtests showed no clear picture of high prevalence of low levels of Running and Agility and Balance. For the sub test Strength, the results were less favorable (22% in the lower range), which could be caused by real strength deficits but also partly by the children not being used to making isolated movements. These movements may be more familiar to children doing physical education classes (push-ups and sit-ups) tested in the American norm sample.
4.3. Differences in BMI between Motor Performance Classification Groups
Obesity in the current sample was 10 percent (
n = 17), seven of these children showed poor motor skill levels on both tests. Although one needs to be cautious given these small numbers, the finding that children with low motor coordination had higher BMI concurs with the literature. Hendrix and colleagues, based on a systematic review, concluded that the prevalence of overweight and obesity was consistently higher in children with DCD in studies originating in Australia, Canada, Greece, the Netherlands, Taiwan and Hong Kong [
17]. De Meester et al. also reported that 90% of children in a cohort with low motor coordination did not meet the daily physical activity recommendations for children [
47]. Along with unhealthy dietary habits, physical inactivity is an important risk factor for developing overweight and obesity [
48]. It was suggested by Rivilis that the detrimental effect of poor coordination on body composition might not manifest itself until later in childhood or early adolescence [
18]. However, our research was on younger children (6–10 year), most of which are on a food program. This makes the food intake between our participants with different levels of motor competency more similar, compared to children studied in Western countries. Our results make the explanation that children with low motor skills are more likely to avoid participation in physical activities leading to a secondary exercise deficit disorder and weight gain, feasible [
26,
49].




{kind=link}
{kind=link}