
The Effectiveness of Interventions to Evaluate and Reduce Healthcare Costs of Potentially Inappropriate Prescriptions among the Older Adults: A Systematic Review

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Search Strategy
2.3. Eligibility Criteria
- Patient (P): subjects receiving any specific and nonspecific PIP, aged 65 and over;
- Intervention (I): Any type of intervention aimed at health professionals (i.e., physicians, clinicians, pharmacists, nurses), structures (i.e., nursing homes, hospitals, pharmacies), patients, or any monitoring activities of potentially inappropriate prescriptions and costs incurred, using any explicit criteria for identifying inappropriateness (such as Beers Criteria, PRISCUS list, STOPP/START criteria);
- Comparator (C): No intervention or any other intervention and no monitoring activities;
- Outcomes (O): Postintervention outcomes in terms of cost variation, intervention effectiveness, and avoidable healthcare costs.
2.4. Selection and Data Process
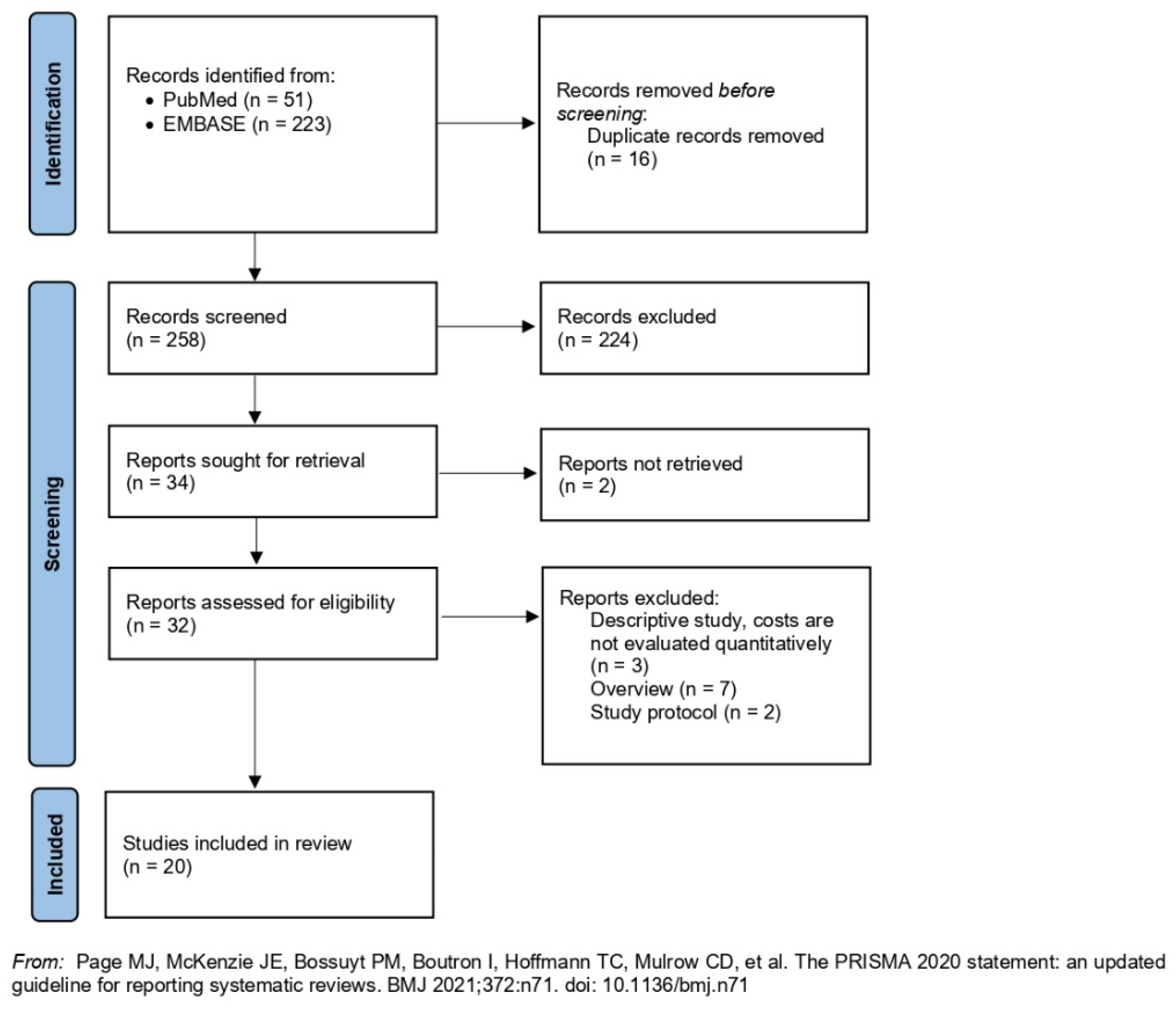
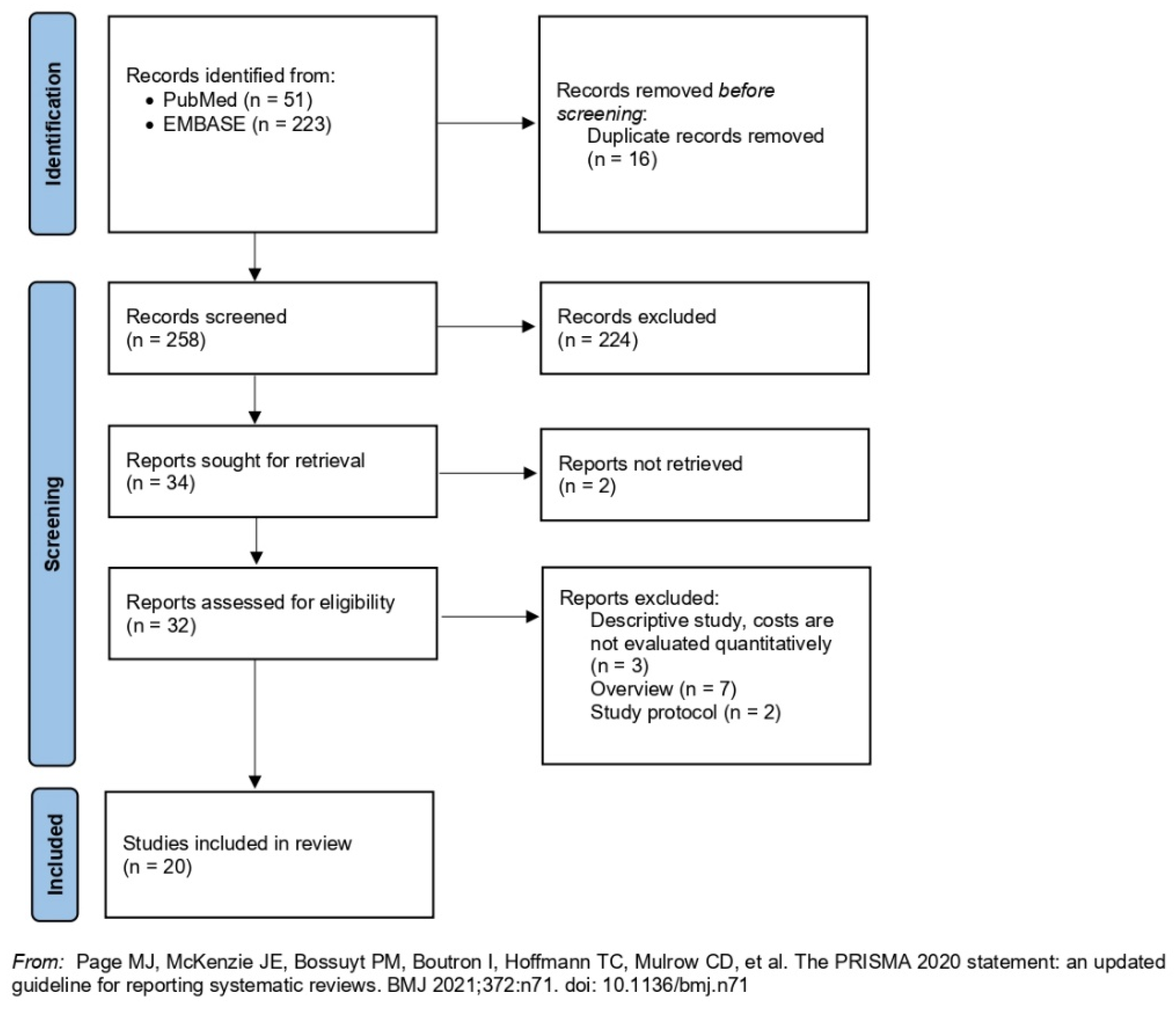
3. Results
- (i)
- Observational studies assessing the frequency of PIPs and associated avoidable costs (n = 12);
- (ii)
- Trials and observational studies carried out on tailored educational interventions and observations of outcomes in terms of postintervention effectiveness and avoided costs (n = 8).
3.1. Studies without Intervention
3.2. Studies with Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Search Strategy Performed in Pubmed/Medline |
| ((((((((((((((((((((((((Inappropriate prescribing [Title/Abstract])) OR (Appropriate Prescribing [Title/Abstract])) OR (high-risk medications [Title/Abstract])) OR (Suboptimal prescribing [Title/Abstract])) OR (Over-prescribing [Title/Abstract])) OR (Under-prescribing [Title/Abstract])) OR (Misprescribing [Title/Abstract])) OR (Inappropriate Drug [Title/Abstract])) OR (Inappropriate Drugs [Title/Abstract])) OR (Inappropriate Medication [Title/Abstract])) OR (OR Inappropriate Medications [Title/Abstract])) OR (Inappropriate Medicines [Title/Abstract])) OR (Inappropriate Prescription [Title/Abstract])) OR (Inappropriate Prescribing [Title/Abstract])) OR (Inappropriate Prescriptions [Title/Abstract])) OR (Inappropriate Use [Title/Abstract])) OR (Medication Appropriateness [Title/Abstract])) OR (Pharmacological Inappropriateness [Title/Abstract])) OR (Potential Drug Therapy Problems [Title/Abstract])) OR (Potentially Harmful Medications [Title/Abstract])) OR (Prescribing Appropriateness [Title/Abstract])) AND (((((aged [MeSH Terms]) OR (Aged, 65 and over [MeSH Terms])) OR (elderly [Title/Abstract])) OR (older adult [Title/Abstract])) OR (older people [Title/Abstract]))) AND ((((((Cost [Title/Abstract]) OR (costs [Title/Abstract])) OR (cost analysis [Title/Abstract])) OR (cost analyses [Title/Abstract])) OR (cost evaluation [Title/Abstract])) OR (economic evaluation [Title/Abstract]))) AND ((((((Intervention [MeSH Terms]) OR (action [MeSH Terms])) OR (general practitioner [MeSH Terms])) OR (clinician [MeSH Terms])) OR (physician [MeSH Terms])) OR (patient [MeSH Terms])) |
| Search Strategy Performed in Embase |
| (‘inappropriate prescribing’:ab,ti OR ‘appropriate prescribing’:ab,ti OR ‘high-risk medications’:ab,ti OR ‘suboptimal prescribing’:ab,ti OR ‘over-prescribing’:ab,ti OR ‘under-prescribing’:ab,ti OR ‘misprescribing’:ab,ti OR ‘inappropriate drug’:ab,ti OR ‘inappropriate drugs’:ab,ti OR ‘inappropriate medication’:ab,ti OR ‘inappropriate medications’:ab,ti OR ‘inappropriate medicines’:ab,ti OR ‘inappropriate prescription’:ab,ti OR ‘inappropriate prescriptions’:ab,ti OR ‘inappropriate use’:ab,ti OR ‘medication appropriateness’:ab,ti OR ‘pharmacological inappropriateness’:ab,ti OR ‘potential drug therapy problems’:ab,ti OR ‘potentially harmful medications’:ab,ti OR ‘prescribing appropriateness’:ab,ti) AND (‘aged’/exp OR ‘aged 65 over’ OR ‘elderly’:ab,ti OR ‘older adult’:ab,ti) AND (‘cost’:ab,ti OR ‘costs’:ab,ti OR ‘cost analysis’:ab,ti OR ‘cost analyses’:ab,ti OR ‘cost evaluation’:ab,ti OR ‘economic evaluation’:ab,ti) AND (‘intervention’/exp OR ‘action’/exp OR ‘general practitioner’/exp OR ‘clinician’/exp OR ‘physician’/exp OR ‘patient’/exp) AND [embase]/lim |
| Author (Year) | Country | Study Design | GRADE Score |
|---|---|---|---|
| Pagès A. et al. (2020) [9] | France | Cross-sectional study | High ⨁⨁⨁⨁ |
| Clark C.M. et al. (2020) [10] | USA | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Sattayalertyanyong O. et al. (2020) [11] | Thailand | Prospective study | High ⨁⨁⨁⨁ |
| Rahel S. et al. (2019) [12] | Switzerland | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Feng X. et al. (2019) [13] | USA | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Tachi T. et al. (2019) [14] | Japan | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Shah K. et al. (2016) [15] | India | Cross-sectional study | High ⨁⨁⨁⨁ |
| Ladd A.M. et al. (2014) [16] | USA | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Blozik E. et al. (2013) [17] | Switzerland | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Dionne P.-A. et al. (2013) [18] | Canada | Retrospective cohort study | High ⨁⨁⨁⨁ |
| Bradley M.C. et al. (2012) [19] | Northern Ireland | Cross-sectional study | High ⨁⨁⨁⨁ |
| Cahir C. et al. (2010) [20] | Ireland | Retrospective national population study | High ⨁⨁⨁⨁ |
| Desborough J.A. et al. (2020) [21] | England | Cluster randomized controlled trial | High ⨁⨁⨁⨁ |
| Leguelinel-Blache G. et al. (2020) [22] | France | Monocentric before–after pilot and paired study | High ⨁⨁⨁⨁ |
| Whitman A. et al. (2018) [23] | Germany | Pilot study | Moderate ⨁⨁⨁◯ |
| Kim S.J. et al. (2018) [24] | Republic of Korea | Interrupted time-series study design | High ⨁⨁⨁⨁ |
| Christensen D.B. et al. (2007) [25] | USA | Before/after design with two control groups | High ⨁⨁⨁⨁ |
| Foubert K. et al. (2020) [26] | Belgium | Prospective observational study | High ⨁⨁⨁⨁ |
| Fischer K.E. et al. (2018) [27] | Germany | Prospective observational study | High ⨁⨁⨁⨁ |
| Reeve E. et al. (2015) [28] | Australia | Prospective feasibility study | High ⨁⨁⨁⨁ |
References
- United Nations Department of Economic and Social Affairs, Population Division. World Population Ageing. Highlights: Living Arrangements of Older Persons (ST/ESA/SER.A/451). 2020. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd-2020_world_population_ageing_highlights.pdf (accessed on 31 July 2021).
- Salive, M.E. Multimorbidity in older adults. Epidemiol. Rev. 2013, 35, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Mekonnen, A.B.; Redley, B.; de Courten, B.; Manias, E. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br. J. Clin. Pharmacol. 2021, 87, 4150–4172. [Google Scholar] [CrossRef]
- Cadogan, C.A.; Ryan, C.; Hughes, C.M. Appropriate Polypharmacy and Medicine Safety: When Many is not Too Many. Drug Saf. 2015, 39, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Promoting Rational Use of Medicines: Core Components; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Aronson, J.K. Rational prescribing, appropriate prescribing. Br. J. Clin. Pharmacol. 2004, 57, 229–230. [Google Scholar] [CrossRef] [Green Version]
- Buetow, S.A.; Sibbald, B.; Cantrill, J.A.; Halliwell, S. Appropriateness in health care: Application to prescribing. Soc. Sci. Med. 1997, 45, 261–271. [Google Scholar] [CrossRef]
- Pagès, A.; Mazon, M.; Cool, C.; McCambridge, C.; Cestac, P.; Rouch, L.; Juillard-Condat, B. Cost analysis of potentially inappropriate medication in older hospitalized patients. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.M.; Shaver, A.L.; Aurelio, L.A.; Feuerstein, S.; Wahler, R.G.; Daly, C.J.; Jacobs, D.M. Potentially Inappropriate Medications Are Associated with Increased Healthcare Utilization and Costs. J. Am. Geriatr. Soc. 2020, 68, 2542–2550. [Google Scholar] [CrossRef]
- Sattayalertyanyong, O.; Thitilertdecha, P.; Auesomwang, C. The inappropriate use of proton pump inhibitors during admission and after discharge: A prospective cross-sectional study. Int. J. Clin. Pharm. 2020, 42, 174–183. [Google Scholar] [CrossRef]
- Schneider, R.; Reinau, D.; Schur, N.; Blozik, E.; Früh, M.; Signorell, A.; Meier, C.R.; Schwenkglenks, M. Drug prescription patterns, polypharmacy and potentially inappropriate medication in Swiss nursing homes: A descriptive analysis based on claims data. Swiss Med. Wkly. 2019, 149, w20126. [Google Scholar] [CrossRef] [PubMed]
- Feng, X.; Higa, G.M.; Safarudin, F.; Sambamoorthi, U.; Tan, X. Potentially inappropriate medication use and associated healthcare utilization and costs among older adults with colorectal, breast, and prostate cancers. J. Geriatr. Oncol. 2019, 10, 698–704. [Google Scholar] [CrossRef] [PubMed]
- Tachi, T.; Kanematsu, Y.; Aoyama, S.; Katsuno, H.; Otsubo, M.; Ueno, A.; Sugita, I.; Yoshida, A.; Noguchi, Y.; Yasuda, M.; et al. Analysis of Adverse Reactions Caused by Potentially Inappropriate Prescriptions and Related Medical Costs That Are Avoidable Using the Beers Criteria: The Japanese Version and Guidelines for Medical Treatment and Its Safety in the Elderly 2015. Biol. Pharm. Bull. 2019, 42, 712–720. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.N.; Joshi, H.M.; Christian, R.P.; Patel, K.P.; Malhotra, S.D. Prevalence of potentially inappropriate medications and prescription cost analysis among older cardiac patients in an outpatient department of a tertiary care hospital in India. J. Basic Clin. Pharm. 2016, 7, 110–115. [Google Scholar] [PubMed] [Green Version]
- Ladd, A.M.; Panagopoulos, G.; Cohen, J.; Mar, N.; Graham, R. Potential costs of inappropriate use of proton pump inhibitors. Am. J. Med. Sci. 2014, 347, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Blozik, E.; Rapold, R.; von Overbeck, J.; Reich, O. Polypharmacy and potentially inappropriate medication in the adult, community-dwelling population in Switzerland. Drugs Aging. 2013, 30, 561–568. [Google Scholar] [CrossRef]
- Dionne, P.A.; Vasiliadis, H.M.; Latimer, E.; Berbiche, D.; Preville, M. Economic impact of inappropriate benzodiazepine prescribing and related drug interactions among elderly persons. Psychiatr. Serv. 2013, 64, 331–338. [Google Scholar] [CrossRef]
- Bradley, M.C.; Fahey, T.; Cahir, C.; Bennett, K.; O’Reilly, D.; Parsons, C.; Hughes, C.M. Potentially inappropriate prescribing and cost outcomes for older people: A cross-sectional study using the Northern Ireland Enhanced Prescribing Database. Eur. J. Clin. Pharmacol. 2012, 68, 1425–1433. [Google Scholar] [CrossRef]
- Cahir, C.; Fahey, T.; Teeling, M.; Teljeur, C.; Feely, J.; Bennett, K. Potentially inappropriate prescribing and cost outcomes for older people: A national population study. Br. J. Clin. Pharmacol. 2010, 69, 543–552. [Google Scholar] [CrossRef] [Green Version]
- Desborough, J.A.; Clark, A.; Houghton, J.; Sach, T.; Shaw, V.; Kirthisingha, V.; Holland, R.C.; Wright, D.J. Clinical and cost effectiveness of a multi-professional medication reviews in care homes (CAREMED). Int. J. Pharm. Pract. 2020, 28, 626–634. [Google Scholar] [CrossRef]
- Leguelinel-Blache, G.; Castelli, C.; Rolain, J.; Bouvet, S.; Chkair, S.; Kabani, S.; Jalabert, B.; Rouvière, S.; Choukroun, C.; Richard, H.; et al. Impact of pharmacist-led multidisciplinary medication review on the safety and medication cost of the elderly people living in a nursing home: A before-after study. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 481–490. [Google Scholar] [CrossRef]
- Whitman, A.; DeGregory, K.; Morris, A.; Mohile, S.; Ramsdale, E. Pharmacist-led medication assessment and deprescribing intervention for older adults with cancer and polypharmacy: A pilot study. Support Care Cancer 2018, 26, 4105–4113. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Han, K.T.; Kang, H.G.; Park, E.C. Toward safer prescribing: Evaluation of a prospective drug utilization review system on inappropriate prescriptions, prescribing patterns, and adverse drug events and related health expenditure in South Korea. Public Health 2018, 163, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Christensen, D.B.; Roth, M.; Trygstad, T.; Byrd, J. Evaluation of a pilot medication therapy management project within the North Carolina State Health Plan. J. Am. Pharm. Assoc. 2007, 47, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Foubert, K.; Muylaert, P.; Mehuys, E.; Somers, A.; Petrovic, M.; Boussery, K. Application of the GheOP3S-tool in nursing home residents: Acceptance and implementation of pharmacist recommendations. Acta Clin. Belg. 2020, 75, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.E.; Koch, T.; Kostev, K.; Stargardt, T. The impact of physician-level drug budgets on prescribing behavior. Eur. J. Health Econ. 2018, 19, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Reeve, E.; Andrews, J.M.; Wiese, M.D.; Hendrix, I.; Roberts, M.S.; Shakib, S. Feasibility of a patient-centered deprescribing process to reduce inappropriate use of proton pump inhibitors. Ann. Pharmacother. 2015, 49, 29–38. [Google Scholar] [CrossRef]
- Casula, M.; Menditto, E.; Galimberti, F.; Russo, V.; Olmastroni, E.; Scotti, L.; Tragni, E. A pragmatic controlled trial to improve the appropriate prescription of drugs in adult outpatients: Design and rationale of the EDU. RE. DRUG study. Prim. Health Care Res. Dev. 2020, 21, E23. [Google Scholar] [CrossRef]
- Russo, V.; Orlando, V.; Monetti, V.M.; Galimberti, F.; Casula, M.; Olmastroni, E.; Tragni, E.; Menditto, E.; EDU.RE.DRUG Group. Geographical Variation in Medication Prescriptions: A Multiregional Drug-Utilization Study. Front. Pharmacol. 2020, 11, 418. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Re-porting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef]
- Jano, E.; Aparasu, R.R. Healthcare outcomes associated with beers’criteria: A systematic review. Ann. Pharmacother. 2007, 41, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Hyttinen, V.; Jyrkkä, J.; Valtonen, H. A systematic review of the impact of potentially inappropriate medication on health care utilization and costs among older adults. Med. Care 2016, 54, 950–964. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.X.; Zhu, C.; Liang, H.Y.; Wang, K.; Chu, Y.Q.; Zhao, L.B.; Jiang, C.; Wang, Y.Q.; Yan, S.Y. Associations Between Potentially Inappropriate Medications and Adverse Health Outcomes in the Elderly: A Systematic Review and Meta-analysis. Ann. Pharmacother. 2019, 53, 1005–1019. [Google Scholar] [CrossRef] [PubMed]
- Muhlack, D.C.; Hoppe, L.K.; Weberpals, J.; Brenner, H.; Schöttker, B. The association of potentially inappropriate medication at older age with cardiovascular events and overall mortality: A systematic review and meta-analysis of cohort studies. J. Am. Med. Dir. Assoc. 2017, 18, 211–220. [Google Scholar] [CrossRef]
- Liew, T.M.; Lee, C.S.; Goh, S.K.L.; Chang, Z.Y. The prevalence and impact of potentially inappropriate prescribing among older persons in primary care settings: Multilevel meta-analysis. Age Ageing 2020, 49, 570–579. [Google Scholar] [CrossRef]
- Liew, T.M.; Lee, C.S.; Goh Shawn, K.L.; Chang, Z.Y. Potentially inappropriate prescribing among older persons: A meta-analysis of observational studies. Ann. Fam. Med. 2019, 17, 257–266. [Google Scholar] [CrossRef] [Green Version]
- Malakouti, S.K.; Javan-Noughabi, J.; Yousefzadeh, N.; Rezapour, A.; Mortazavi, S.S.; Jahangiri, R.; Moghri, J. A Systematic Review of Potentially Inappropriate Medications Use and Related Costs Among the Elderly. Value Health Reg. Issues 2021, 25, 172–179. [Google Scholar] [CrossRef]
- Ridde, V.; Pérez, D.; Robert, E. Using implementation science theories and frameworks in global health. BMJ Glob. Health 2020, 5, e002269. [Google Scholar] [CrossRef]
- Nilsen, P. Making sense of implementation theories, models and frameworks. Implement. Sci. 2015, 10, 53. [Google Scholar] [CrossRef] [Green Version]
| Query | Keywords (in Mesh/Emtree OR Title and Abstract) | Number of Records | |
|---|---|---|---|
| Pubmed/Medline | Embase | ||
| #1 | Inappropriate prescribing OR Appropriate Prescribing OR High-risk medications OR Suboptimal prescribing OR Over-prescribing OR Under-prescribing OR Misprescribing OR Inappropriate Drug OR Inappropriate Medication OR Inappropriate Medicines OR Inappropriate Prescription OR Inappropriate Use OR Medication Appropriateness OR Pharmacological Inappropriateness OR Potential Drug Therapy Problems OR Potentially Harmful Medications OR Prescribing Appropriateness | 8946 | 12,116 |
| #2 | Aged OR Aged, 65 and over OR Elderly OR Older Adult OR Older people | 3,321,229 | 2,491,812 |
| #3 | Cost OR Cost analysis OR Cost evaluation OR Economic evaluation | 594,294 | 616,13 |
| #4 | Intervention OR Action OR General practitioner OR Physician OR Patient | 905,693 | 2,997,717 |
| #1 AND #2 AND #3 AND #4 | 51 | 223 | |
| Data Extraction | Description |
|---|---|
| Reference | All identification details of the paper |
| Year | Year of publication |
| Country | Country in which the study was carried out |
| Study Design | Type of study conducted |
| Patient (P) | Population receiving both specific and nonspecific Potentially Inappropriate Prescribing (PIPs) |
| Intervention (I) | Any type of intervention aimed at health professionals (i.e., physicians, clinicians, pharmacists, nurses), structures (i.e., nursing homes, hospitals, pharmacies), patients, or any monitoring activities of potentially inappropriate prescriptions and costs incurred use any explicit criteria for identifying inappropriateness (such as Beers Criteria, PRISCUS list, STOPP/START criteria) |
| Comparator (C) | No intervention or any other intervention and no monitoring activities |
| Outcomes (O) | The postintervention outcome in terms of costs variation and intervention effectiveness; Avoidable costs related to inappropriate prescriptions |
| Cost types | The perspective of analysis (NHS, society, government, patient) and associated costs (direct healthcare costs, direct non healthcare costs, indirect costs, intangible costs) |
| Author (Year) | Country | Study Design | Setting | Target Population | Criteria Used | PIPs Frequency | Avoidable Costs (2021 EUR Currency) | Conclusions |
|---|---|---|---|---|---|---|---|---|
| Pagès A. et al. (2020) [9] | France | Cross-sectional study | University hospital | Inpatients (n = 365) | The EU(7) -PIM List -STOPP/START Criteria | 50.4% | EUR 1449.05 per patient per year | 1. Substitution of PIPs identified with recommended alternatives was cost saving. 2. Both polypharmacy and type of ward providing care were associated with increased costs of PIMs. |
| Clark C.M. et al. (2020) [10] | USA | Retrospective cohort study | The 2011–2015 Medical Expenditure Panel Survey (MEPS) | Community-dwelling adults aged > 65 years (n = 75,135,061) | 2019 AGS Beers Criteria | 34.4% | EUR 11,628.69 per patient per year | PIMs continue to be prescribed at a high rate among older adults and are associated with increased costs. |
| Sattayalertyanyong O. et al. (2020) [11] | Thailand | Prospective study | Medicine wards | Inpatients and outpatients treated with PPIs (n = 265) | Guidelines for PPIs | 50.6% | EUR 676.18 per patient per year | PPIs are inappropriately prescribed during hospital admission and after discharge, associated with high costs |
| Rahel S. et al. (2019) [12] | Switzerland | Retrospective cohort study | Nursing homes | Patients aged ≥ 65 years (NHR = 91,166; individuals = 1,364,755) | 2015 Beers criteria and the PRISCUS list | 79.1% | EUR 597.19 per patient per year | 1. Polypharmacy and PIMs are frequent and associated with poor health outcomes in older adults. 2. Drug costs constitute a minor part of the total healthcare costs of these patients. |
| Feng X. et al. (2019) [13] | USA | Retrospective cohort study | The SEER-Medicare linked database | Older adults with breast (n = 17,630), prostate (n = 18,721), or colorectal (n = 9420) cancer | 2015 Beers Criteria | -Breast cancer: 61.7% -Prostate cancer: 47.3% -Colorectal cancer: 66.3% | -Breast cancer: EUR 8288.18 per patient per year -Prostate cancer: EUR 7773.14 per patient per year -Colorectal cancer: EUR 44,258.17 per patient per year | PIMs use was significantly associated with greater healthcare utilization and higher healthcare costs in cancer patients |
| Tachi T. et al. (2019) [14] | Japan | Retrospective cohort study | Hospital | Inpatients and outpatients aged ≥ 65 years (inpatients = 1236; outpatients = 980) | -Japanese Version (BCJV) -Guidelines for Medical treatment and Its Safety in the Elderly 2015 (GL2015) | -Inpatients BCJV: 24.0%; GL2015: 72.0% -Outpatients BCJV: 26.2%; GL2015: 59.9% | -Inpatients EUR 240.55 per patient per year -Outpatients EUR 18.66 per patient per year | Appropriate use of drugs based on Beers Criteria reduces ADRs and associated costs |
| Shah K. et al. (2016) [15] | India | Cross-sectional study | Cardiology outpatient department | Patients aged ≥ 65 years (n = 236) | 2012 Beers criteria | 29.3% | EUR 162.76 per patient per year | The high prevalence of PIMs was associated with increased costs in older patients suffering from cardiac diseases |
| Ladd A.M. et al. (2014) [16] | USA | Retrospective cohort study | Urban hospital | Inpatients and outpatients treated with PPIs (n = 2094) | Guidelines for PPIs | 76.0% | EUR 2425.34 per patient per year | PPIs are overused in the majority of hospitalized patients with low risk for gastrointestinal bleeding and are associated with high healthcare costs |
| Blozik E. et al. (2013) [17] | Switzerland | Retrospective cohort study | Community-dwelling population | Beneficiaries of health service (n = 5000) | -2003 Beers criteria -PRISCUS list. | 21.0% | EUR 1861.77 per patient per year | 1. The prevalence of polypharmacy and PIMs in the adult and elderly was high; 2. The elderly were associated with higher costs |
| Dionne P.-A. et al. (2013) [18] | Canada | Retrospective cohort study | Community-dwelling population | Beneficiaries of health service aged ≥ 65 years (n = 744) | 2003 Beers criteria | 44.0% | EUR 2567.67 per patient per year | A significant association between benzodiazepine-related drug interactions and healthcare costs. |
| Bradley M.C. et al. (2012) [19] | Northern Ireland | Cross-sectional study | Hospital | Patients aged ≥ 70 years (n = 166,108) | -STOPP criteria -Beers criteria | 34% | EUR 36.71 per patient per year | The prevalence of PIP was high among the study cohort, increased with polypharmacy, and was associated with a significant cost. |
| Cahir C. et al. (2010) [20] | Ireland | Retrospective national population study | Geriatric units, nursing homes and hospitals | Patients aged ≥ 70 years (n = 338,801) | 2007 STOPP criteria | 36% | EUR 134.68 per patient per year | The findings identify a high prevalence of PIP in Ireland with significant cost consequences. |
| Author (Year) | Country | Study Design | Intervention Aim | Time Frame | Setting | Target Population | Intervention | Outcome | Avoidable Costs (2021 EUR Currency) | Conclusions |
|---|---|---|---|---|---|---|---|---|---|---|
| Trials | ||||||||||
| Desborough J.A. et al. (2020) [21] | England | Cluster randomized controlled trial | To determine the clinical cost-effectiveness of multiprofessional medication review service (MPMR). | 1 year | Care homes | Care home medical staff (n = 826) | Intervention care homes received an MPMR from a team consisting of a clinical pharmacist, GP, and a care home member. | 1. Intervention reduced PIMs by 20% at 12 months 2. Intervention group had higher costs and falls per person per year. | / | The intervention was dominated by usual care and would not be considered cost-effective. |
| Leguelinel-Blache G. et al. (2020) [22] | France | Monocentric before-after pilot and paired study | To assess the impact of multidisciplinary medication review (MMR) and costs incurred by the hospital and the national health service. | 1 year | Nursing homes | -Nurses -GPs (n = 49) | Two hospital pharmacists, using different criteria, reviewed patients’ prescriptions and conducted multidisciplinary meetings suggesting modifications to the patients’ medical team. | The number of patients taking at least one PIMs decreased from 30.6% before to 6.1% after the intervention. | EUR 232.00 per patient per year | The MMR reduced the iatrogenic drug risk for elderly residents and costs from the nursing home perspective, particularly drug expenditure. |
| Whitman A. et al. (2018) [23] | Germany | Pilot study | 1. To compare the application of three geriatric medication screening tools to the Beers Criteria alone for PIM quantification 2. To determine the feasibility of a pharmacist-led polypharmacy assessment. | 9 months | Ambulatory care clinic | -Geriatric oncologist -Patient -Caregiver (n = 26) | 1. Pharmacist performed an assessment of all drug therapies by reviewing all PIPs through different criteria 2. Reduction in prescribing occurred after a discussion with a pharmacist, oncologist, patient, or caregiver. | After the application of the three-tool assessment, 73% of PIMs identified were deprescribed, resulting in a mean of 3 medications deprescribed per patient. | EUR 872.69 per patient per year | 1. The three-tool assessment identified 3 times more PIMs than the Beers Criteria alone. 2. Pharmacist-led deprescribing interventions were feasible, leading to improved patient outcomes and cost savings. |
| Kim S.J. et al. (2018) [24] | Republic of Korea | Interrupted time-series study design | To evaluate the effect of the prospective drug utilization review (DUR) system to improve prescribing practices, adverse drug events (ADEs), and healthcare expenditure. | Rolling 6-year period | Outpatient | Patients with musculoskeletal or connective tissue disorders (n = 54,58) | Introduction of DUR systems for monitoring drugs’ prescription operating prospectively and retrospectively, providing feedback to the provider. | More efficient prescribing, reduction in DDIs, and increase in the use of gastro-protective drugs. | / | The intervention had a positive effect on patient outcomes but was not associated with reduced ADE-related costs. |
| Christensen D.B. et al. (2007) [25] | USA | Before/after design with two control groups | To assess the feasibility of a pharmacist-based Medication Therapy Management (MTM) service. | 8 months | -Community pharmacies -Ambulatory care clinic | -Community and Ambulatory care Pharmacists -Volunteering patients (n = 1000) | 1. Educational training for pharmacists 2. MTM-type program offered to patients with polytherapy | 1. Pharmacists identified an average of 3.6 potential drug therapy problems (PDTPs) per patient at the first visit. 2. Pharmacists recommended a drug therapy change in about 50% of patients and contacted the prescriber more than 85% of the time. 3. No significant differences were observed in patient co-payment or insurer prescription costs. | / | 1. The intervention reduced the number of potential drug therapy problems 2. The intervention did not necessarily result in reductions in prescription drug use or cost. |
| Observational studies | ||||||||||
| Foubert K. et al. (2020) [26] | Belgium | Prospective observational study | To investigate the acceptance of pharmacist recommendations based on a screening tool for PIP: Ghent Older People’s Prescriptions community Pharmacy Screening (GheOP3S)-tool. | 5 months | Nursing homes | -Pharmacists -GPs -Nurse (n = 50) | 1. Collection of the medication list for each patient 2. Lists’ screening using the GheOP3 S-tool and formulation of recommendations for every detected GheOP3 S-criterion 3. Face-to-face pharmacist-GP meetings to discuss the pharmacist recommendations, resulting in an agreed action plan 4. Final meeting between the pharmacist, head nurses, and coordinating physician to communicate these plans. | 1. Most pharmacist recommendations on PIP considered stopping the medication 2. The 45% of relevant recommendations were accepted by the GPs 3. Number of GheOP3S-criteria and medication costs remained unchanged | / | The acceptance and implementation of pharmacist recommendations were relatively low |
| Fischer K.E. et al. (2018) [27] | Germany | Prospective observational study | To analyze costs and quality of prescribing conditional on the level of utilization of the drug budget | 7 years | Outpatient | Physicians (n = 440) | drug-budgets introduction and motoring of Drug Budget for Physicians, the level of drug budget utilization, and differentiation by varying levels of enforcement where physicians overspent their budgets. | The level of drug budget utilization influences the cost and quality of prescribing PIMs to the elderly. | / | 1. Drug use expressed as the number of prescriptions per visit had not changed 2. The cost of prescribing changed when a drug budget mechanism was put in place |
| Reeve E. et al. (2015) [28] | Australia | Prospective feasibility study | To assess the feasibility of a patient-centered deprescribing process | 6 months | Hospital outpatient clinics | -GPs -Patients (n = 43) | 1. Identification of PPIs by Pharmacists 2. Determine if the medication can be discontinued by GPs 3. Withdrawal of PPI. | Of the eight participants who were invited to have their PPI withdrawn, six were willing to undergo trial withdrawal, and all achieved cessation/dose reduction. | / | 1. The patient-centered deprescribing process can safely reduce inappropriate PPI prescribing 2. Cost-effectiveness of this approach needs to be determined |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mucherino, S.; Casula, M.; Galimberti, F.; Guarino, I.; Olmastroni, E.; Tragni, E.; Orlando, V.; Menditto, E.; on behalf of the EDU.RE.DRUG Group. The Effectiveness of Interventions to Evaluate and Reduce Healthcare Costs of Potentially Inappropriate Prescriptions among the Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 6724. https://doi.org/10.3390/ijerph19116724
Mucherino S, Casula M, Galimberti F, Guarino I, Olmastroni E, Tragni E, Orlando V, Menditto E, on behalf of the EDU.RE.DRUG Group. The Effectiveness of Interventions to Evaluate and Reduce Healthcare Costs of Potentially Inappropriate Prescriptions among the Older Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(11):6724. https://doi.org/10.3390/ijerph19116724
Chicago/Turabian StyleMucherino, Sara, Manuela Casula, Federica Galimberti, Ilaria Guarino, Elena Olmastroni, Elena Tragni, Valentina Orlando, Enrica Menditto, and on behalf of the EDU.RE.DRUG Group. 2022. "The Effectiveness of Interventions to Evaluate and Reduce Healthcare Costs of Potentially Inappropriate Prescriptions among the Older Adults: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 11: 6724. https://doi.org/10.3390/ijerph19116724
APA StyleMucherino, S., Casula, M., Galimberti, F., Guarino, I., Olmastroni, E., Tragni, E., Orlando, V., Menditto, E., & on behalf of the EDU.RE.DRUG Group. (2022). The Effectiveness of Interventions to Evaluate and Reduce Healthcare Costs of Potentially Inappropriate Prescriptions among the Older Adults: A Systematic Review. International Journal of Environmental Research and Public Health, 19(11), 6724. https://doi.org/10.3390/ijerph19116724