
Income Disparity and Mental Wellbeing among Adults in Semi-Urban and Rural Areas in Malaysia: The Mediating Role of Social Capital

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Instrument
2.3. Explanatory Variables
Monthly Household Income
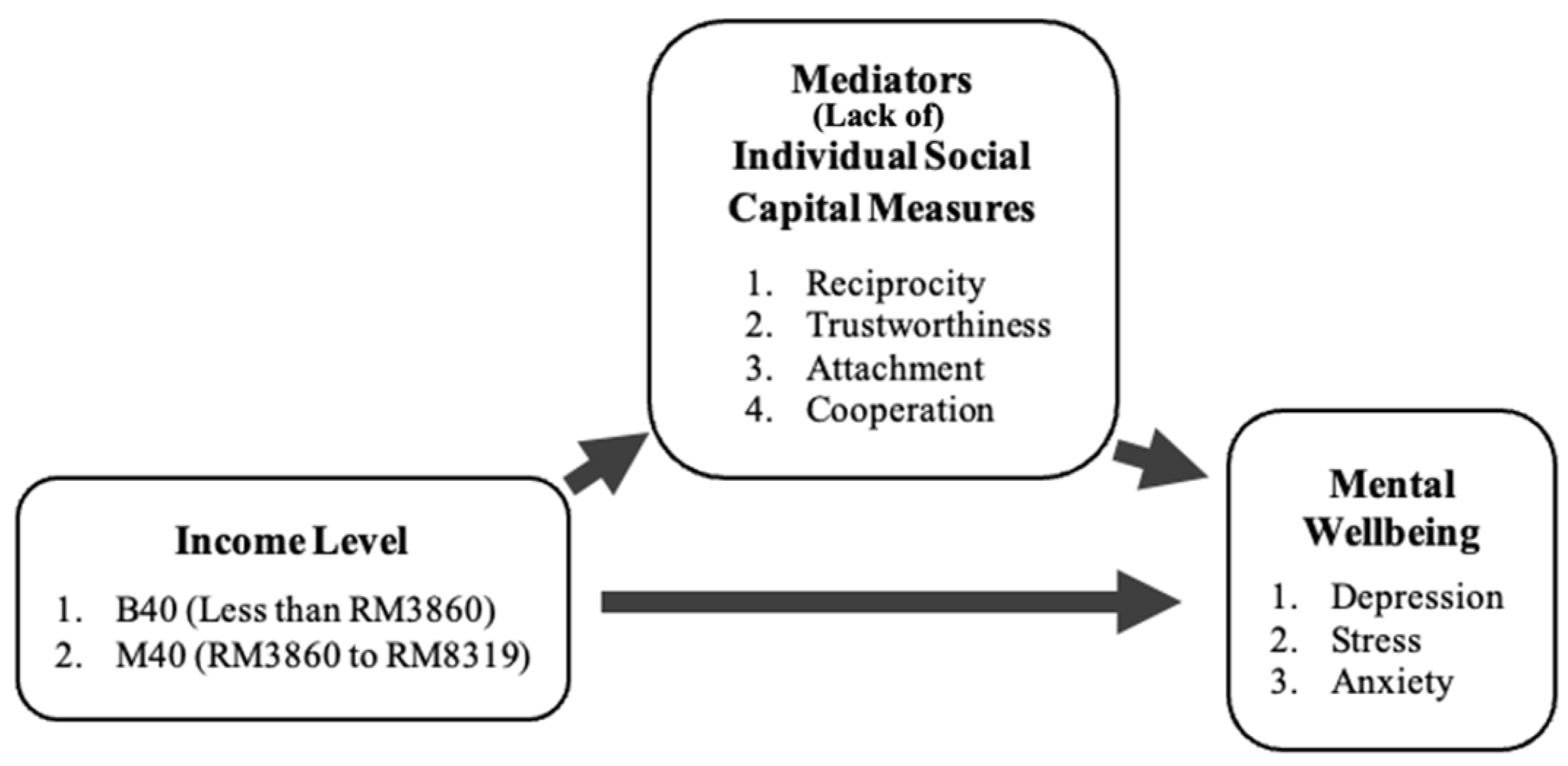
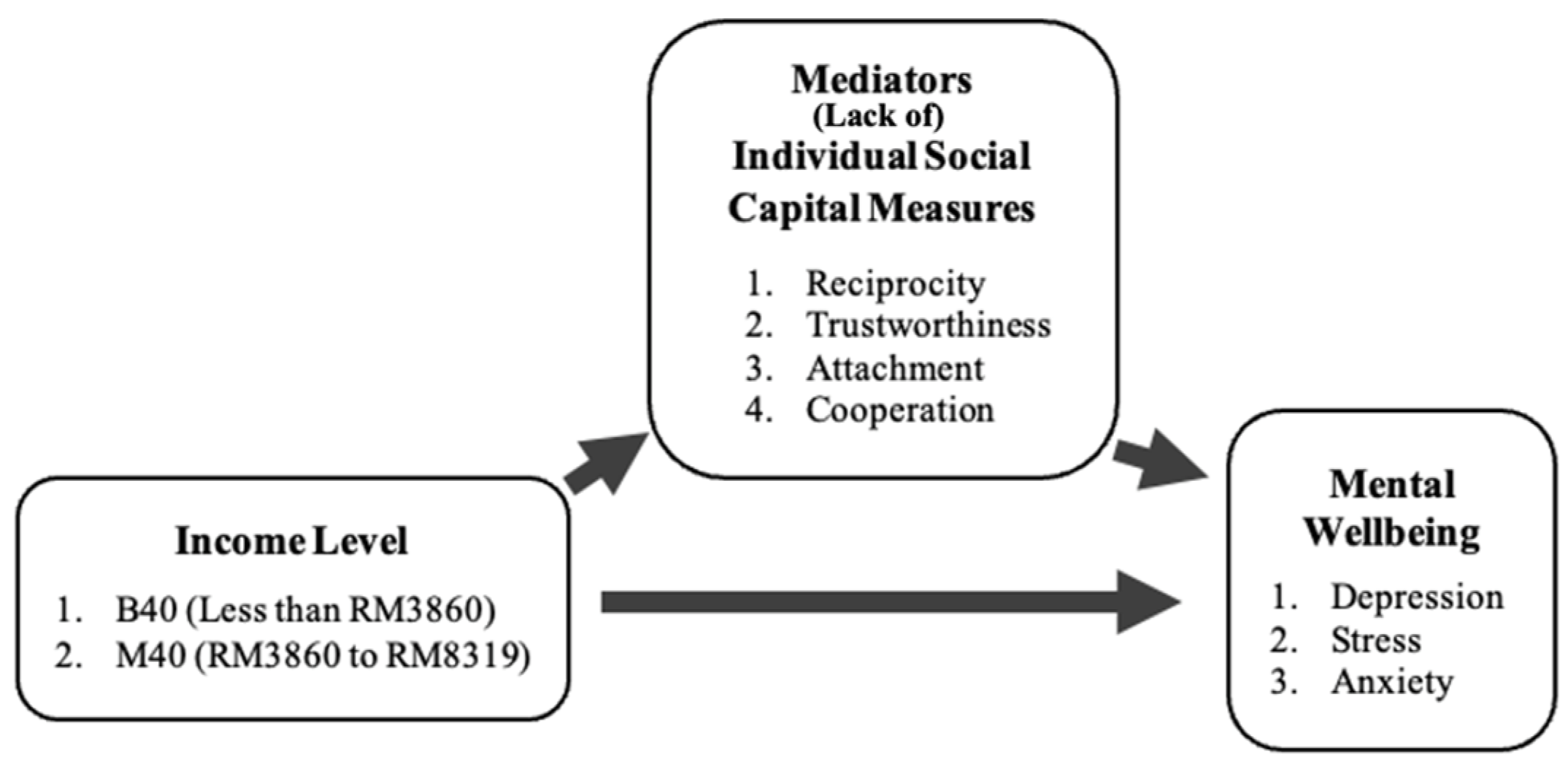
2.4. Mediators
2.4.1. Individual Social Capital Measure
2.4.2. Control Variables
2.5. Statistical Analysis
3. Results
Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Characteristics | Stress | Chi-Square | Anxiety | Chi-Square | Depression | Chi-Square | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal | Mild, Moderate, Severe, and Extremely Severe | Normal | Mild, Moderate, Severe, and Extremely Severe | Normal | Mild, Moderate, Severe, and Extremely Severe | |||||
| Ethnicity | Malay | 3849 94.40% | 230 5.60% | 32.6 *** | 3103 75.90% | 987 24.10% | 22.3 *** | 3441 84.10% | 649 15.90% | 8.36 ** |
| Indian | 461 88.80% | 58 11.20% | 404 77.70% | 116 22.30% | 415 79.70% | 106 20.30% | ||||
| Chinese | 1768 91.50% | 164 8.50% | 1570 81.10% | 365 18.90% | 1602 83.00% | 328 17.00% | ||||
| Others | 53 94.60% | 3 5.40% | 47 83.90% | 9 16.10% | 49 89.10% | 6 10.90% | ||||
| Gender | Female | 3292 93.30% | 235 6.70% | 0.77 | 2737 77.5% | 794 22.5% | 0.06 | 2941 83.3% | 590 16.7% | 0.21 |
| Male | 2843 92.80% | 221 7.20% | 2391 77.8% | 684 22.2% | 2570 83.7% | 500 16.3% | ||||
| Marital status | Single | 146 88.50% | 19 11.50% | 24.3 *** | 126 76.4% | 39 23.6% | 10.1 ** | 130 79.3% | 34 20.7% | 9.53 ** |
| Married | 4585 92.50% | 371 7.50% | 3816 76.8% | 1154 23.2% | 4118 82.9% | 849 17.1% | ||||
| Separated/ divorced/Other | 95 91.30% | 9 8.70% | 81 77.9% | 23 22.1% | 90 85.7% | 15 14.3% | ||||
| Widow | 1307 95.80% | 57 4.20% | 1103 80.8% | 262 19.2% | 1171 85.9% | 192 14.1% | ||||
| Education Status | None | 351 94.1% | 22 5.9% | 164.2 *** | 314 83.7% | 61 16.3% | 34.5 *** | 322 86.8% | 49 13.2% | 48.9 *** |
| Primary | 3624 95.5% | 171 4.5% | 2949 77.5% | 857 22.5% | 3207 84.2% | 601 15.8% | ||||
| Secondary | 1548 86.8% | 236 13.2% | 1344 75.2% | 444 24.8% | 1430 80.1% | 356 19.9% | ||||
| Tertiary | 139 92.7% | 11 7.3% | 123 82.0% | 27 18.0% | 125 84.5% | 23 15.5% | ||||
| Other | 325 99.1% | 3 0.9% | 287 87.5% | 41 12.5% | 310 94.5% | 18 5.5% | ||||
| Employment Status | Housewife | 2052 95.6% | 95 4.4% | 327.0 *** | 1734 80.9% | 411 19.1% | 211.0 *** | 1860 86.4% | 293 13.6% | 273.7 *** |
| Unemployed | 1286 91.9% | 114 8.1% | 995 71.1% | 404 28.9% | 1102 78.7% | 298 21.3% | ||||
| Paid employment | 719 80.2% | 177 19.8% | 573 63.8% | 325 36.2% | 610 68.0% | 287 32.0% | ||||
| Pensioners | 841 94.2% | 52 5.8% | 752 83.6% | 148 16.4% | 803 89.4% | 95 10.6% | ||||
| Self employed | 1213 99.1% | 11 0.9% | 1048 85.7% | 175 14.3% | 1119 91.5% | 104 8.5% | ||||
| Income | B40 | 5590 93.10% | 412 6.90% | 94.3 *** | 4617 76.7% | 1400 23.3% | 19.9 *** | 5001 83.2% | 1011 16.8% | 39.5 *** |
| M40 | 55 65.50% | 29 34.50% | 47 56.0% | 37 44.0% | 48 57.1% | 36 42.9% | ||||
| Reciprocity | Agree | 4245 96.00% | 179 4.00% | 182.9 *** | 3788 85.4% | 647 14.6% | 493.4 *** | 4011 90.5% | 421 9.5% | 494.9 *** |
| Disagree or “neutral” | 1808 86.80% | 275 13.20% | 1269 60.8% | 818 39.2% | 1431 68.6% | 656 31.4% | ||||
| Cooperation among community members | Agree | 4616 96.90% | 147 3.10% | 408.3 *** | 4138 86.7% | 634 13.3% | 855.3*** | 4383 91.9% | 388 8.1% | 903.8 *** |
| Disagree or “neutral” | 1443 82.60% | 305 17.40% | 924 52.6% | 831 47.4% | 1064 60.7% | 689 39.3% | ||||
| Trust in community | Disagree or “neutral” | 4182 97.80% | 94 2.20% | 435.0 *** | 3792 88.5% | 491 11.5% | 867.8 *** | 3999 93.3% | 285 6.7% | 883.0 *** |
| Agree | 1860 83.90% | 356 16.10% | 1254 56.4% | 969 43.6% | 1432 64.5% | 788 35.5% | ||||
| Attached to local community | Disagree or “neutral” | 4095 98.30% | 70 1.70% | 466.3 *** | 3709 88.90% | 461 11.10% | 835.7 *** | 3925 94.1% | 247 5.9% | 914.5 *** |
| Agree | 1970 84.40% | 365 15.60% | 1357 57.9% | 986 42.1% | 1526 65.2% | 813 34.8% | ||||
References
- Sagar, R.; Dandona, R.; Gururaj, G.; Dhaliwal, R.; Singh, A.; Ferrari, A.; Dua, T.; Ganguli, A.; Varghese, M.; Chakma, J. The burden of mental disorders across the states of India: The global burden of disease study 1990–2017. Lancet Psychiatry 2020, 7, 148–161. [Google Scholar] [CrossRef] [Green Version]
- Baingana, F.; Al’Absi, M.; Becker, A.E.; Pringle, B. Global research challenges and opportunities for mental health and substance-use disorders. Nature 2015, 527, S172–S177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. COVID-19 Pandemic Triggers 25% Increase in Prevalence of Anxiety and Depression Worldwide. World Health Organization, 2022. Available online: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (accessed on 29 April 2022).
- Lewis, G.; Hayes, J.J.L.P. Common mental disorders: Falling through the gap. Lancet Psychiatry 2019, 6, 636–637. [Google Scholar] [CrossRef]
- Patel, V.; Kleinman, A.W.H.O. Poverty and common mental disorders in developing countries. Bull. World Health Organ. 2003, 81, 609–615. [Google Scholar] [PubMed]
- Araya, R.; Lewis, G.; Rojas, G.; Fritsch, R. Education and income: Which is more important for mental health? J. Epidemiol. Community Health 2003, 57, 501–505. [Google Scholar] [CrossRef] [Green Version]
- Lund, C.; Brooke-Sumner, C.; Baingana, F.; Baron, E.C.; Breuer, E.; Chandra, P.; Haushofer, J.; Herrman, H.; Jordans, M.; Kieling, C.; et al. Social determinants of mental disorders and the Sustainable Development Goals: A systematic review of reviews. Lancet Psychiatry 2018, 5, 357–369. [Google Scholar] [CrossRef]
- Paananen, R.; Ristikari, T.; Merikukka, M.; Gissler, M. Social determinants of mental health: A Finnish nationwide follow-up study on mental disorders. J. Epidemiol Community Health 2013, 67, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Golberstein, E.J. The effects of income on mental health: Evidence from the social security notch. J. Ment. Health Policy Econ. 2015, 18, 27. [Google Scholar]
- Du, W.; Zhou, J.; Liu, J.; Yang, X.; Wang, H.; He, M.; Mao, Z.; Liu, X.J.S. Social-demographic correlates of the mental health conditions among the Chinese elderly. Sustainability 2019, 11, 7114. [Google Scholar] [CrossRef] [Green Version]
- Williams, L.; Zhang, R.; Packard, K. Factors affecting the physical and mental health of older adults in China: The importance of marital status, child proximity, and gender. SSM Popul. Health 2017, 3, 20–36. [Google Scholar] [CrossRef]
- Sareen, J.; Afifi, T.O.; McMillan, K.A.; Asmundson, G. Relationship between household income and mental disorders: Findings from a population-based longitudinal study. JAMA Psychiatry 2011, 68, 419–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorant, V.; Deliège, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Am. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, I. Poverty and Mental Health: A review to Inform the Joseph Rowntree Foundation’s Anti-Poverty Strategy; Mental Health Foundation: London, UK, 2016; pp. 1–110. [Google Scholar]
- Hakulinen, C.; Elovainio, M.; Arffman, M.; Lumme, S.; Pirkola, S.; Keskimäki, I.; Manderbacka, K.; Böckerman, P. Mental disorders and long-term labour market outcomes: Nationwide cohort study of 2055720 individuals. Acta Psychiatr. Scand. 2019, 140, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Mojtabai, R.; Stuart, E.A.; Hwang, I.; Susukida, R.; Eaton, W.W.; Sampson, N.; Kessler, R. Long-term effects of mental disorders on employment in the National Comorbidity Survey ten-year follow-up. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1657–1668. [Google Scholar] [CrossRef] [Green Version]
- Andrade, L.; Caraveo-Anduaga, J.J.; Berglund, P.; Bijl, R.V.; De Graaf, R.; Vollebergh, W.; Dragomirecka, E.; Kohn, R.; Keller, M.; Kessler, R.C.; et al. The epidemiology of major depressive episodes: Results from the International Consortium of Psychiatric Epidemiology (ICPE) Surveys. Int. J. Methods Psychiatr. Res. 2003, 12, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Ridley, M.W.; Rao, G.; Schilbach, F.; Patel, V.H. Poverty, depression, and anxiety: Causal evidence and mechanisms. Natl. Bur. Econ. Res. 2020, 370, eaay0214. [Google Scholar]
- Domènech-Abella, J.; Mundó, J.; Leonardi, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Ayuso-Mateos, J.L.; Haro, J.M. The association between socioeconomic status and depression among older adults in Finland, Poland and Spain: A comparative cross-sectional study of distinct measures and pathways. J. Affect. Disord. 2018, 241, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Layte, R. The association between income inequality and mental health: Testing status anxiety, social capital, and neo-materialist explanations. Eur. Sociol. Rev. 2011, 28, 498–511. [Google Scholar] [CrossRef]
- Ribeiro, W.S.; Bauer, A.; Andrade, M.C.R.; York-Smith, M.; Pan, P.M.; Pingani, L.; Knapp, M.; Coutinho, E.S.F.; Evans-Lacko, S. Income inequality and mental illness-related morbidity and resilience: A systematic review and meta-analysis. Lancet 2017, 4, 554–562. [Google Scholar] [CrossRef]
- Prince, M.J.; Harwood, R.H.; Blizard, R.A.; Thomas, A.; Mann, A.H. Social support deficits, loneliness and life events as risk factors for depression in old age. The Gospel Oak Project VI. Psychol. Med. 1997, 27, 323–332. [Google Scholar] [CrossRef]
- Kim, J.M.; Stewart, R.; Shin, I.S.; Yoon, J.S.; Lee, H.Y. Lifetime urban/rural residence, social support and late-life depression in Korea. Int. J. Geriatr. Psychiatry 2004, 19, 843–851. [Google Scholar] [CrossRef]
- Harris, T.; Cook, D.G.; Victor, C.; Rink, E.; Mann, A.H.; Shah, S.; DeWilde, S.; Beighton, C.J.A. Predictors of depressive symptoms in older people—A survey of two general practice populations. Ageing 2003, 32, 510–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, H.; Yue, Z.; Liu, E.; Xiang, N. How does social capital affect individual health among the elderly in rural China? Mediating effect analysis of physical exercise and positive attitude. PLoS ONE 2020, 15, e0231318. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Yeatts, D.E.; Cai, T.; Yang, P.Q.; Cready, C.M. Social capital and self-rated health among middle-aged and older adults in China: A multilevel analysis. J. Aging Res. 2014, 36, 497–521. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Liang, C.; Lucas, J.; Cheng, W.; Zhao, Z.J.S. The Influence of income and social capital on the subjective well-being of elderly Chinese people, based on a panel survey. Sustainability 2020, 12, 4786. [Google Scholar] [CrossRef]
- Muramatsu, N. County-level income inequality and depression among older Americans. Health Serv. Res. 2003, 38, 1863–1883. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Kennedy, B.P. Health and social cohesion: Why care about income inequality? BMJ 1997, 314, 1037–1040. [Google Scholar] [CrossRef]
- Partap, U.; Young, E.H.; Allotey, P.; Soyiri, I.N.; Jahan, N.; Komahan, K.; Devarajan, N.; Sandhu, M.S.; Reidpath, D.D. HDSS profile: The South East Asia Community Observatory Health and Demographic Surveillance System (SEACO HDSS). Int. J. Epidemiol. 2017, 46, 1370–1371g. [Google Scholar] [CrossRef] [Green Version]
- Musa, R.; Fadzil, M.A.; Zain, Z. Translation, validation and psychometric properties of Bahasa Malaysia version of the Depression Anxiety and Stress Scales (DASS). ASEAN J. Psychiatry 2007, 8, 82–89. [Google Scholar]
- Donovan, S.A. A Guide to Describing the Income Distribution; Congressional Research Service: Washington, DC, USA, 2015; Volume 17, p. 617. [Google Scholar]
- Goh, K.-L.; Tey, N. Personal income in Malaysia: Distribution and differentials. Econ. Bull. 2018, 38, 973–982. [Google Scholar]
- Sun, X.; Rehnberg, C.; Meng, Q.J. How are individual-level social capital and poverty associated with health equity? A study from two Chinese cities. Int. J. Equity Health 2009, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaoka, K.J.S. Social capital and health and well-being in East Asia: A population-based study. Soc. Sci. Med. 2008, 66, 885–899. [Google Scholar] [CrossRef] [PubMed]
- Aida, J.; Kondo, K.; Hirai, H.; Subramanian, S.; Murata, C.; Kondo, N.; Ichida, Y.; Shirai, K.; Osaka, K.J. Assessing the association between all-cause mortality and multiple aspects of individual social capital among the older Japanese. BMC Public Health 2011, 11, 499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieminen, T.; Martelin, T.; Koskinen, S.; Aro, H.; Alanen, E.; Hyyppä, M.T. Social capital as a determinant of self-rated health and psychological well-being. Int. J. Public Health 2010, 55, 531–542. [Google Scholar] [CrossRef]
- Kawachi, I.; Kennedy, B.P.; Glass, R. Social capital and self-rated health: A contextual analysis. Am. J. Public Health 1999, 89, 1187–1193. [Google Scholar] [CrossRef] [Green Version]
- Kohler, U.; Karlson, K.B.; Holm, A. Comparing coefficients of nested nonlinear probability models. Stata J. 2011, 11, 420–438. [Google Scholar] [CrossRef] [Green Version]
- Breen, R.; Karlson, K.B.; Holm, A. Total, direct, and indirect effects in logit and probit models. Sociol. Methods Res. 2013, 42, 164–191. [Google Scholar] [CrossRef]
- Zolkifeli, Z.; Amin, A.J. Mental health and social capital among B40 groups in east coast of peninsular Malaysia. Indian J. Public Health Res. Dev. 2019, 10, 808–812. [Google Scholar] [CrossRef]
- Zolkifeli, Z.; Amin, A.J. The effects of social capital and mental health on quality of life among low income group in urban areas in east coast of peninsula Malaysia. Int. J. Res. Eng. Technol. 2018, 9, 904–909. [Google Scholar]
- Rizal, H.; Said, M.A.; Majid, A.H.; Su, T.T.; Pin, T.M.; Ismail, R.; Shah, M.A.Z. Health-related quality of life of younger and older lower-income households in Malaysia. PLoS ONE 2022, 17, e0263751. [Google Scholar] [CrossRef]
- Tomita, A.; Burns, J.K. A multilevel analysis of association between neighborhood social capital and depression: Evidence from the first South African National Income Dynamics Study. J. Affect. Disord. 2013, 144, 101–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-S.; Chung, Y.; Perry, M.J.; Kawachi, I.; Subramanian, S.V. Association between interpersonal trust, reciprocity, and depression in South Korea: A prospective analysis. PLoS ONE 2012, 7, e30602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Insel, T.R. Assessing the economic costs of serious mental illness. Am. J. Psychiatry 2008, 165, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Haseda, M.; Kondo, N.; Takagi, D.; Kondo, K.J.H. Community social capital and inequality in depressive symptoms among older Japanese adults: A multilevel study. Health Place 2018, 52, 8–17. [Google Scholar] [CrossRef]
- Wang, R.; Chen, H.; Liu, Y.; Lu, Y.; Yao, Y. Neighborhood social reciprocity and mental health among older adults in China: The mediating effects of physical activity, social interaction, and volunteering. BMC Public Health 2019, 19, 1036. [Google Scholar] [CrossRef]
- Fyrand, L. Reciprocity: A predictor of mental health and continuity in elderly people’s relationships? A review. Curr. Gerontol. Geriatr. Res. 2010, 2010, 340161. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.; Kitchen, P. Sense of place and health in Hamilton, Ontario: A case study. Soc. Indic. Res. 2012, 108, 257–276. [Google Scholar] [CrossRef] [Green Version]
- Wind, T.R.; Fordham, M.; Komproe, I.H. Social capital and post-disaster mental health. Glob. Health Action 2011, 4, 6351. [Google Scholar] [CrossRef]
- Wind, T.R.; Joshi, P.C.; Kleber, R.J.; Komproe, I.H. The effect of the postdisaster context on the assessment of individual mental health scores. Am. J. Orthopsychiatry 2014, 84, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, T.; Natsume, K.; Okuyama, M.; Sato, T.; Kawachi, I. Do home-visit programs for mothers with infants reduce parenting stress and increase social capital in Japan? J. Epidemiol. Community Health 2012, 66, 1167. [Google Scholar] [CrossRef]
- Coll-Planas, L.; Del Valle Gómez, G.; Bonilla, P.; Masat, T.; Puig, T.; Monteserin, R. Promoting social capital to alleviate loneliness and improve health among older people in Spain. Health Soc. Care Community 2017, 25, 145–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramli, M.; Salmiah, M.; Nurul, A.M. Validation and pychometric properties of Bahasa Malaysia version of the Depression Anxiety and Stress Scales (DASS) among diabetic patients. MJP Online Early 2009, 8, 1–7. [Google Scholar]
- Musa, R.; Ramli, R.; Abdullah, K.; Sarkarsi, R. Concurrent validity of the depression and anxiety components in the Bahasa Malaysia version of the Depression Anxiety and Stress scales (DASS). ASEAN J. Psychiatry 2011, 12, 66–70. [Google Scholar]
- De Miquel, C.; Domènech-Abella, J.; Felez-Nobrega, M.; Cristóbal-Narváez, P.; Mortier, P.; Vilagut, G.; Alonso, J.; Olaya, B.; Haro, J.M. The mental health of employees with job loss and income loss during the COVID-19 pandemic: The mediating role of perceived financial stress. Int J. Environ. Res. Public Health 2022, 19, 3158. [Google Scholar] [CrossRef] [PubMed]
| Characteristics | Prevalence, n (%) | Mean ± SD |
|---|---|---|
| Age (n = 6651) | 6651 (100.0) | 65.5 ± 7.7 |
| Gender (n = 6651) | ||
| Female | 3556 (53.5) | |
| Male | 3095 (46.5) | |
| Ethnicity (n = 6646) | ||
| Malays | 4111 (61.9) | |
| Indians | 522 (7.9) | |
| Chinese | 1957 (29.4) | |
| Others | 56 (0.8) | |
| Marital Status (n = 6649) | ||
| Single | 167 (2.5) | |
| Married | 5000 (75.2) | |
| Separated/divorced/other | 105 (1.6) | |
| Widow | 1377 (20.7) | |
| Education Level (n = 6487) | ||
| None | 381 (5.9) | |
| Primary | 3822 (58.9) | |
| Secondary | 1804 (27.8) | |
| Tertiary | 150 (2.3) | |
| Others | 330 (5.1) | |
| Employment Status (n = 6617) | ||
| Housewife | 2163 (32.7) | |
| Unemployed | 1420 (21.5) | |
| Paid employment | 901 (13.6) | |
| Pensioners | 907 (13.7) | |
| Self employed | 1226 (18.5) | |
| Income groups (n = 6145) | ||
| B40 (Less than RM3860) | 6061 (99.7) | |
| M40 (RM3860 to RM8319) | 84 (0.3) | |
| Individual social capital variables | ||
| Reciprocity (n = 6542) | ||
| Agree | 4439 (67.9) | |
| Disagree or “neutral” | 2103 (32.1) | |
| Cooperation (n = 6549) | ||
| Agree | 4780 (73.0) | |
| Disagree or “neutral” | 1769 (27.0) | |
| Trust in community (n = 6527) | ||
| Disagree or “neutral” | 4290 (65.7) | |
| Agree | 2237 (34.3) | |
| Attached to community (n = 6534) | ||
| Disagree or “neutral” | 4176 (63.9) | |
| Agree | 2358 (36.1) | |
| Mental health (DASS-21) | 12.39 (17.80) | |
| Depression (n = 6601) | ||
| Normal | 5511 (83.5) | |
| Mild and above | 1090 (16.5) | |
| Anxiety (n = 6606) | ||
| Normal | 5128 (77.6) | |
| Mild and above | 1478 (22.4) | |
| Stress (n = 6591) | ||
| Normal | 6135 (93.1) | |
| Mild and above | 456 (6.9) |
| Outcome | Mediator | |||
|---|---|---|---|---|
| Reciprocity | Cooperation among Community Members | Trust in Community | Attached to Local Community | |
| Anxiety | ||||
| Total effect M40 | 0.74 *** (0.25) | 0.79 *** (0.27) | 0.78 *** (0.27) | 0.78 *** (0.27) |
| Direct effect M40 | 0.57 ** (0.25) | 0.63 ** (0.27) | 0.54 * (0.27) | 0.57 ** (0.27) |
| Indirect effect | 0.17 ** (0.08) | 0.15 (0.10) | 0.24 ** (0.10) | 0.21 ** (0.10) |
| Mediation (%) | 22.8 | 19.5 | 30.8 | 26.5 |
| Partial mediation | yes | no | yes | yes |
| Full mediation | no | no | no | no |
| Depression | ||||
| Total effect M40 | 1.01 *** (0.26) | 1.09 *** (0.28) | 1.07 *** (0.28) | 1.08 *** (0.29) |
| Direct effect M40 | 0.82 *** (0.26) | 0.92 *** (0.28) | 0.80 *** (0.28) | 0.82 *** (0.29) |
| Indirect effect | 0.19 ** (0.08) | 0.17 (0.11) | 0.26 ** (0.11) | 0.24 ** (0.11) |
| Mediation (%) | 18.5 | 15.3 | 24.8 | 22.6 |
| Partial mediation | yes | no | yes | yes |
| Full mediation | no | no | no | no |
| Stress | ||||
| Total effect M40 | 1.28 *** (0.28) | 1.34 *** (0.29) | 1.34 *** (0.31) | 1.31 *** (0.30) |
| Direct effect M40 | 1.12 *** (0.28) | 1.17 *** (0.29) | 1.08 *** (0.31) | 1.05 *** (0.30) |
| Indirect effect | 0.15 ** (0.07) | 0.17 ** (0.10) | 0.26 ** (0.12) | 0.26 ** (0.11) |
| Mediation (%) | 12.0 | 12.9 | 19.5 | 19.7 |
| Partial mediation | yes | yes | yes | yes |
| Full mediation | no | no | no | no |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Said, M.A.; Thangiah, G.; Abdul Majid, H.; Ismail, R.; Maw Pin, T.; Rizal, H.; Zaidi, M.A.S.; Reidpath, D.; Su, T.T. Income Disparity and Mental Wellbeing among Adults in Semi-Urban and Rural Areas in Malaysia: The Mediating Role of Social Capital. Int. J. Environ. Res. Public Health 2022, 19, 6604. https://doi.org/10.3390/ijerph19116604
Said MA, Thangiah G, Abdul Majid H, Ismail R, Maw Pin T, Rizal H, Zaidi MAS, Reidpath D, Su TT. Income Disparity and Mental Wellbeing among Adults in Semi-Urban and Rural Areas in Malaysia: The Mediating Role of Social Capital. International Journal of Environmental Research and Public Health. 2022; 19(11):6604. https://doi.org/10.3390/ijerph19116604
Chicago/Turabian StyleSaid, Mas Ayu, Govindamal Thangiah, Hazreen Abdul Majid, Rozmi Ismail, Tan Maw Pin, Hussein Rizal, Mohd Azlan Shah Zaidi, Daniel Reidpath, and Tin Tin Su. 2022. "Income Disparity and Mental Wellbeing among Adults in Semi-Urban and Rural Areas in Malaysia: The Mediating Role of Social Capital" International Journal of Environmental Research and Public Health 19, no. 11: 6604. https://doi.org/10.3390/ijerph19116604
APA StyleSaid, M. A., Thangiah, G., Abdul Majid, H., Ismail, R., Maw Pin, T., Rizal, H., Zaidi, M. A. S., Reidpath, D., & Su, T. T. (2022). Income Disparity and Mental Wellbeing among Adults in Semi-Urban and Rural Areas in Malaysia: The Mediating Role of Social Capital. International Journal of Environmental Research and Public Health, 19(11), 6604. https://doi.org/10.3390/ijerph19116604