
Recollection of Physician Information about Risk Factor and Lifestyle Changes in Chronic Coronary Syndrome Patients

 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Study Variables
2.3. Strategy in Defining the Exposure Group
2.4. Risk Factor Goal Achievement
2.5. Ethical Statement
2.6. Data Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Patient Characteristics Compared with the Recollection of Risk Factor Information Status (Good Recollection Versus Poor Recollection)
3.3. Cardiovascular Parameter Changes between RRFI Status and Different Time Points on Risk Factors and Medication Intake
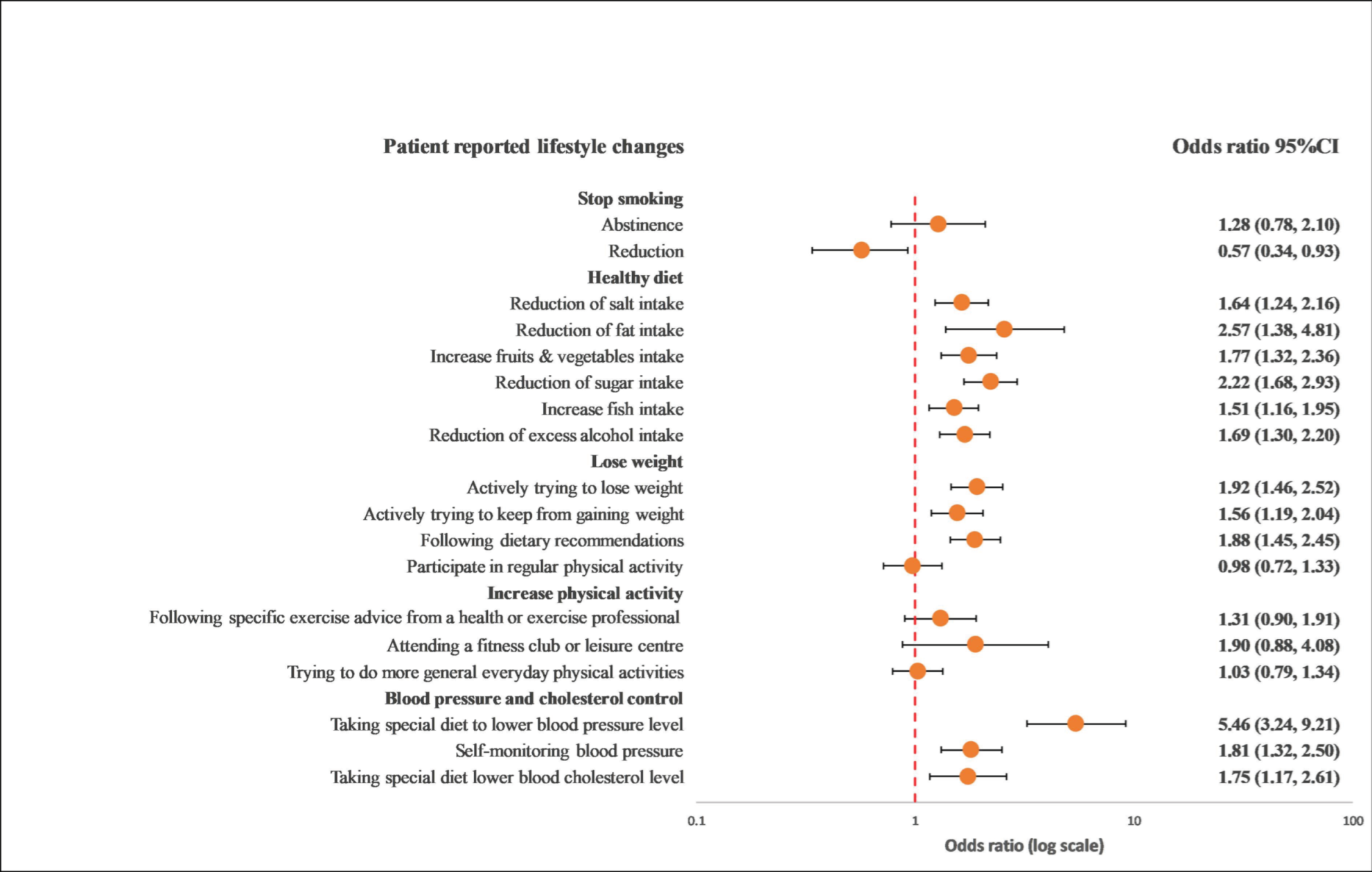
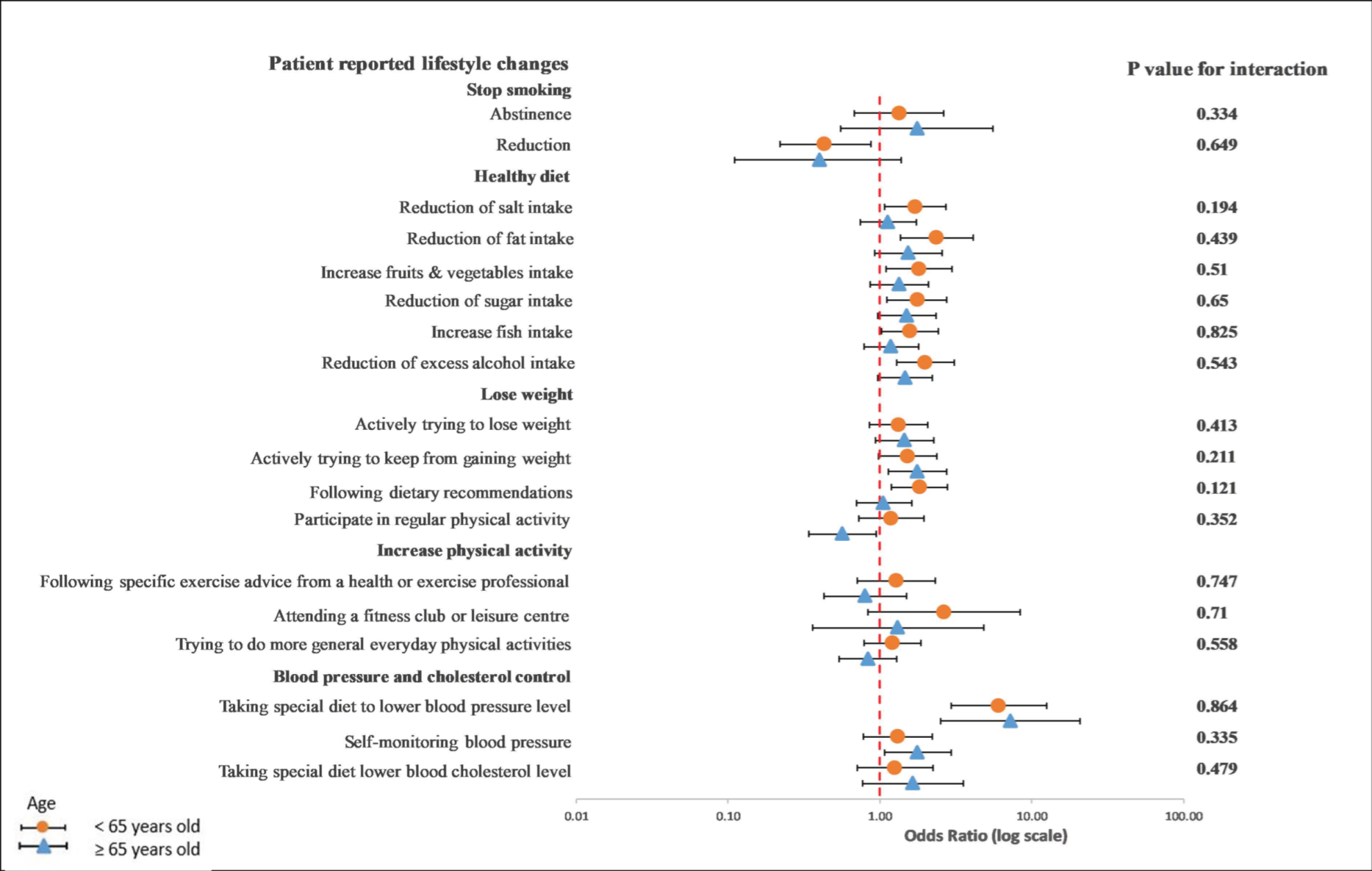
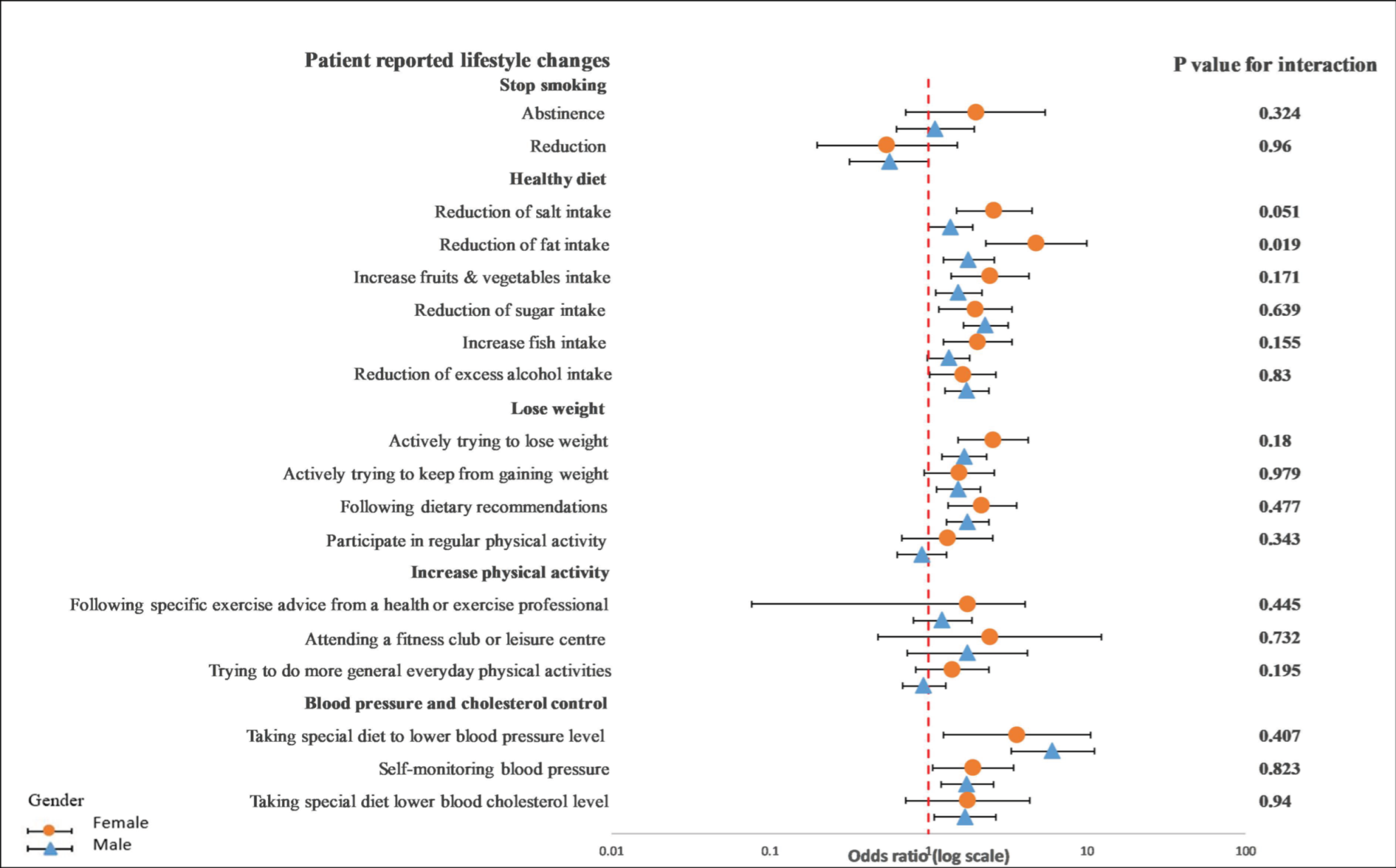
3.4. Recollection of Risk Factor Information and Lifestyle Changes
4. Discussion
5. Conclusions
Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002.
- Mokdad, A.H.; Marks, J.S.; Stroup, D.F.; Gerberding, J.L. Actual causes of death in the United States, 2000. JAMA 2004, 291, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Corrà, U.; Adamopoulos, S.; Benzer, W.; Bjarnason-Wehrens, B.; Cupples, M.; Dendale, P.; Doherty, P.; Gaita, D.; Höfer, S.; et al. Secondary prevention in the clinical management of patients with cardiovascular diseases. Core components, standards and outcome measures for referral and delivery: A policy statement from the cardiac rehabilitation section of the European Association for Cardiovascular Prevention & Rehabilitation. Endorsed by the Committee for Practice Guidelines of the European Society of Cardiology. Eur. J. Prev. Cardiol. 2014, 21, 664–681. [Google Scholar] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case–control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Kotseva, K.; Investigators, E. The EUROASPIRE surveys: Lessons learned in cardiovascular disease prevention. Cardiovasc. Diagn. Ther. 2017, 7, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Colpani, V.; Baena, C.P.; Jaspers, L.; van Dijk, G.M.; Farajzadegan, Z.; Dhana, K.; Tielemans, M.J.; Voortman, T.; Freak-Poli, R.; Veloso, G.G.V.; et al. Lifestyle factors, cardiovascular disease and all-cause mortality in middle-aged and elderly women: A systematic review and meta-analysis. Eur. J. Epidemiol. 2018, 33, 831–845. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar]
- Rees, K.; Takeda, A.; Martin, N.; Ellis, L.; Wijesekara, D.; Vepa, A.; Das, A.; Hartley, L.; Stranges, S. Mediterranean-style diet for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2019, 3, Cd009825. [Google Scholar] [CrossRef] [Green Version]
- Jankowski, P.; Kosior, D.; Sowa, P.; Szóstak-Janiak, K.; Kozieł, P.; Krzykwa, A.; Sawicka, E.; Haberka, M.; Setny, M.; Kamiński, K.; et al. Secondary prevention of coronary artery disease in Poland. Results from the POLASPIRE survey. Cardiol. J. 2020, 27, 533–540. [Google Scholar] [CrossRef]
- Kotseva, K.; Wood, D.; De Backer, G.; De Bacquer, D. Use and effects of cardiac rehabilitation in patients with coronary heart disease: Results from the EUROASPIRE III survey. Eur. J. Prev. Cardiol. 2013, 20, 817–826. [Google Scholar] [CrossRef]
- Kotseva, K.; Wood, D.; De Bacquer, D. Determinants of participation and risk factor control according to attendance in cardiac rehabilitation programmes in coronary patients in Europe: EUROASPIRE IV survey. Eur. J. Prev. Cardiol. 2018, 25, 1242–1251. [Google Scholar] [CrossRef]
- Kotseva, K.; Wood, D.; De Bacquer, D.; De Backer, G.; Rydén, L.; Jennings, C.; Gyberg, V.; Amouyel, P.; Bruthans, J.; Castro Conde, A.; et al. EUROASPIRE IV: A European Society of Cardiology survey on the lifestyle, risk factor and therapeutic management of coronary patients from 24 European countries. Eur. J. Prev. Cardiol. 2016, 23, 636–648. [Google Scholar] [CrossRef] [PubMed]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Waldron, C.A.; van der Weijden, T.; Ludt, S.; Gallacher, J.; Elwyn, G. What are effective strategies to communicate cardiovascular risk information to patients? A systematic review. Patient Educ. Couns. 2011, 82, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Usher-Smith, J.A.; Silarova, B.; Schuit, E.; Moons, K.G.; Griffin, S.J. Impact of provision of cardiovascular disease risk estimates to healthcare professionals and patients: A systematic review. BMJ Open 2015, 5, e008717. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardio-vascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar]
- Tiffe, T.; Morbach, C.; Malsch, C.; Gelbrich, G.; Wahl, V.; Wagner, M.; Kotseva, K.; Wood, D.; Leyh, R.; Ertl, G.; et al. Physicians’ lifestyle advice on primary and secondary cardiovascular disease prevention in Germany: A comparison between the STAAB cohort study and the German subset of EUROASPIRE IV. Eur. J. Prev. Cardiol. 2019, 28, 1175–1183. [Google Scholar] [CrossRef]
- Setny, M.; Jankowski, P.; Krzykwa, A.; Kamiński, K.A.; Gąsior, Z.; Haberka, M.; Czarnecka, D.; Pająk, A.; Kozieł, P.; Szóstak-Janiak, K.; et al. Management of Dyslipidemia in Women and Men with Coronary Heart Disease: Results from POLASPIRE Study. J. Clin. Med. 2021, 10, 2594. [Google Scholar] [CrossRef]
- Haberka, M.; Jankowski, P.; Kosior, D.A.; Szpakowicz, M.; Szóstak-Janiak, K.; Kozieł, P.; Krzykwa, A.; Łapińska, M.; Setny, M.; Kamiński, K.; et al. Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus—Polish multicenter study POLASPIRE. Arch. Med. Sci. 2020. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar]
- Stewart, R.A.H.; Held, C.; Hadziosmanovic, N.; Armstrong, P.W.; Cannon, C.P.; Granger, C.B.; Hagström, E.; Hochman, J.S.; Koenig, W.; Lonn, E.; et al. Physical Activity and Mortality in Patients with Stable Coronary Heart Disease. J. Am. Coll. Cardiol. 2017, 70, 1689–1700. [Google Scholar] [CrossRef]
- Barkas, F.; Nomikos, T.; Liberopoulos, E.; Panagiotakos, D. Diet and Cardiovascular Disease Risk Among Individuals with Familial Hypercholesterolemia: Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2436. [Google Scholar] [CrossRef] [PubMed]
- Ley, P. Doctor-patient communication: Some quantitative estimates of the role of cognitive factors in non-compliance. J. Hypertens. Suppl. 1985, 3, S51–S55. [Google Scholar] [PubMed]
- Ferrini, R.; Edelstein, S.; Barrettconnor, E. The Association between Health Beliefs and Health Behavior Change in Older Adults. Prev. Med. 1994, 23, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Woodward, M.; Vaartjes, I.; Millett, E.R.C.; Klipstein-Grobusch, K.; Hyun, K.; Carcel, C.; Peters, S.A.E. Sex differences in cardiovascular medication prescription in primary care: A systematic review and meta-analysis. J. Am. Heart Assoc. 2020, 9, e014742. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Colantonio, L.D.; Zhao, H.; Bittner, V.; Dai, Y.; Farkouh, M.E.; Monda, K.L.; Safford, M.M.; Muntner, P.; Woodward, M. Sex Differences in High-Intensity Statin Use Following Myocardial Infarction in the United States. J. Am. Coll. Cardiol. 2018, 71, 1729–1737. [Google Scholar] [CrossRef]
- Rosano, G.M.; Lewis, B.; Agewall, S.; Wassmann, S.; Vitale, C.; Schmidt, H.; Drexel, H.; Patak, A.; Torp-Pedersen, C.; Kjeldsen, K.P.; et al. Gender differences in the effect of cardiovascular drugs: A position document of the Working Group on Pharmacology and Drug Therapy of the ESC. Eur. Heart J. 2015, 36, 2677–2680. [Google Scholar] [CrossRef] [Green Version]
- Tamargo, J.; Rosano, G.; Walther, T.; Duarte, J.; Niessner, A.; Kaski, J.C.; Ceconi, C.; Drexel, H.; Kjeldsen, K.; Savarese, G. Gender differences in the effects of cardiovascular drugs. Eur. Heart J.-Cardiovasc. Pharmacother. 2017, 3, 163–182. [Google Scholar] [CrossRef] [Green Version]
- Bansilal, S.; Castellano, J.M.; Garrido, E.; Wei, H.G.; Freeman, A.; Spettell, C.; Garcia-Alonso, F.; Lizano, I.; Arnold, R.J.; Rajda, J.; et al. Assessing the Impact of Medication Adherence on Long-Term Cardiovascular Outcomes. J. Am. Coll. Cardiol. 2016, 68, 789–801. [Google Scholar] [CrossRef]
- Rasmussen, J.N.; Chong, A.; Alter, D.A. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA 2007, 297, 177–186. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Glynn, R.J.; Avorn, J.; Lee, J.L.; Brennan, T.A.; Reisman, L.; Toscano, M.; Levin, R.; Matlin, O.S.; Antman, E.M.; et al. Untangling the relationship between medication adherence and post-myocardial infarction outcomes: Medication adherence and clinical outcomes. Am. Heart J. 2014, 167, 51–58.e5. [Google Scholar] [CrossRef]
- Sowa, P.; Kiszkiel, L.; Laskowski, P.P.; Alimowski, M.; Szczerbiński, L.; Paniczko, M.; Moniuszko-Malinowska, A.; Kamiński, K. COVID-19 Vaccine Hesitancy in Poland-Multifactorial Impact Trajectories. Vaccines 2021, 9, 876. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Patients n = 946 | Physician Risk Factor Information Recollection | p-Value | Multivariate Odds Ratio (95% CI) a | |
|---|---|---|---|---|---|
| Poor Recollection n = 445 | Good Recollection n = 501 | ||||
| Age Group, Years | 0.194 | ||||
| <54 | 104 (11.0) | 51 (11.5) | 53 (10.6) | 1.00 | |
| 55–64 | 349 (36.9) | 151 (33.9) | 198 (39.5) | 0.97 (0.59–1.59) | |
| 65–74 | 379 (40.1) | 181 (40.7) | 198 (39.5) | 0.59 (0.36–0.98) | |
| ≥75 | 114 (12.1) | 62 (13.9) | 52 (10.4) | 0.51 (0.27–0.96) | |
| Gender | 0.286 | ||||
| Female | 273 (28.9) | 121 (27.2) | 152 (30.3) | ||
| Male | 673 (71.1) | 324 (72.8) | 349 (69.7) | - | |
| - | |||||
| Center | 0.756 | ||||
| Nonteaching hospitals | 162 (17.1) | 78 (17.5) | 84 (16.8) | - | |
| Teaching hospitals | 784 (82.9) | 367 (82.5) | 417 (83.2) | - | |
| Education Level | 0.304 | ||||
| Primary education | 129 (13.6) | 55 (12.4) | 74 (14.8) | - | |
| Middle education | 640 (67.7) | 312 (70.1) | 328 (65.5) | - | |
| Higher education | 177 (18.7) | 78 (17.5) | 99 (19.8) | - | |
| Recruiting Event | 0.087 | ||||
| CABG | 38 (4.0) | 21 (4.7) | 17 (3.4) | - | |
| PCI | 355 (37.5) | 157 (35.3) | 198 (39.5) | - | |
| ST-EMI | 148 (15.6) | 73 (16.4) | 75 (15.0) | - | |
| Non-ST-EMI | 200 (21.1) | 84 (18.9) | 116 (23.2) | - | |
| UA | 205 (21.7) | 110 (24.7) | 95 (19.0) | - | |
| Smoking Habit | 0.152 | ||||
| Nonsmoker | 422 (44.6) | 191 (42.9) | 231 (46.1) | - | |
| Former smoker | 296 (31.3) | 134 (30.1) | 162 (32.3) | - | |
| Current smoker | 228 (24.1) | 120 (27.0) | 108 (21.6) | - | |
| Obesity | <0.001 | ||||
| 49 | 1.00 | ||||
| Yes | 370 (39.1) | 87 (19.6) | 283 (56.5) | 4.41 (3.09–6.30) | |
| Unknown | 180 (19.0) | 87 (19.6) | 93 (18.6) | 1.07 (0.72–1.59) | |
| Weight, kg | 82.75 (74.0, 94.0) | 79.0 (70.52, 88.0) | 89.0 (79.0, 98.0) | <0.001 | - |
| BMI, kg/m2 | 29.03 (26.27, 32.16) | 27.73 (25.51, 29.74) | 31.0 (28.82, 33.46) | <0.001 | - |
| Hypertension | <0.001 | ||||
| Yes | 863 (91.2) | 389 (87.4) | 474 (94.6) | ||
| SBP, mm Hg | 136.0 (125.0, 150.0) | 130.0 (122.2, 146.75) | 140 (128.0, 153.5) | 0.010 | - |
| DBP, mm Hg | 80.0 (73.0, 88.0) | 80.0 (72.0, 85.0) | 80.0 (74.0, 90.0) | <0.001 | - |
| Hyperlipidemia | <0.001 | ||||
| Yes | 733 (90.6) | 328 (87.5) | 405 (93.3) | - | |
| LDL-C, mmol/L | 2.43 (1.86, 3.39) | 2.50 (1.83, 3.39) | 2.40 (1.83, 3.34) | 0.474 | - |
| HDL-C, mmol/L | 1.14 (0.95, 1.39) | 1.21 (0.98, 1.45) | 1.11 (0.93, 1.34) | 0.003 | - |
| Triglycerides, mmol/L | 1.30 (0.97, 1.86) | 1.22 (0.87, 1.71) | 1.38 (1.05, 1.92) | 0.007 | - |
| Diabetes | <0.001 | ||||
| No | 628 (66.4) | 370 (83.1) | 258 (51.5) | 1.00 | |
| Yes | 318 (33.6) | 75 (16.9) | 243 (48.5) | 4.16 (2.96–5.84) | |
| Medication Prescribed | |||||
| Antiplatelets | 934 (98.7) | 441 (99.1) | 493 (98.4) | 0.338 | - |
| Beta-blockers | 867 (91.6) | 406 (91.2) | 461 (92.0) | 0.665 | - |
| ACEI/sartan | 722 (76.3) | 358 (80.4) | 364 (72.7) | 0.005 | 0.65 (0.45–0.94) |
| Statins | 894 (94.5) | 420 (94.4) | 474 (94.6) | 0.878 | - |
| Calcium channel blockers | 260 (27.5) | 92 (20.7) | 168 (33.5) | <0.001 | 1.47 (1.04–2.09) |
| Diuretics | 466 (49.3) | 188 (42.2) | 278 (55.5) | <0.001 | 1.41 (1.03–1.91) |
| Anticoagulants | 139 (14.7) | 57 (12.8) | 82 (16.4) | 0.124 | - |
| Recollection of a Physician’s Information on Risk Factors | ||||||
|---|---|---|---|---|---|---|
| Dependent Variables | Poor Recollection n = 445 | Good Recollection n = 501 | OR a | Bb | 95% CI | p-Value |
| Risk Factor Goals | ||||||
| Stopped smoking c | 58 (50.9) | 56 (49.1) | 1.48 | - | 0.85 to 2.60 | 0.161 |
| Reduction in smoking c | 77 (61.1) | 49 (38.9) | 0.41 | - | 0.23–0.73 | 0.003 |
| Increased physical activity d | 68 (15.3) | 63 (12.6) | 0.77 | - | 0.50–1.19 | 0.252 |
| BMI, kg/m2 | ||||||
| <25 | 108 (24.3) | 35 (7.0) | 0.45 | 0.28–0.71 | 0.001 | |
| <30 | 332 (74.6) | 217 (43.3) | 0.52 | - | 0.37–0.74 | 0.000 |
| Blood pressure on target e | 393 (88.9) | 427 (85.4) | 0.65 | - | 0.41–1.01 | 0.058 |
| LDL cholesterol on target f | 175 (39.8) | 180 (36.1) | 0.70 | - | 0.52–0.96 | 0.028 |
| HbA1c on target g | 357 (93.5) | 351 (77.8) | 0.63 | - | 0.36–1.08 | 0.097 |
| Antiplatelet, n% | ||||||
| Aspirin | 401 (90.1) | 439 (87.6) | 0.75 | - | 0.47–1.21 | 0.247 |
| Clopidogrel | 222 (49.9) | 233 (46.5) | 0.76 | - | 0.56–1.02 | 0.068 |
| Lipid-Lowering Drugs, n% | ||||||
| Atorvastatin | 292 (65.6) | 316 (63.1) | 0.90 | - | 0.66–1.23 | 0.476 |
| Rosuvastatin | 90 (20.2) | 120 (24.0) | 1.14 | - | 0.80–1.62 | 0.456 |
| ACE inhibitors, n% | 311 (69.9) | 354 (70.7) | 1.01 | - | 0.73–1.39 | 0.951 |
| Beta-blockers, n% | 385 (86.5) | 457 (91.2) | 1.16 | - | 0.72–1.86 | 0.528 |
| Medication Adherence h | ||||||
| Lipid-lowering drug > 75% intake | 385 (88.1) | 455 (92.9) | 1.46 | 0.87–2.42 | 0.145 | |
| Antihypertensive drug > 75% intake | 372 (85.7) | 463 (94.1) | 1.80 | - | 1.07–3.03 | 0.026 |
| Glucose-lowering drug > 75% intake | 103 (23.7) | 242 (49.3) | 0.81 | - | 0.48–1.38 | 0.458 |
| Quality of life | ||||||
| HADS—anxiety, mean ± SD | 5.70 ± 3.77 | 5.90 ± 3.54 | - | 0.35 | −0.17 to 0.88 | 0.184 |
| HADS—depression, mean ± SD | 5.45 ± 3.66 | 5.50 ± 3.36 | - | −0.01 | −0.51 to 0.49 | 0.964 |
| Heart QoL f global, mean ± SD | 29.06 ± 8.41 | 27.36 ± 9.02 | - | −2.08 | −3.75 to −0.42 | 0.014 |
| Heart QoL emotional, mean ± SD | 7.70 ± 2.30 | 7.39 ± 2.31 | - | −0.49 | −0.94 to −0.05 | 0.027 |
| Heart QoL physical, mean ± SD | 21.37 ± 7.07 | 20.0 ± 7.66 | - | −1.57 | −2.97 to 00.16 | 0.029 |
| VAS overall | 0.86 ± 0.12 | 0.84 ± 0.14 | - | −0.02 | −0.05 to 0.00 | 0.068 |
| Dependent Variables | Physician Risk Factor Information Recollection | Difference in Change from Regression (Crude Model) | p-Value | Difference in Change from Regression (Adjusted Model) | p-Value a | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Poor Recollection (n = 445) | Good Recollection (n = 501) | |||||||||
| Clinical Parameters | Baseline | Interview | Mean Change in Baseline to Interview | Baseline | Interview | Mean Change in Baseline to Interview | ||||
| BMI, kg/m2 | 27.58 ± 3.99 | 27.73 ± 3.97 | 0.15 ± 2.23 | 30.95 ± 4.25 | 31.12 ± 4.30 | 0.16 ± 2.23 | 0.01 (−0.30 to 0.33) | 0.923 | 0.47 (0.11 to 0.83) | 0.010 |
| SBP, mm Hg | 135.37 ± 19.87 | 132.29 ± 19.12 | −3.08 ± 22.18 | 139.98 ± 21.75 | 134.64 ± 18.32 | −5.34 ± 24.37 | −2.25 (−5.32 to 0.81) | 0.150 | −2.50 (−5.99 to 0.98) | 0.159 |
| DBP, mm Hg | 79.44 ± 10.64 | 79.13 ± 10.28 | −0.31± 12.13 | 81.71 ± 12.31 | 80.77 ± 10.92 | −0.94 ± 14.38 | −0.63 (−2.39 to 1.12) | 0.478 | −0.13 (−2.11 to 1.85) | 0.896 |
| LDL-C, mmol | 2.69 ± 1.11 | 2.20 ± 0.91 | −0.49 ± 1.12 | 2.66 ± 1.16 | 2.24 ± 1.01 | −0.42 ± 1.20 | 0.06 (−0.10 to 0.23) | 0.427 | −0.05 (−0.24 to 0.13) | 0.588 |
| HDL-C, mmol/L | 1.26 ± 0.44 | 1.34 ± 0.38 | 0.08 ± 0.36 | 1.16 ± 0.39 | 1.27 ± 0.36 | 0.10 ± 0.33 | 0.02 (−0.02 to 0.07) | 0.369 | 0.01 (−0.04 to 0.07) | 0.577 |
| Triglycerides, mmol/L | 1.42 ± 0.90 | 1.38 ± 0.85 | −0.03 ± 0.76 | 1.62 ± 0.96 | 1.54 ± 0.84 | −0.08 ± 0.96 | −0.05 (−0.17 to 0.07) | 0.418 | −0.05 (−0.19 to 0.08) | 0.455 |
| Dependent Variables | Physician Risk Factor Information Recollection | Estimate of Difference in Change From Regression Model 1 | p-Value | Estimate of Difference in Change from Regression Model 2 | p-Value a | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Poor Recollection (n = 445) | Good Recollection (n = 501) | |||||||||
| Medication | Baseline | Interview | Percentage Change in Baseline to Interview | Baseline | Interview | Percentage Change in Baseline to Interview | ||||
| Antiplatelets | 441 (99.1) | 413 (93.7) | −5.4 % | 493 (98.4) | 463 (93.9) | % 5.6 | 1.04 (0.61–1.78) | 0.867 | 1.05 (0.57–1.92) | 0.87 |
| Beta-blockers | 406 (91.2) | 369 (90.9) | −0.3% | 461 (92.2) | 441 (95.7) | 1.9% | 2.21 (1.26–3.87) | 0.006 | 1.54 (0.81–2.91) | 0.182 |
| ACE inhibitors | 358 (80.4) | 289 (80.7) | 0.3% | 364 (72.7) | 313 (86.0) | 2.1% | 1.46 (0.98–2.17) | 0.058 | 1.47 (0.94–2.30) | 0.091 |
| Statins | 420 (94.4) | 380 (90.5) | −3.9% | 474 (94.6) | 434 (91.6) | 0.4% | 1.14 (0.72–1.80) | 0.571 | 1.07 (0.63–1.80) | 0.795 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinnadurai, S.; Sowa, P.; Jankowski, P.; Gasior, Z.; Kosior, D.A.; Haberka, M.; Czarnecka, D.; Pajak, A.; Setny, M.; Jamiolkowski, J.; et al. Recollection of Physician Information about Risk Factor and Lifestyle Changes in Chronic Coronary Syndrome Patients. Int. J. Environ. Res. Public Health 2022, 19, 6416. https://doi.org/10.3390/ijerph19116416
Sinnadurai S, Sowa P, Jankowski P, Gasior Z, Kosior DA, Haberka M, Czarnecka D, Pajak A, Setny M, Jamiolkowski J, et al. Recollection of Physician Information about Risk Factor and Lifestyle Changes in Chronic Coronary Syndrome Patients. International Journal of Environmental Research and Public Health. 2022; 19(11):6416. https://doi.org/10.3390/ijerph19116416
Chicago/Turabian StyleSinnadurai, Siamala, Pawel Sowa, Piotr Jankowski, Zbigniew Gasior, Dariusz A. Kosior, Maciej Haberka, Danuta Czarnecka, Andrzej Pajak, Malgorzata Setny, Jacek Jamiolkowski, and et al. 2022. "Recollection of Physician Information about Risk Factor and Lifestyle Changes in Chronic Coronary Syndrome Patients" International Journal of Environmental Research and Public Health 19, no. 11: 6416. https://doi.org/10.3390/ijerph19116416
APA StyleSinnadurai, S., Sowa, P., Jankowski, P., Gasior, Z., Kosior, D. A., Haberka, M., Czarnecka, D., Pajak, A., Setny, M., Jamiolkowski, J., Sawicka-Śmiarowska, E., & Kaminski, K. (2022). Recollection of Physician Information about Risk Factor and Lifestyle Changes in Chronic Coronary Syndrome Patients. International Journal of Environmental Research and Public Health, 19(11), 6416. https://doi.org/10.3390/ijerph19116416