
Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature




Abstract
1. Introduction
- Are the higher amounts of glycated hemoglobin, indicating poorer control of blood glucose levels, associated with shoulder dysfunction in type 2 DM patients?
- What are the mechanisms behind the increased incidence of shoulder complaints in type 2 DM patients?
2. Methods
2.1. Eligibility Criteria
- P: subjects with a glucose metabolism disorder
- I: Randomized Controlled Trial, case control, cohort, and cross-sectional studies
- C: compared with a non-type 2 DM control group
- O: association between metabolic derangements and shoulder dysfunction, full text written in English, Dutch, German, or French,
- diseased (acute non metabolic disease),
- children (<10 years of age) and geriatric population (>65 years of age)
- languages other than mentioned above and
- meta-analysis, systematic reviews.
2.2. Information Sourcesand Search Strategy
2.3. Data Extraction and Analysis
2.4. Assessment of Risk of Bias across Studies
2.5. Data Items
3. Results
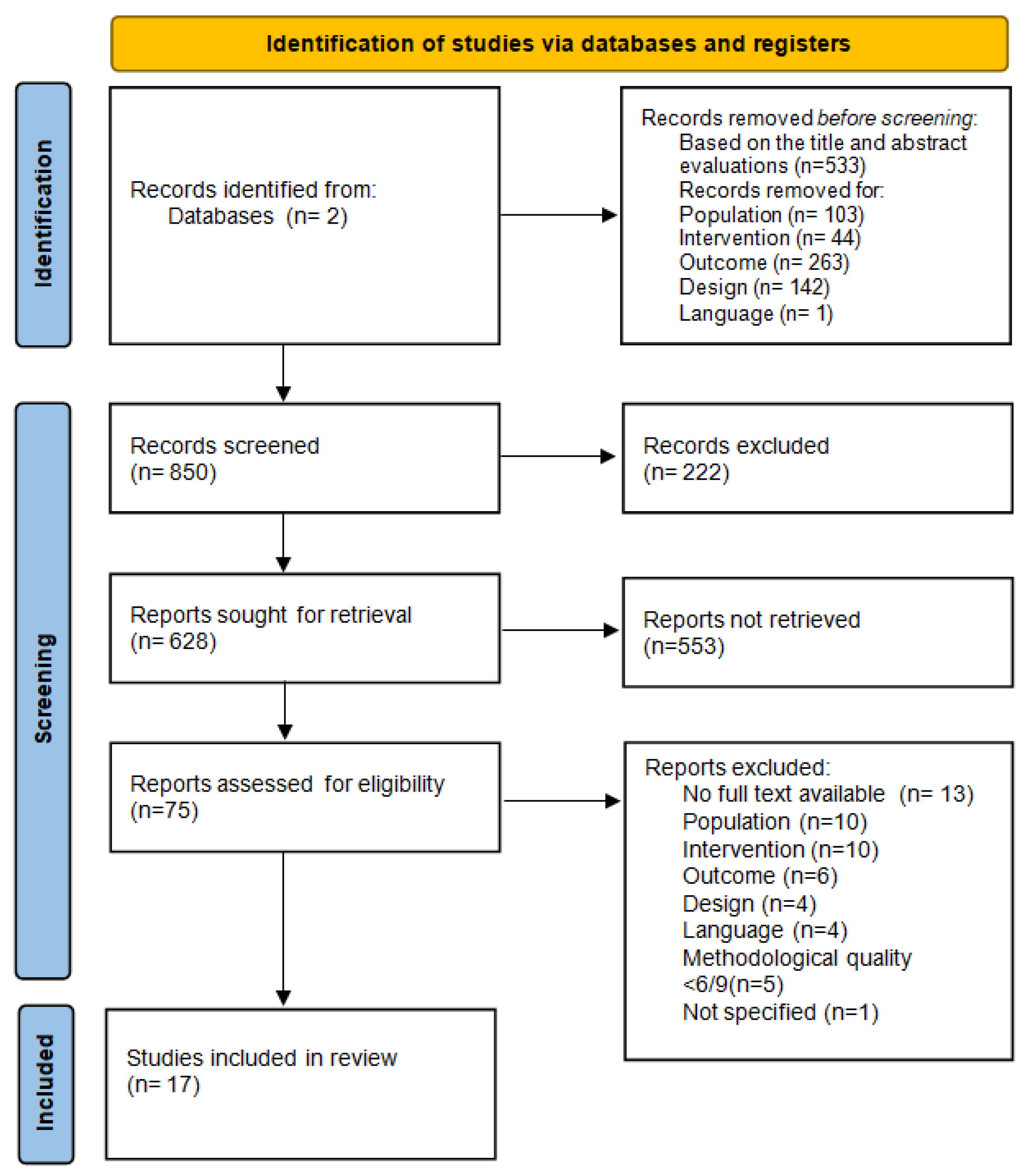
3.1. Study Selection
3.2. Risk of Bias within Studies
3.3. Risk of Bias across Studies
3.4. Risk of Bias in Individual Studies
3.5. Synthesis of Results
3.6. Results of Individual Studies
3.6.1. Shoulder Range of Motion (SROM)
3.6.2. Questionnaires
3.6.3. Medical Imaging
3.6.4. Blood Analysis
3.6.5. Synovial Fluid
3.6.6. Chronic Complications of DM
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization; International Diabetes Federation. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation; WHO: Geneva, Switzerland, 2006; Available online: https://www.who.int/publications/i/item/definition-and-diagnosis-of-diabetes-mellitus-and-intermediate-hyperglycaemia (accessed on 16 November 2016).
- Kujala, U. NCD Risk Factor Collaboration. Lancet 2016, 387, 1513–1530. [Google Scholar]
- World Health Organization; International Diabetes Federation. Global Report on Diabetes; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Cade, W.T. Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys. Ther. 2008, 88, 1322–1335. [Google Scholar] [CrossRef] [PubMed]
- Molsted, S.; Tribler, J.; Snorgaard, O. Musculoskeletal pain in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2012, 96, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Laslett, L.L.; Burnet, S.P.; Jones, J.A.; Redmond, C.L.; McNeil, J.D. Musculoskeletal morbidity: The growing burden of shoulder pain and disability and poor quality of life in diabetic outpatients. Clin. Exp. Rheumatol. 2007, 25, 422–429. [Google Scholar]
- Kiani, J.; Goharifar, H.; Moghimbeigi, A.; Azizkhani, H. Prevalence and risk factors of five most common upper extremity disorders in diabetics. J. Res. Health Sci. 2014, 14, 92–95. [Google Scholar]
- Cole, A.; Gill, T.K.; Shanahan, E.M.; Phillips, P.; Taylor, A.W.; Hill, C.L. Is diabetes associated with shoulder pain or stiffness? Results from a population based study. J. Rheumatol. 2009, 36, 371–377. [Google Scholar] [CrossRef]
- Ko, J.Y.; Wang, F.S. Rotator cuff lesions with shoulder stiffness: Updated pathomechanisms and management. Chang Gung Med. J. 2011, 34, 331–340. [Google Scholar]
- Lebiedz-Odrobina, D.; Kay, J. Rheumatic manifestations of diabetes mellitus. Rheum. Dis. Clin. N. Am. 2010, 36, 681–699. [Google Scholar] [CrossRef]
- Boivin, G.P.; Elenes, E.Y.; Schultze, A.K.; Chodavarapu, H.; Hunter, S.A.; Elased, K.M. Biomechanical properties and histology of db/db diabetic mouse Achilles tendon. Muscles Ligaments Tendons J. 2014, 4, 280–284. [Google Scholar] [CrossRef]
- Kaviratne, M.; Hesse, M.; Leusink, M.; Cheever, A.W.; Davies, S.J.; McKerrow, J.H.; Wakefield, L.M.; Letterio, J.J.; Wynn, T.A. IL-13 activates a mechanism of tissue fibrosis that is completely TGF-beta independent. J. Immunol. 2004, 173, 4020–4029. [Google Scholar] [CrossRef]
- Spite, M.; Claria, J.; Serhan, C.N. Resolvins, specialized proresolving lipid mediators, and their potential roles in metabolic diseases. Cell Metab. 2014, 19, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, R.; Enjoji, M.; Nakamuta, M.; Ohta, S.; Kohjima, M.; Fukushima, M.; Kuniyoshi, M.; Arimura, E.; Morizono, S.; Kotoh, K.; et al. Effect of IL-4 and IL-13 on collagen production in cultured LI90 human hepatic stellate cells. Liver Int. 2005, 25, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Welty, F.K.; Alfaddagh, A.; Elajami, T.K. Targeting inflammation in metabolic syndrome. Transl. Res. 2016, 167, 257–280. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.-H.; Lho, Y.M.; Ha, E.; Hwang, I.; Song, K.S.; Min, B.W.; Bae, K.C.; Kim, D.H. Up-regulation of acid-sensing ion channels in the capsule of the joint in frozen shoulder. Bone Jt. J. 2015, 97, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Lai-Fook, S.J.; Hyatt, R.E. Effects of age on elastic moduli of human lungs. J. Appl. Physiol. 2000, 89, 163–168. [Google Scholar] [CrossRef]
- Oliva, F.; Piccirilli, E.; Berardi, A.C.; Frizziero, A.; Tarantino, U.; Maffulli, N. Hormones and tendinopathies: The current evidence. Br. Med. Bull. 2016, 117, 39–58. [Google Scholar] [CrossRef]
- Rodeo, S.A.; Hannafin, J.A.; Tom, J.; Warren, R.F.; Wickiewicz, T.L. Immunolocalization of cytokines and their receptors in adhesive capsulitis of the shoulder. J. Orthop. Res. 1997, 15, 427–436. [Google Scholar] [CrossRef]
- Schnider, S.L.; Kohn, R.R. Effects of age and diabetes mellitus on the solubility of collagen from human skin, tracheal cartilage and dura mater. Exp. Gerontol. 1982, 17, 185–194. [Google Scholar] [CrossRef]
- Snedeker, J.G.; Gautieri, A. The role of collagen crosslinks in ageing and diabetes—The good, the bad, and the ugly. Muscles Ligaments Tendons J. 2014, 4, 303–308. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Me. Analyses: The PRISMA Statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Berkman, N.D.; Dryden, D.M.; Hartling, L. Assessing Risk of Bias and Confounding in Observational Studies of Interventions or Exposures: Further Development of the RTI Item Bank; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2013.
- Abate, M.; Schiavone, C.; Pelotti, P.; Salini, V. Limited joint mobility (LJM) in elderly subjects with type II diabetes mellitus. Arch. Gerontol. Geriatr. 2011, 53, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Schiavone, C.; Salini, V. Sonographic evaluation of the shoulder in asymptomatic elderly subjects with diabetes. BMC Musculoskelet. Disord. 2010, 11, 278. [Google Scholar] [CrossRef] [PubMed]
- Balci, N.; Balci, M.K.; Tuzuner, S. Shoulder adhesive capsulitis and shoulder range of motion in type II diabetes mellitus: Association with diabetic complications. J. Diabetes Complicat. 1999, 13, 135–140. [Google Scholar] [CrossRef]
- Czelusniak, P.; Walczak, T.G.; Skare, T.L. Shoulder pain and dysfunction in 150 type 2 diabetes mellitus patients. Arq. Bras. Endocrinol. Metabol. 2012, 56, 233–237. [Google Scholar] [CrossRef][Green Version]
- Handa, A.; Gotoh, M.; Hamada, K.; Yanagisawa, K.; Yamazaki, H.; Nakamura, M.; Ueyama, Y.; Mochida, J.; Fukuda, H. Vascular endothelial growth factor 121 and 165 in the subacromial bursa are involved in shoulder joint contracture in type II diabetics with rotator cuff disease. J. Orthop. Res. 2003, 21, 1138–1144. [Google Scholar] [CrossRef]
- Kang, J.-H.; Tseng, S.-H.; Jaw, F.-S.; Lai, C.-H.; Chen, H.-C.; Chen, S.-C. Comparison of ultrasonographic findings of the rotator cuff between diabetic and nondiabetic patients with chronic shoulder pain: A retrospective study. Ultrasound Med. Biol. 2010, 36, 1792–1796. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, K.J.; Kim, W.; Chung, S.G. Relationships Between Capsular Stiffness and Clinical Features in Adhesive Capsulitis of the Shoulder. Phys. Med. Rehabil. 2015, 7, 1226–1234. [Google Scholar] [CrossRef]
- Mavrikakis, M.E.; Drimis, S.; Kontoyannis, D.A.; Rasidakis, A.; Moulopoulou, E.S.; Kontoyannis, S. Calcific shoulder periarthritis (tendinitis) in adult onset diabetes mellitus: A controlled study. Ann. Rheum. Dis. 1989, 48, 211–214. [Google Scholar] [CrossRef]
- Mavrikakis, M.E.; Sfikakis, P.P.; Kontoyannis, S.A.; Antoniades, L.G.; Moulopoulou, D.S. Clinical and laboratory parameters in adult diabetics with and without calcific shoulder periarthritis. Calcif. Tissue Int. 1991, 49, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Ramchurn, N.; Mashamba, C.; Leitch, E.; Arutchelvam, V.; Narayanan, K.; Weaver, J.; Hamilton, J.; Heycock, C.; Saravanan, V.; Kelly, C. Upper limb musculoskeletal abnormalities and poor metabolic control in diabetes. Eur. J. Intern. Med. 2009, 20, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Salek, A.K.M.; Mamun, M.A.A.; Haque, M.A.; Mannan, M.; Ali, E.; Islam, S.; Rizvi, A.N.; Chowdhury, A.Z.; Islam, J.; Rahman, M.H.; et al. Serum triglyceride level in type 2 diabetes mellitus patients with or without frozen shoulder. Bangladesh Med. Res. Counc. Bull. 2010, 36, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Schulte, L.; Roberts, M.S.; Zimmerman, C.; Ketler, J.; Simon, L.S. A quantitative assessment of limited joint mobility in patients with diabetes. Goniometric analysis of upper extremity passive range of motion. Arthritis Rheum. 1993, 36, 1429–1443. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.M.; Clark, B.R.; McGill, J.B.; Lang, C.E.; Maynard, J.; Mueller, M.J. Relationship Between Skin Intrinsic Fluorescence—An Indicator of Advanced Glycation End Products—And Upper Extremity Impairments in Individuals with Diabetes Mellitus. Phys.Ther. 2015, 95, 1111–1119. [Google Scholar] [CrossRef]
- Shah, K.M.; Clark, B.R.; McGill, J.B.; Lang, C.E.; Mueller, M.J. Shoulder limited joint mobility in people with diabetes mellitus. Clin. Biomech. 2015, 30, 308–313. [Google Scholar] [CrossRef]
- Siu, K.K.; Zheng, L.B.; Ko, J.Y.; Wang, F.S.; Wang, C.J.; Wong, T.; Chou, W.Y. Increased interleukin 1β levels in the subacromial fluid in diabetic patients with rotator cuff lesions compared with nondiabetic patients. J. Shoulder Elb. Surg. 2013, 22, 1547–1551. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Kim, J.-M.; Lee, Y.-G.; Hong, O.-K.; Kwon, H.-S.; Ji, J.-H. Intercellular adhesion molecule-1 (ICAM-1, CD54) is increased in adhesive capsulitis. J. Bone Jt. Surg. Am. 2013, 95, e18. [Google Scholar] [CrossRef]
- Sattar, M.A.; Luqman, W.A. Periarthritis: Another duration-related complication of diabetes mellitus. Diabetes Care 1985, 8, 507–510. [Google Scholar] [CrossRef]
- Bridgman, J.F. Periarthritis of the shoulder and diabetes mellitus. Ann. Rheum. Dis. 1972, 31, 69–71. [Google Scholar] [CrossRef]
- Escalante, A.; Lichtenstein, M.J.; Hazuda, H.P. Determinants of shoulder and elbow flexion range: Results from the San Antonio Longitudinal Study of Aging. Arthritis Care Res. 1999, 12, 277–286. [Google Scholar] [CrossRef]
- Withrington, R.H.; Girgis, F.L.; Seifert, M.H. A comparative study of the aetilogical factors in shoulder pain. Br. J. Rheumatol. 1995, 24, 24–26. [Google Scholar] [CrossRef] [PubMed]
- Yian, E.H.; Contreras, R.; Sodl, J.F. Effects of glycemic control on prevalence of diabetic frozen shoulder. J. Bone Jt. Surg. Am. 2012, 94, 919–923. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar]
- Courties, A.; Sellam, J.; Berenbaum, F. Metabolic syndrome-associated osteoarthritis. Curr. Opin. Rheumatol. 2017, 29, 214–222. [Google Scholar] [CrossRef]
- Burner, T.; Gohr, C.; Mitton-Fitzgerald, E.; Rosenthal, A.K. Hyperglycemia reduces proteoglycan levels in tendons. Connect. Tissue Res. 2012, 53, 535–541. [Google Scholar] [CrossRef]
- Thomas, S.J.; Sarver, J.J.; Yannascoli, S.M.; Tucker, J.J.; Kelly, J.D.; Ahima, R.S.; Barbe, M.F.; Soslowsky, L.J. Effect of isolated hyperglycemia on native mechanical and biologic shoulder joint properties in a rat model. J. Orthop. Res. 2014, 32, 1464–1470. [Google Scholar] [CrossRef]
- De la Serna, D.; Navarro-Ledesma, S.; Alayón, F.; López, E.; Pruimboom, L. A Comprehensive View of Frozen Shoulder: A Mystery Syndrome. Front. Med. 2021, 8, 663703. [Google Scholar] [CrossRef]
- Kelley, M.J.; McClure, P.W.; Leggin, B.G. Frozen shoulder: Evidence and a proposed model guiding rehabilitation. J. Orthop. Sports Phys. Ther. 2009, 39, 135–148. [Google Scholar] [CrossRef]
- Januszewski, A.; Alderson, N.; Metz, T.; Thorpe, S.; Baynes, J. Role of lipids in chemical modification of proteins and development of complications in diabetes. Biochem. Soc. Trans. 2003, 31, 1413–1416. [Google Scholar] [CrossRef]
- DeGroot, J. The AGE of the matrix: Chemistry, consequence and cure. Curr. Opin. Pharmacol. 2004, 4, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Baynes, J.W. Chemical modification of proteins by lipids in diabetes. Clin. Chem. Lab. Med. 2003, 41, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Vlassara, H.; Cai, W.; Crandall, J.; Goldberg, T.; Oberstein, R.; Dardaine, V.; Peppa, M.; Rayfield, E.J. Inflammatory mediators are induced by dietary glycotoxins, a major risk factor for diabetic angiopathy. Proc. Natl. Acad. Sci. USA 2002, 99, 15596–15601. [Google Scholar] [CrossRef] [PubMed]
- Park, H.B.; Gwark, J.Y.; Kam, M.; Jung, J. Association between fasting glucose levels and adhesive capsulitis in a normoglycemic population: A case-control study. J. Shoulder Elb. Surg. 2020, 29, 2240–2247. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Title | Design | Sample | Outcome | Results |
|---|---|---|---|---|
| Abate et al. (2011) [26] | Case control | Group 1: 30 subjects with NIDDM type Il and good glycemic control (age 73.9 ± 12.72) Group 2: 30 subjects without DM matched for age and gender (159 age 74.3 ± 4.24) group 3: 10 normal young subjects (age 26.3 ± 1.6) | /a/ROM (goniometer) US evaluation SST | ROM (ABD & FL) reduced in both group 1 and 2 vs. 3 (p < 0.001); ROM (ABD & FL) reduced in group 1 vs. 2 (p < 0.001). More US abnormalities in group 1 vs. 2. |
| Abate et al. (2010) [27] | Case control | Group 1: 48 asymptomatic subjects with NIDDM type Il (age 71.5 ± 4.8) Group 2: 32 asymptomatic subjects, matched for age and sex, without NIDDM (age 70.7 ± 4.5) | US evaluation SST, IST, SScT, BT and SAD | SST and BT thickness greater in DM group (p < 0.001). More frequent observed degeneration in rotator cuff and BT in DM group (p < 0.002). Increased rate of SST tears in DM group (p < 0.03). More effusions in SAD (p < 0.03) and tenosynovitis in BT (p < 0.001) in the DM group. Pathological findings prevalent in both groups, but not related with duration of DM |
| Balci et al. (1999) [28] | Cross sectional | 297 subjects with DM type Il Group 1: 86 subjects DM type Il and adhesive capsulitis (age 59.23 ± 24 Group 2: 211 subjects DM type Il without adhesive capsulitis (age 53.6 ± 10.2) | /p/ROM (goniometer): ABD, IR, Blood samples | FS associated with reduced/p/ROM (p = 0.006), the age (p = 0.000), and duration of DM (p = 0.03). |
| Cole A et al. (2009) [8] | Cross sectional | 3206 subjects (of which 682 with shoulder pain and/or stiffness; 221 with DM (age 20–95; median 45) | ROM (inclinometer, visual): SPADI-questionnaire Blood samples | DM patients (or elevated HbA1c levels) had higher prevalence of shoulder pain and/or stiffness (p = 0.02). |
| Czelusniak et al. (2012)) [29] | Cross sectional | 150 subjects with DM type Il (age 60.5 ± 12) | UCLA-m rating scale Blood samples | Pain present in 63,4% and dysfunction in 53.4%. No association between HbA1c and joint function, except for/a/FLROM and fasting blood glucose (p = 0.026) |
| Handa et al. (2003) [30] | Case control | Group 1: 14 subjects with rotator cuff disease and DM type Il (age 56.8 ± 7.2 yrs) Group 2: 53 subjects with rotator cuff disease without DM (age 54.9 ± 8.5 yrs) | Synovia specimens from subacromial bursa | Symptom duration not different between groups. Synovial proliferation more frequent in DM vs. non DM (p =0.0329) Shoulder joint contracture more frequent in DM vs. non DM (p = 0.0045) |
| Kang et al. (2010) [31] | case control | Group 1: 80 subjects with DM type Il and chronicshoulder pain (age 62.6) Group 2: 339 controls without DM type Il and chronic shoulder pain (age 56.9) | US evaluation rotator cuff | No difference in RC tearsor calcifying tendinopathy between DM vs non DM (p =ns) |
| Lee et al. (2015) [32] | Cross sectional | 107 subjects with FS (age 46–68) | Diabetes status, Kcap /p/ROM (goniometer): FL, ABD, ER | Kcap: DM = nDM (p = ns) Kcap was negatively correlated with/p/ROM (p < 0.005) |
| Mavrikakis et al. (1989) [33] | Case control | Group 1: 824 subjects with DM type Il (age 66.1 yrs) Group 2: 320 non DM controls matched for age and sex (age 65.7 yrs) | X rays of the shouldersblood sample | Calcific shoulder periarthritis in DM> non DM (p < 0.001) Serum mean values: DM = non DM (p = ns) |
| Mavrikakis et al. (1991) [34] | Case control | Group 1: 900 subjects with DM type Il (age 36–93 yrs) Group 2: 350 non DM controls matched for age and sex (age 34–87 yrs) | X rays of the shoulders blood sample | 3× more frequent calcific shoulder periarthritis in DM vs. non DM, associated with longstanding/poorly controlled DM, hypercholesterolemia, and hypertriglyceridemia. |
| Ramchurn et al. (2009) [35] | Cross sectional | Group 1: 96 subjects with DM (46 type I & 50 with type Il) Group 2: 100 controls | HAQ health assessment questionnaire) Blood sample | Shoulder capsulitis (25%), carpal tunnel syndrome (20%), tenosynovitis (29%), limited joint mobility (28%) and Dupuytrens contracture (13%) more prevalent in DM vs. non DM (p = 0.02); Mean HbA1c was higher in patients with combined shoulder and hand problems (9.1%) than in those with no upper limb problems (8.0%) (p = 0.018). No differences between type 1 and 2. |
| Salek et al. (2010) [36] | Case control | Group 1: 30 subjects with DM type Il with FS Group 2: 30 matched type Il DM without frozen shoulder | Blood sample | Fasting blood sugar (p = 0.012) and blood sugar 2 h after breakfast (p < 0.01), HbA1C (p < 0.05) and serum triglyceride levels (p < 0.001) were elevated in group 1 vs. group. |
| Schulte et al. (1993) [37] | Cross sectional | Group 1: 70 IDDM (age 38.4 yrs +/− 12.8) Group 2: 70 non DM matched controls (age 40.1 yrs +/− 13.3) | /p/ROM (goniometry): FL, EXT, ADD, ER, IR | In general, 6.1% lesser shoulder mobility in DM vs. non DM (p < 0.01) |
| Shah et al. (2015) [38] | case control | Group 1: 26 subjects with DM type Il (age 64.5) Group 2: 26 matched non DM (age 64.2) | SIF, ultrasound evaluation, /a/ROM (Flock of Birds), Shoulder FL strength (dynamometer), DASH. | The mean SIF measure was higher in DM vs. non DM controls (p = 0.047). The BT and SST were 47% and 31% thicker (p < 0.001), respectively, in DM vs. non DM. Reduced shoulder elevation and ER in DM vs. non DM (p < 0.01). Shoulder FL strength was reduced by 27% (p = 0.004) in DM vs non DM. DM showed higher disabilities (DASH) than non DM (p < 0.01). |
| Shah et al. (2015) [39] | Case control | Group 1: 26 subjects with DM type Il (age 64.5) Group 2: 26 matched non DM (age 64.2) | /a/ROM (Flock of Birds), SPADI, DASH. | DM showed higher pain and disabilities (SPADI & DASH) vs. non DM (p < 0.01). Decreased shoulder EL and ER in DM vs. non DM (p < 0.05). No between groups difference in scapular upward rotation, or shoulder IR (p > 0.05) |
| Siu et al. (2013) [40] | Case control | Group 1: 23 with DM; Group 2: 45 non DM. All subjects had with rotator cuff tearing based on MRI or sonographic findings. | Sum of ROM deficit score, Constant score, VAS score, subacromial synovial fluid collection | DM had increased subacromial IL-1β levels (p = 0.048), increased Sum of ROM deficit (p < 0.001) and increased VAS scores (p = 0.022) and lower Constant scores (p < 0.001) than non DM. |
| Studies | ltems | Quality | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Score | ||
| Abate et al. (2011) [26] | + | + | + | + | + | + | + | + | + | 9/9 | B |
| Abate et al. (2010) [27] | + | + | + | + | + | + | + | + | + | 9/9 | B |
| Handa et al. (2003) [30] | + | + | − | + | + | − | + | + | + | 7/9 | B |
| Kang et al. (2010) [31] | + | + | − | − | + | + | − | + | + | 6/9 | B |
| Kim et al. (2013) [41] | − | + | − | + | − | − | + | + | − | 5/9 | B |
| Mavrikakis et al. (1989) [33] | + | + | + | + | + | + | + | + | + | 9/9 | B |
| Mavrikakis et al. (1991) [34] | + | + | + | + | + | + | + | + | + | 9/9 | B |
| Salek et al. (2010) [36] | + | + | + | + | − | − | + | + | + | 7/9 | B |
| Sattar et al. (1985) [42] | + | + | − | − | − | − | + | + | + | 5/9 | B |
| Shahet al. (2015) [38] | − | + | + | + | + | + | + | + | + | 8/9 | B |
| Shah et al. (2015) [39] | − | + | + | + | + | + | + | + | + | 8/9 | B |
| Siu et al. (2013) [40] | − | + | − | + | − | − | + | + | + | 6/9 | B |
| Selection 1: Is the case definition adequate? 2: Representativeness of the cases 3: Selection of controls. 4: Definition of controls | |||||||||||
| Comparability 5+6: Comparability of cases and controls on the basis of the the design or analysis | |||||||||||
| Exposure 7: Ascertainment of exposure 8: Same method of ascertainment for cases and controls 9: Non-Responserate | |||||||||||
| Studies | ltems | Quality | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | Score | ||
| Balci et al. (1999) [28] | + | + | + | − | − | + | + | − | + | 6/9 | C |
| Bridgman et al. (1972) [43] | + | − | + | − | − | + | + | − | + | 5/9 | C |
| Cole et al. (2009) [8] | + | + | + | + | − | + | + | + | + | 8/9 | C |
| Czelusniak et al. (2012) [29] | + | − | + | + | − | + | + | − | + | 6/9 | C |
| Escalente et al. (1999) [44] | − | + | + | − | − | − | + | + | + | 5/9 | C |
| Lee et al. (2015) [32] | + | + | + | + | − | + | + | + | + | 8/9 | C |
| Ramchurn et al. (2009) [35] | − | + | − | + | + | + | + | − | + | 6/9 | C |
| Schulte et al. (1993) [37] | + | + | + | + | − | + | + | + | + | 8/9 | C |
| Withrington et al. (1985) [45] | − | − | − | − | − | + | − | − | + | 2/9 | C |
| Yian et al. (2012) [46] | + | + | + | + | − | + | + | + | + | 8/9 | C |
| Selection bias 1: Did the study apply inclusion/exclusion criteria uniformly to all comparison groups? 2: Does the design or analysis control account for important confounding and modifying variables through matching, stratification, multivariable analysis, or other approaches? | |||||||||||
| Performance bias 3: Did researchers rule out any impact from a concurrent intervention or an unintended exposure that might bias results? | |||||||||||
| Attrition bias 4: If attrition (overall or differential non response, dropout, loss to follow-up, or exclusion of participants) was a concern, were missing data handled appropriately (e.g., intention-to-treat analysis and imputation)? | |||||||||||
| Detection of bias 5: Were the outcome assessors blinded to the intervention or exposure status of participants? 6: Were interventions/exposures assessed/defined using valid and reliable measures, implemented consistently across all study participants? 7: Were outcomes assessed/defined using valid and reliable measures, implemented consistently across all study participants? 8: Were confounding variables assessed using valid and reliable measures, implemented consistently across all study participants? | |||||||||||
| Reporting bias 9: Were the potential outcomes prespecified by the researchers? Are all prespecified outcomes reported? | |||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Struyf, F.; Mertens, M.G.; Navarro-Ledesma, S. Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature. Int. J. Environ. Res. Public Health 2022, 19, 6228. https://doi.org/10.3390/ijerph19106228
Struyf F, Mertens MG, Navarro-Ledesma S. Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature. International Journal of Environmental Research and Public Health. 2022; 19(10):6228. https://doi.org/10.3390/ijerph19106228
Chicago/Turabian StyleStruyf, Filip, Michel GCAM Mertens, and Santiago Navarro-Ledesma. 2022. "Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature" International Journal of Environmental Research and Public Health 19, no. 10: 6228. https://doi.org/10.3390/ijerph19106228
APA StyleStruyf, F., Mertens, M. G., & Navarro-Ledesma, S. (2022). Causes of Shoulder Dysfunction in Diabetic Patients: A Review of Literature. International Journal of Environmental Research and Public Health, 19(10), 6228. https://doi.org/10.3390/ijerph19106228