
On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process

 , ,
, ,
Abstract
:1. Introduction
1.1. Epidemiology, General Aspects, and Oral Health in Older People
1.2. Objective of the Present Work
2. Materials and Methods
2.1. Methodology
2.2. Transition Models in General
2.3. Core Elements and Processes of a Transition Process
3. Results
3.1. Transition Levels
3.2. Development of Terms of Transitional Dentistry
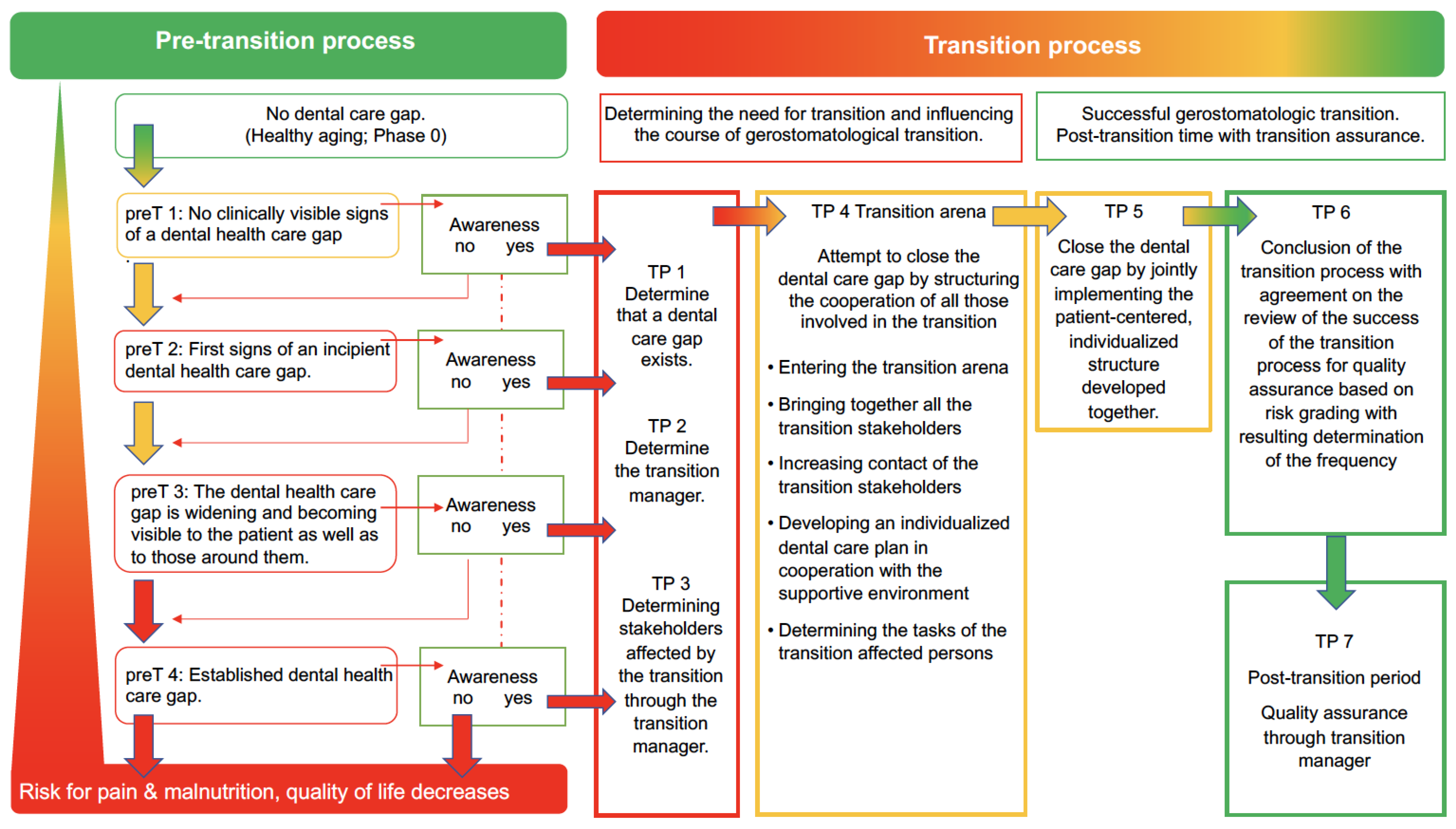
3.3. The Geriatric Oral Health Care Transition (GOHCT) Model
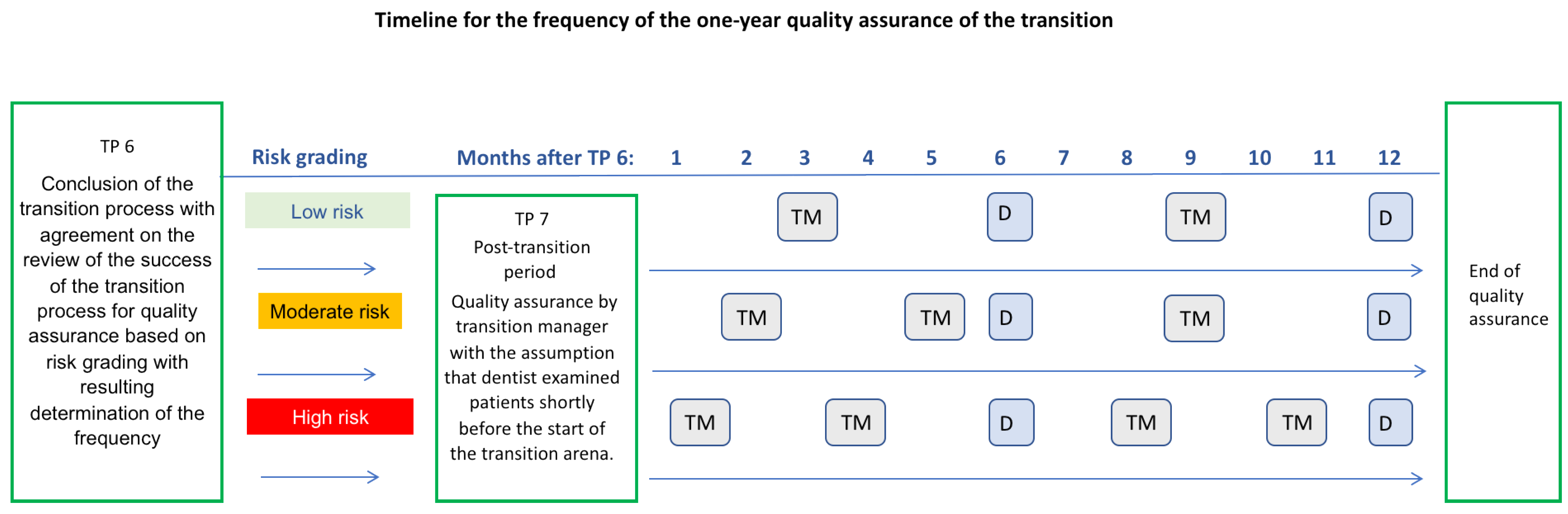
3.4. Risk Grading within the Framework of Quality Assurance
- If no risk factors or one risk factor are identified for the patient, the quality assurance of the transition results in a quality control check by the transition manager every 2–4 months after the last routine dental examination (at least twice a year).
- If at least two risk factors are identified, a medium risk is present. A quality control check should be performed every 4 months after completion of the transition.
- If more than two risk factors are present, there is a high risk. A quality control check should be performed every 3 months after completion of the transition.
4. Discussion
4.1. Notes on the Population-Representative Oral Health Care Transition Model
4.2. Notes on the Individual, Patient-Adapted Oral Health Care Transition Model
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gesellschaft für Transitionsmedizin e.V. Transition von der Pädiatrie in die Erwachsenenmedizin. S3-Leitlinie der. Gesellschaft für Transitionsmedizin. 2021. Available online: https://www.awmf.org/uploads/tx_szleitlinien/186-001l_S3_Transition_Paediatrie_Erwachsenenmedizin_2021-04.pdf (accessed on 9 May 2022).
- Odone, A.; Gianfredi, V.; Vigezzi, G.P.; Amerio, A.; Ardito, C.; d’Errico, A.; Stuckler, D.; Costa, G.; Italian Working Group on Retirement and Health. Does retirement trigger depressive symptoms? A systematic review and meta-analysis. Epidemiol. Psychiatr. Sci. 2021, 30, e77. [Google Scholar] [CrossRef]
- Bundesinstitut für Bevölkerungsforschung. Anteil der Altersgruppen unter 20 Jahren, ab 65 Jahre und ab 80 Jahre (1871–2060). 2021. Available online: https://www.bib.bund.de/DE/Fakten/Fakt/B15-Altersgruppen-Bevoelkerung-1871-Vorausberechnung.html (accessed on 5 April 2022).
- Lenz, E. Prävalenzen Zu ausgewählten klinischen Variablen bei Senioren (65–74 Jahre): Zahnprothetischer Status bei den Senioren. In Deutsche Mundgesundheitsstudie (DMS III). Ergebnisse, Trends und Problemanalysen auf der Grundlage Bevölkerungsrepräsentativer Stichproben in Deutschland 1997; Deutscher Zahnärzteverlag DÄV: Köln, Germany, 1999; pp. 385–411. [Google Scholar]
- Kerschbaum, T. Zahnverlust und Prothetische Versorgung. In Vierte Deutsche Mundgesundheitsstudie (DMS IV); Deutscher Zahnärzte Verlag: Köln, Germany, 2006; Volume 31, pp. 354–373. [Google Scholar]
- Nitschke, I.; Stark, H. Krankheits-und Versorgungsprävalenzen bei jüngeren Senioren (65-Bis 74-Jährige): Zahnverlust und prothetische Versorgung. In Fünfte Deutsche Mundgesundheitsstudie (DMS V); Deutscher Zahnärzte Verlag: Köln, Germany, 2016; pp. 416–451. ISBN 978-3-7691-0020-4. [Google Scholar]
- Kocher, T.; Hoffmann, T. Parodontalerkrankungen. In Fünfte Deutsche Mundgesundheitsstudie; Deutscher Zahnärzte Verlag: Köln, Germany, 2016; pp. 503–516. [Google Scholar]
- Barmer. BARMER Zahnreport 2020. Available online: https://www.barmer.de/presse/infothek/studien-und-reporte/zahnreporte/zahnreport-2020-1058930 (accessed on 5 April 2022).
- Kiyak, H.A.; Reichmuth, M. Barriers to and enablers of older adults’ use of dental services. J. Dent. Educ. 2005, 69, 975–986. [Google Scholar] [CrossRef] [PubMed]
- Bundesministerium der Justiz. Sozialgesetzbuch (SGB)—Elftes Buch (XI)—Soziale Pflegeversicherung; Artikel 1 Des Gesetzes Vom 26. Mai 1994, BGBl. I S. 1014; Bundesministerium der Justiz: Berlin, Germay, 2014.
- DESTATIS (Statistisches Bundesamt, Wiesbaden) Pflegestatistik. Pflege Im Rahmen Der Pflegeversicherung. Ländervergleich—Pflegebedürftige. 2019. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Gesundheit/Pflege/Publikationen/Downloads-Pflege/laender-pflegebeduerftige-5224002199004.pdf;jsessionid=F89F477E7B32F748A489AB550BD4E1C8.live742?__blob=publicationFile (accessed on 5 April 2022).
- Bundesministerium für Gesundheit. Pflege-Wissen. Pflegegrade und Neuer Pflegebedürftigkeitsbegriff. 2020. Available online: http://www.pflegestaerkungsgesetz.de/pflege-wissen-von-a-bis-z/pflege-details/erklaerung/pflegegrade-und-neuer-pflegebeduerftigkeitsbegriff/ (accessed on 5 April 2022).
- Lauritano, D.; Moreo, G.; Della Vella, F.; Di Stasio, D.; Carinci, F.; Lucchese, A.; Petruzzi, M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4558. [Google Scholar] [CrossRef] [Green Version]
- Rapp, L.; Sourdet, S.; Vellas, B.; Lacoste-Ferré, M.-H. Oral Health and the Frail Elderly. J. Frailty Aging 2017, 6, 154–160. [Google Scholar] [CrossRef]
- Nitschke, I.; Micheelis, W. Krankheits-und Versorgungsprävalenzen bei älteren Senioren mit Pflegebedarf. In Fünfte Deutsche Mundgesundheitsstudie (DMS V); Institut der Deutschen Zahnärzte (IDZ): Köln, Germany, 2016; pp. 557–578. [Google Scholar]
- Frese, C.; Zenthöfer, A.; Aurin, K.; Schoilew, K.; Wohlrab, T.; Sekundo, C. Oral Health of Centenarians and Supercentenarians. J. Oral Sci. 2020, 62, 9–12. [Google Scholar] [CrossRef] [Green Version]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Mercer, A.J. Updating the Epidemiological Transition Model. Epidemiol. Infect. 2018, 146, 680–687. [Google Scholar] [CrossRef] [Green Version]
- Alexandersson, G. The Demographic Transition: Model and Reality. Fennia 1981, 159, 35–42. [Google Scholar]
- Inaba, H.; Saito, R.; Bacaër, N. An Age-Structured Epidemic Model for the Demographic Transition. J. Math. Biol. 2018, 77, 1299–1339. [Google Scholar] [CrossRef]
- Hirschman, K.B.; Shaid, E.; McCauley, K.; Pauly, M.V.; Naylor, M.D. Continuity of Care: The Transitional Care Model. Online J. Issues Nurs. 2015, 20, 1. [Google Scholar] [CrossRef]
- Arora, V.; Gangireddy, S.; Mehrotra, A.; Ginde, R.; Tormey, M.; Meltzer, D. Ability of Hospitalized Patients to Identify Their In-Hospital Physicians. Arch. Intern. Med. 2009, 169, 199–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krumholz, H.M. Post-Hospital Syndrome—An Acquired, Transient Condition of Generalized Risk. N. Engl. J. Med. 2013, 368, 100–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogeli, C.; Shields, A.E.; Lee, T.A.; Gibson, T.B.; Marder, W.D.; Weiss, K.B.; Blumenthal, D. Multiple Chronic Conditions: Prevalence, Health Consequences, and Implications for Quality, Care Management, and Costs. J. Gen. Intern. Med. 2007, 22, 391–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumacher, K.L.; Meleis, A.I. Transitions: A Central Concept in Nursing. Image J. Nurs. Sch. 1994, 26, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Morkisch, N.; Upegui-Arango, L.D.; Cardona, M.I.; van den Heuvel, D.; Rimmele, M.; Sieber, C.C.; Freiberger, E. Components of the Transitional Care Model (TCM) to Reduce Readmission in Geriatric Patients: A Systematic Review. BMC Geriatr. 2020, 20, 345. [Google Scholar] [CrossRef] [PubMed]
- Schapira, M.; Outumuro, M.B.; Giber, F.; Pino, C.; Mattiussi, M.; Montero-Odasso, M.; Boietti, B.; Saimovici, J.; Gallo, C.; Hornstein, L.; et al. Geriatric Co-Management and Interdisciplinary Transitional Care Reduced Hospital Readmissions in Frail Older Patients in Argentina: Results from a Randomized Controlled Trial. Aging Clin. Exp. Res. 2022, 34, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Mennito, S.H.; Clark, J.K. Transition Medicine: A Review of Current Theory and Practice. South Med. J. 2010, 103, 339–342. [Google Scholar] [CrossRef]
- Berens, J.; Wozow, C.; Peacock, C. Transition to Adult Care. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 159–170. [Google Scholar] [CrossRef]
- Berrouiguet, S.; Perez-Rodriguez, M.M.; Larsen, M.; Baca-García, E.; Courtet, P.; Oquendo, M. From EHealth to IHealth: Transition to Participatory and Personalized Medicine in Mental Health. J. Med. Internet Res. 2018, 20, e2. [Google Scholar] [CrossRef]
- Gesellschaft für Transitionsmedizin e.V. Ziele Der “Gesellschaft für Transitionsmedizin e.V.”. Available online: https://transitionsmedizin.net/index.php/ueber-uns/verein/unsere-ziele (accessed on 5 April 2022).
- Virtuelle Unternehmen. Transitionskompetenz. 2022. Available online: https://virtuelleunternehmen.wordpress.com/web-dossier-das-virtuelle-unternehmen/kapitel-drei/transitionskompetenz/ (accessed on 5 April 2022).
- Schneidewind, U. Wie Systemübergänge nachhaltig gestaltet werden können. Ökologisches Wirtschaften-Fachzeitschrift 2010, 25. [Google Scholar] [CrossRef] [Green Version]
- Hafkesbrink, J.; Evers, J.; Knipperts, J.; Spitzner, G.; Wöhrmann, T. Transition-Management-Modell “Demografischer Wandel und Innovationsfähigkeit”; RIAS eV.: Duisburg, Germany, 2015. [Google Scholar]
- Nitschke, I.; Hahnel, S.; Jockusch, J. Health-Related Social and Ethical Considerations towards the Utilization of Dental Medical Services by Seniors: Influencing and Protective Factors, Vulnerability, Resilience and Sense of Coherence. Int. J. Environ. Res. Public Health 2021, 18, 2048. [Google Scholar] [CrossRef] [PubMed]
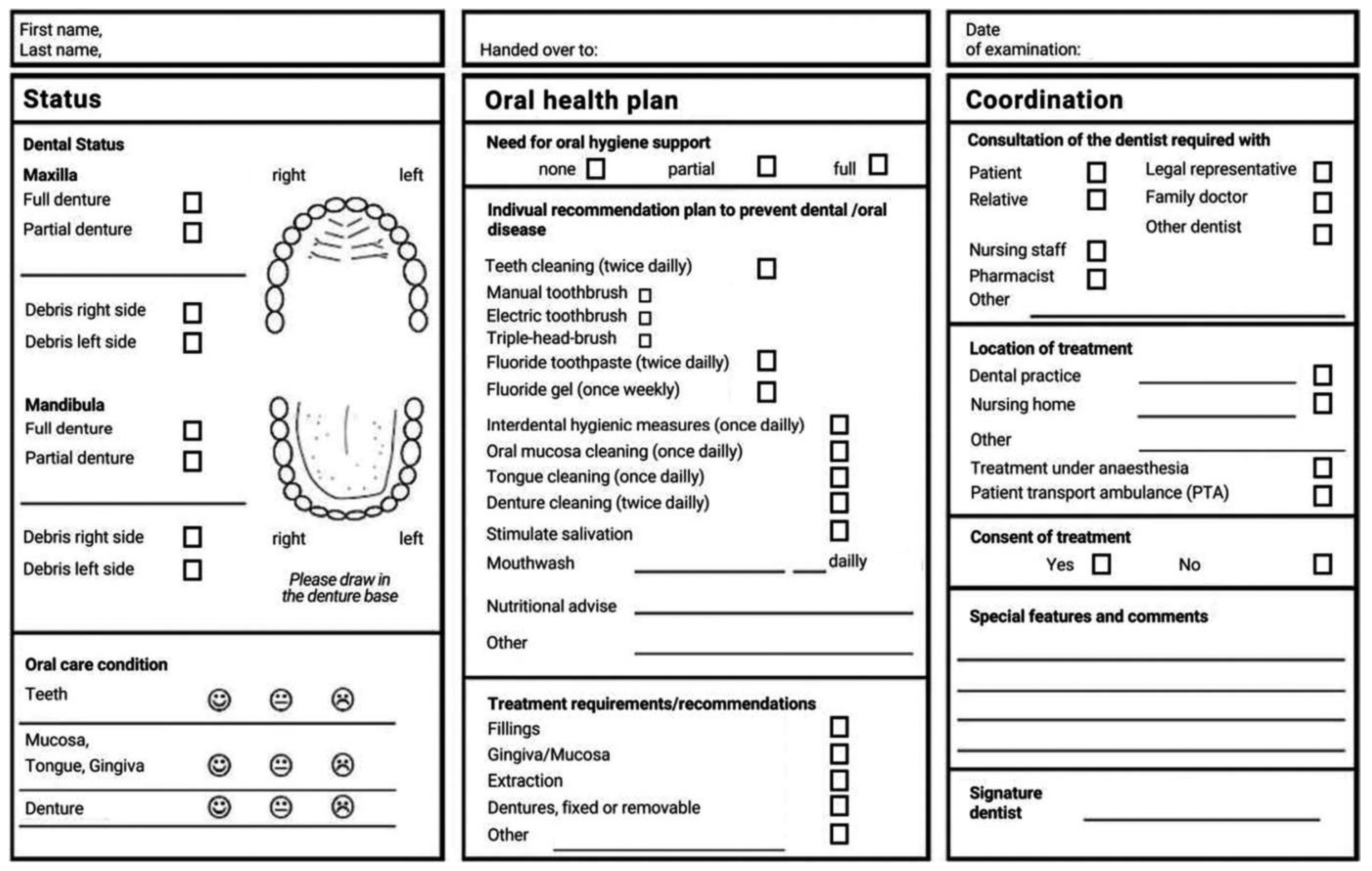
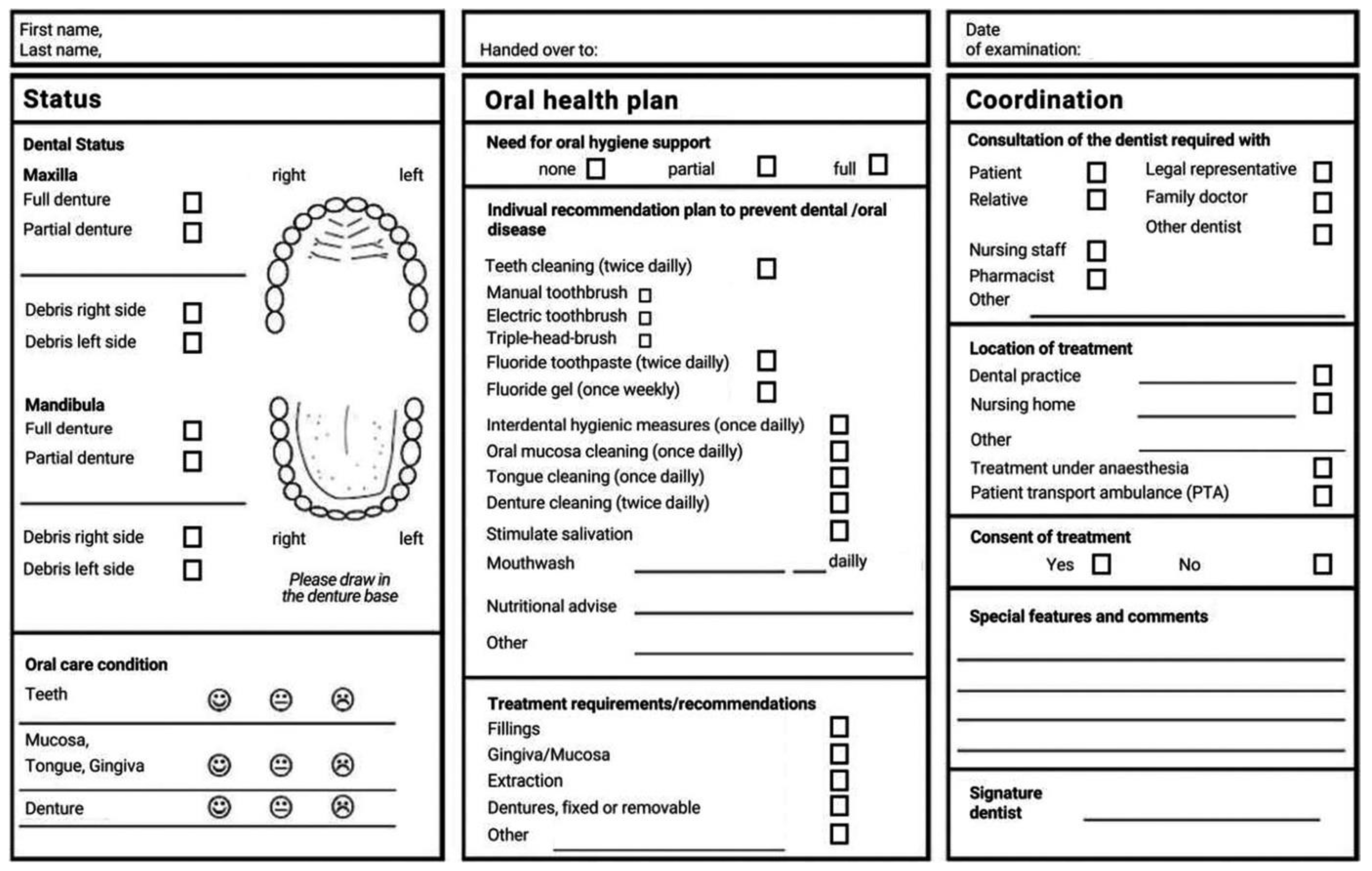
- Bleiel, D.; Nitschke, I.; Noack, M.J.; Barbe, A.G. Impact of Care Level, Setting and Accommodation Costs on a Newly Developed Oral Care Nursing Plan Format for Elderly Patients with Care Needs—Results from a Cross-Sectional Study. Int. J. Dent. Hyg. 2021. [Google Scholar] [CrossRef] [PubMed]
- León, S.; Giacaman, R.A. Proposal for a Conceptual Framework for the Development of Geriatric Dentistry. J. Dent. Res. 2022, 101, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, R.L.; Marchini, L. Cohort Differences among Aging Populations: An Update. J. Am. Dent. Assoc. 2020, 151, 519–526. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Sinjari, B.; Xhajanka, E.; Rexhepi, I.; Mangifesta, R.; Caputi, S. Access to Dental Care-A Survey from Dentists, People with Disabilities and Caregivers. Int. J. Environ. Res. Public Health 2021, 18, 1556. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Transitional dentistry | Transitional dentistry is not yet established, although various transitions exist in dentistry too. Securing dental care for children in transition to adolescence or later to adulthood, where, for example, some benefits from the statutory health insurance system expire, should be dealt with in transitional dentistry. People with disabilities and people with care needs require different dental care pathways than healthy adults. Dental services should also always be adapted to the differing clinical situations. Differing knowledge and experience of different stakeholders and attention to changes during the transition help to ensure quality dental care within the framework of transitional dentistry. |
| Dental transition models | In order to cope with relevant dental transitions, not only the competence of the individual dentist or patient is required, but the cooperation of all those involved during the transition. The transition model describes the tasks of those involved as well as the goals and the joint path to an optimal dental transition. In addition to specialist dental expertise, the competence of the social health care system is also required, and other disciplines are involved for the benefit of the oral health of the affected patient. |
| Gerostomatological transition | Structured support from dental treatment to dental care for people with a need for help or care when their own oral health competence is declining, with the aim of maintaining or restoring good individual oral health through substitution with other people’s oral health competence. The gerostomatological transition ensures dental care for seniors, regardless of their stage of life. |
| Transition competencies and skills | The competencies and skills needed to recognize and manage the need for transition are provided by various professionals within and outside of dentistry. These include dentists, dental hygienists, and dental assistants, as well as medical professionals (e.g., pediatricians, geriatricians). A successful transition in a crisis due to gaps in care is only possible if the competencies are present, to recognize and report such gaps. Family members, physicians, and/or caregivers, for example, can contribute to this end. Bringing transition competence into dental transition processes requires interdisciplinary cooperation on the part of those involved. In the dental context, it is important that participants in the transition do not nurture any prejudices against dentists—possibly stemming from dental phobias or negative experiences of their own—which could impair the group processes. Depending on the need for transition, a competent group must be found so that there is sufficient transition competence. |
| Transition stakeholders | The geriatric patient as a person in transition must emotionally cope with and allow the ever-necessary adjustments and recurring changes in his or her dental care. In doing so, he or she should also allow other people in the transition process to pick up his or her deficits as his oral hygiene ability deteriorates. This also includes, if independent use of dental services is no longer assured, that other people will ensure control-oriented dental attendance. All persons involved in the transition arena are transition stakeholders. |
| Transition manager | The transition manager may be the dentist or an employee of the dental practice of the geriatric patient, but other persons from the competence network are also conceivable as transition managers, e.g., nurses or relatives. He or she conceptually initiates the desired or necessary changes and implements them until the pre-agreed goals are achieved. |
| Transition arena | In the transition arena, the experiences, opinions, and expertise of all participants in the arena are exchanged and the problems of the patient or a group of geriatric patients are analyzed (e.g., people with pronounced dementia in a senior care facility). The arena is designed as a group meeting and facilitated by the development of a common language that allows all participants to exchange their ideas and perceptions of dental issues. There, problems are highlighted (e.g., no control-oriented utilization, refusal of oral hygiene measures by the caregiver), activities, such as the individual oral hygiene plan, are agreed upon, and a common way is identified to resolve the oral problems. Typically, professionals from many specialties are involved, who, in turn, can influence their own spheres. They must represent goals agreed upon internally in their own spheres and externally in the transition arena. The transition arena can be used to address the oral health of an individual patient, as well as oral health issues of defined groups with a population-based approach. |
| Transition level | The transition arena with the different transition levels can be used as a meeting point for both the oral health of an individual patient with individual needs (micro-level of health care) as well as for defined groups with dental problems (e.g., adolescents, people with dementia, patients with disabilities) with a population-representative approach (macro- and meso-level of health care). |
| Transition completion | The transition is completed when, for example, the dental care gap has been closed and adjustments to the care system have been organized. All those involved in the transition system, i.e., also the patient’s relatives and the patient himself, should feel comfortable, as the benefit of the transition is then recognizable for all stakeholders and the goals of the transition have been achieved. |
| Transition assurance | After the completion of the transition, the transition manager shall ensure that the quality of the transition is reviewed. Therefore, the patient’s risk of reoccurrence of a dental care gap and the patient’s supportive dental care gap as well as the patient’s supportive environment must be considered. The quality assurance measures carried out by the transition manager are standardized in the transition arena according to risk assessment and the existing support environment. |
| Geriatric Oral Health Care Transition Model | ||
|---|---|---|
| Superordinate Stages of Pre-Transition | Pretransition Phase | Description of Pretransition Stages. |
| I Healthy aging. | 0 |
|
| II Onset of gerostomatologic pretransition. First limitations, risk factors and morbidities on the part of the patient take effect | preT1 |
|
| III Progressing gerostomatological pre-transition. Increasing restrictions, reduced use of dental services and dental prophylaxis, deterioration of domestic oral and denture hygiene on the part of the patient Identifying other determining stakeholders of the gerostomatological transition on the part of the dentist | preT2 |
|
| preT3 |
| |
| preT4 |
| |
| Overarching Areas of Transition | Transition Phase | Description of the Transition Process |
| I Determining the need for transition. Transition can be determined at any stage (preT 1–4) | TP 1 |
|
| TP 2 |
| |
| TP 3 |
| |
| II Influencing the course of gerostomatological transition. Cooperation with the supportive environment and increasing contact with reference persons | TP 4 |
|
| TP 5 |
| |
| III Successful gerostomatologic transition. Structured collaboration in the supportive environment | TP 6 |
|
| IV Post-transition time with transition assurance. Quality management implementation | TP 7 |
|
| (A) | ||
| Risk Factor | Possible Specification of Risk | |
| Living situation | Death of partner or child Change in place of residence Change in support environment | |
| General medical | Diabetes mellitus Dementia Systemic diseases (e.g., chronic inflammatory diseases) Etc. | |
| Limitation of cognitive abilities | Restriction of therapeutic capability as of resilience level 3 [35] Reduced adaptability Reduced compliance with treatments and adherence to therapy instructions | |
| Medication with oral consequence | Saliva-reducing drugs (e.g., antidepressants) Bisphosphonates | |
| Limitation of dexterity reducing oral hygiene ability | Reduction of gripping ability Reduction of hand strength Uncorrected visual impairment (control of prosthetic plaque) | |
| Teeth | Dentate | |
| Dentures | Combined fixed–removable dentures Dentures with implants | |
| (B) | ||
| Number of Identified Individual Oral Risk Factors | Individualized Oral Risk | Classification of the Frequency of Quality Assurance Measures |
| No or one risk factor | Low risk | 2–4 months after last dental check-up (two times a year) |
| At least two risk factors | Moderate risk | every 4 months after completion of the transition (three times a year) |
| >Two risk factors | High risk | every 3 months after completion of the transition (four times a year) |
| Steps of the Transition | Tasks Requiring Time and Financial Resources |
|---|---|
| Preparation for the transition | Advanced training of the transition manager |
| Advanced training of the transition nurse | |
| Preparation of the meeting of the transition patient by the transition manager | |
| Assessment of the geriatric patient’s transition phase by the dentist | |
| Dentist’s documentation of transition needs | |
| Preparation of an oral health plan by the dentist | |
| Transition plan | Meeting with the transition stakeholders, sharing the wishes, needs and care options in the transition arena. |
| Determination of a collaborative approach to benefit the patient’s oral health, decide distribution of tasks within individual oral health plan | |
| Implementation of the adapted patient-centered oral health plan | |
| Risk grading (determining oral and general medical risk and identifying the supportive environment) to determine the frequency and content of quality assurance interventions | |
| Ensuring the quality of the transition | Transition quality assurance review by transition managers to determine if implementation of the plan is a reality for all transition stakeholders. Frequency of quality assurance after definition of risk grading in the transition arena. |
| Adjustment when new difficulties arise | |
| Semi-annual checks with dentist to see if patient is in transition stage 7 or whether new dental care difficulties have emerged with gaps in dental care. Decision between dentist and transition manager as to whether fine-tuning is possible within the next six months through a renewed organization between transition stakeholders, or whether a renewed convening of the transition stakeholders in the transition arena is necessary. After one year, quality assurance of the transition process is completed. In case a dental or nursing professional identifies a new dental care gap, transition phase 1 must be re-entered. |
Transition in the Population-Representative Approach.
|
Transition in a Patient-Oriented, Needs-Adapted Individual Approach
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitschke, I.; Nitschke, S.; Haffner, C.; Sobotta, B.A.J.; Jockusch, J. On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process. Int. J. Environ. Res. Public Health 2022, 19, 6148. https://doi.org/10.3390/ijerph19106148
Nitschke I, Nitschke S, Haffner C, Sobotta BAJ, Jockusch J. On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process. International Journal of Environmental Research and Public Health. 2022; 19(10):6148. https://doi.org/10.3390/ijerph19106148
Chicago/Turabian StyleNitschke, Ina, Siri Nitschke, Cornelius Haffner, Bernhard A. J. Sobotta, and Julia Jockusch. 2022. "On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process" International Journal of Environmental Research and Public Health 19, no. 10: 6148. https://doi.org/10.3390/ijerph19106148
APA StyleNitschke, I., Nitschke, S., Haffner, C., Sobotta, B. A. J., & Jockusch, J. (2022). On the Necessity of a Geriatric Oral Health Care Transition Model: Towards an Inclusive and Resource-Oriented Transition Process. International Journal of Environmental Research and Public Health, 19(10), 6148. https://doi.org/10.3390/ijerph19106148