
Psychological Flexibility Is Associated with Parental Stress in Relatives of People with Intellectual Disabilities



Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.4. Procedure
2.5. Statistical Analysis
3. Results
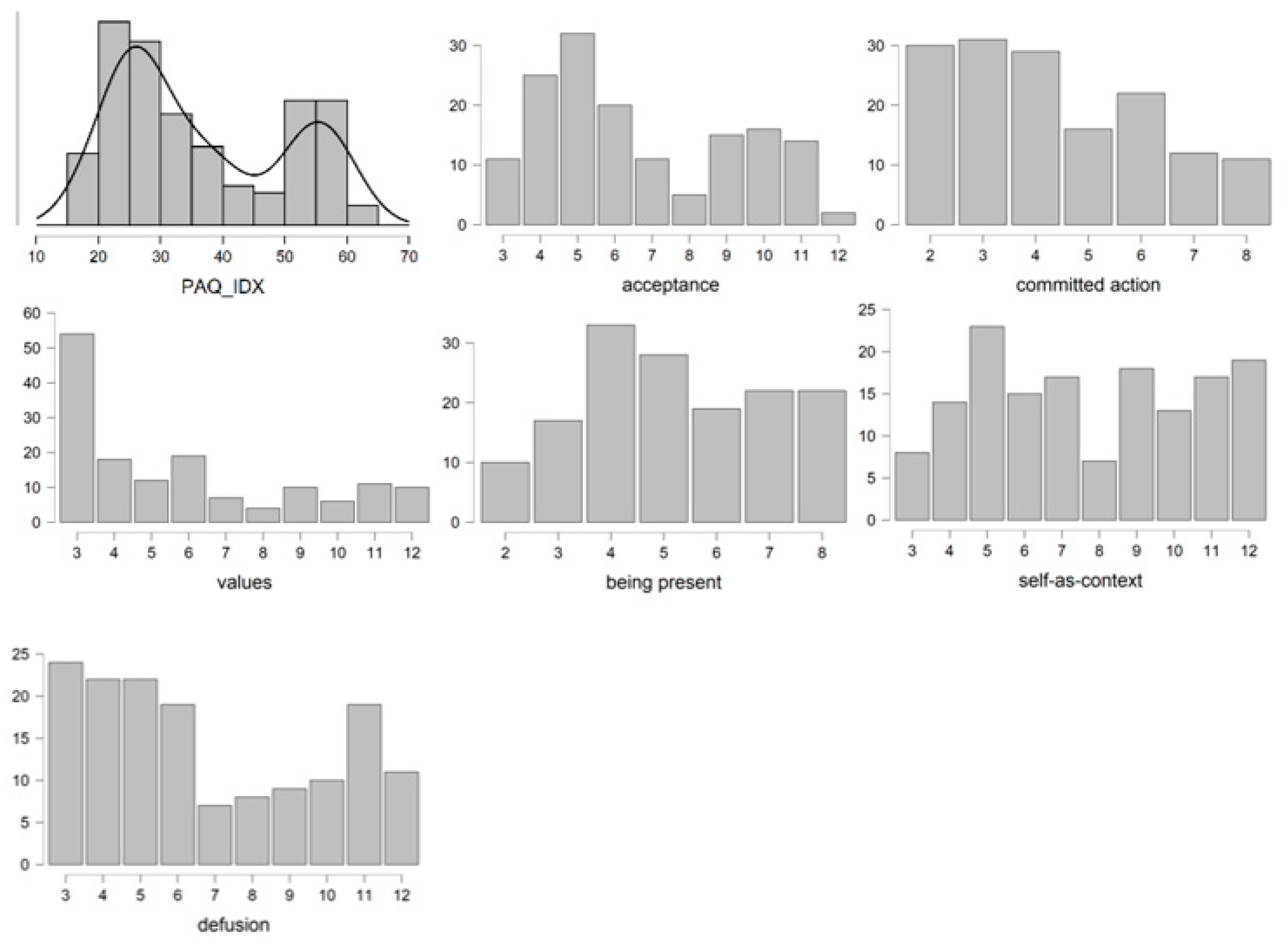
3.1. Descriptive Analysis
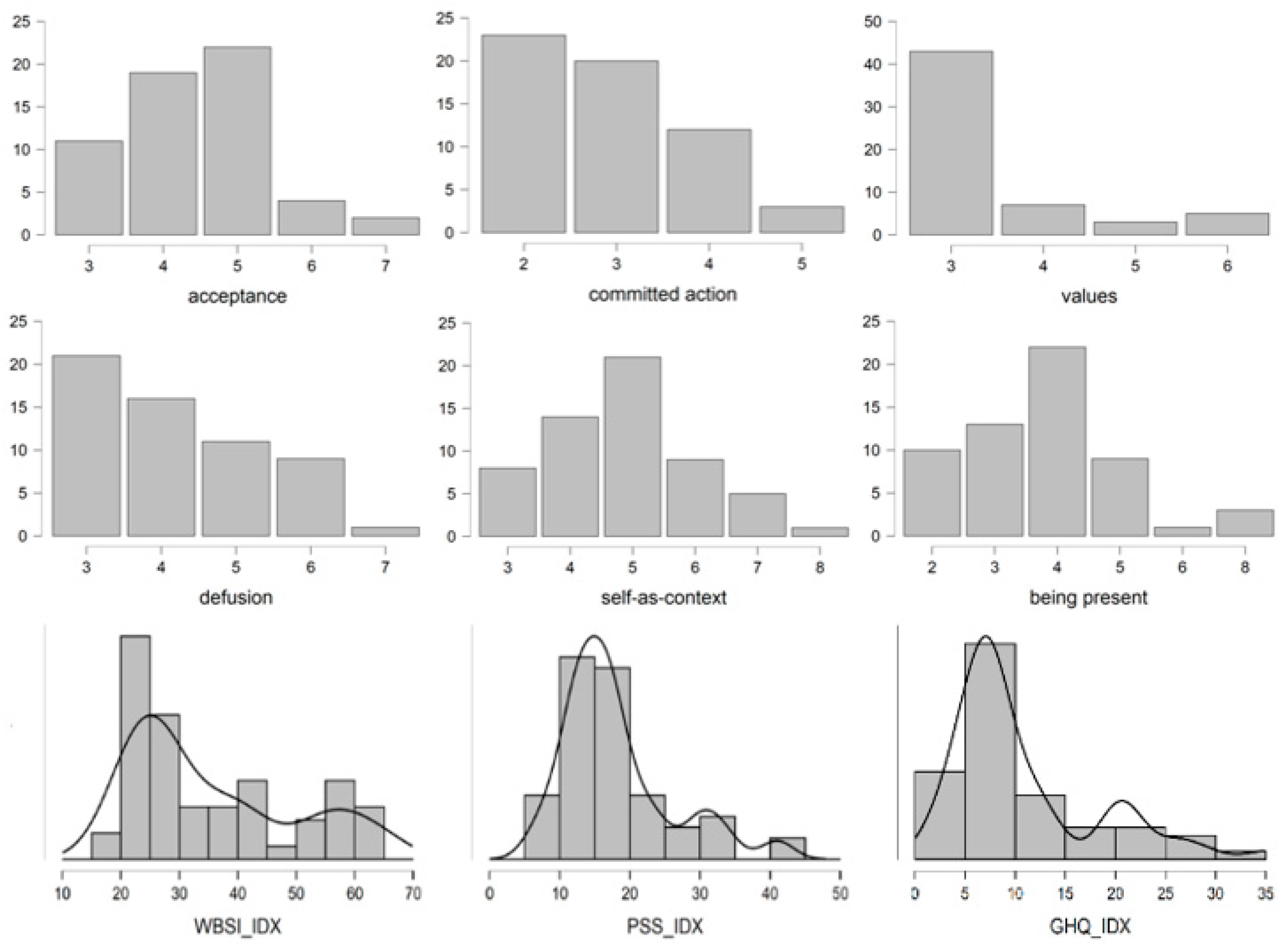
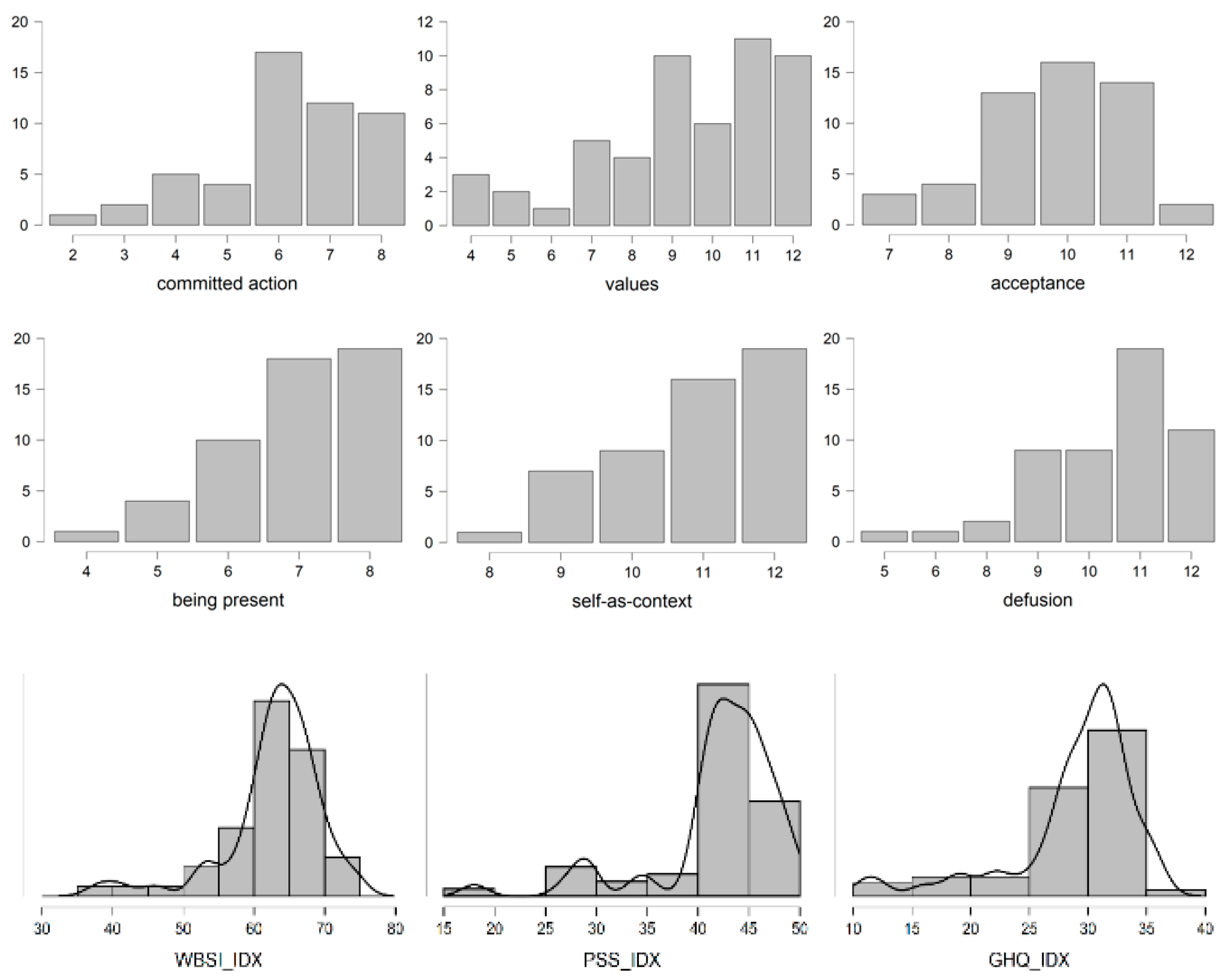
3.2. Analysis of the Scores of Participants That Reported Extreme Levels of PI
3.3. Correlation Analysis and Lineal Regression of the Complete Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Schalock, R.L.; Luckasson, R.; Tassé, M.J. An Overview of Intellectual Disability: Definition, Diagnosis, Classification, and Systems of Supports. Am. J. Intellect. Dev. Disabil. 2021, 126, 439–442. [Google Scholar] [CrossRef] [PubMed]
- Davis, N.O.; Carter, A.S. Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. J. Autism Dev. Disord. 2008, 38, 1278. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.A.; Watson, S.L. The impact of parenting stress: A meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J. Autism Dev. Disord. 2013, 43, 629–642. [Google Scholar] [CrossRef] [PubMed]
- Raina, P.; O’Donnell, M.; Schwellnus, H.; Rosenbaum, P.; King, G.; Brehaut, J.; Russell, D.; Swinton, M.; King, S.; Wong, M.; et al. Caregiving process and caregiver burden: Conceptual models to guide research and practice. BMC Pediatr. 2004, 4, 1. [Google Scholar] [CrossRef]
- Woodman, A.C.; Mawdsley, H.P.; Hauser-Cram, P. Parenting stress and child behavior problems within families of children with developmental disabilities: Transactional relations across 15 years. Res. Dev. Disabil. 2015, 36, 264–276. [Google Scholar] [CrossRef]
- Ngo, H.; Shin, J.Y.; Nhan, N.V.; Yang, L.H. Stigma and restriction on the social life of families of children with intellectual disabilities in Vietnam. Singap. Med. J. 2012, 53, 451–457. [Google Scholar]
- Brown, M.A.; McIntyre, L.L.; Crnic, K.A.; Baker, B.L.; Blacher, J. Preschool children with and without developmental delay: Risk, parenting, and child demandingness. J. Ment. Health Res. Intellect. Disabil. 2011, 4, 206–226. [Google Scholar] [CrossRef][Green Version]
- Emerson, E.; Shahtahmasebi, S.; Lancaster, G.; Berridge, D. Poverty transitions among families supporting a child with intellectual disability. J. Intellect. Dev. Disabil. 2010, 35, 224–234. [Google Scholar] [CrossRef]
- Scherer, N.; Verhey, I.; Kuper, H. Depression and anxiety in parents of children with intellectual and developmental disabilities: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219888. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Navas, P.; Verdugo, M.A.; Amor, A.M.; Crespo, M.; Martínez, S. COVID-19 y Discapacidades Intelectuales y del Desarrollo: Impacto del Confinamiento desde la Perspectiva de las Personas, sus Familiares y los Profesionales y Organizaciones que Prestan Apoyo; Plena inclusión España e Instituto Universitario de Integración en la Comunidad (INICO), Universidad de Salamanca: Salamanca, Spain, 2020. [Google Scholar]
- Gloster, A.T.; Walder, N.; Levin, M.; Twohig, M.; Karekla, M. The empirical status of acceptance and commitment therapy: A review of meta-analyses. J. Contextual Behav. Sci. 2020, 18, 181–192. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Terapia de Aceptación y Compromiso: Proceso y Práctica del Cambio Consciente (Mindfulness); Desclee de Brouwer: Bilbao, Spain, 2014. [Google Scholar]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.S.; Kearney, P.; Klieve, H.; Lang, W.; Roberts, J. Cultivating mind: Mindfulness interventions for children with autism spectrum disorder and problem behaviours, and their mothers. J. Child Fam. Stud. 2015, 24, 3093–3106. [Google Scholar] [CrossRef]
- Lewallen, A.C.; Neece, C.L. Improved social skills in children with developmental delays after parent participation in MBSR: The role of parent–child relational factors. J. Child Fam. Stud. 2015, 24, 3117–3129. [Google Scholar] [CrossRef]
- McConachie, D.A.J.; McKenzie, K.; Morris, P.G.; Walley, R.M. Acceptance and mindfulness-based stress management for support staff caring for individuals with intellectual disabilities. Res. Dev. Disabil. 2014, 35, 1216–1227. [Google Scholar] [CrossRef]
- Hastings, R.P. Do children with intellectual and developmental disabilities have a negative impact on other family members? The case for rejecting a negative narrative. Int. Rev. Res. Dev. Disabil. 2016, 50, 165–194. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Trujillo, H.M.; González-Cabrera, J. Propiedades psicométricas de la versión española de la “Escala de estrés percibido” (EEP). Psicol. Conduct. 2007, 15, 457–477. [Google Scholar]
- Greene, R.L.; Field, C.E.; Fargo, J.D.; Twohig, M.P. Development and validation of the parental acceptance questionnaire (6-PAQ). J. Contextual Behav. Sci. 2015, 4, 170–175. [Google Scholar] [CrossRef]
- Flujas-Contreras, J.M.; García-Palacios, A.; Gómez, I. Spanish validation of the parental acceptance questionnaire (6-PAQ). Int. J. Clin. Health Psychol. 2020, 20, 163–172. [Google Scholar] [CrossRef]
- Wegner, D.M.; Zanakos, S. Chronic thought suppression. J. Personal. 1994, 62, 615–640. [Google Scholar] [CrossRef]
- Rodríguez, M.G.; Delgado, P.A.; Rovella, A.T.; León, R.C. Structural validity and reliability of the Spanish version of the White Bear Suppression Inventory (WBSI) in a sample of the general Spanish population. Span. J. Psychol. 2008, 11, 650–659. [Google Scholar] [CrossRef]
- Goldberg, D.; Bridges, K. Screening for psychiatric illness in general practice: The general practitioner versus the screening questionnaire. J. R. Coll. Gen. Pract. 1987, 37, 15–18. [Google Scholar] [PubMed]
- del Pilar Sánchez-López, M.; Dresch, V. The 12-Item Psychological health Questionnaire (GHQ-12): Reliability, external validity and factor structure in the Spanish population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Daks, J.S.; Peltz, J.S.; Rogge, R.D. Psychological flexibility and inflexibility as sources of resiliency and risk during a pandemic: Modeling the cascade of COVID-19 stress on family systems with a contextual behavioral science lens. J. Contextual Behav. Sci. 2020, 18, 16–27. [Google Scholar] [CrossRef]
- Herr, R.M.; Li, J.; Loerbroks, A.; Angerer, P.; Siegrist, J.; Fischer, J.E. Effects and mediators of psychosocial work characteristics on somatic symptoms six years later: Prospective findings from the Mannheim Industrial Cohort Studies (MICS). J. Psychosom. Res. 2017, 98, 27–33. [Google Scholar] [CrossRef]
- Li, J.; Zhang, M.; Loerbroks, A.; Angerer, P.; Siegrist, J. Work stress and the risk of recurrent coronary heart disease events: A systematic review and meta-analysis. Int. J. Occup. Med. Environ. Health 2015, 28, 8–19. [Google Scholar] [CrossRef]
- Faber, J.; Schlarb, A. The Relation of Sleep, Distress, and Coping Strategies—What Male and Female Students Can Learn from Each Other? Health 2016, 8, 1356–1367. [Google Scholar] [CrossRef]
- Neece, C.L.; Green, S.A.; Baker, B.L. Parenting stress and child behavior problems: A transactional relationship across time. Am. J. Intellect. Dev. Disabil. 2012, 117, 48–66. [Google Scholar] [CrossRef]
- Wenzlaff, R.M.; Wegner, D.M. Thought suppression. Annu. Rev. Psychol. 2000, 51, 59–91. [Google Scholar] [CrossRef]
- McCaffrey, S.; Reitman, D.; Black, R. Mindfulness in Parenting Questionnaire (MIPQ): Development and validation of a measure of mindful parenting. Mindfulness 2017, 8, 232–246. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | M | SD |
|---|---|---|
| 6-PAQ Psychological Inflexibility-Total | 36.6 | 13.6 |
| 6-PAQ Acceptance | 6.6 | 2.5 |
| 6-PAQ Committed action | 4.3 | 1.8 |
| 6-PAQ Values | 5.8 | 3 |
| 6-PAQ Being present | 5.2 | 1.8 |
| 6-PAQ The self | 7.7 | 2.8 |
| 6-PAQ Defusion | 6.7 | 3 |
| PSS Perceived Stress | 29.4 | 12.4 |
| GHQ-12 Psychological health | 19.4 | 10.2 |
| WBSI Thought suppression | 48.2 | 6.5 |
| Variable | Group 1 (n = 58) | Group 2 (n = 52) | ||
|---|---|---|---|---|
| M (SD) | M (SD) | t | p | |
| 6-PAQ Psychological Inflexibility-Total | 23.6 (2.9) | 53.6 (5.5) | −36.091 | <0.001 |
| 6-PAQ Acceptance | 4.4 (0.9) | 9.7 (1.2) | −25.336 | <0.001 |
| 6-PAQ Committed action | 2,9 (0.9) | 6.1 (1.4) | −14.164 | <0.001 |
| 6-PAQ Values | 3.4 (0.9) | 9.3 (2.3) | −17.719 | <0.001 |
| 6-PAQ Being present | 3,8 (1.9) | 9.9 (1) | −13.228 | <0.001 |
| 6-PAQ The self | 4.8 (1.2) | 10.8 (1.1) | −26.948 | <0.001 |
| 6-PAQ Defusion | 4.1 (1.1) | 10.3 (1.4) | −24.447 | <0.001 |
| PSS Perceived Stress | 18 (7.8) | 42 (6.1) | −17.698 | <0.001 |
| GHQ-12 Psychological health | 10.7 (7.3) | 28.8 (5.4) | −14.578 | <0.001 |
| WBSI Thought suppression | 35.5 (14.2) | 62.7 (7) | −12.493 | <0.001 |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Psychological Inflexibility | - | |||
| 2. Perceived Stress | −0.075 | - | - | - |
| 3. Psychological Health | 0.066 | 0.801 *** | - | - |
| 4. Thought Suppression | −0.104 | 0.627 *** | 0.482 *** | - |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Psychological Inflexibility | - | - | - | - |
| 2. Perceived Stress | 0.660 *** | - | - | - |
| 3. Psychological Health | 0.794 *** | 0.827 *** | - | - |
| 4. Thought Suppression | 0.341 * | 0.413 ** | 0.460 *** | - |
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. 6 PAQ | - | ||||||||
| 2. Acceptance | 0.916 * | - | |||||||
| 3. Committed action | 0.827 * | 0.791 * | - | ||||||
| 4. Values | 0.915 * | 0.802 * | 0.815 * | - | |||||
| 5. Being present | 0.797 * | 0.694 * | 0.598 * | 0.635 * | - | ||||
| 6. Self-as-context | 0.916 * | 0.793 * | 0.673 * | 0.784 * | 0.692 * | - | |||
| 7. Defusion | 0.934 * | 0.824 * | 0.692 * | 0.832 * | 0.719 * | 0.837 * | - | ||
| 8. PSS | 0.827 * | 0.739 * | 0.709 * | 0.758 * | 0.594 * | 0.803 * | 0.762 * | - | |
| 9. GHQ | 0.783 * | 0.681 * | 0.688 * | 0.720 * | 0.588 * | 0.733 * | 0.731 * | 0.919 * | |
| 10. WBSI | 0.690 * | 0.649 * | 0.524 * | 0.593 * | 0.576 * | 0.668 * | 0.627 * | 0.804 * | 0.757 * |
| Unstandardized | Standardized | ||||
|---|---|---|---|---|---|
| β | Tip. Error | Beta | t | p | |
| IV: Parental stress | |||||
| 1. Self | 2.047 | 0.368 | 0.468 | 5.565 | <0.001 |
| 2. Actions | 1.765 | 0.426 | 0.264 | 4.140 | <0.001 |
| 3. Defusion | 0.772 | 0.353 | 0.188 | 2.183 | 0.031 |
| IV: General Health | |||||
| 1. Self | 1.121 | 0.341 | 0.312 | 3.289 | 0.001 |
| 2. Actions | 1.606 | 0.395 | 0.293 | 4.068 | <0.001 |
| 3. Defusion | 0.901 | 0.327 | 0.268 | 2.753 | 0.007 |
| IV: Thought supression | |||||
| 1. Self | 2.392 | 0.559 | 0.414 | 4.276 | <0.001 |
| 2. Acceptance | 2.039 | 0.615 | 0.321 | 3.315 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lobato, D.; Montesinos, F.; Flujas-Contreras, J.M. Psychological Flexibility Is Associated with Parental Stress in Relatives of People with Intellectual Disabilities. Int. J. Environ. Res. Public Health 2022, 19, 6118. https://doi.org/10.3390/ijerph19106118
Lobato D, Montesinos F, Flujas-Contreras JM. Psychological Flexibility Is Associated with Parental Stress in Relatives of People with Intellectual Disabilities. International Journal of Environmental Research and Public Health. 2022; 19(10):6118. https://doi.org/10.3390/ijerph19106118
Chicago/Turabian StyleLobato, David, Francisco Montesinos, and Juan M. Flujas-Contreras. 2022. "Psychological Flexibility Is Associated with Parental Stress in Relatives of People with Intellectual Disabilities" International Journal of Environmental Research and Public Health 19, no. 10: 6118. https://doi.org/10.3390/ijerph19106118
APA StyleLobato, D., Montesinos, F., & Flujas-Contreras, J. M. (2022). Psychological Flexibility Is Associated with Parental Stress in Relatives of People with Intellectual Disabilities. International Journal of Environmental Research and Public Health, 19(10), 6118. https://doi.org/10.3390/ijerph19106118