
Efficacy and Safety of Extracorporeal Membrane Oxygenation in Patients under Mechanical Ventilation with COVID-19 and Severe Acute Respiratory Distress Syndrome: A Health Technology Assessment

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Question (PICO)
2.2. Search of Evidence
2.3. Selection Criteria
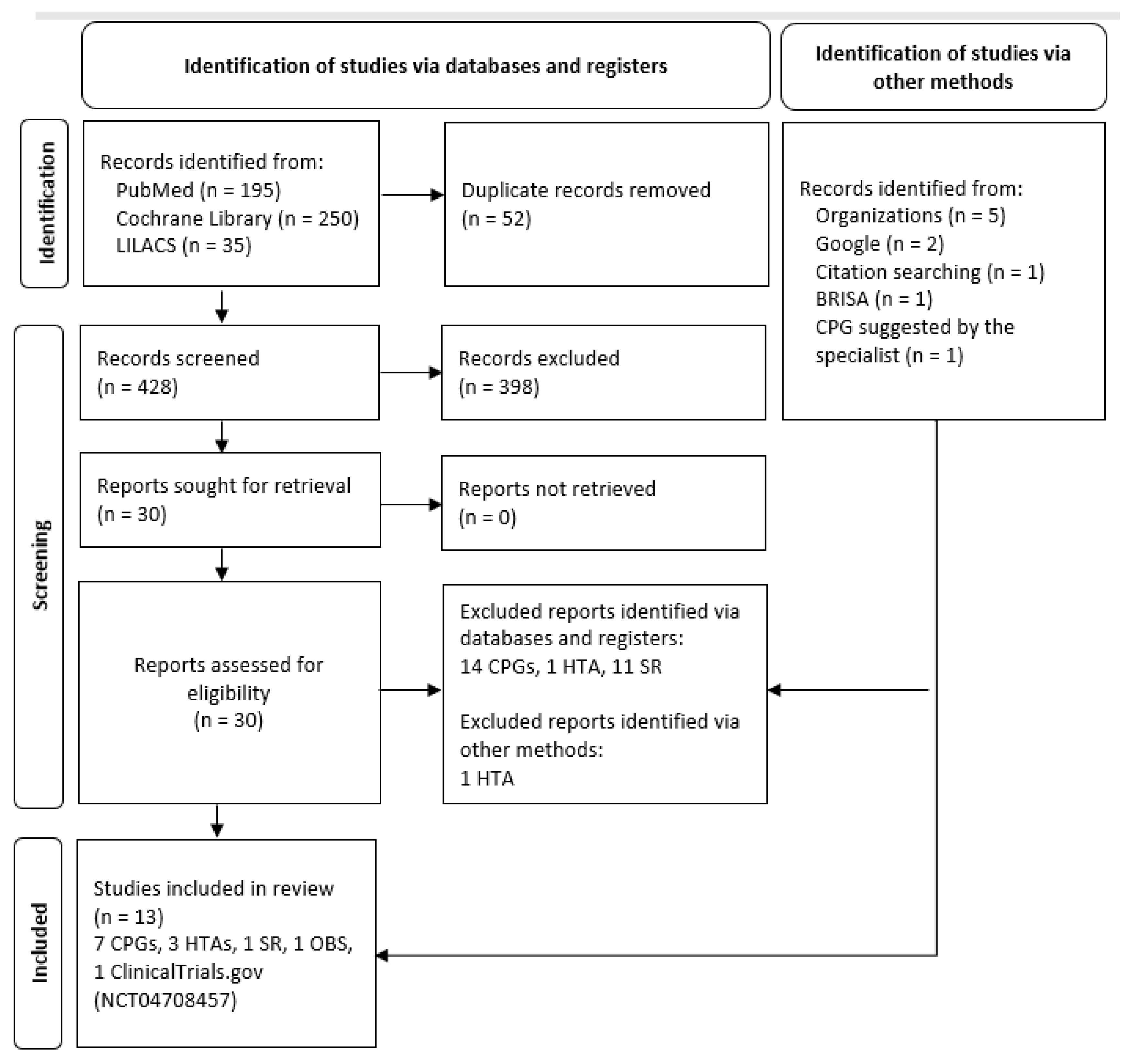
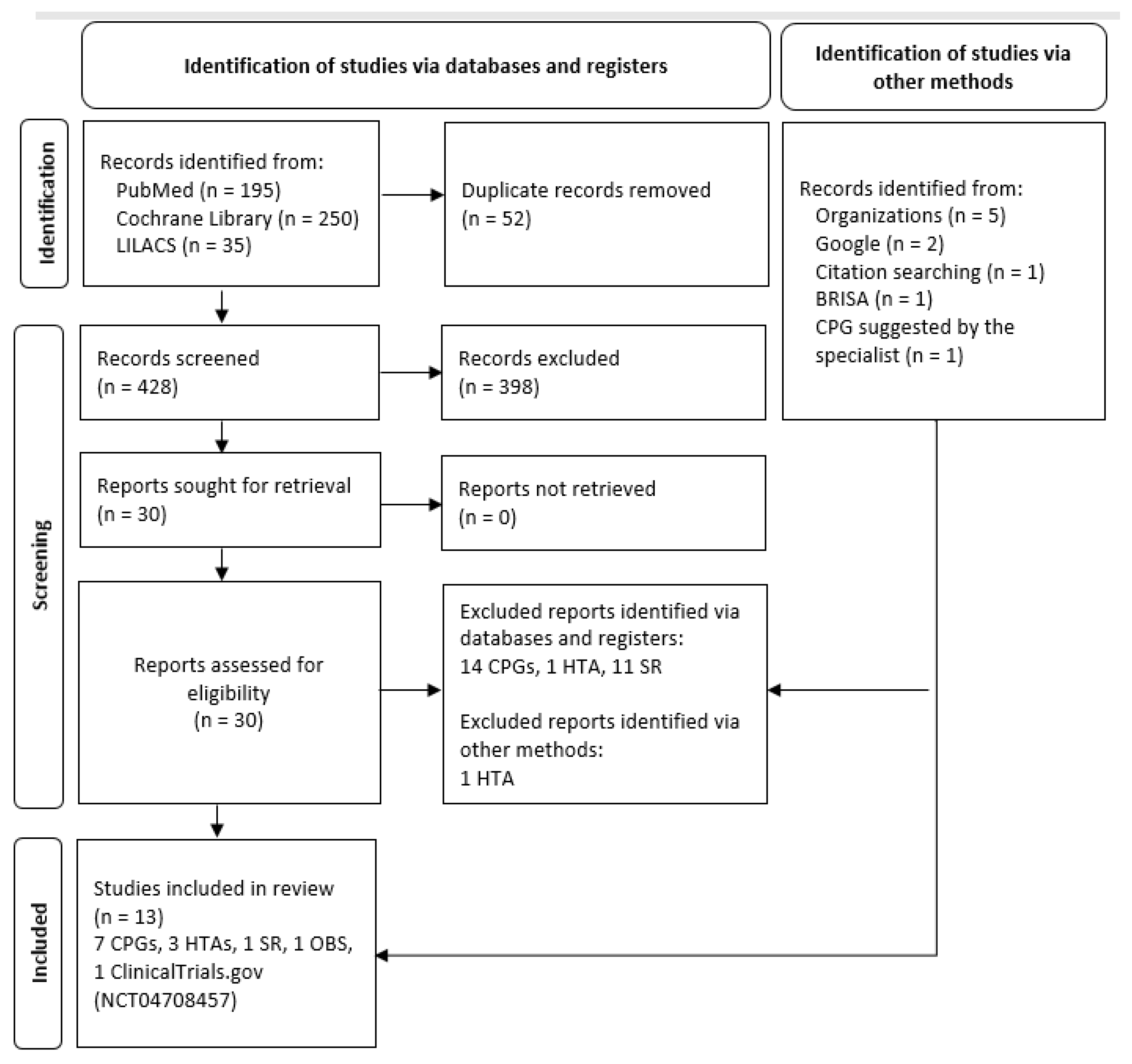
2.4. Selection Process
3. Evidence Description and Critical Appraisal
3.1. Clinical Practice Guidelines
3.1.1. “Living Guidance for Clinical Management of COVID-19: Living Guidance, 23 November 2021”
EOLIA Trial
Bayesian Post-Hoc Analysis of the EOLIA Trial
Case Series of Critically Ill Patients with MERS
Final Comments for This Clinical Practice Guideline
3.1.2. “Guidelines for Care of Critically Ill Adult Patients with COVID-19 in the Americas. Version 3”
3.1.3. “COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines”
3.1.4. “Extracorporeal Membrane Oxygenation for COVID-19: Updated 2021 Guidelines from the Extracorporeal Life Support Organization”
3.1.5. “Surviving Sepsis Campaign Guidelines on the Management of Adults with Coronavirus Disease 2019 (COVID-19) in the ICU: First Update”
CESAR Trial
Final Comments for This Clinical Practice Guideline
3.1.6. “Australian Guidelines for the Clinical Care of People with COVID-19, v51”
3.1.7. “Chemoprophylaxis, Diagnosis, Treatments, and Discharge Management of COVID-19: An Evidence-Based Clinical Practice Guideline (Updated Version)”
3.2. Health Technology Assessments
3.2.1. “Oxigenação por Membrana Extracorpórea (ECMO) Para Tratamento de Pacientes com COVID-19”
3.2.2. “Membrana de Oxigenación Extracorpórea en Infección por COVID-19. Documentos de Evaluación de Tecnologías Sanitarias, Informe de Respuesta Rápida N° 783”
3.2.3. “Extracorporeal Membrane Oxygenation (ECMO) for COVID-19 Patients with ARDS”
3.3. Systematic Reviews
“Extracorporeal Membrane Oxygenation (ECMO) in Patients with Severe COVID-19 Adult Respiratory Distress Syndrome: A Systematic Review and Meta-Analysis”
3.4. Observational Studies
3.5. Randomized Ongoing or Unpublished Clinical Trials
The REDEEM Pilot Study: A Feasibility RCT of Early ECMO in Severe Acute Respiratory Infection, including COVID-19, WHO (REDEEM) (NCT04708457)
4. Discussion
4.1. Main Findings
4.2. About the Clinical Practice Guidelines
4.3. About Health Technology Assessments
4.4. About the Systematic Review and the Observational Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2022. Available online: https://covid19.who.int/ (accessed on 31 March 2022).
- Ministerio de Salud. Sala Situacional COVID-19 Perú [Internet]. 2022. Available online: https://covid19.minsa.gob.pe/sala_situacional.asp (accessed on 30 March 2022).
- Abate, S.M.; Checkol, Y.A.; Mantefardo, B. Global prevalence and determinants of mortality among patients with COVID-19: A systematic review and meta-analysis. Ann. Med. Surg. 2021, 64, 102204. [Google Scholar] [CrossRef] [PubMed]
- Noor, F.M.; Islam, M.M. Prevalence and Associated Risk Factors of Mortality Among COVID-19 Patients: A Meta-Analysis. J. Community Health 2020, 45, 1270–1282. [Google Scholar] [CrossRef] [PubMed]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Khamis, F.; Memish, Z.; Bahrani, M.A.; Dowaiki, S.A.; Pandak, N.; Bolushi, Z.A.; AlSalmi, I.; Al-Zakwanie, I. Prevalence and predictors of in-hospital mortality of patients hospitalized with COVID-19 infection. J. Infect. Public Health 2021, 14, 759–765. [Google Scholar] [CrossRef]
- Tzotzos, S.J.; Fischer, B.; Fischer, H.; Zeitlinger, M. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: A global literature survey. Crit. Care 2020, 24, 516. [Google Scholar] [CrossRef] [PubMed]
- Hendrickson, K.W.; Peltan, I.D.; Brown, S.M. The Epidemiology of Acute Respiratory Distress Syndrome Before and After Coronavirus Disease 2019. Crit. Care Clin. 2021, 37, 703–716. [Google Scholar] [CrossRef]
- Sasidharan, S.; Singh, V.; Singh, J.; Madan, G.S.; Dhillon, H.S.; Dash, P.K.; Shibu, B.; Dhillon, G.K. COVID-19 ARDS: A Multispecialty Assessment of Challenges in Care, Review of Research, and Recommendations. J. Anaesthesiol. Clin. Pharmacol. 2021, 37, 179–195. [Google Scholar] [CrossRef] [PubMed]
- Gattinoni, L.; Gattarello, S.; Steinberg, I.; Busana, M.; Palermo, P.; Lazzari, S.; Romitti, F.; Quintel, M.; Meissner, K.; Marini, G.G.; et al. COVID-19 pneumonia: Pathophysiology and management. Eur. Respir. Rev. 2021, 30, 210138. [Google Scholar] [CrossRef]
- Kondili, E.; Makris, D.; Georgopoulos, D.; Rovina, N.; Kotanidou, A.; Koutsoukou, A. COVID-19 ARDS: Points to Be Considered in Mechanical Ventilation and Weaning. J. Pers. Med. 2021, 11, 1109. [Google Scholar] [CrossRef]
- Mega, C.; Cavalli, I.; Ranieri, V.M.; Tonetti, T. Protective ventilation in patients with acute respiratory distress syndrome related to COVID-19: Always, sometimes or never? Curr. Opin. Crit. Care 2022, 28, 51–56. [Google Scholar] [CrossRef]
- Badulak, J.; Antonini, M.V.; Stead, C.M.; Shekerdemian, L.; Raman, L.; Paden, M.L.; Agerstrand, C.; Bartlett, R.H.; Barrett, N.; Combes, A.; et al. Extracorporeal Membrane Oxygenation for COVID-19: Updated 2021 Guidelines from the Extracorporeal Life Support Organization. ASAIO 2021, 67, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Lippi, G. Poor survival with extracorporeal membrane oxygenation in acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19): Pooled analysis of early reports. J. Crit. Care 2020, 58, 27–28. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Pham, T.T. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- Zeng, Y.; Cai, Z.; Xianyu, Y.; Yang, B.X.; Song, T.; Yan, Q. Prognosis when using extracorporeal membrane oxygenation (ECMO) for critically ill COVID-19 patients in China: A retrospective case series. Crit. Care 2020, 24, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, A.K.; Alexander, P.J.; Joshi, D.J.; Tabachnick, D.R.; Cross, C.A.; Pappas, P.S.; Tatooles, A.J. Extracorporeal Membrane Oxygenation for Patients With COVID-19 in Severe Respiratory Failure. JAMA Surg. 2020, 155, 990–992. [Google Scholar] [CrossRef]
- Seeliger, B.; Doebler, M.; Hofmaenner, D.A.; Wendel-Garcia, P.D.; Schuepbach, R.A.; Schmidt, J.J.; Welte, T.M.D.; Tobias, M.D.; Hoeper, M.M.D.; Gillmann, H.M.D.; et al. Intracranial Hemorrhages on Extracorporeal Membrane Oxygenation: Differences Between COVID-19 and Other Viral Acute Respiratory Distress Syndrome. Crit. Care Med. 2022. [Google Scholar] [CrossRef]
- Raff, L.A.; Reid, T.D.; Johnson, D.; Raff, E.J.; Schneider, A.B.; Charles, A.G.; Gallaher, J.R. Comparative outcomes between COVID-19 and influenza patients placed on veno-venous extracorporeal membrane oxygenation for severe ARDS. Am. J. Surg. 2022, 223, 388–394. [Google Scholar] [CrossRef]
- World Health Organization. Living Guidance for Clinical Management of COVID-19: Living Guidance; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- World Health Organization. WHO Handbook for Guideline Development, 2nd ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Levy, M. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063. [Google Scholar] [CrossRef]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Alexandre, D.; Sylvain, L.; Christophe, G.; Da Silva, D.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Goligher, E.C.; Tomlinson, G.; Hajage, D.; Wijeysundera, D.; Fan, E.; Jüni, P.; Brodie, D.; Slutsky, A.S.; Combes, A. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome and Posterior Probability of Mortality Benefit in a Post Hoc Bayesian Analysis of a Randomized Clinical Trial. JAMA 2018, 320, 2251–2259. [Google Scholar] [CrossRef]
- Arabi, Y.M.; Arifi, A.A.; Balkhy, H.H.; Najm, H.; Aldawood, A.S.; Ghabashi, A.; Hawa, H.; Alothman, A.; Khaldi, A.; Al Raiy, B. Clinical course and outcomes of critically ill patients with Middle East respiratory syndrome coronavirus infection. Ann. Intern. Med. 2014, 160, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Montori, V.; Permanyer-Miralda, G.; Ferreira-González, I.; Busse, J.; Pacheco-Huergo, V.; Bryant, D.; Alonso, J.; A Akl, E.; Domingo-Salvany, A.; Mills, E.; et al. Validity of composite end points in clinical trials. BMJ 2005, 330, 594–596. [Google Scholar] [CrossRef] [Green Version]
- Organización Panamericana de la Salud. Guía Para el Cuidado de Pacientes Adultos Críticos con COVID-19 en las Américas; Versión 3; Organización Panamericana de la Salud: Washington, DC, USA, 2021. [Google Scholar]
- Organización Panamericana de la Salud. Directriz para el Fortalecimiento de los Programas Nacionales de GUÍAS Informadas por la Evidencia. Una Herramienta para la Adaptación e Implementación de Guías en las Américas; Organización Panamericana de la Salud: Washington, DC, USA, 2018. [Google Scholar]
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines; National Institutes of Health: Bethesda, MD, USA, 2022.
- Alhazzani, W.; Evans, L.; Alshamsi, F.; Møller, M.H.; Ostermann, M.; Prescott, H.C.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; et al. Surviving Sepsis Campaign Guidelines on the Management of Adults With Coronavirus Disease 2019 (COVID-19) in the ICU: First Update. Crit. Care Med. 2021, 49, e219. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Crit. Care Med. 2020, 48, e440–e469. [Google Scholar] [CrossRef] [PubMed]
- Peek, G.L.; Mugford, M.; Tiruvoipati, R.; Wilson, A.; Allen, E.; Thalanany, M.M.; Hibbert, C.L.; Truesdale, A.; Clemens, F.; Cooper, N.; et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): A multicentre randomised controlled trial. Lancet 2009, 374, 1351–1363. [Google Scholar] [CrossRef]
- Montori, V.M.; Guyatt, G.H. Intention-to-treat principle. Can. Med. Assoc. J. 2001, 165, 1339–1341. [Google Scholar]
- Australian National COVID-19 Clinical Evidence Taskforce. Australian Guidelines for the Clinical Care of People with COVID-19; v51; Australian National COVID-19 Clinical Evidence Taskforce: Melbourne, Australia, 2022. [Google Scholar]
- National COVID-19 Clinical Evidence Taskforce. Methods for Living Guidelines for Management and Care of People in Primary, Hospital and Critical Care with Suspected or Confirmed COVID-19 Infection: Technical Report [Internet]. 2020. Available online: https://covid19evidence.net.au/wp-content/uploads/Technical-Report_20201022.pdf?=201022-72442 (accessed on 25 March 2022).
- National COVID-19 Clinical Evidence Taskforce. Search Methods Version 3, 1 July 2021 [Internet]. 2021. Available online: https://covid19evidence.net.au/wp-content/uploads/NC19CET-Search-Methods-V3.pdf (accessed on 25 March 2022).
- National Health and Medical Research Council. 2016 NHMRC Standards for Guidelines [Internet]. 2016. Available online: https://www.nhmrc.gov.au/guidelinesforguidelines/standards (accessed on 25 March 2022).
- Schmidt, M.; Hajage, D.; Lebreton, G.; Monsel, A.; Voiriot, G.; Levy, D.; Baron, E.; Beurton, A.; Chommeloux, J.; Meng, P.; et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome associated with COVID-19: A retrospective cohort study. Lancet Respir. Med. 2020, 8, 1121–1131. [Google Scholar] [CrossRef]
- Hasan, S.S.; Capstick, T.; Ahmed, R.; Kow, C.S.; Mazhar, F.; Merchant, H.A.; Zaidi, S.T.R. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: A systematic review and meta-analysis. Expert Rev. Respir. Med. 2020, 14, 1149–1163. [Google Scholar] [CrossRef]
- Jin, Y.-H.; Zhan, Q.-Y.; Peng, Z.-Y.; Ren, X.-Q.; Yin, X.-T.; Cai, L.; Yuan, Y.-F.; Yue, J.-R.; Zhang, X.-C.; Yang, Q.-W.; et al. Chemoprophylaxis, diagnosis, treatments, and discharge management of COVID-19: An evidence-based clinical practice guideline (updated version). Mil. Med. Res. 2020, 7, 41. [Google Scholar] [CrossRef]
- Ministério Da Saúde. Oxigenação por Membrana Extracorpórea (ECMO) Para Tratamento de Pacientes com COVID-19; Ministério Da Saúde: Brasília, Brazil, 2020.
- Instituto de Efectividad Clínica y Sanitaria. Membrana de Oxigenación Extracorpórea en Infección por COVID-19. Documentos de Evaluación de Tecnologías Sanitarias; Informe de Respuesta Rápida: Buenos Aires, Argentina, 2020. [Google Scholar]
- Health Technology Assessment Unit; DOH. Extracorporeal Membrane Oxygenation (ECMO) for COVID-19 Patients with ARDS; DOH: Abu Dhabi, United Arab Emirates, 2020.
- Aretha, D.; Fligou, F.; Kiekkas, P.; Karamouzos, V.; Voyagis, G. Extracorporeal Life Support: The Next Step in Moderate to Severe ARDS-A Review and Meta-Analysis of the Literature. BioMed Res. Int. 2019, 2019, 1035730. [Google Scholar] [CrossRef]
- Haiduc, A.A.; Alom, S.; Melamed, N.; Harky, A. Role of extracorporeal membrane oxygenation in COVID-19: A systematic review. J. Card. Surg. 2020, 35, 2679–2687. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, H.H.; Hassaballa, A.S.; Ahmed, T.A.; Gumaa, M.; Sharkawy, H.Y. Extracorporeal membrane oxygenation (ECMO) in patients with severe COVID-19 adult respiratory distress syndrome: A systematic review and meta-analysis. Cardiothorac. Surg. 2021, 29, 9. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Yin, P.-F.; Li, A.; Shen, M.R.; Yao, Y.-X. Acute Respiratory Distress Syndrome Treated With Awake Extracorporeal Membrane Oxygenation in a Patient With COVID-19 Pneumonia. J. Cardiothorac. Vasc. Anesthesia 2021, 35, 2467–2470. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Cai, S.; Luo, Y.; Zhu, F.; Hu, M.; Zhao, Y.; Zheng, R.; Li, X.; Hu, B.; Peng, Z. Extracorporeal Membrane Oxygenation for Coronavirus Disease 2019-Induced Acute Respiratory Distress Syndrome: A Multicenter Descriptive Study*. Crit. Care Med. 2020, 48, 1289–1295. [Google Scholar] [CrossRef]
- Luo, X.; Liu, Y.; Ren, M.; Zhang, X.; Janne, E.; Lv, M.; Wang, Q.; Song, Y.; Mathew, J.L.; Ahn, H.S.; et al. Consistency of recommendations and methodological quality of guidelines for the diagnosis and treatment of COVID-19. J. Evid.-Based Med. 2021, 14, 40–55. [Google Scholar] [CrossRef]
- Mazzeffi, M.; Greenwood, J.; Tanaka, K.; Menaker, J.; Rector, R.; Herr, D.; Kon, Z.; Lee, J.; Griffith, B.; Rajagopal, K.; et al. Bleeding, Transfusion, and Mortality on Extracorporeal Life Support: ECLS Working Group on Thrombosis and Hemostasis. Ann. Thorac. Surg. 2016, 101, 682–689. [Google Scholar] [CrossRef] [Green Version]
- Sklar, M.C.; Sy, E.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation Practices during Venovenous Extracorporeal Membrane Oxygenation for Respiratory Failure. A Systematic Review. Ann. Am. Thorac. Soc. 2016, 13, 2242–2250. [Google Scholar] [CrossRef]
- Olson, S.R.; Murphree, C.R.; Zonies, D.; Meyer, A.D.; Mccarty, O.J.T.; Deloughery, T.G.; Shatzel, J.J. Thrombosis and Bleeding in Extracorporeal Membrane Oxygenation (ECMO) Without Anticoagulation: A Systematic Review. ASAIO J. 2020, 67, 290–296. [Google Scholar] [CrossRef]
- Hartley, E.L.; Singh, N.; Barrett, N.; Wyncoll, D.; Retter, A. Screening pulmonary angiogram and the effect on anticoagulation strategies in severe respiratory failure patients on venovenous extracorporeal membrane oxygenation. J. Thromb. Haemost. 2019, 18, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parzy, G.; Daviet, F.; Persico, N.; Rambaud, R.; Scemama, U.; Adda, M.; Guervilly, C.; Hraiech, S.; Chaumoitre, K.; Roch, A.; et al. Prevalence and Risk Factors for Thrombotic Complications Following Venovenous Extracorporeal Membrane Oxygenation. Crit. Care Med. 2020, 48, 192–199. [Google Scholar] [CrossRef]
- Chapman, J.T.; Breeding, J.; Kerr, S.J.; Bajic, M.; Nair, P.; Buscher, H. CNS Complications in Adult Patients Treated With Extracorporeal Membrane Oxygenation. Crit. Care Med. 2020, 49, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Nasr, D.M.; A Rabinstein, A. Neurologic Complications of Extracorporeal Membrane Oxygenation. J. Clin. Neurol. 2015, 11, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bemtgen, X.; Zotzmann, V.; Benk, C.; Rilinger, J.; Steiner, K.; Asmussen, A.; Bode, C.; Wengenmayer, T.; Maier, S.; Staudacher, D.L. Thrombotic circuit complications during venovenous extracorporeal membrane oxygenation in COVID-19. J. Thromb. Thrombolysis 2020, 51, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Arachchillage, D.J.; Rajakaruna, I.; Scott, I.; Gaspar, M.; Odho, Z.; Banya, W.; Vlachou, A.; Isgro, G.; Cagova, L.; Wade, J.; et al. Impact of major bleeding and thrombosis on 180-day survival in patients with severe COVID-19 supported with veno-venous extracorporeal membrane oxygenation in the United Kingdom: A multicentre observational study. Br. J. Haematol. 2021, 196, 566–576. [Google Scholar] [CrossRef] [PubMed]
- Kannapadi, N.V.; Jami, M.; Premraj, L.; Etchill, E.W.; Giuliano, K.; Bush, E.L.; Kim, B.S.; Seal, S.; Whitman, G.; Cho, S.-M. Neurological Complications in COVID-19 Patients With ECMO Support: A Systematic Review and Meta-Analysis. Heart Lung Circ. 2021, 31, 292–298. [Google Scholar] [CrossRef]
- Masur, J.; Freeman, C.; Mohan, S. A Double-Edged Sword: Neurologic Complications and Mortality in Extracorporeal Membrane Oxygenation Therapy for COVID-19–Related Severe Acute Respiratory Distress Syndrome at a Tertiary Care Center. Am. J. Neuroradiol. 2020, 41, 2009–2011. [Google Scholar] [CrossRef]

{kind=link}
| Population | Patients under mechanical ventilation, with confirmed COVID-19 * and severe acute respiratory distress syndrome ** |
| Intervention | Extracorporeal Membrane Oxygenation |
| Control | Mechanical ventilation |
| Outcome | Efficacy: Mortality, Length of stay (in hospital or ICU), Quality of lifeSafety: Adverse events related to the procedure, Adverse events related to the device |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toro-Huamanchumo, C.J.; Castro-Reyes, M.M.; Peralta, V.; Venancio-Huerta, J.E.; Puescas-Sanchez, P.R.; Peña-Sanchez, E.R. Efficacy and Safety of Extracorporeal Membrane Oxygenation in Patients under Mechanical Ventilation with COVID-19 and Severe Acute Respiratory Distress Syndrome: A Health Technology Assessment. Int. J. Environ. Res. Public Health 2022, 19, 6080. https://doi.org/10.3390/ijerph19106080
Toro-Huamanchumo CJ, Castro-Reyes MM, Peralta V, Venancio-Huerta JE, Puescas-Sanchez PR, Peña-Sanchez ER. Efficacy and Safety of Extracorporeal Membrane Oxygenation in Patients under Mechanical Ventilation with COVID-19 and Severe Acute Respiratory Distress Syndrome: A Health Technology Assessment. International Journal of Environmental Research and Public Health. 2022; 19(10):6080. https://doi.org/10.3390/ijerph19106080
Chicago/Turabian StyleToro-Huamanchumo, Carlos J., Maribel M. Castro-Reyes, Verónica Peralta, Julissa E. Venancio-Huerta, Pablo R. Puescas-Sanchez, and Eric R. Peña-Sanchez. 2022. "Efficacy and Safety of Extracorporeal Membrane Oxygenation in Patients under Mechanical Ventilation with COVID-19 and Severe Acute Respiratory Distress Syndrome: A Health Technology Assessment" International Journal of Environmental Research and Public Health 19, no. 10: 6080. https://doi.org/10.3390/ijerph19106080
APA StyleToro-Huamanchumo, C. J., Castro-Reyes, M. M., Peralta, V., Venancio-Huerta, J. E., Puescas-Sanchez, P. R., & Peña-Sanchez, E. R. (2022). Efficacy and Safety of Extracorporeal Membrane Oxygenation in Patients under Mechanical Ventilation with COVID-19 and Severe Acute Respiratory Distress Syndrome: A Health Technology Assessment. International Journal of Environmental Research and Public Health, 19(10), 6080. https://doi.org/10.3390/ijerph19106080