
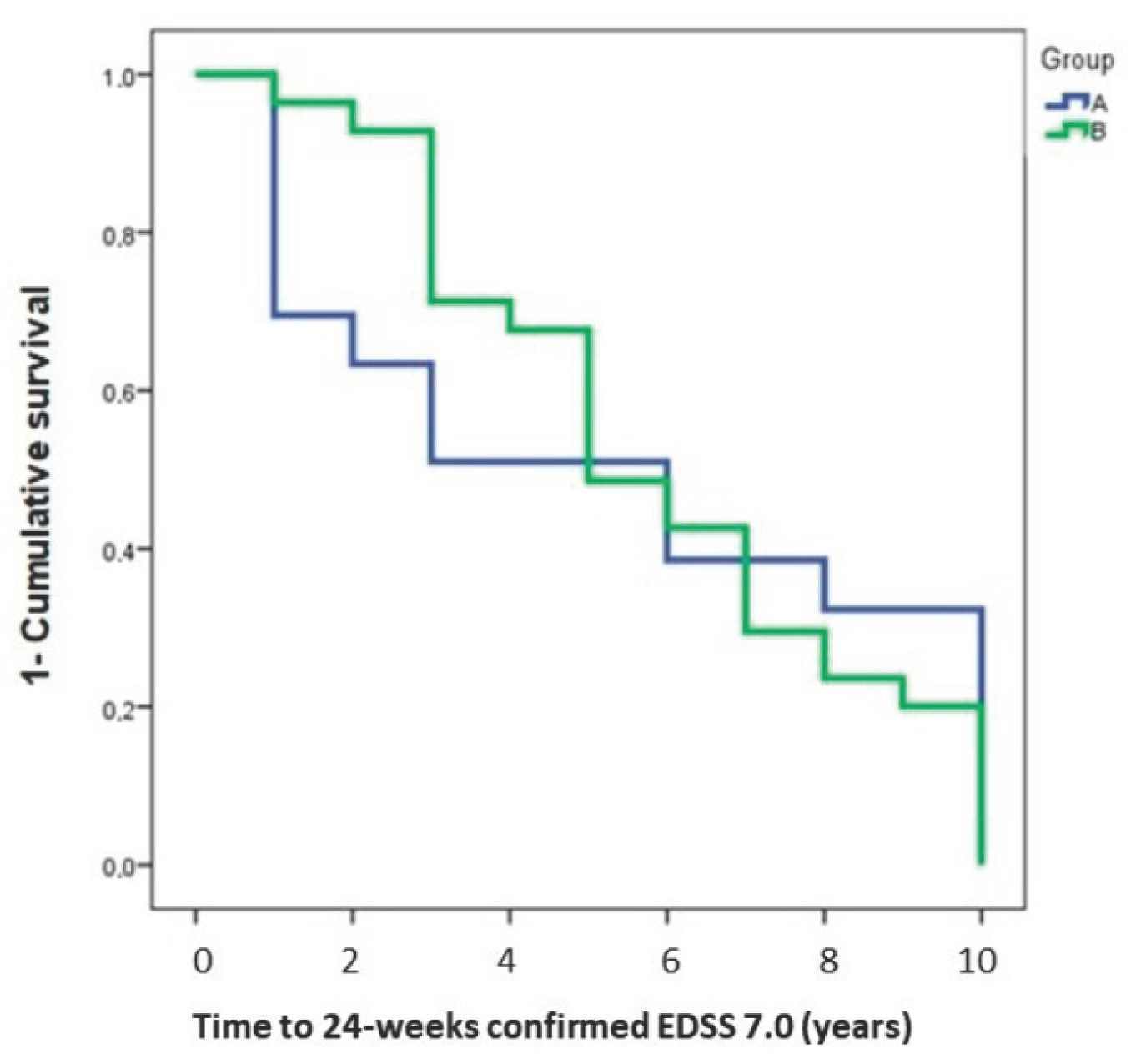
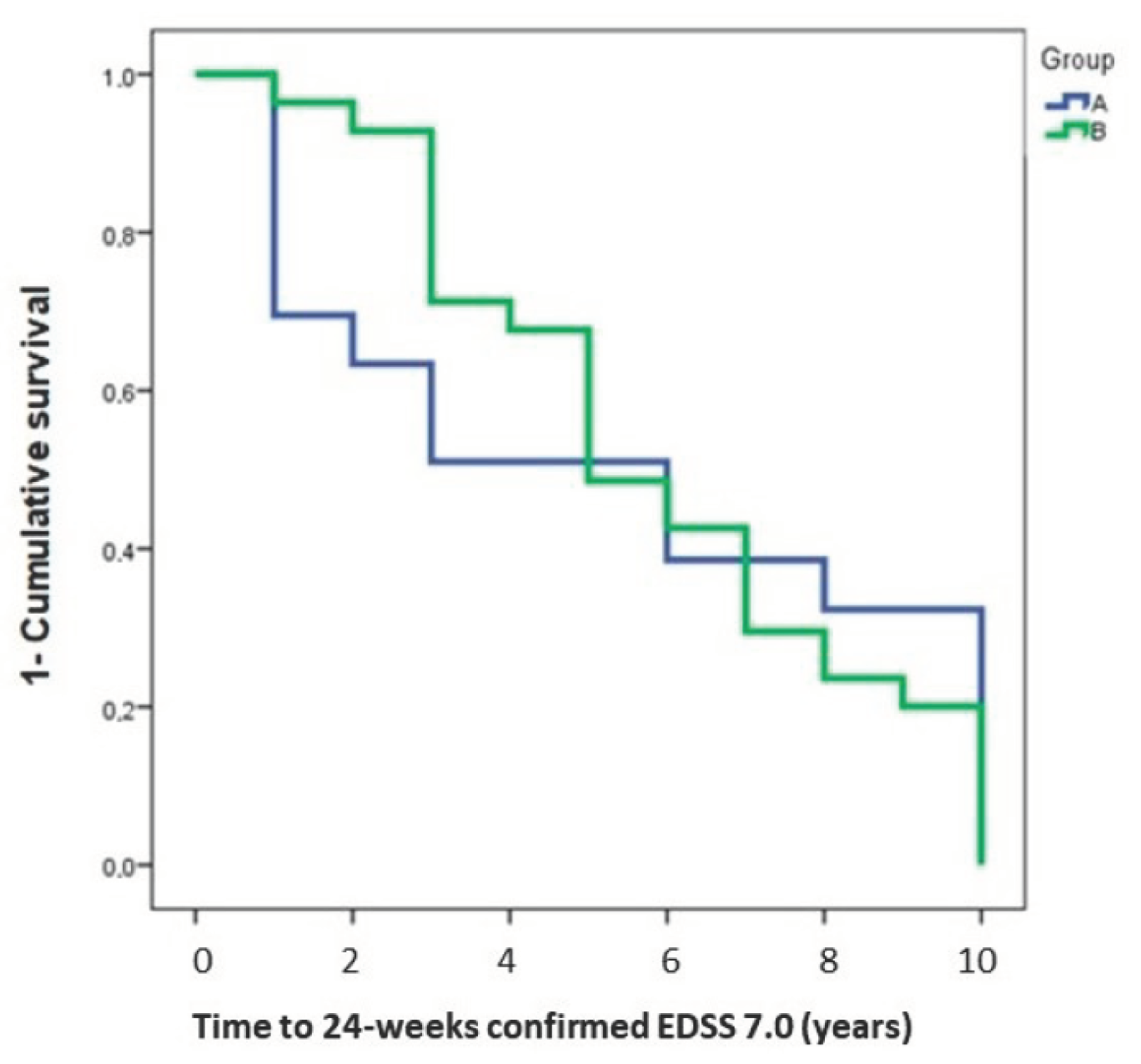
Stopping Interferon Beta 1b Does Not Influence the Risk of Disability Accrual in Non-Active SPMS: Results from an Italian Real-World Study


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Protocol Approval Standard, Registrations, and Patient Consents
2.3. Data Dollection
2.4. Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Patti, F.; Zanghì, A.; Chisari, C.G.; Lo Fermo, S.; Zappia, M. Late-onset and young-onset relapsing-remitting multiple sclerosis: Evidence from a retrospective long-term follow-up study. Eur. J. Neurol. 2018, 25, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Mahad, D.H.; Trapp, B.D.; Lassmann, H. Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol. 2015, 14, 183–193. [Google Scholar] [CrossRef]
- D’Amico, E.; Zanghì, A.; Parrinello, N.L.; Romano, A.; Palumbo, G.A.; Chisari, C.G.; Toscano, S.; di Raimondo, F.; Zappia, M.; Patti, F. Immunological subsets characterization in newly diagnosed relapsing-remitting multiple sclerosis. Front. Immunol. 2022, 13, 819136. [Google Scholar] [CrossRef] [PubMed]
- Solaro, C.; Cella, M.; Signori, A.; Martinelli, V.; Radaelli, M.; Centonze, D.; Sica, F.; Grasso, M.G.; Clemenzi, A.; Bonavita, S.; et al. Identifying neuropathic pain in patients with multiple sclerosis: A cross-sectional multicenter study using highly specific criteria. J. Neurol. 2018, 265, 828–835. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Patti, F.; Zanghì, A.; Zappia, M. A Personalized approach in progressive multiple sclerosis: The current status of disease modifying therapies (DMTs) and future perspectives. Int. J. Mol. Sci. 2016, 17, 1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Amico, E.; Zanghì, A.; Gastaldi, M.; Patti, F.; Zappia, M.; Franciotta, D. Placing CD20-targeted B cell depletion in multiple sclerosis therapeutic scenario: Present and future perspectives. Autoimmun. Rev. 2019, 18, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.; Forte, M.L.; Schwehr, N.; Carpenter, A.; Kane, R.L. Decisional Dilemmas in Discontinuing Prolonged Disease—Modifying Treatment for Multiple Sclerosis; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015.
- D’Amico, E.; Ziemssen, T.; Cottone, S. To stop or not to stop disease modifying therapies in secondary progressive multiple sclerosis, that is the question. Expert Rev. Neurother. 2017, 17, 847–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Mantia, L.; Vacchi, L.; Di Pietrantonj, C.; Ebers, G.; Rovaris, M.; Fredrikson, S.; Filippini, G. Interferon beta for secondary progressive multiple sclerosis. Cochrane Database Syst. Rev. 2012, 1, cd005181. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, G. Stopping disease—Modifying therapy in nonrelapsing multiple sclerosis: Experience from a clinical practice. Int. J. MS Care 2017, 19, 11–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lizak, N.; Malpas, C.B.; Sharmin, S.; Havrdova, E.K.; Horakova, D.; Izquierdo, G.; Eichau, S.; Lugaresi, A.; Duquette, P.; Girard, M.; et al. Association of sustained immunotherapy with disability outcomes in patients with active secondary progressive multiple sclerosis. JAMA Neurol. 2020, 77, 1398–1407. [Google Scholar] [CrossRef] [PubMed]
- Lorscheider, J.; Buzzard, K.; Jokubaitis, V.; Spelman, T.; Havrdova, E.; Horakova, D.; Trojano, M.; Izquierdo, G.; Girard, M.; Duquette, P.; et al. Defining secondary progressive multiple sclerosis. Brain A J. Neurol. 2016, 139, 2395–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworkin, J.D.; Linn, K.A.; Oguz, I.; Fleishman, G.M.; Bakshi, R.; Nair, G.; Calabresi, P.A.; Henry, R.G.; Oh, J.; Papinutto, N.; et al. An automated statistical technique for counting distinct multiple sclerosis lesions. Am. J. Neuroradiol. 2018, 39, 626–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorscheider, J.; Jokubaitis, V.G.; Spelman, T.; Izquierdo, G.; Lugaresi, A.; Havrdova, E.; Horakova, D.; Trojano, M.; Duquette, P.; Girard, M.; et al. Anti-inflammatory disease-modifying treatment and short-term disability progression in SPMS. Neurology 2017, 89, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Rae-Grant, A.; Day, G.S.; Marrie, R.A.; Rabinstein, A.; Cree, B.A.C.; Gronseth, G.S.; Haboubi, M.; Halper, J.; Hosey, J.P.; Jones, D.E.; et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the guideline development, dissemination, and implementation subcommittee of the American academy of neurology. Neurology 2018, 90, 777–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inojosa, H.; Proschmann, U.; Akgün, K.; Ziemssen, T. The need for a strategic therapeutic approach: Multiple sclerosis in check. Ther. Adv. Chronic Dis. 2022, 13, 20406223211063032. [Google Scholar] [CrossRef] [PubMed]
- Solari, A.; Giovannetti, A.M.; Giordano, A.; Tortorella, C.; Torri Clerici, V.; Brichetto, G.; Granella, F.; Lugaresi, A.; Patti, F.; Salvetti, M.; et al. Conversion to secondary progressive multiple sclerosis: Patient awareness and needs. Results from an online survey in Italy and Germany. Front. Neurol. 2019, 10, 916. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Factors * | Group A (165) | Group B (146) | p-Value |
|---|---|---|---|
| Male n (%) | 88 (53.3%) | 80 (54.8%) | ns |
| Female n (%) | 77 (46.7%) | 66 (45.2%) | ns |
| Age (years) | 57.3 ± 9.5 | 55.8 ± 10.9 | ns |
| Level of education | |||
| Primary level (≤10 years) | 30 (18.2%) | 25 (17.1%) | ns |
| Secondary level (11–13 years) | 92 (55.8%) | 85 (58.2%) | ns |
| Tertiary level (>13 years) | 43 (26%) | 36 (24.7%) | ns |
| N. of DMTs switch pre-progression | 0.3 ± 0.6 | 0.4 ± 0.7 | ns |
| Patients on interferon beta 1b at the time of SPMS conversion n (%) | 72 (43.6%) | 76 (52%) | ns |
| Patients on other DMTs n (%) | 93 (56.4%) | 70 (48%) | ns |
| Follow-up duration (months) | 79.3 ± 18.7 | 85.3 ± 23.5 | ns |
| EDSS at disease progression (median; min-max) | 4.5 (4.0–5.5) | 5.0 (4.5–5.5) | ns |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanghì, A.; D’Amico, E.; Patti, F.; Avolio, C. Stopping Interferon Beta 1b Does Not Influence the Risk of Disability Accrual in Non-Active SPMS: Results from an Italian Real-World Study. Int. J. Environ. Res. Public Health 2022, 19, 6069. https://doi.org/10.3390/ijerph19106069
Zanghì A, D’Amico E, Patti F, Avolio C. Stopping Interferon Beta 1b Does Not Influence the Risk of Disability Accrual in Non-Active SPMS: Results from an Italian Real-World Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6069. https://doi.org/10.3390/ijerph19106069
Chicago/Turabian StyleZanghì, Aurora, Emanuele D’Amico, Francesco Patti, and Carlo Avolio. 2022. "Stopping Interferon Beta 1b Does Not Influence the Risk of Disability Accrual in Non-Active SPMS: Results from an Italian Real-World Study" International Journal of Environmental Research and Public Health 19, no. 10: 6069. https://doi.org/10.3390/ijerph19106069
APA StyleZanghì, A., D’Amico, E., Patti, F., & Avolio, C. (2022). Stopping Interferon Beta 1b Does Not Influence the Risk of Disability Accrual in Non-Active SPMS: Results from an Italian Real-World Study. International Journal of Environmental Research and Public Health, 19(10), 6069. https://doi.org/10.3390/ijerph19106069