
Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
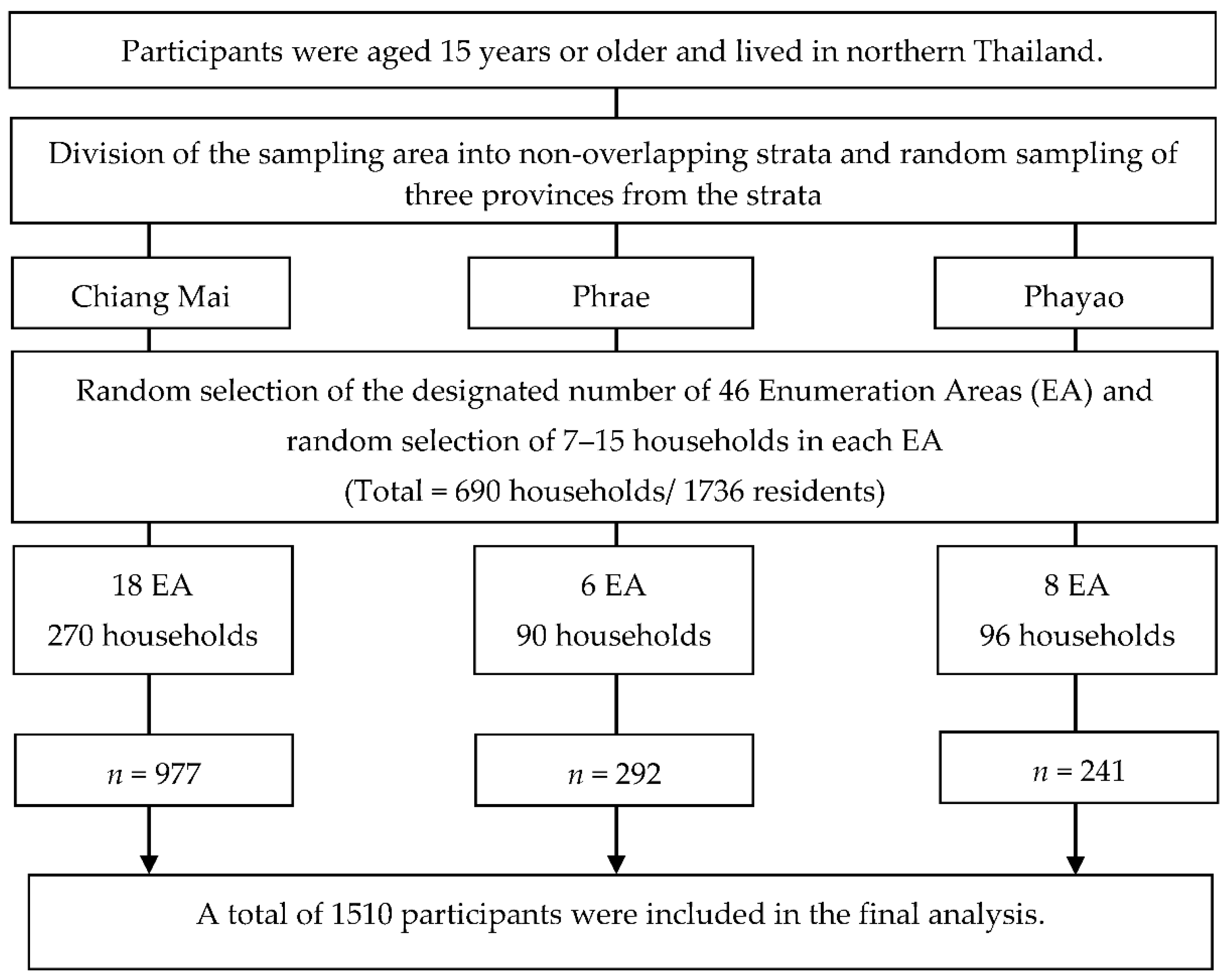
2.1. Study Design and Sampling Method
2.2. Participants and Data Collection Procedure
2.3. Variables and Measurement
2.3.1. Participant Characteristics, Socio-Demographics, and Health Information Sources
2.3.2. The Thai Version of the Health Literacy Questionnaire (THLQ)
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. The Study Participants’ Characteristics
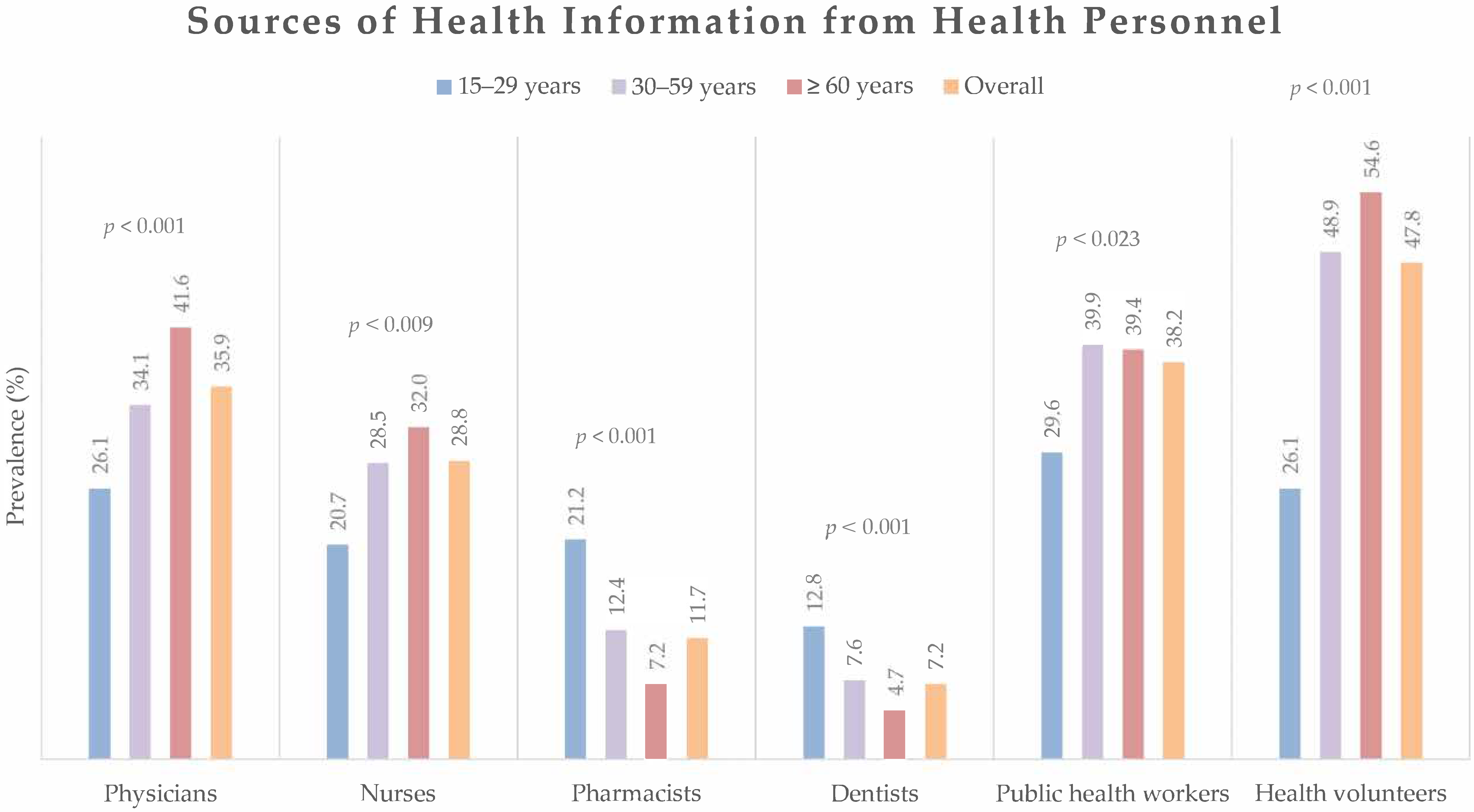
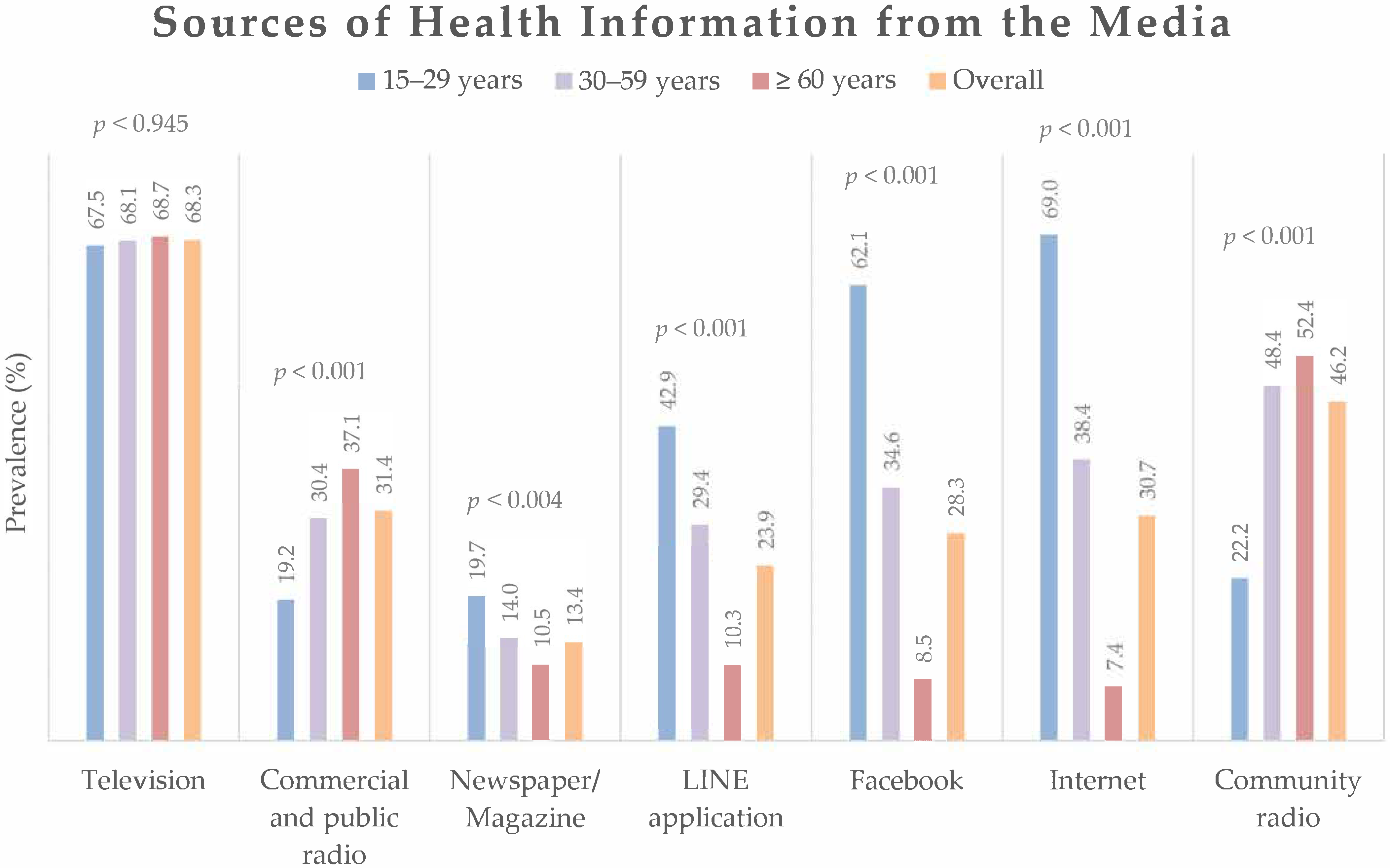
3.2. Sources of Health Information
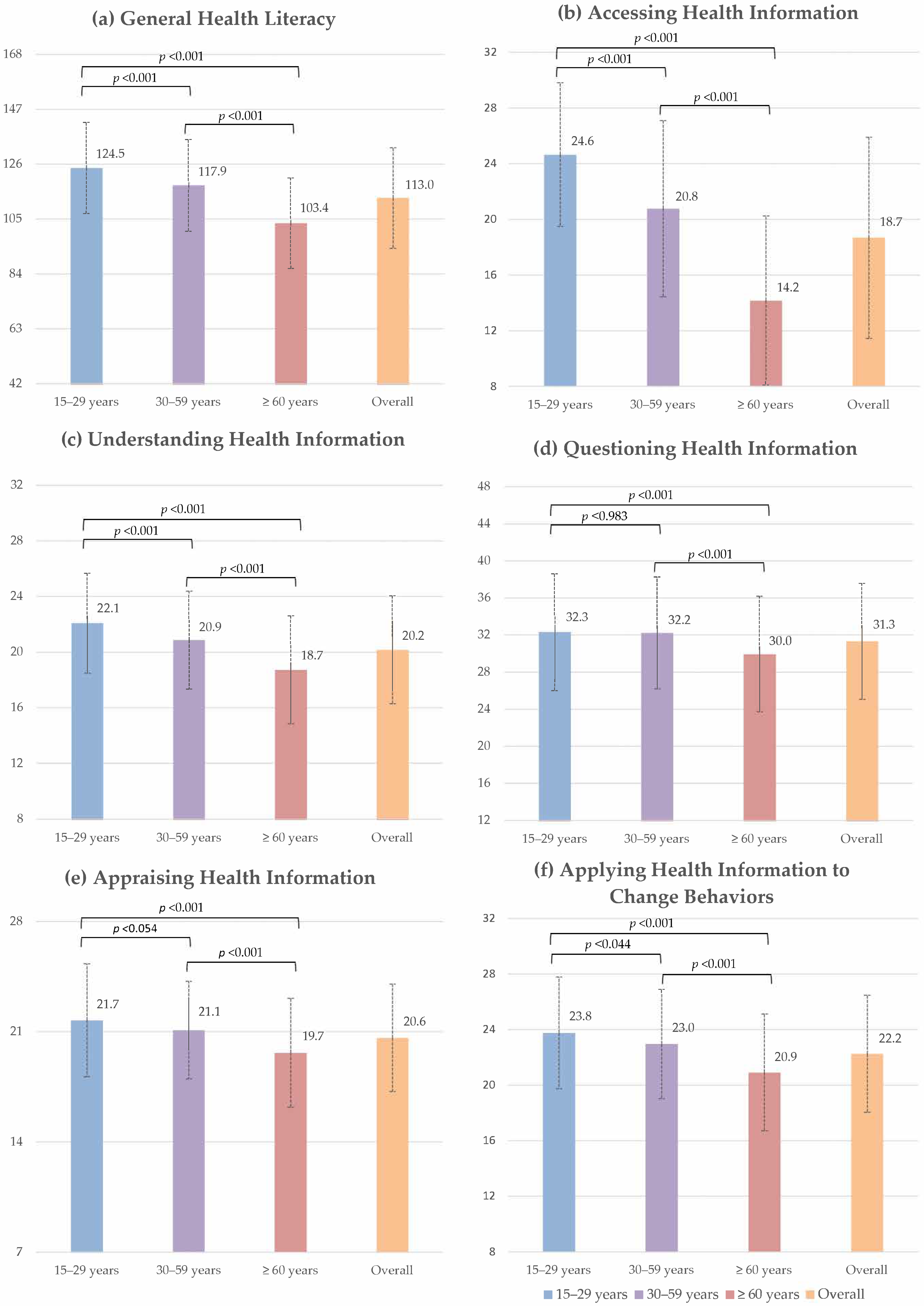
3.3. General and Subindices Health Literacy
3.4. Exploration of the Factors Associated with General Health Literacy
4. Discussion
4.1. Sociodemographic Factors Influencing Health Literacy
4.2. Sources of Health Information
4.3. Relationship between the Health Information Sources and Health Literacy
4.4. Health Literacy in COVID-19 Pandemic
4.5. Generalizability, Implications and Future Studies
4.6. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Health Promotion Glossary. Available online: https://www.who.int/publications/i/item/WHO-HPR-HEP-98.1 (accessed on 16 March 2022).
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Simonds, S.K. Health Education as Social Policy. Health Educ. 1974, 2, 1–10. [Google Scholar] [CrossRef]
- McDonald, M.; Shenkman, L. Health Literacy and Health Outcomes of Adults in the United States: Implications for Providers. Internet J. Allied Health Sci. Pract. 2018, 1, 4. [Google Scholar] [CrossRef]
- Baccolini, V.; Isonne, C.; Salerno, C.; Giffi, M.; Migliara, G.; Mazzalai, E.; Turatto, F.; Sinopoli, A.; Rosso, A.; De Vito, C.; et al. The association between adherence to cancer screening programs and health literacy: A systematic review and meta-analysis. Prev. Med. 2022, 155, 106927. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Coordination Mechanism on the Prevention and Control of Noncommunicable Diseases Using Health Literacy to Impact on NCDs in the SDG–Era; World Health Organization: Geneva, Switzerland, 2020; pp. 1–16. [Google Scholar]
- Olesen, K.; Reynheim, A.L.F.; Joensen, L.; Ridderstråle, M.; Kayser, L.; Maindal, H.T.; Osborne, R.H.; Skinner, T.; Willaing, I. Higher health literacy is associated with better glycemic control in adults with type 1 diabetes: A cohort study among 1399 Danes. BMJ Open Diab. Res. Care 2017, 5, e000437. [Google Scholar] [CrossRef]
- Bostock, S.; Steptoe, A.J.B. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef]
- Peterson, P.N.; Shetterly, S.M.; Clarke, C.L.; Bekelman, D.B.; Chan, P.S.; Allen, L.A.; Matlock, D.D.; Magid, D.J.; Masoudi, F.A. Health literacy and outcomes among patients with heart failure. JAMA 2011, 305, 1695–1701. [Google Scholar] [CrossRef]
- Haun, J.N.; Patel, N.R.; French, D.D.; Campbell, R.R.; Bradham, D.D.; Lapcevic, W.A. Association between health literacy and medical care costs in an integrated healthcare system: A regional population based study. BMC Health Serv. Res. 2015, 15, 249. [Google Scholar] [CrossRef]
- Maon, S.N.; Hassan, N.M.; Seman, S.A.A. Online Health Information Seeking Behavior Pattern. Adv. Sci. Lett. 2017, 23, 10582–10585. [Google Scholar] [CrossRef]
- Chu, J.T.; Wang, M.P.; Shen, C.; Viswanath, K.; Lam, T.H.; Chan, S.C.C. How, When and Why People Seek Health Information Online: Qualitative Study in Hong Kong. Interact. J. Med. Res. 2017, 6, 24. [Google Scholar] [CrossRef]
- Benigeri, M.; Pluye, P. Shortcomings of health information on the Internet. Health Promot. Int. 2003, 18, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Stormacq, C.; Wosinski, J.; Boillat, E.; Van den Broucke, S. Effects of health literacy interventions on health-related outcomes in socioeconomically disadvantaged adults living in the community: A systematic review. JBI Evid. Synth. 2020, 18, 1389–1469. [Google Scholar] [CrossRef] [PubMed]
- Javadzade, S.H.; Sharifirad, G.; Radjati, F.; Mostafavi, F.; Reisi, M.; Hasanzade, A. Relationship between health literacy, health status, and healthy behaviors among older adults in Isfahan, Iran. J. Edu. Health Promot. 2012, 1, 31. [Google Scholar] [CrossRef]
- Toçi, E.; Burazeri, G.; Kamberi, H.; Jerliu, N.; Sørensen, K.; Brand, H. Socio-economic correlates of functional health literacy among patients of primary health care in Kosovo. Public Health 2014, 128, 842–848. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, L.; Cai, Z.; Bao, L.; Ai, P.; Ai, Z. Prevalence and Risk Factors of Low Health Literacy: A Community-Based Study in Shanghai, China. Int. J. Environ. Res. Public Health 2017, 14, 628. [Google Scholar] [CrossRef]
- Jovic-Vranes, A.; Bjegovic-Mikanovic, V.; Marinkovic, J.; Kocev, N. Health literacy in a population of primary health-care patients in Belgrade, Serbia. Int. J. Public Health 2011, 56, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, K.; Pelikan, J.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef]
- Rajah, R.; Hassali, M.A.A.; Murugiah, M.K. A systematic review of the prevalence of limited health literacy in Southeast Asian countries. Public Health 2019, 167, 8–15. [Google Scholar] [CrossRef]
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults: Results From the 2003 National Assessment of Adult Literacy (NCES 2006–483); National Center for Education Statistics, Institute of Education Sciences: Washington, DC, USA, 2006.
- Nie, X.; Li, Y.; Li, L.; Huang, X. A study on health information literacy among urban and suburban residents in six provinces in China. Chin. J. Prev. Med. 2014, 48, 566–570. [Google Scholar]
- Hillyer, G.C.; Schmitt, K.M.; Lizardo, M.; Reyes, A.; Bazan, M.; Alvarez, M.C.; Sandoval, R.; Abdul, K.; Orjuela, M.A. Electronic Communication Channel Use and Health Information Source Preferences Among Latinos in Northern Manhattan. J. Community Health 2017, 42, 349–357. [Google Scholar] [CrossRef]
- Cutilli, C.C.; Simko, L.C.; Colbert, A.M.; Bennett, I.M. Health Literacy, Health Disparities, and Sources of Health Information in U.S. Older Adults. Orthop. Nurs. 2018, 37, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Fagnano, M.; Halterman, J.S.; Conn, K.M.; Shone, L.P. Health literacy and sources of health information for caregivers of urban children with asthma. Clin. Pediatr. 2012, 51, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Santana, S. Trends of internet use for health matters in Portugal: 2005–2007. Acta Med. Port. 2009, 22, 5–14. [Google Scholar]
- Connell, C.M.; Crawford, C.O. How people obtain their health information--A survey in two Pennsylvania counties. Public Health Rep. 1988, 103, 189–195. [Google Scholar] [PubMed]
- Safeer, R.S.; Keenan, J. Health literacy: The gap between physicians and patients. Am. Fam. Physician 2005, 72, 463–468. [Google Scholar]
- Barry, M.; Sixsmith, J.; D’Eath, M. A Rapid Evidence Review of Interventions for Improving Health Literacy: Insights into Health Communication; European Centre for Disease Prevention Control: Stockholm, Sweden, 2012. [Google Scholar]
- Davis, T.C.; Wolf, M.S. Health literacy: Implications for family medicine. Fam. Med. 2004, 36, 595–598. [Google Scholar]
- Roma, W.; Kloyiam, S.; Sookawong, W.; Kaew-Amdee, T.; Tunnung, A.; Khampang, R.; Butchon, R. Thai Health Literacy Survey (THL-S) of Thai Aged 15 Years and Above. Available online: https://kb.hsri.or.th/dspace/handle/11228/5216 (accessed on 20 February 2022).
- Hone, T.; Mirelman, A.J.; Rasella, D.; Paes-Sousa, R.; Barreto, M.L.; Rocha, R.; Millett, C. Effect of economic recession and impact of health and social protection expenditures on adult mortality: A longitudinal analysis of 5565 Brazilian municipalities. Lancet Glob. Health 2019, 7, e1575–e1583. [Google Scholar] [CrossRef]
- de Moraes Ferrari, G.L.; Kovalskys, I.; Fisberg, M.; Gómez, G.; Rigotti, A.; Sanabria, L.Y.C.; García, M.C.Y.; Torres, R.G.P.; Herrera-Cuenca, M.; Zimberg, I.Z.; et al. Original research Socio-demographic patterning of self-reported physical activity and sitting time in Latin American countries: Findings from ELANS. BMC Public Health 2019, 19, 1723. [Google Scholar] [CrossRef]
- Knodel, J.; Teerawichitchainan, B.; Prachuabmoh, V.; Pothisiri, W. The Situation of Thailand’s Older Population: An Update Based on the 2014 Survey of Older Persons. Available online: https://www.psc.isr.umich.edu/pubs/pdf/rr15-847.pdf (accessed on 16 March 2022).
- Aldin, A.; Chakraverty, D.; Baumeister, A.; Monsef, I.; Noyes, J.; Jakob, T.; Seven, Ü.; Anapa, G.; Woopen, C.; Kalbe, E.; et al. Gender differences in health literacy of migrants: A synthesis of qualitative evidence. Cochrane Database Syst. Rev. 2019, 15, CD013302. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.R. The prevalence of limited health literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef]
- Christy, S.M.; Gwede, C.K.; Sutton, S.K.; Chavarria, E.; Davis, S.N.; Abdulla, R.; Ravindra, C.; Schultz, I.; Roetzheim, R.; Meade, C.D. Health Literacy among Medically Underserved: The Role of Demographic Factors, Social Influence, and Religious Beliefs. J. Health Commun. 2017, 22, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Zanobini, P.; Lorini, C.; Lastrucci, V.; Minardi, V.; Possenti, V.; Masocco, M.; Garofalo, G.; Mereu, G.; Bonaccorsi, G. Health Literacy, Socio-Economic Determinants, and Healthy Behaviours: Results from a Large Representative Sample of Tuscany Region, Italy. Int. J. Environ. Res. Public Health 2021, 18, 12432. [Google Scholar] [CrossRef] [PubMed]
- Peterson, N.B.; Dwyer, K.A.; Mulvaney, S.A.; Dietrich, M.S.; Rothman, R.L. The influence of health literacy on colorectal cancer screening knowledge, beliefs and behavior. J. Natl. Med. Assoc. 2007, 99, 1105–1112. [Google Scholar]
- Gazmararian, J.A.; Kripalani, S.; Miller, M.J.; Echt, K.V.; Ren, J.; Rask, K. Factors associated with medication refill adherence in cardiovascular-related diseases: A focus on health literacy. J. Gen. Intern. Med. 2006, 21, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Manganello, J.A.; Gerstner, G.; Pergolino, K.; Graham, Y.; Strogatz, D. Understanding Digital Technology Access and Use Among New York State Residents to Enhance Dissemination of Health Information. JMIR Public Health Surveill. 2016, 2, e9. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.W.; Gazmararian, J.A.; Sudano, J.; Patterson, M. The Association Between Age and Health Literacy Among Elderly Persons. J. Gerontol. B Psychol. Sci. Soc. Sci. 2000, 55, S368–S374. [Google Scholar] [CrossRef]
- Ashida, S.; Goodman, M.; Pandya, C.; Koehly, L.M.; Lachance, C.; Stafford, J.; Kaphingst, K.A. Age Differences in Genetic Knowledge, Health Literacy and Causal Beliefs for Health Conditions. Public Health Genom. 2011, 14, 307–316. [Google Scholar] [CrossRef]
- Robson, N.; Hosseinzadeh, H. Impact of Telehealth Care among Adults Living with Type 2 Diabetes in Primary Care: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2021, 18, 12171. [Google Scholar] [CrossRef]
- Hanlon, P.; Daines, L.; Campbell, C.; McKinstry, B.; Weller, D.; Pinnock, H. Telehealth Interventions to Support Self-Management of Long-Term Conditions: A Systematic Metareview of Diabetes, Heart Failure, Asthma, Chronic Obstructive Pulmonary Disease, and Cancer. J. Med. Internet. Res. 2017, 19, e172. [Google Scholar] [CrossRef]
- Ang, S.M.; Chen, J.; Liew, J.H.; Johal, J.; Dan, Y.Y.; Allman-Farinelli, M.; Lim, S.L. Efficacy of Interventions That Incorporate Mobile Apps in Facilitating Weight Loss and Health Behavior Change in the Asian Population: Systematic Review and Meta-analysis. J. Med. Internet. Res. 2021, 23, e28185. [Google Scholar] [CrossRef]
- Jiamjariyaporn, T.; Ingsathit, A.; Tungsanga, K.; Banchuin, C.; Vipattawat, K.; Kanchanakorn, S.; Leesmidt, V.; Watcharasaksilp, W.; Saetie, A.; Pachotikarn, C.; et al. Effectiveness of integrated care on delaying chronic kidney disease progression in rural communities of Thailand (ESCORT study): Rationale and design of the study [NCT01978951]. BMC Nephrol. 2014, 15, 99. [Google Scholar] [CrossRef] [PubMed]
- Augsornwan, D.; Pradubwong, S.; Prathumwiwattana, P.; Sucontaman, D.; Surakunprapha, P. Home visit patients and family with cleft lip and palate. J. Med. Assoc. Thai. 2011, 94 (Suppl. 6), S109–S113. [Google Scholar] [PubMed]
- Songserm, N.; Butprom, S.; Thongchai, C.; Ruksilp, M.; Charoenbut, P.; Woradet, S.; Souvanaa, T.; Buonhoseng, V.; Ali, A. Effectiveness of Village Health Volunteer Parallel Program for Proactive Action to Reduce Risk Factors for Cholangiocarcinoma in Two High-Risk Countries in the Greater Mekong Subregion. Nutr. Cancer 2021, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pattanarattanamolee, R.; Sanglun, R.Y.; Nakahara, S. Community-Based First Responder Network in Rural Thailand: A Case Study of Out-of-Hospital Cardiac Arrest. Prehosp. Disaster Med. 2021, 36, 234–236. [Google Scholar] [CrossRef]
- Kowitt, S.D.; Emmerling, D.; Fisher, E.B.; Tanasugarn, C. Community Health Workers as Agents of Health Promotion: Analyzing Thailand’s Village Health Volunteer Program. J. Community Health 2015, 40, 780–788. [Google Scholar] [CrossRef] [PubMed]
- Sawaengthong, P.; Sanguanprasit, B. Community Health Volunteer: Experience From Rural Thailand. J. Ambul. Care Manag. 2015, 38, 215–216. [Google Scholar] [CrossRef]
- Ben Hassen, C.; Fayosse, A.; Landré, B.; Raggi, M.; Bloomberg, M.; Sabia, S.; Singh-Manoux, A. Association between age at onset of multimorbidity and incidence of dementia: 30 year follow-up in Whitehall II prospective cohort study. BMJ 2022, 376, e068005. [Google Scholar] [CrossRef]
- Wang, X.; Shi, J.; Kong, H. Online Health Information Seeking: A Review and Meta-Analysis. Health Commun. 2021, 36, 1163–1175. [Google Scholar] [CrossRef]
- Williams, S.J.; Nightingale, E.O.; Filner, B. Chapter 4, The Physician’s Role in a Changing Health Care System. In Medical Education and Societal Needs: A Planning Report for the Health Professions; National Academies Press: Washington, DC, USA, 1983. [Google Scholar]
- Avery, L.S.; Du Plessis, E.; Shaw, S.Y.; Sankaran, D.; Njoroge, P.; Kayima, R.; Makau, N.; Munga, J.; Kadzo, M.; Blanchard, J.; et al. Enhancing the capacity and effectiveness of community health volunteers to improve maternal, newborn and child health: Experience from Kenya. Can. J. Public Health 2017, 108, e427–e434. [Google Scholar] [CrossRef]
- Barnet, B.; Duggan, A.K.; Devoe, M.; Burrell, L. The effect of volunteer home visitation for adolescent mothers on parenting and mental health outcomes: A randomized trial. Arch. Pediatr. Adolesc. Med. 2002, 156, 1216–1222. [Google Scholar] [CrossRef][Green Version]
- Nonaka, D.; Pongvongsa, T.; Nishimoto, F.; Nansounthavong, P.; Hongwei, J.; Vongsouvanh, A.; Moji, K.; Phongmany, P.; Kobayashi, J. Successful mobile phone network-based approach to integration of the health care system in rural Laos: Strengthening lay health worker performance. Rural Remote Health 2014, 14, 2588. [Google Scholar] [CrossRef] [PubMed]
- Gyawali, B.; Sharma, R.; Mishra, S.R.; Neupane, D.; Vaidya, A.; Sandbæk, A.; Kallestrup, P. Effectiveness of a Female Community Health Volunteer-Delivered Intervention in Reducing Blood Glucose Among Adults With Type 2 Diabetes: An Open-Label, Cluster Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2035799. [Google Scholar] [CrossRef] [PubMed]
- Kshatri, J.S.; Palo, S.K.; Panda, M.; Swain, S.; Sinha, R.; Mahapatra, P.; Pati, S. Reach, accessibility and acceptance of different communication channels for health promotion: A community-based analysis in Odisha, India. J. Prev. Med. Hyg. 2021, 62, e455–e465. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.C.; Pathak, A.; Chaurasia, R.N.; Joshi, D.; Singh, R.K.; Mishra, V.N. Fighting infodemic: Need for robust health journalism in India. Diabetes Metab. Syndr. 2020, 14, 1445–1447. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Simply Put; a Guide for Creating Easy-to-Understand Materials; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010.
- Jia, X.; Pang, Y.; Liu, L.S. Online Health Information Seeking Behavior: A Systematic Review. Healthcare 2021, 9, 1740. [Google Scholar] [CrossRef]
- Van Olmen, J. The Promise of Digital Self-Management: A Reflection about the Effects of Patient-Targeted e-Health Tools on Self-Management and Wellbeing. Int. J. Environ. Res. Public Health 2022, 19, 1360. [Google Scholar] [CrossRef]
- Zhang, D.; Zhan, W.; Zheng, C.; Zhang, J.; Huang, A.; Hu, S.; Ba-Thein, W. Online health information-seeking behaviors and skills of Chinese college students. BMC Public Health 2021, 21, 736. [Google Scholar] [CrossRef]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayrek, J.; Batcup, C.; Isautier, J.M.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Health literacy and disparities in COVID-19-related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pract. 2020, 30, e30342012. [Google Scholar] [CrossRef]
- Turhan, Z.; Dilcen, H.Y.; Dolu, İ. The mediating role of health literacy on the relationship between health care system distrust and vaccine hesitancy during COVID-19 pandemic. Curr. Psychol. 2021, 8, 1–10. [Google Scholar] [CrossRef]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- Paakkari, L.; Okan, O. COVID-19: Health literacy is an underestimated problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Bandyopadhyay, M.; Stanzel, K.; Hammarberg, K.; Hickey, M.; Fisher, J. Accessibility of web-based health information for women in midlife from culturally and linguistically diverse backgrounds or with low health literacy. Aust. N. Z. J. Public Health 2021, 13, 192. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hay, J.L.; Waters, E.A.; Kiviniemi, M.T.; Biddle, C.; Schofield, E.; Li, Y.; Kaphingst, K.; Orom, H. Health Literacy and Use and Trust in Health Information. J. Health Commun. 2018, 23, 724–734. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subindices | Topics | Questions | |
|---|---|---|---|
| (1) Accessing information relevant to health (8 items) | Health services | S1 | What to do if someone is unconscious |
| S2 | Symptoms require immediate hospitalization | ||
| Disease prevention | S3 | Health check-up or vaccinations should be given | |
| S4 | Self-prevention from communicable diseases | ||
| Health promotion | S5 | How to maintain health | |
| S6 | Proper way to manage stress | ||
| Consumer protection | S7 | Reliable information about medicines, cosmetics, herbs, and supplements | |
| S8 | Reliable information about health services, new products, or equipment | ||
| (2) Understanding information relevant to health (7 items) | Health services | U9 | Public media, online media or what to do in a medical emergency |
| Disease prevention | U10 | Why you should have a health screening | |
| U11 | Understand why you need a vaccine | ||
| Health promotion | U12 | Warnings about how important and necessary healthy behaviors are | |
| U13 | How to maintain good mental health | ||
| Consumer protection | U14 | Understand the labels for drugs, cosmetics, dietary supplements, herbs, medical devices, and dangerous substances | |
| U15 | Description of new health services, products, or equipment | ||
| (3) Questioning information relevant to health (12 items) | Health services | Q16 | Ask your doctor about your rights, expenses, and concerns |
| Q17 | Ask the nurse about your rights, expenses, and concerns. | ||
| Q18 | Ask the hospital worker about your rights, expenses, and concerns. | ||
| Disease prevention | Q19 | Ask your doctor about the disease and the practice of prevention | |
| Q20 | Ask the nurse about the disease and the practice of prevention | ||
| Q21 | Ask the health volunteer about the disease and the practice of prevention | ||
| Health promotion | Q22 | Ask your doctor for information on how to stay healthy | |
| Q23 | Ask the nurse for information on how to stay healthy | ||
| Q24 | Ask the health volunteer for information on how to stay healthy | ||
| Consumer protection | Q25 | Ask your doctor about health products | |
| Q26 | Ask the nurse about health products | ||
| Q27 | Ask the health volunteer about health products | ||
| (4) Appraising information relevant to health (7 items) | Health services | D28 | Decide how you follow an emergency information |
| Disease prevention | D29 | Decide how you follow a complete treatment plan | |
| D30 | Decide what you will do in order to use the drug correctly | ||
| Health promotion | D31 | Decide how you should exercise | |
| D32 | Decide what foods to buy or how to cook | ||
| D33 | Decide what activities you should do to reduce stress | ||
| Consumer protection | D34 | Decide to choose a supplement, nutrition, or herbs | |
| (5) Applying information to change behaviors (8 items) | Health promotion | B35 | Choose bland food more than sweet, salty, and oily food |
| Disease prevention/Health promotion | B36 | Do not share a spoon with others while eating | |
| Health promotion | B37 | Exercise to strengthen muscles 3–4 days a week. | |
| Disease prevention/Health promotion | B38 | Manage your stress appropriately | |
| Consumer protection | B39 | Read and review the information provided with cosmetics, supplements, or herbs | |
| B40 | Inspect health products, services, cosmetics, medical devices, and hazardous substances | ||
| Health services | B41 | If you find someone drowning, help by “yelling, throwing, handing” and calling 1669. | |
| Health promotion | B42 | Encourage all children to receive developmental assessment and vaccination as needed |
| Characteristics | Total (n = 1510) | Age Group (Years) | p-Value | ||
|---|---|---|---|---|---|
| 15–29 (n = 214) | 30–59 (n = 691) | ≥60 (n = 605) | |||
| n (%) | n (%) | n (%) | n (%) | ||
| Gender | |||||
| Male | 614 (40.7) | 94 (43.9) | 279 (40.4) | 241 (39.8) | 0.566 |
| Female | 896 (59.3) | 120 (56.1) | 412 (59.6) | 364 (60.2) | |
| Marital status | |||||
| Single | 323 (21.4) | 159 (74.3) | 127 (18.4) | 37 (6.1) | <0.001 ** |
| Married | 976 (64.7) | 52 (24.3) | 502 (72.8) | 422 (69.8) | |
| Divorced/Widowed | 210 (13.9) | 3 (1.4) | 61 (8.8) | 146 (24.1) | |
| Education level | |||||
| Illiterate | 142 (9.4) | 4 (1.9) | 45 (6.5) | 93 (15.4) | <0.001 ** |
| Primary school | 713 (47.2) | 13 (6.1) | 279 (40.4) | 421 (69.6) | |
| High school/vocational school | 423 (28.0) | 145 (67.7) | 216 (31.3) | 62 (10.2) | |
| University | 232 (15.4) | 52 (24.3) | 151 (21.8) | 29 (4.8) | |
| Occupation | |||||
| Unemployed/retired/housekeeper | 398 (26.4) | 27 (12.6) | 72 (10.4) | 299 (49.4) | <0.001 ** |
| Official worker | 113 (7.5) | 21 (9.8) | 83 (12.0) | 9 (1.5) | |
| Farmer/laborer | 624 (41.3) | 54 (25.3) | 349 (50.5) | 221 (36.5) | |
| Merchant/business owner | 281 (18.6) | 21 (9.8) | 184 (26.6) | 76 (12.6) | |
| Student | 94 (6.2) | 91 (42.5) | 3 (0.4) | 0 (0.0) | |
| Self-perception of income | |||||
| Insufficient | 752 (49.8) | 109 (50.9) | 351 (50.8) | 292 (48.3) | 0.802 |
| Sufficient | 627 (41.5) | 84 (39.3) | 284 (41.1) | 259 (42.8) | |
| More than sufficient | 131 (8.7) | 21 (9.8) | 56 (8.1) | 54 (8.9) | |
| Household size (person) | |||||
| One | 140 (9.3) | 13 (6.1) | 67 (9.7) | 60 (9.9) | <0.001 ** |
| Two | 619 (41.0) | 46 (21.5) | 281 (40.7) | 292 (48.3) | |
| Three to four | 665 (44.0) | 126 (58.9) | 311 (45.0) | 228 (37.7) | |
| Five or more | 86 (5.7) | 29 (13.5) | 32 (4.6) | 25 (4.1) | |
| Living location | |||||
| In municipality | 942 (62.4) | 136 (63.6) | 410 (59.3) | 396 (65.4) | 0.071 |
| Outside municipality | 568 (37.6) | 78 (36.4) | 281 (40.7) | 209 (34.6) | |
| Number of chronic conditions | |||||
| None | 816 (54.0) | 195 (91.1) | 428 (61.9) | 193 (31.9) | <0.001 ** |
| One | 363 (24.0) | 16 (7.5) | 160 (23.2) | 187 (30.9) | |
| Two | 214 (14.2) | 3 (1.4) | 72 (10.4) | 139 (23.0) | |
| Three or more | 117 (7.8) | 0 (0.0) | 31 (4.5) | 86 (14.2) | |
| Variables | β | (95%CI) | p-Value |
|---|---|---|---|
| Characteristics and socio-demographics | |||
| Age (years) | |||
| 15–29 | Ref. | ||
| 30–59 | −2.45 | −5.23 to 0.33 | 0.084 |
| ≥60 | −9.26 | −12.62 to −5.89 | <0.001 ** |
| Gender | |||
| Male | Ref. | ||
| Female | 1.67 | 0.06 to 3.28 | 0.042 * |
| Marital status | |||
| Single | Ref. | ||
| Married | 0.29 | −1.99 to 2.58 | 0.800 |
| Divorced/Widowed | −4.43 | −7.55 to −1.31 | 0.005 * |
| Education level | |||
| Illiterate | Ref. | ||
| Primary school | 14.53 | 11.52 to 17.55 | <0.001 ** |
| High school/vocational school | 20.77 | 17.32 to 24.22 | <0.001 ** |
| University | 23.66 | 19.75 to 27.56 | <0.001 ** |
| Occupation | |||
| Unemployed | Ref. | ||
| Employed | 2.11 | 0.14 to 4.07 | 0.036 |
| Self-perception of income | |||
| Insufficient | Ref. | ||
| Sufficient | 0.55 | −1.08 to 2.18 | 0.507 |
| More than sufficient | 2.69 | −0.16 to 5.54 | 0.064 |
| Living location | |||
| In municipality | Ref. | ||
| Outside municipality | −1.41 | −3.14 to 0.32 | 0.109 |
| Household size (no. of person) | −0.55 | −1.61 to 0.51 | 0.311 |
| No. of chronic conditions | −0.13 | −0.93 to 0.68 | 0.756 |
| Source of health information from health personnel | |||
| Health volunteer | 2.64 | 0.90 to 4.37 | 0.003 * |
| Public health worker | 0.97 | −0.75 to 2.71 | 0.270 |
| Physician | 4.02 | 1.62 to 6.07 | 0.001 ** |
| Nurse | 0.46 | −1.82 to 2.73 | 0.695 |
| Pharmacist | −0.50 | −3.19 to 2.19 | 0.715 |
| Source of health information from media | |||
| Television | −0.43 | −2.20 to 1.33 | 0.631 |
| Community radio | −2.87 | −4.57 to -1.18 | 0.001 * |
| Commercial and public radio | 1.87 | 0.06 to 3.68 | 0.043 * |
| Internet | 3.51 | 1.08 to 5.93 | 0.005 * |
| 1.21 | −1.32 to 3.75 | 0.348 | |
| LINE application | 2.63 | 0.25 to 5.01 | 0.031 * |
| Magazine/Newspaper | 4.62 | 2.24 to 7.01 | <0.001 ** |
| Constant | 88.17 | 82.41 to 93.92 | <0.001 ** |
| R = 0.405, Adjusted R2 = 0.394, F = 36.38, p < 0.001 ** | |||
| Variables | Subgroup Analysis by Age Groups | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 15–29 Years (n = 214) | 30–59 Years (n = 691) | ≥60 years (n = 605) | |||||||
| β | (95%CI) | p-Value | β | (95%CI) | p-Value | β | (95%CI) | p-Value | |
| Characteristics and socio-demographics | |||||||||
| Gender | |||||||||
| Male | Ref. | Ref. | Ref. | ||||||
| Female | 1.83 | −2.61 to 6.26 | 0.418 | 1.36 | −1.02 to 3.74 | 0.262 | 1.83 | −0.84 to 4.49 | 0.178 |
| Marital status | |||||||||
| Single | Ref. | Ref. | Ref. | ||||||
| Married | −0.18 | −5.48 to 5.11 | 0.773 | −0.49 | −3.51 to 2.53 | 0.751 | 3.35 | −1.96 to 8.66 | 0.215 |
| Divorced/Widowed | −10.98 | −29.26 to 7.30 | 0.237 | −2.60 | −7.38 to 2.17 | 0.285 | −2.01 | −7.60 to 3.58 | 0.481 |
| Education level | |||||||||
| Illiterate | Ref. | Ref. | Ref. | ||||||
| Primary school | −16.43 | −35.08 to 2.22 | 0.084 | 22.08 | 17.06 to 27.09 | <0.001 ** | 11.13 | 7.22 to 15.05 | <0.001 ** |
| High school/vocational school | −3.69 | −20.68 to 13.31 | 0.669 | 27.49 | 22.20 to 32.77 | <0.001 ** | 16.21 | 10.78 to 21.63 | <0.001 ** |
| University | −0.21 | −17.77 to 17.34 | 0.981 | 30.44 | 24.58 to 36.31 | <0.001 ** | 18.89 | 11.78 to 26.00 | <0.001 ** |
| Occupation | |||||||||
| Unemployed | Ref. | Ref. | Ref. | ||||||
| Employed | −5.59 | −12.33 to 1.16 | 0.104 | 2.14 | −1.57 to 5.84 | 0.258 | 3.33 | 0.80 to 5.86 | 0.010 * |
| Self-perception of income | |||||||||
| Insufficient | Ref. | Ref. | Ref. | ||||||
| Sufficient | −0.45 | −5.01 to 4.12 | 0.848 | −0.92 | −3.32 to 1.48 | 0.451 | 1.99 | −0.61 to 4.59 | 0.133 |
| More than sufficient | 7.14 | −0.34 to 14.63 | 0.061 | 0.28 | −4.11 to 4.67 | 0.899 | 4.00 | −0.40 to 8.41 | 0.075 |
| Living location | |||||||||
| In municipality | Ref. | Ref. | Ref. | ||||||
| Outside municipality | 1.25 | −3.75 to 6.24 | 0.623 | −0.27 | −2.82 to 2.27 | 0.833 | −2.11 | −4.86 to 0.64 | 0.133 |
| Household size (no. of person) | −1.59 | −4.54 to 1.37 | 0.291 | −0.24 | −1.82 to 1.33 | 0.761 | −0.69 | −2.37 to 0.99 | 0.418 |
| No. of chronic conditions | −1.02 | −7.32 to 5.28 | 0.749 | −0.15 | −1.42 to 1.13 | 0.822 | −0.25 | −1.30 to 0.80 | 0.640 |
| Source of health information from health personnel | |||||||||
| Health volunteer | 5.37 | −0.83 to 11.57 | 0.089 | 2.89 | 0.38 to 5.39 | 0.024 * | 0.49 | −2.16 to 3.14 | 0.716 |
| Public health worker | −2.59 | −8.48 to 3.29 | 0.386 | 1.14 | −1.47 to 3.75 | 0.391 | 1.56 | −1.05 to 4.17 | 0.241 |
| Physician | 6.45 | 0.44 to 12.45 | 0.035 * | 1.74 | −1.66 to 5.12 | 0.315 | 5.18 | 1.84 to 8.52 | 0.002 * |
| Nurse | 0.21 | −5.96 to 6.38 | 0.947 | −0.83 | −4.48 to 2.82 | 0.655 | 1.90 | −1.53 to 5.34 | 0.277 |
| Pharmacist | 3.27 | −3.10 to 9.63 | 0.312 | −0.42 | −4.37 to 3.52 | 0.832 | −1.15 | −6.17 to 3.85 | 0.651 |
| Source of health information from media | |||||||||
| Television | −3.05 | −8.03 to 1.93 | 0.228 | −0.69 | −3.31 to 1.94 | 0.609 | 0.41 | −2.37 to 3.18 | 0.774 |
| Community radio | −4.68 | −10.70 to 1.33 | 0.126 | −1.89 | −4.32 to 0.54 | 0.128 | −3.13 | −5.71 to −0.55 | 0.018 * |
| Commercial and public radio | −2.75 | −8.74 to 3.24 | 0.366 | 0.84 | −1.86 to 3.55 | 0.541 | 4.15 | 1.44 to 6.85 | 0.003 * |
| Internet | 0.45 | −5.15 to 6.06 | 0.874 | 5.41 | 2.27 to 8.54 | <0.001 * | 1.23 | −5.01 to 7.48 | 0.698 |
| 0.36 | −4.71 to 5.45 | 0.886 | 0.85 | −2.57 to 4.28 | 0.626 | 5.03 | −1.48 to 11.53 | 0.130 | |
| LINE application | 3.12 | −1.75 to 8.00 | 0.208 | 2.92 | −0.36 to 6.20 | 0.081 | 2.89 | −2.73 to 8.52 | 0.313 |
| Magazine/Newspaper | 4.17 | −1.52 to 9.85 | 0.150 | 4.43 | 0.85 to 8.00 | 0.015 * | 5.97 | 1.89 to 10.06 | 0.004 * |
| Constant | 129.78 | 109.45 to 150.10 | <0.001 ** | 86.89 | 77.94 to 95.84 | <0.001 ** | 85.29 | 75.80 to 94.78 | <0.001 ** |
| R = 0.240, Adjusted R2 = 0.137 F = 2.34, p= 0.001 ** | R = 0.335, Adjusted R2 = 0.309, F = 13.26, p < 0.001 ** | R = 0.321, Adjusted R2 = 0.290, F = 10.41, p < 0.001 ** | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buawangpong, N.; Sirikul, W.; Anukhro, C.; Seesen, M.; La-up, A.; Siviroj, P. Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens. Int. J. Environ. Res. Public Health 2022, 19, 6051. https://doi.org/10.3390/ijerph19106051
Buawangpong N, Sirikul W, Anukhro C, Seesen M, La-up A, Siviroj P. Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens. International Journal of Environmental Research and Public Health. 2022; 19(10):6051. https://doi.org/10.3390/ijerph19106051
Chicago/Turabian StyleBuawangpong, Nida, Wachiranun Sirikul, Chanya Anukhro, Mathuramat Seesen, Aroon La-up, and Penprapa Siviroj. 2022. "Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens" International Journal of Environmental Research and Public Health 19, no. 10: 6051. https://doi.org/10.3390/ijerph19106051
APA StyleBuawangpong, N., Sirikul, W., Anukhro, C., Seesen, M., La-up, A., & Siviroj, P. (2022). Health Information Sources Influencing Health Literacy in Different Social Contexts across Age Groups in Northern Thailand Citizens. International Journal of Environmental Research and Public Health, 19(10), 6051. https://doi.org/10.3390/ijerph19106051