
Injuries in Wheelchair Basketball Players: A Systematic Review

 ,
,  ,
, 
 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
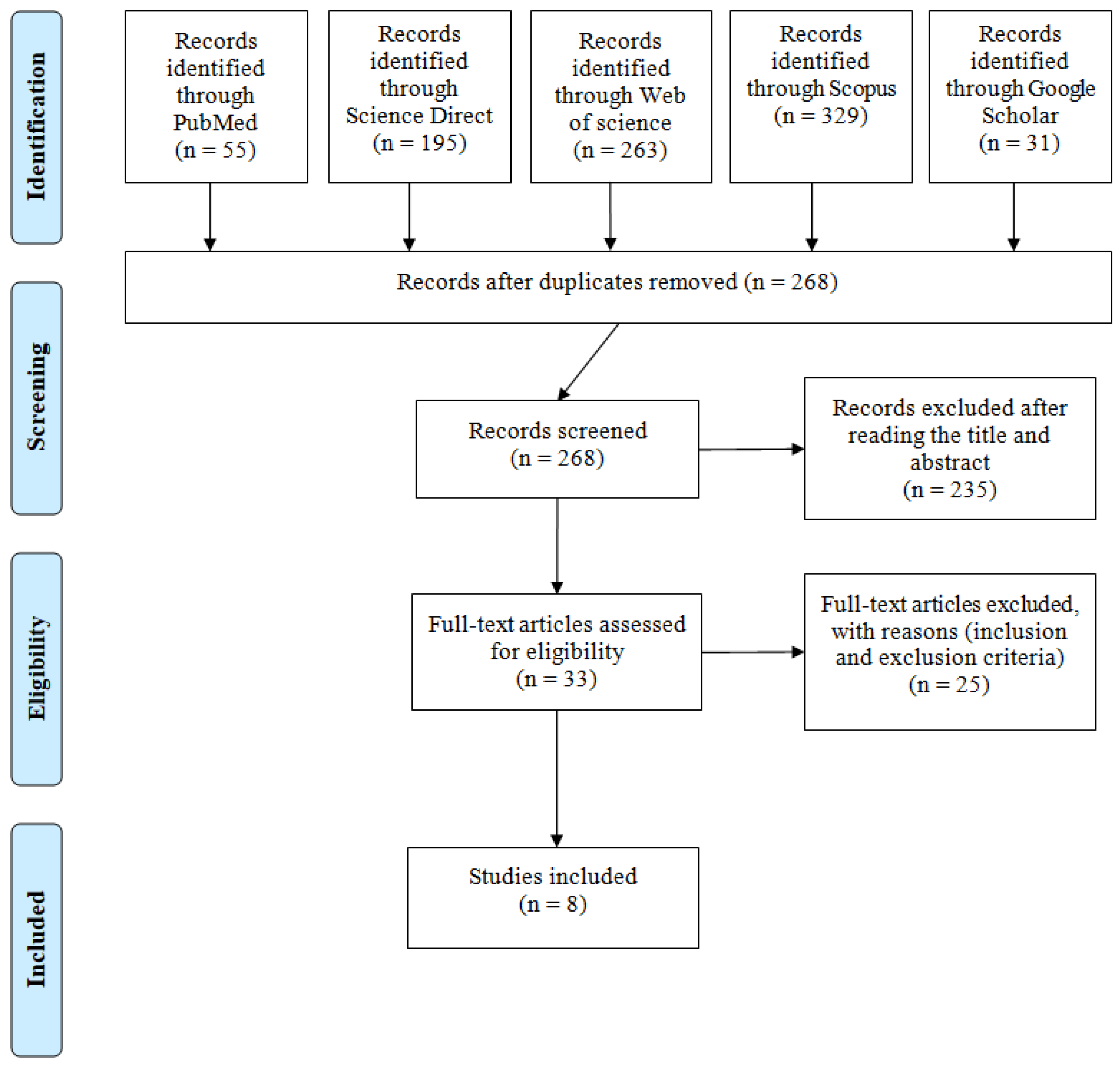
3.1. Included Studies
3.2. Quality Assessment
3.3. Study Characteristics
4. Discussion
4.1. Study Populations
4.2. Sports Injury Mechanism
4.3. Upper Limb Injuries
4.4. Head Injuries
4.5. Lower Limbs Injuries (Knee, Hip and Ischiatic Region)
4.6. Spinal Injuries (Cervical, Thoracic and Lumbar)
4.7. Collection Pattern
4.8. Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Item | Item No | Recommendation from the STROBE Statement | STROBE-SIIS Extension | Soo Hoo et al. (2018) | Shimizu et al. (2017) | Wessels et al. (2012) | Mutsuzaki et al. (2014) | Huzmeli et al. (2017) | Rocco and Saito (2006) | Curtis and Black (1999) | Hollander et al. (2020) |
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | Yes | Yes | Yes | No | Yes | No | Yes | Yes | |
| (b) Provide in the abstract an informative and balanced summary of what was carried out and what was found | SIIS-1.1. Include information on the sport, athlete population (sex, age, geographic region) and level of competition. SIIS-1.2. Include the duration of observation (e.g., one season, one year, multiple years). | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| Introduction | |||||||||||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Objectives | 3 | State specific objectives, including any pre-specified hypotheses | SIIS-3.1. State whether study was registered. Identify the registration number and database used. SIIS-3.2. State the specific purpose of your study (e.g., to describe the injury burden associated with Olympic-level rowing) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Methods | |||||||||||
| Study design | 4 | Present key elements of study design early in the paper | SIIS-4.1. Clearly specify which health problems are being observed. SIIS-4.2. State explicitly which approach was used to record the health problem data, including all outcome measures or tools SIIS-4.3. State explicitly which coding system was used to classify the health problems (e.g., OSIICS, SMDCS, ICD, etc.) SIIS-4.4. Where relevant, clearly describe how athletes were categorized. Variables to consider could include the type of athlete and/or sport, the environment in which the sport occurs (e.g., type of course or playing area), the typical duration of the sport, the degree of physical contact permitted in the sport and the equipment permitted. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Setting | 5 | Describe the setting, locations and relevant dates, including periods of recruitment, exposure, follow-up and data collection | SIIS-5.1. Describe the location, level of play, dates of observation and data collection methods (i.e., who, what, where). SIIS-5.2. Specify the dates of the surveillance period and how the data were handled when the study covered more than one season/calendar year. SIIS-5.3. Define whether the health problem data were collected prospectively or retrospectively. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Participants | 6 | (a) Cohort study—give the eligibility criteria and the sources and methods of selection of participants. Describe methods of follow-up Case-control study—give the eligibility criteria and the sources and methods of case ascertainment and control selection. Give the rationale for the choice of cases and controls Cross-sectional study—give the eligibility criteria and the sources and methods of selection of participants | SIIS-6.1. Define the population of athletes and how they were selected and recruited. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| (b) Cohort study—for matched studies, give matching criteria and number of exposed and unexposed Case-control study—for matched studies, give matching criteria and the number of controls per case | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders and effect modifiers. Give diagnostic criteria, if applicable | SIIS-7.1. Justify why you measured your primary and secondary outcomes of interest in the specific way chosen. SIIS-7.2. Describe the method for identifying your health predictor | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Data sources/measurement | 8 | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | SIIS-8.1. Specify who collected/reported the data for the study and their qualifications (e.g., qualified doctor, data analyst, etc.). SIIS-8.2. Specify who coded the data for the study and their qualifications (e.g., qualified doctor, data analyst, etc.). In many instances, this will not be the same as SIIS-8.1. SIIS-8.3. Specify the direct methods used to collect the data and the use of physical documents or any electronic tools. If extracting information from existing sources, specify the data source. SIIS-8.4. Specify the timing of and window for data collection (e.g., day health problem occurred or following day). Specify the frequency of data collection (e.g., daily, weekly, monthly). SIIS-8.5. Report the duration of surveillance (e.g., tournament, season, whole year, playing career). | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Bias | 9 | Describe any efforts to address potential sources of bias | SIIS-9.1. Clearly report any validation or reliability assessment of the data collection of tools. SIIS-9.2. Formally acknowledge any potential biases in associated with the data collection method (e.g., self- report, recall bias, reporting by nonmedically trained staff, etc.) | No | No | No | No | No | No | No | No |
| Study size | 10 | Explain how the study size was arrived at | No | Yes | Yes | Yes | Yes | No | Yes | Yes | |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | SIIS-11.1 Explain in detail how multiple injuries/illness episodes are handled both in individual athletes and across athletes/surveillance periods. SIIS-11.2. Specify how injury severity was calculated. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | SIIS-12.1. Specify how exposure to risk has been adjusted for and specify the units (e.g., per participant, per athlete exposure, etc.). SIIS-12.2 Specify how relevant risk measures (incidence, prevalence, etc.) were calculated. SIIS-12.3. When relevant to the study aim, specify how injury occurred. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| (b) Describe any methods used to examine subgroups and interactions | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| (c) Explain how missing data were addressed | SIIS-12.4. For studies reporting multiple health problems, state clearly how these were handled (e.g., time to the first injury only, ignoring subsequent return to play and reinjuries, or modeling of all injuries). SIIS-12.5. Explain how/if athletes not included at outset (e.g., those already injured) were handled in the analyses. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| (d) Cohort study—if applicable, explain how loss to follow-up was addressed Case-control study—if applicable, explain how matching of cases and controls was addressed Cross-sectional study—if applicable, describe analytical methods taking account of sampling strategy | SIIS-12.6. In longitudinal studies, it is particularly important to explain how athlete follow-up has been managed. For example, what happened if a player was transferred to another team or has been censored (for those no longer part of the study due to removal during the observation period). Censoring can occur when athletes are removed due to transfer out of the team/study, injury/illness or due to study design. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| (e) Describe any sensitivity analyses | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| Results | |||||||||||
| Participants | 13 | (a) Report numbers of individuals at each stage of study—e.g., numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up and analyzed | SIIS-13.1. Clearly state the number of athletes followed-up, the number (and %) of those with the health problem and the number of problems reported among them (a median number of problems per affected athlete could be useful). SIIS-13.2. For studies over multiple seasons/years, report the total numbers of health problems for each year and numbers common to each period. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| (b) Give reasons for non-participation at each stage | SIIS-13.3. Report how athletes removed (e.g., due to transfer of teams or time-out due to injury or illness) impact upon data at key data collection/reporting points, ideally with a flow diagram | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| Descriptive data | 14 | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders | SIIS-14.1. Include detail on the level of competition being observed (e.g., by age levels, skill level, sex, etc.). | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| (b) Indicate number of participants with missing data for each variable of interest | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| (c) Cohort study—summarize follow-up time (e.g., average and total amount) | NA | NA | NA | NA | NA | NA | NA | NA | |||
| Outcome data | 15 | Cohort study—report numbers of outcome events or summary measures over time | SIIS-15.1. In many observational studies, individuals will sustain more than one health problem over the surveillance period. Take care to ensure descriptive data representing both the number of health problems and the number of athletes affected. It is important to represent effectively both the analysis and reporting of correct units for frequency data, i.e., the % of affected athletes or the % of injuries, body regions, etc. | NA | NA | NA | NA | NA | NA | NA | NA |
| Case-control study—report numbers in each exposure category, or summary measures of exposure | NA | NA | NA | NA | NA | NA | NA | NA | |||
| Cross-sectional study—report numbers of outcome events or summary measures | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | SIIS-16.1. Report exposure-adjusted incidence or prevalence measures with appropriate confidence intervals when presenting risk measures. SIIS-16.2. Report details of interest, such as mode of onset | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| (b) Report category boundaries when continuous variables were categorized | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | No | No | No | No | No | No | No | No | |||
| Other analyses | 17 | Report other analyses conducted—e.g., analyses of subgroups and interactions, and sensitivity analyses | SIIS-17.1 Report injury diagnosis information, including region and tissue type in tabular form. | No | No | No | No | No | No | No | No |
| Discussion | |||||||||||
| Key results | 18 | Summarize key results with reference to study objectives | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | SIIS-19.1. Discuss limitations in the data collection and coding procedures adopted, including in relation to any risk measures calculated. | Yes | Yes | Yes | Yes | No | No | Yes | Yes |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies and other relevant evidence | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Generalizability | 21 | Discuss the generalizability (external validity) of the study results | SIIS-21.1. Discuss the generalizability of the athlete study population, and health problem subgroups of interest, to broader athlete groups. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Other information | |||||||||||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |
| Ethics | 23 | SIIS-23.1. Outline how individual athlete data privacy and confidentiality considerations were addressed, in line with the Declaration of Helsinki. | No | Yes | Yes | Yes | No | No | No | Yes | |
References
- IWBF History of Wheelchair Basketball. IWBF—International Wheelchair Basketball Federation. IWBF, Switzerland 2018. Available online: https://iwbf.org/the-game/history-wheelchair-basketball/ (accessed on 10 November 2020).
- Schneider, S.; Seither, B.; Tönges, S.; Schmitt, H. Sports injuries: Population based representative data on incidence, diagnosis, sequelae, and high risk groups. Br. J. Sports Med. 2006, 40, 334–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.-J.; Meierbachtol, A.; George, S.Z.; Chmielewski, T.L. Fear of Reinjury in Athletes. Sports Health 2017, 9, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M.; et al. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br. J. Sports Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willick, S.E.; Webborn, N.; Emery, C.; Blauwet, C.A.; Pit-Grosheide, P.; Stomphorst, J.; Van de Vliet, P.; Marques, N.A.P.; Martinez-Ferrer, J.O.; Jordaan, E.; et al. The epidemiology of injuries at the London 2012 Paralympic Games. Br. J. Sports Med. 2013, 47, 426–432. [Google Scholar] [CrossRef]
- Macedo, C.S.G.; Tadiello, F.F.; Medeiros, L.T.; Antonelo, M.C.; Alves, M.A.F.; Mendonça, L.D. Physical Therapy Service delivered in the Polyclinic During the Rio 2016 Paralympic Games. Phys. Ther. Sport 2019, 36, 62–67. [Google Scholar] [CrossRef]
- Derman, W.; Schwellnus, M.P.; Jordaan, E.; Runciman, P.; Blauwet, C.; Webborn, N.; Lexell, J.; Van de Vliet, P.; Tuakli-Wosornu, Y.; Kissick, J.; et al. Sport, sex and age increase risk of illness at the Rio 2016 Summer Paralympic Games: A prospective cohort study of 51,198 athlete days. Br. J. Sports Med. 2018, 52, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Soligard, T.; Steffen, K.; Palmer, D.; Alonso, J.M.; Bahr, R.; Lopes, A.D.; Dvorak, J.; Grant, M.-E.; Meeuwisse, W.; Mountjoy, M.; et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: A prospective study of 11274 athletes from 207 countries. Br. J. Sports Med. 2017, 51, 1265–1271. [Google Scholar] [CrossRef]
- Junge, A.; Langevoort, G.; Pipe, A.; Peytavin, A.; Wong, F.; Mountjoy, M.; Beltrami, G.; Terrell, R.; Holzgraefe, M.; Charles, R.; et al. Injuries in Team Sport Tournaments during the 2004 Olympic Games. Am. J. Sports Med. 2006, 34, 565–576. [Google Scholar] [CrossRef]
- Junge, A.; Engebretsen, L.; Mountjoy, M.L.; Alonso, J.M.; Renström, P.A.F.H.; Aubry, M.J.; Dvorak, J. Sports Injuries during the Summer Olympic Games 2008. Am. J. Sports Med. 2009, 37, 2165–2172. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Phys. Ther. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, K.A.; Black, K. Shoulder pain in female wheelchair basketball players. J. Orthop. Sports Phys. Ther. 1999, 29, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Rocco, F.M.; Saito, E.T. Epidemiology of sportive injuries in basketball wheelchair players. Acta Fisiatr 2006, 13, 17–20. [Google Scholar]
- Wessels, K.K.; Broglio, S.P.; Sosnoff, J.J. Concussions in Wheelchair Basketball. Arch. Phys. Med. Rehabil. 2012, 93, 275–278. [Google Scholar] [CrossRef]
- Mutsuzaki, H.; Tachibana, K.; Shimizu, Y.; Hotta, K.; Fukaya, T.; Karasawa, M.; Ikeda, E.; Wadano, Y. Factors associated with deep tissue injury in male wheelchair basketball players of a Japanese national team. Asia-Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2014, 1, 72–76. [Google Scholar] [CrossRef] [Green Version]
- Shimizu, Y.; Mutsuzaki, H.; Tachibana, K.; Tsunoda, K.; Hotta, K.; Fukaya, T.; Ikeda, E.; Yamazaki, M.; Wadano, Y. A survey of deep tissue injury in elite female wheelchair basketball players. J. Back Musculoskelet. Rehabil. 2017, 30, 427–434. [Google Scholar] [CrossRef]
- Huzmeli, E.D.; Katayifci, N.; Hallaceli, H. Injuries in Wheelchair Basketball Players. New Trends Issues Proc. Adv. Pure Appl. Sci. 2017, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Soo Hoo, J.A.; Latzka, E.; Harrast, M.A. A Descriptive Study of Self-Reported Injury in Non-elite Adaptive Athletes. PM&R 2019, 11, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Hollander, K.; Kluge, S.; Glöer, F.; Riepenhof, H.; Zech, A.; Junge, A. Epidemiology of injuries during the Wheelchair Basketball World Championships 2018: A prospective cohort study. Scand. J. Med. Sci. Sports 2020, 30, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.A.; Finch, C.F.; Hägglund, M.; Junge, A.; Kemp, S.; Khan, K.M.; et al. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS)). Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, R.Ø.; Shrier, I.; Casals, M.; Nettel-Aguirre, A.; Møller, M.; Bolling, C.; Bittencourt, N.F.N.; Clarsen, B.; Wedderkopp, N.; Soligard, T.; et al. Statement on Methods in Sport Injury Research from the First METHODS MATTER Meeting, Copenhagen, 2019. J. Orthop. Sports Phys. Ther. 2020, 50, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Daily, J.P.; Stumbo, J.R. Female Athlete Triad. Prim. Care 2018, 45, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Loveless, M.B. Female athlete triad. Curr. Opin. Obs. Gynecol. 2017, 29, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Saremi, H.; Yavarikia, A.; Jafari, N. Generalized Ligamentous Laxity: An Important Predisposing Factor for Shoulder Injuries in Athletes. Iran Red Crescent Med. J. 2016, 18, e38903. [Google Scholar] [CrossRef] [Green Version]
- Faryniarz, D.A.; Bhargava, M.; Lajam, C.; Attia, E.T.; Hannafin, J.A. Quantitation of estrogen receptors and relaxin binding in human anterior cruciate ligament fibroblasts. In Vitro Cell Dev. Biol. Anim. 2006, 42, 176–181. [Google Scholar] [CrossRef]
- Verhagen, E. Sports Injury Research; Van Mechelen, W., Ed.; Oxford University Press: Oxford, UK; New York, NY, USA, 2010. [Google Scholar]
- Wilroy, J.; Hibberd, E. Evaluation of a Shoulder Injury Prevention Program in Wheelchair Basketball. J. Sport Rehabil. 2018, 27, 554–559. [Google Scholar] [CrossRef]
- Morriën, F.; Taylor, M.J.D.; Hettinga, F.J. Biomechanics in Paralympics: Implications for Performance. Int. J. Sports Physiol. Perform. 2017, 12, 578–589. [Google Scholar] [CrossRef] [Green Version]
- Vanlandewijck, Y.; Theisen, D.; Daly, D. Wheelchair propulsion biomechanics: Implications for wheelchair sports. Sports Med. 2001, 31, 339–367. [Google Scholar] [CrossRef]
- Cuéllar, R.; Ruiz-Ibán, M.A.; Cuéllar, A. Anatomy and Biomechanics of the Unstable Shoulder. Open Orthop. J. 2017, 11, 919–933. [Google Scholar] [CrossRef]
- Edmonds, E.W.; Hopsital, R.C.; Diego, S. Common Conditions in the Overhead Athlete. Am. Fam. Physician 2014, 89, 5. [Google Scholar]
- Morrow, M.M.B.; Kaufman, K.R.; An, K.-N. Scapula Kinematics and Associated Impingement Risk in Manual Wheelchair Users During Propulsion and a Weight Relief Lift. Clin. Biomech. 2011, 26, 352–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, K.W.; Hearns, K.A.; Carlson, M.G. Return to Play after Forearm and Hand Injuries in the National Basketball Association. Orthop. J. Sports Med. 2017, 5, 2325967117690002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, M.W.; Kontos, A.P.; Okonkwo, D.O.; Almquist, J.; Bailes, J.; Barisa, M.; Bazarian, J.; Bloom, O.J.; Brody, D.L.; Cantu, R.; et al. Concussion is Treatable: Statements of Agreement from the Targeted Evaluation and Active Management (TEAM) Approaches to Treating Concussion Meeting held in Pittsburgh, October 15–16, 2015. Neurosurgery 2016, 79, 912–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCrory, P.; Meeuwisse, W.; Dvorak, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [PubMed] [Green Version]
- Weiler, R.; Blauwet, C.; Clarke, D.; Dalton, K.; Derman, W.; Fagher, K.; Gouttebarge, V.; Kissick, J.; Lee, K.; Lexell, J.; et al. Concussion in para sport: The first position statement of the Concussion in Para Sport (CIPS) Group. Br. J. Sports Med. 2021, 55, 1187–1195. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Seco, J.; Royuela, A.; Barriga, A.; Zamora, J. Prevalence and factors associated with a higher risk of neck and back pain among permanent wheelchair users: A cross-sectional study. Spinal. Cord. 2018, 56, 392–405. [Google Scholar] [CrossRef] [Green Version]
- Li, C.-T.; Chen, Y.-N.; Chang, C.-H.; Tsai, K.-H. The Effects of Backward Adjustable Thoracic Support in Wheelchair on Spinal Curvature and Back Muscle Activation for Elderly People. PLoS ONE 2014, 9, e113644. [Google Scholar] [CrossRef]
- Silva, M.E.; Passos, M. Protocolo de Lesão Esportiva no Esporte Paralímpico (PLEEP): Proposta Para a Coleta de Dados. Sports Injuries Protocol for Paralympic Sport: Proposal for Data Acquisition. 2013. Available online: http://repositorio.unicamp.br/acervo/detalhe/917378?guid=1652035045095&returnUrl=%2fresultado%2flistar%3fguid%3d1652035045095%26quantidadePaginas%3d1%26codigoRegistro%3d917378%23917378&i=1 (accessed on 17 December 2020).
- Barengo, N.C.; Meneses-Echávez, J.F.; Ramírez-Vélez, R.; Cohen, D.D.; Tovar, G.; Bautista, J.E.C. The impact of the FIFA 11+ training program on injury prevention in football players: A systematic review. Int. J. Environ. Res. Public Health 2014, 11, 11986–12000. [Google Scholar] [CrossRef] [Green Version]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+ Injury Prevention Program Reduce the Incidence of ACL Injury in Male Soccer Players? Clin. Orthop. Relat. Res. 2017, 475, 2447–2455. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Author | Design | Purpose | Definition of Injury | Sample | Number of Injured Athletes | Incidence and Prevalence |
|---|---|---|---|---|---|---|
| Curtis and Black (1999) [13] | Descriptive self-report survey. | To assess activity level, medical history and prevalence and intensity of shoulder and upper extremity pain during functional activities in female wheelchair athletes. | Not reported. | 46 WB female athletes. | 33 athletes. | 14% of the subjects reported shoulder pain prior to wheelchair use. 72% of the subjects reported shoulder pain since wheelchair use. 52% reported current shoulder pain. |
| Rocco and Saito (2006) [14] | Cross-sectional study. | To identify the most frequent sports injuries of basketball wheelchair players. | “contusion (injury caused by a direct trauma on the body leading to internal involvement); muscular rupture (solution of muscle continuity); muscle stretching (micro-lesion due to excessive stretching of the muscle); muscular cramps (muscular contractions in which the athlete cannot relax the muscle voluntarily); sprains (abrupt movement beyond the normal amplitude); joint dislocation (loss of joint congruence); fracture (solution of bone continuity), tendonitis and bursitis, among others.” | 26 male WB athletes | 20 athletes | 54% of athletes reported pain and 79% localized in the upper limbs. |
| Wessels et al. (2012) [15] | Survey. | To estimate the incidence rate of WB concussion. | “Concussions are a mild traumatic brain injury (mTBI) seen in athletic participation.” | 263 WB players (188 male and 75 female). | 50 athletes affected in the current or previous season. | 6.1% reported experiencing a concussion during the publication year season |
| Mutsuzaki et al. (2014) [16] | Cross-sectional study. | To use ultrasound to investigate tissue injuries in male WB players and determine factors associated with injuries. | “Deep tissue injury is defined as injury to soft tissue resulting from pressure and/or shear.” | 20 WB male athletes. | 9 athletes. | 45% of players had low-echoic lesions |
| Shimizu et al. (2017) [17] | Cross-sectional study. | To investigate deep tissue injuries (DTIs) in elite WB players and identify factors associated with their occurrence. | “Deep tissue injury was defined as a purple or maroon localized area of discoloured intact skin or a blood-filled blister due to damage to the underlying soft tissue from pressure and/or shear forces.” | 22 female WB athletes. | 15 athletes. | 68.2% of players reported DTIs |
| Huzmeli et al. (2017) [18] | Cross-sectional study. | To determine the prevalence and nature of injuries in wheelchair sports participants. | Not reported. | 15 WB athletes (14 male and 1 female). | 4 athletes in the last 12 months. | 26.6% of individuals had injuries in the past one year and 75% of them had injuries because of muscle tear. |
| Soo Hoo et al. (2018) [19] | Descriptive cross-sectional study. | To evaluate the demographics, training regime and injuries suffered by para-athletes participating in sports clubs and to evaluate the type of medical care of athletes and the prevalence of those with spasticity. | “an injury while playing an adaptive sport that required you to sit out of a practice or a game.” | 43 athletes, of which, 25 are WB players (22 male and 3 female). | 11 players in the last 12 months. | In the past 12 months, 39.5% of athletes surveyed sustained an injury. Injury prevalence by sport was 44% in WB. |
| Hollander et al. (2020) [20] | Prospective study |
To assess the rate and characteristics of injuries during the WB World Championships 2018 (WBWC). | “any newly incurred musculoskeletal complaint (traumatic or overuse) and/or concussion during the tournament receiving medical attention regardless of the consequences for participation.” | 336 players (male: 192; female: 144) | 132 players | 75.8 per 100 players (95% CI: 60.9–90.7) or 68.9 per 1000 player-days (55.4–82.4). |
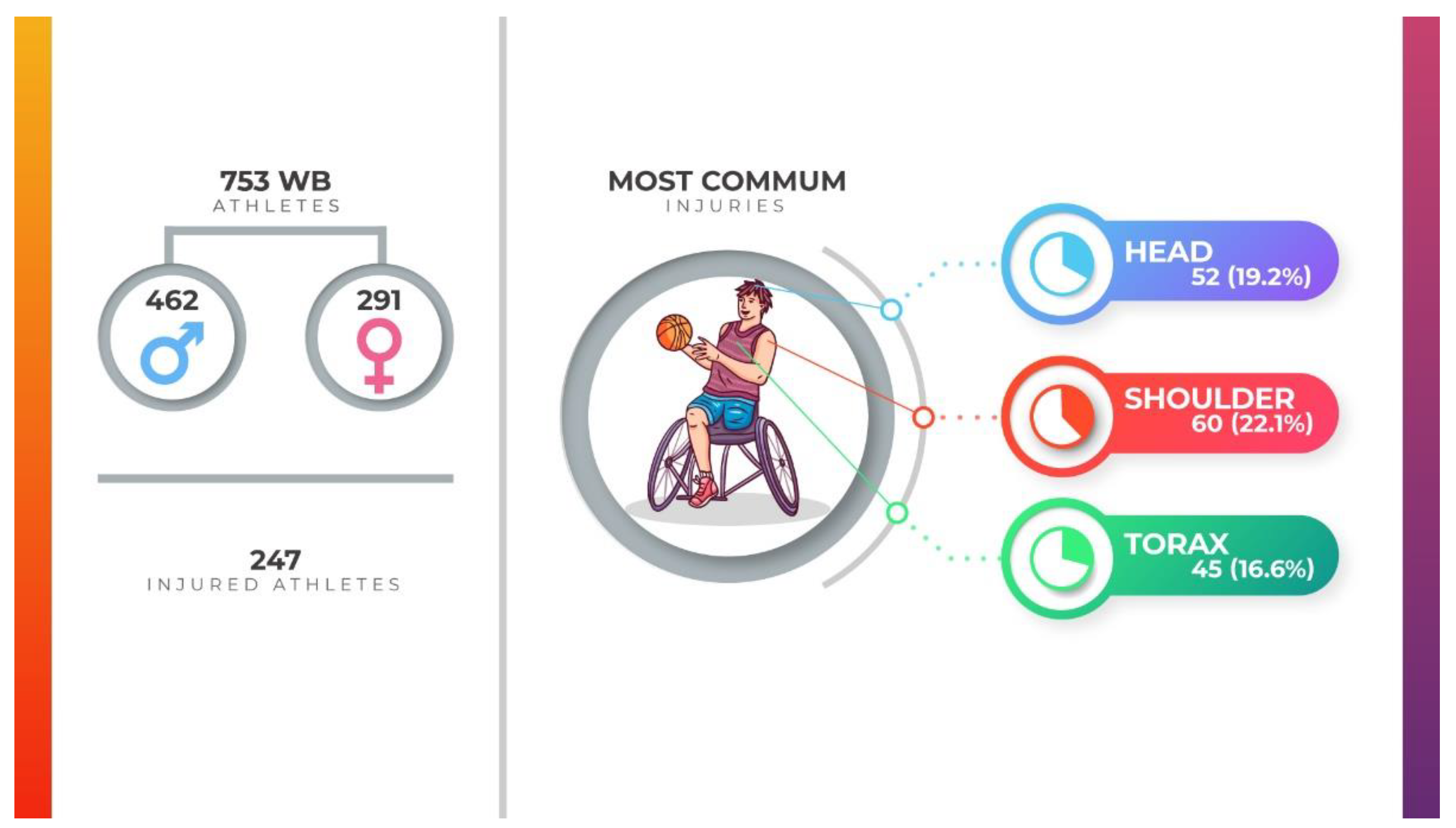
| Body Regions | Number of Injuries (%) | Studies |
| Shoulder | 60 (22.2%) | [13,14,18,19,20] |
| Spine (cervical/thoracic/lumbar) | 45 (16.6%) | [14,18,19,20] |
| Head | 52 (19.2%) | [15,19,20] |
| Wrist | 17 (6.3%) | [14,19,20] |
| Elbow | 18 (6.6%) | [19,20] |
| Sacrum | 21 (7.7%) | [16,19,20] |
| Arm | 11 (4.1%) | [14,18,20] |
| Ischiatic region | 15 (5.5%) | [16,17] |
| Hand/fingers | 19 (7.0%) | [14,18,19,20] |
| Forearm | 3 (1.1%) | [18] |
| Knee | 4 (1.5%) | [18,19,20] |
| Face | 1 (0.4%) | [19] |
| Ribs | 1 (0.4%) | [19] |
| Abdomen | 2 (0.7%) | [20] |
| Thigh | 2 (0.7%) | [20] |
| Body Segments | Number of Injuries (%) | Studies |
| Upper limb | 128 (47.2%) | [13,14,18,19] |
| Trunk (spine and ribs included) | 48 (17.8%) | [14,18,19] |
| Lower limbs | 42 (15.5%) | [16,17,18,19] |
| Head and/or face | 53 (19.5%) | [15,19] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sá, K.; Costa e Silva, A.; Gorla, J.; Silva, A.; Magno e Silva, M. Injuries in Wheelchair Basketball Players: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 5869. https://doi.org/10.3390/ijerph19105869
Sá K, Costa e Silva A, Gorla J, Silva A, Magno e Silva M. Injuries in Wheelchair Basketball Players: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(10):5869. https://doi.org/10.3390/ijerph19105869
Chicago/Turabian StyleSá, Karina, Anselmo Costa e Silva, José Gorla, Andressa Silva, and Marília Magno e Silva. 2022. "Injuries in Wheelchair Basketball Players: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 10: 5869. https://doi.org/10.3390/ijerph19105869
APA StyleSá, K., Costa e Silva, A., Gorla, J., Silva, A., & Magno e Silva, M. (2022). Injuries in Wheelchair Basketball Players: A Systematic Review. International Journal of Environmental Research and Public Health, 19(10), 5869. https://doi.org/10.3390/ijerph19105869