
Prevalence and Correlates of Intimate Partner Violence among Women Attending Different Primary Health Centers in Aljouf Region, Saudi Arabia

 , ,
, ,
Abstract
:1. Introduction
2. Participants and Methodology
2.1. Study Design and Setting
2.2. Sample Size Estimation
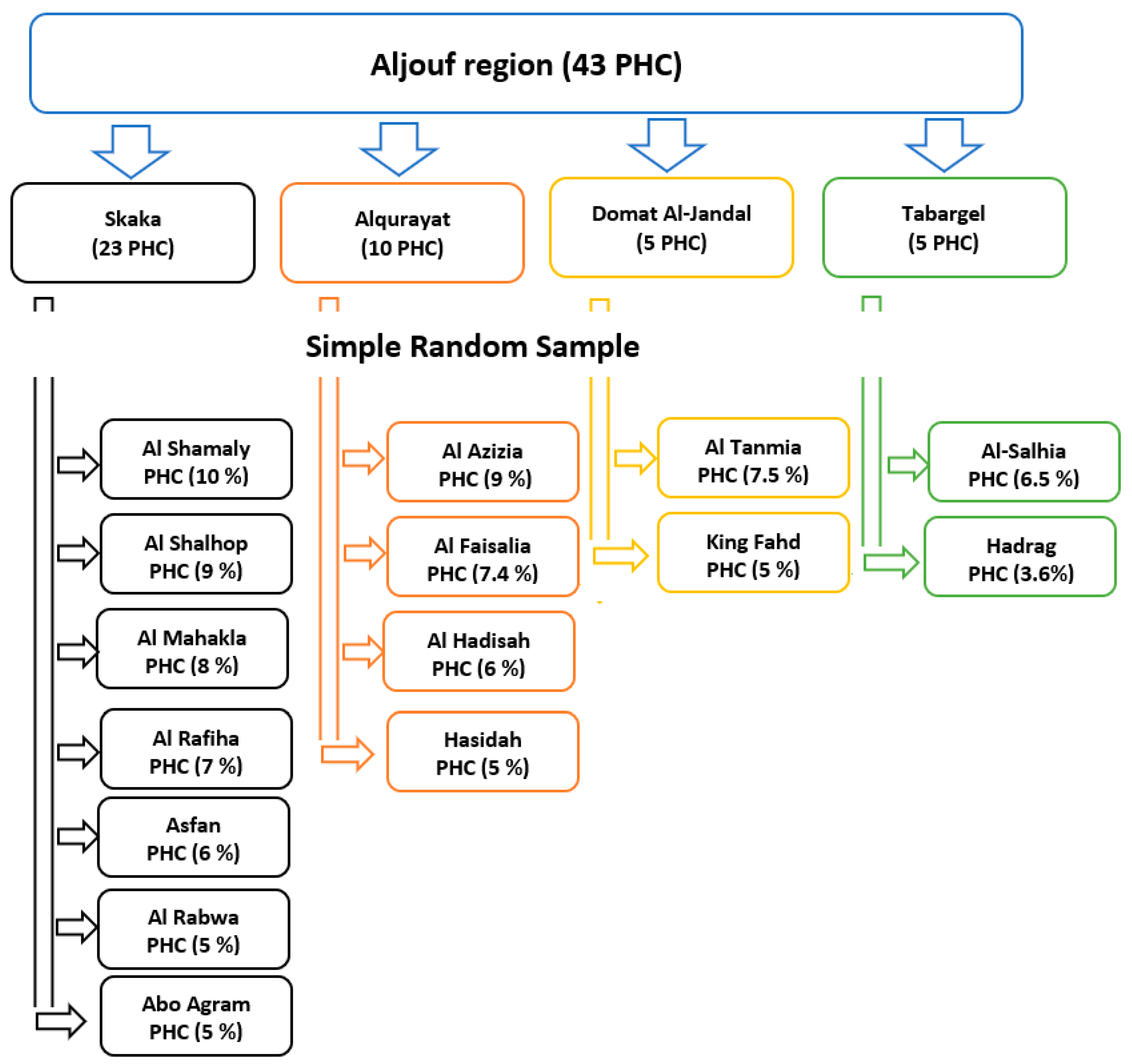
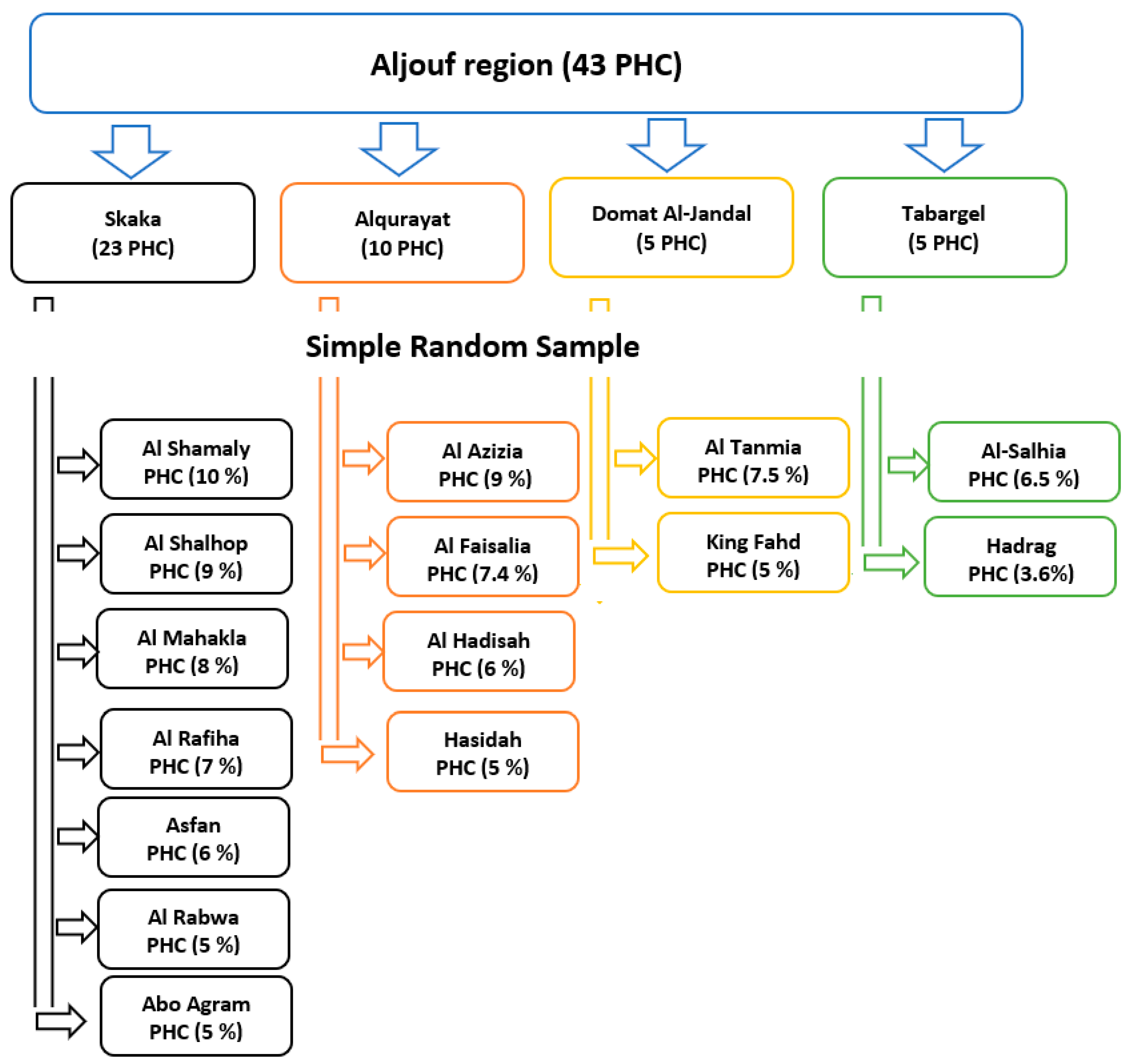
2.3. Sampling Technique
2.4. Inclusion and Exclusion Criteria
2.5. Data Collection Tool
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Violence against Women Prevalence Estimates. 2021. Available online: https://www.who.int/publications/i/item/9789240022256 (accessed on 24 November 2021).
- United Nations. United Nations General Assembly, 61st Session—Intensification of Efforts to Eliminate All Forms of Violence against Women. 2006. Available online: https://www.un.org/womenwatch/daw/documents/ga61.htm (accessed on 24 November 2021).
- World Health Organization. Violence against Women: Domestic and Sexual Violence against Women (Fact Sheet No. 239). 2013. Available online: http://www.who.int/mediacentre/factsheets/fs239/en/ (accessed on 24 November 2021).
- Elghossain, T.; Bott, S.; Akik, C.; Obermeyer, C.M. Prevalence of intimate partner violence against women in the Arab world: A systematic review. BMC Int. Health Hum. Rights 2019, 19, 29. [Google Scholar] [CrossRef]
- World Health Organization. Responding to Intimate Partner Violence and Sexual Violence against Women, WHO Clinical and Policy Guidelines. 2013. Available online: https://www.who.int/reproductivehealth/publications/violence/9789241548595/en/ (accessed on 24 November 2021).
- Yount, K.M. Resources, Family Organization, and Domestic Violence against Married Women in Minya, Egypt. J. Marriage Fam. 2005, 67, 579–596. [Google Scholar] [CrossRef]
- Douki, S.; Nacef, F.; Belhadj, A.; Bouasker, A.; Ghachem, R. Violence against women in Arab and Islamic countries. Arch. Women’s Ment. Health 2003, 6, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Wali, R.; Khalil, A.; Alattas, R.; Foudah, R.; Meftah, I.; Sarhan, S. Prevalence and risk factors of domestic violence in women attending the National Guard Primary Health Care Centers in the Western Region, Saudi Arabia, 2018. BMC Public Health 2020, 20, 239. [Google Scholar] [CrossRef] [PubMed]
- Fageeh, W.M.K. Factors associated with domestic violence: A cross-sectional survey among women in Jeddah, Saudi Arabia. BMJ Open 2014, 4, e004242. [Google Scholar] [CrossRef] [Green Version]
- Barnawi, F.H. Prevalence and Risk Factors of Domestic Violence against Women Attending a Primary Care Center in Riyadh, Saudi Arabia. J. Interpers. Violence 2017, 32, 1171–1186. [Google Scholar] [CrossRef]
- Alzahrani, T.A.; Abaalkhail, B.A.; Ramadan, I.K. Prevalence of intimate partner violence and its associated risk factors among Saudi female patients attending the primary healthcare centers in Western Saudi Arabia. Saudi Med J. 2016, 37, 96–99. [Google Scholar] [CrossRef]
- Afifi, Z.E.M.; Al-Muhaideb, N.S.; Hadish, N.F.; I Ismail, F.; Al-Qeamy, F.M. Domestic violence and its impact on married women’s health in Eastern Saudi Arabia. Saudi Med. J. 2011, 32, 612–620. [Google Scholar]
- Breiding, M.; Basile, K.C.; Smith, S.G.; Black, M.C.; Mahendra, R.R. Intimate Partner Violence Surveillance: Uniform Definitions and Recommended Data Elements, Version 2.0; Centers for Disease Control and Prevention, National Center for Injury Prevention and Control: Atlanta, GA, USA, 2015. Available online: https://stacks.cdc.gov/view/cdc/31292 (accessed on 24 November 2021).
- United States Department of Justice. Domestic Violence. Office on Violence against Women. 2014. Available online: https://www.justice.gov/ovw/domestic-violence (accessed on 24 November 2021).
- Haddad, L.G.; Shotar, A.; Younger, J.B.; Alzyoud, S.; Bouhaidar, C.M. Screening for domestic violence in Jordan: Validation of an Arabic version of a domestic violence against women questionnaire. Int. J. Women’s Health 2011, 3, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Aljuhani, S.; Alateeq, M. Intimate partner violence in Saudi Arabia: A topic of growing interest. J. Fam. Med. Prim. Care 2020, 9, 481–484. [Google Scholar] [CrossRef]
- Abrahams, N.; Jewkes, R. Effects of South African Men’s Having Witnessed Abuse of Their Mothers During Childhood on Their Levels of Violence in Adulthood. Am. J. Public Health 2005, 95, 1811–1816. [Google Scholar] [CrossRef]
- Al Kendi, A.; Al Shidhan, N.; Al Kiyumi, M. Domestic violence among Omani women: Prevalence, risk factors and help-seeking behaviour. East. Mediterr. Health J. 2021, 27, 242–249. [Google Scholar] [CrossRef]
- Halawi, A.A.A.; Almalki, Z.A.A.; Alsadah, A.; Aseeri, A.A.S.; Jabri, S.A.H.; Alasmri, B.S.; Altuwajiri, A.A.S.; Al-Hussan, T.H.; AlHawaj, F.A. Prevalence and Risk Factors for Abuse among Saudi Females, KSA. Egypt. J. Hosp. Med. 2017, 68, 1082–1087. [Google Scholar] [CrossRef]
- Tesfa, A.; Dida, N.; Girma, T.; Aboma, M. Intimate Partner Violence, Its Sociocultural Practice, and Its Associated Factors Among Women in Central Ethiopia. Risk Manag. Healthc. Policy 2020, 13, 2251–2259. [Google Scholar] [CrossRef] [PubMed]
- Al-Atrushi, H.H.; Al-Tawil, N.G.; Shabila, N.P.; Al-Hadithi, T.S. Intimate partner violence against women in the Erbil city of the Kurdistan region, Iraq. BMC Women’s Health 2013, 13, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossen, M.A. Measuring Gender-Based Violence: Results of the Violence against Women (VAW) Survey in Bangladesh; Bangladesh Bureau of Statistics (BBS), Ministry of Planning: Dhaka, Bangladesh, 2014.
- Ahmed, A.M.; E Elmardi, A. A study of domestic violence among women attending a medical centre in Sudan. East. Mediterr. Health J. 2006, 11, 164–174. [Google Scholar]
- Xu, X.; Zhu, F.; O’Campo, P.; Koenig, M.A.; Mock, V.; Campbell, J. Prevalence of and Risk Factors for Intimate Partner Violence in China. Am. J. Public Health 2005, 95, 78–85. [Google Scholar] [CrossRef]
- Boy, A.; Kulczycki, A. What We Know About Intimate Partner Violence in the Middle East and North Africa. Violence Women 2008, 14, 53–70. [Google Scholar] [CrossRef]
- Moazen, B.; Salehi, A.; Soroush, M.; Vardanjani, H.M.; Zarrinhaghighi, A. Domestic violence against women in Shiraz, South-western Iran. J. Inj. Violence Res. 2019, 11, 243–254. [Google Scholar] [CrossRef]
- Wmk, F. Domestic Violence among Women in Jeddah. J. Women’s Health Care 2017, 6, 354. [Google Scholar] [CrossRef] [Green Version]
- Murphy, C.M.; O’Leary, K.D. Psychological aggression predicts physical aggression in early marriage. J. Consult. Clin. Psychol. 1989, 57, 579–582. [Google Scholar] [CrossRef]
- Gubi, D.; Nansubuga, E.; Wandera, S.O. Correlates of intimate partner violence among married women in Uganda: A cross-sectional survey. BMC Public Health 2020, 20, 1008. [Google Scholar] [CrossRef]
- Cwikel, J.; Lev-Wiesel, R.; Al-Krenawi, A. The Physical and Psychosocial Health of Bedouin Arab Women of the Negev Area of Israel: The Impact of High Fertility and Pervasive Domestic Violence. Violence Women 2003, 9, 240–257. [Google Scholar] [CrossRef]
- Al-Badayneh, D.M. Violence against Women in Jordan. J. Fam. Violence 2012, 27, 369–379. [Google Scholar] [CrossRef]
- Karadsheh, M.; Al-Khatatneh, A.K. The impact of demographic and social variables on forms of violence against women in Jordan. J. Soc. Sci. 2007, 35, 109–158. [Google Scholar]
- Maziak, W.; Asfar, T. Physical abuse in low-income women in Aleppo, Syria. Health Care Women Int. 2003, 24, 313–326. [Google Scholar] [CrossRef]
- Shiraz, M.S. The impact of education and occupation on domestic violence in Saudi Arabia. Int. J. Soc. Welf. 2016, 25, 339–346. [Google Scholar] [CrossRef]
- Motsa, N.D.; Morojele, P.J. Vulnerable masculinities: Implications of gender socialisation in three rural Swazi primary schools. S. Afr. J. Child. Educ. 2019, 9, 11. [Google Scholar] [CrossRef]
- Shetty, S.M.; Kundapur, R.; Kempaller, V.J.; Kumar, A.; Anurupa, M. Violence against educated women by intimate partners in Urban Karnataka, India. Indian J. Community Med. 2017, 42, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Krug, E.G.; A Mercy, J.; Dahlberg, L.L.; Zwi, A. The world report on violence and health. Lancet 2002, 360, 1083–1088. [Google Scholar] [CrossRef] [Green Version]
- Izugbara, C.O.; Obiyan, M.; Degfie, T.T.; Bhatti, A. Correlates of intimate partner violence among urban women in sub-Saharan Africa. PLoS ONE 2020, 15, e0230508. [Google Scholar] [CrossRef] [Green Version]
- Fahmy, H.H.; El-Rahman, S.I.A. Determinants and health consequences of domestic violence among women in reproductive age at zagazig district, egypt. J. Egypt. Public Health Assoc. 2008, 83, 87–106. [Google Scholar]
- Mamdouh, H.; Ismail, H.; Kharboush, I.; Tawfik, M.; El Sharkawy, O.; Abdel-Baky, M.; Sallam, H. Prevalence and risk factors for spousal violence among women attending health care centres in Alexandria, Egypt. East. Mediterr. Health J. 2012, 18, 1118–1126. [Google Scholar] [CrossRef]
- Urquia, M.L.; O’Campo, P.J.; Ray, J.G. Marital Status, Duration of Cohabitation, and Psychosocial Well-Being Among Childbearing Women: A Canadian Nationwide Survey. Am. J. Public Health 2013, 103, e8–e15. [Google Scholar] [CrossRef]
- Umubyeyi, A.; Mogren, I.; Ntaganira, J.; Krantz, G. Women are considerably more exposed to intimate partner violence than men in Rwanda: Results from a population-based, cross-sectional study. BMC Women’s Health 2014, 14, 99. [Google Scholar] [CrossRef]
- Sapkota, D.; Bhattarai, S.; Baral, D.; Pokharel, P.K. Domestic violence and its associated factors among married women of a village development committee of rural Nepal. BMC Res. Notes 2016, 9, 178. [Google Scholar] [CrossRef] [Green Version]
- Almosaed, N.; Alazab, S.A. Why stay? Saudi women’s adaptions to violence. Int. J. Humanit. Soc. Sci. 2015, 10, 146–162. [Google Scholar]
- Gokler, M.E.; Arslantas, D.; Ünsal, A. Prevalence of domestic violence and associated factors among married women in a semi-rural area of western Turkey. Pak. J. Med. Sci. 1969, 30, 1088–1093. [Google Scholar] [CrossRef] [PubMed]
- Kury, H.; Obergfell-Fuchs, J.; Woessner, G. The Extent of Family Violence in Europe. Violence Women 2004, 10, 749–769. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variable | No. (%) |
|---|---|
| Exposure to IPV | |
| Yes | 122 (30.3%) |
| No | 281 (69.7%) |
| Types of IPV 1 | |
| Emotional | 113 (92.6%) |
| Physical | 82 (67.2%) |
| Sexual | 54 (44.3%) |
| Sociodemographic Features | Exposure to IPV | p-Value | ||
|---|---|---|---|---|
| Total | Exposed (n = 122) No. (%) | Non-Exposed (n = 281) No. (%) | ||
| Age | p < 0.001 | |||
| ≤20 | 33 (8.2%) | 9 (7.4%) | 24 (8.5%) | |
| 21–30 | 189 (46.9%) | 33 (27.0%) | 156 (55.5%) | |
| 31–40 | 87 (21.6%) | 36 (29.5%) | 51 (18.1%) | |
| ≥41 | 94 (23.3%) | 44 (36.1%) | 50 (17.8%) | |
| Mean ± SD | 32.73 ± 2.12 | |||
| Marital status | p < 0.001 | |||
| Married | 368 (91.3%) | 98 (80.3%) | 270 (96.1%) | |
| Divorced/widowed | 35 (8.7%) | 24 (19.7%) | 11 (3.9%) | |
| Educational level | 0.007 | |||
| Illiterate | 7 (1.8%) | 5 (4.1%) | 2 (0.7%) | |
| Primary/preparatory | 11 (2.7%) | 7 (5.7%) | 4 (1.4%) | |
| Secondary/diploma | 81(20.1%) | 22 (18.0%) | 59 (21.0%) | |
| University/postgraduate | 304 (75.4%) | 88 (72.1%) | 216 (76.9%) | |
| Employment | 0.192 | |||
| Employed | 185 (45.9%) | 62 (50.8%) | 123 (43.8%) | |
| Unemployed | 218 (54.1%) | 60 (49.2%) | 158 (56.2%) | |
| Monthly income | p < 0.001 | |||
| <5000 RS 1 | 86 (21.3%) | 30 (24.6%) | 56 (19.9%) | |
| 5000–7000 RS | 80 (19.9%) | 9 (7.4%) | 71 (25.3%) | |
| >7000 RS | 237 (58.8%) | 83 (68.0%) | 154 (54.8%) | |
| Monthly income sufficient | p < 0.001 | |||
| Yes | 279 (69.2%) | 67 (54.9%) | 212 (75.4%) | |
| No | 124 (30.8%) | 55 (45.1%) | 69 (24.6%) | |
| Age at marriage | 0.192 | |||
| <20 | 88 (21.8%) | 37 (30.3%) | 51(18.1%) | |
| ≥20 | 315 (78.2%) | 85 (69.7%) | 230 (81.9%) | |
| Mean ± SD | 22.39 ± 4.38 | |||
| Marriage duration | p < 0.001 | |||
| 0–5 years | 168 (41.7%) | 34 (27.9%) | 134 (47.7%) | |
| 6–10 years | 55 (13.6%) | 13 (10.7%) | 42 (14.9%) | |
| >10 years | 180 (44.7%) | 75 (61.5%) | 105 (37.4%) | |
| Having children | p < 0.001 | |||
| Yes | 319 (79.2%) | 110 (90.2%) | 209 (74.4%) | |
| No | 84 (20.8 %) | 12 (9.8%) | 72 (25.6%) | |
| Number of children | 0.008 | |||
| 1–3 | 169 (41.9%) | 47 (42.7%) | 122 (58.4%) | |
| ≥4 | 150 (37.2%) | 63 (57.3%) | 87 (41.6%) | |
| Residence | 0.455 | |||
| House of husband | 349 (86.6%) | 108 (88.5%) | 241(85.8%) | |
| House of Husband’s family | 54 (13.4%) | 14 (11.5%) | 40 (14.2%) | |
| Relative relationship with your husband | 0.198 | |||
| Yes | 168 (41.7%) | 45 (36.9%) | 123 (43.8%) | |
| No | 235 (58.3%) | 77 (63.1%) | 158 (56.2%) | |
| Approval on marriage was taken | p < 0.001 | |||
| Yes | 61 (15.1%) | 40 (32.8%) | 21 (7.5%) | |
| No | 342 (84.9%) | 82 (67.2%) | 260 (92.5%) | |
| The age difference between you and your husband | 0.015 | |||
| No difference | 54 (13.4%) | 8 (6.5%) | 46 (16.4%) | |
| 1–10 years | 315 (78.2%) | 100 (82.0%) | 215 (76.5%) | |
| >10 years | 34 (8.4%) | 14 (11.5%) | 20 (7.1%) | |
| Husbands’ Characteristics | Exposure to IPV | p-Value | ||
|---|---|---|---|---|
| Total | Exposed (n = 122) No. (%) | Non-Exposed (n = 281) No. (%) | ||
| Husband education | 0.309 | |||
| Illiterate | 6 (1.5%) | 3 (2.4%) | 3 (1.1%) | |
| Primary/preparatory | 25 (6.2%) | 10 (8.2%) | 15 (5.3%) | |
| Secondary/diploma | 100 (24.8%) | 25 (20.5%) | 75 (26.7%) | |
| University/postgraduate | 272 (67.5%) | 84 (68.9%) | 188 (66.9%) | |
| Husband Employment | 0.082 | |||
| Working | 322 (79.9%) | 94 (77.0%) | 228 (81.1%) | |
| No working | 29 (7.2%) | 6 (4.9%) | 23 (8.2%) | |
| Retired | 52 (12.9%) | 22 (18.1%) | 30 (10.7%) | |
| Job type | 0.427 | |||
| Civil | 266 (66.0%) | 84 (68.9%) | 182 (64.8%) | |
| Military | 137 (34.0%) | 38 (31.1%) | 99 (35.2%) | |
| Smoking status | p < 0.001 | |||
| Yes | 173 (42.9%) | 73 (59.8%) | 100 (35.6%) | |
| No | 230 (57.1%) | 49 (40.2%) | 181(64.4%) | |
| Aggressive behavior | p < 0.001 | |||
| Yes | 109 (27.0%) | 97 (79.5%) | 12 (4.3%) | |
| No | 294 (73.0%) | 25 (20.5%) | 269 (95.7%) | |
| Alcohol drinking | p < 0.001 | |||
| Yes | 27 (6.7%) | 22 (18.0%) | 5 (1.8%) | |
| No | 376 (93.3%) | 100 (82.0%) | 276 (98.2%) | |
| Drug abuse | p < 0.001 | |||
| Yes | 24 (6.0%) | 20 (16.4%) | 4 (1.4%) | |
| No | 379 (94.0%) | 102 (83.6%) | 277 (98.6%) | |
| Adjusted Regression Model | ||||
|---|---|---|---|---|
| OR | 95% C.I. | p-Value | ||
| Upper | Lower | |||
| Women age (in years) | 1.005 | 0.948 | 1.065 | 0.873 |
| Marital status (Married) | Reference Group | |||
| Divorced/widowed | 3.345 | 0.823 | 13.587 | 0.091 |
| Women educational level (University/postgraduate) | Reference Group | |||
| Less than university | 1.011 | 0.395 | 2.586 | 0.983 |
| Monthly income > 7000 RS | Reference Group | |||
| ≤7000 RS | 0.431 | 0.163 | 1.137 | 0.089 |
| Monthly income sufficient (Yes) | Reference Group | |||
| No | 1.378 | 0.562 | 3.378 | 0.484 |
| Marriage duration (0–5 years) | Reference Group | |||
| 6–10 years | 0.645 | 0.183 | 2.266 | 0.494 |
| More than 10 years | 0.326 | 0.081 | 1.318 | 0.116 |
| Number of children (No children) | Reference Group | |||
| One to three children | 7.322 | 1.776 | 30.177 | 0.006 |
| Four children or more | 13.463 | 2.126 | 85.256 | 0.006 |
| Approval on marriage was taken (Yes) | Reference Group | |||
| No | 3.190 | 1.042 | 9.767 | 0.042 |
| The age difference between you and your husband (No difference) | Reference group | |||
| 1–10 years | 2.978 | 0.840 | 10.558 | 0.091 |
| More than 10 years | 2.624 | 0.478 | 14.410 | 0.267 |
| Husband smoking status (No) | Reference group | |||
| Yes | 2.774 | 1.246 | 6.175 | 0.012 |
| Husband aggressive behavior (No) | Reference group | |||
| Yes | 98.703 | 37.881 | 257.179 | p < 0.001 |
| Husband alcohol drinking (No) | Reference group | |||
| Yes | 0.108 | 0.013 | 0.904 | 0.040 |
| Husband drug abuse (No) | Reference group | |||
| Yes | 3.589 | 0.445 | 28.929 | 0.230 |
| No. (%) (n = 122) | |
|---|---|
| Causes of IPV as reported by women 1 | |
| Sociocultural effects | 70 (57.4%) |
| Insufficient income | 35 (28.7%) |
| Jealousy | 28 (23.0%) |
| Alcohol abuse | 22 (18 %) |
| Stressors | 21 (17.2%) |
| Drug abuse | 20 (16.4%) |
| Treachery | 20 (16.4%) |
| Frequency of IPV | |
| Once/day | 16 (13.1%) |
| Once/week | 44 (36.1%) |
| Once or more/month | 62 (50.8%) |
| Residual influences of IPV 1 | |
| Psychological problems | 92 (75.4%) |
| Injuries | 52 (42.6%) |
| No effects | 17 (13.9%) |
| Hospital admission | 12 (9.8%) |
| Taking drugs | 12 (9.8%) |
| Medical problems | 3 (2.5%) |
| Reactions to IPV | |
| No reaction | 45 (36.8%) |
| Leave home | 40 (32.8%) |
| Request divorce | 23 (18.9%) |
| Go to doctor | 9 (7.4%) |
| Call police | 5 (4.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdel-Salam, D.M.; ALruwaili, B.; Osman, D.M.; Alazmi, M.M.M.; ALghayyadh, S.A.M.; Al-sharari, R.G.Z.; Mohamed, R.A. Prevalence and Correlates of Intimate Partner Violence among Women Attending Different Primary Health Centers in Aljouf Region, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 598. https://doi.org/10.3390/ijerph19010598
Abdel-Salam DM, ALruwaili B, Osman DM, Alazmi MMM, ALghayyadh SAM, Al-sharari RGZ, Mohamed RA. Prevalence and Correlates of Intimate Partner Violence among Women Attending Different Primary Health Centers in Aljouf Region, Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(1):598. https://doi.org/10.3390/ijerph19010598
Chicago/Turabian StyleAbdel-Salam, Doaa M., Bashayer ALruwaili, Doaa Mohamed Osman, Maha Mamluh M. Alazmi, Sama Ayman Mater ALghayyadh, Rawan Ghazi Zaki Al-sharari, and Rehab A. Mohamed. 2022. "Prevalence and Correlates of Intimate Partner Violence among Women Attending Different Primary Health Centers in Aljouf Region, Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 1: 598. https://doi.org/10.3390/ijerph19010598
APA StyleAbdel-Salam, D. M., ALruwaili, B., Osman, D. M., Alazmi, M. M. M., ALghayyadh, S. A. M., Al-sharari, R. G. Z., & Mohamed, R. A. (2022). Prevalence and Correlates of Intimate Partner Violence among Women Attending Different Primary Health Centers in Aljouf Region, Saudi Arabia. International Journal of Environmental Research and Public Health, 19(1), 598. https://doi.org/10.3390/ijerph19010598