
The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Group
2.2. Procedures
2.2.1. Rolling of the Hamstring
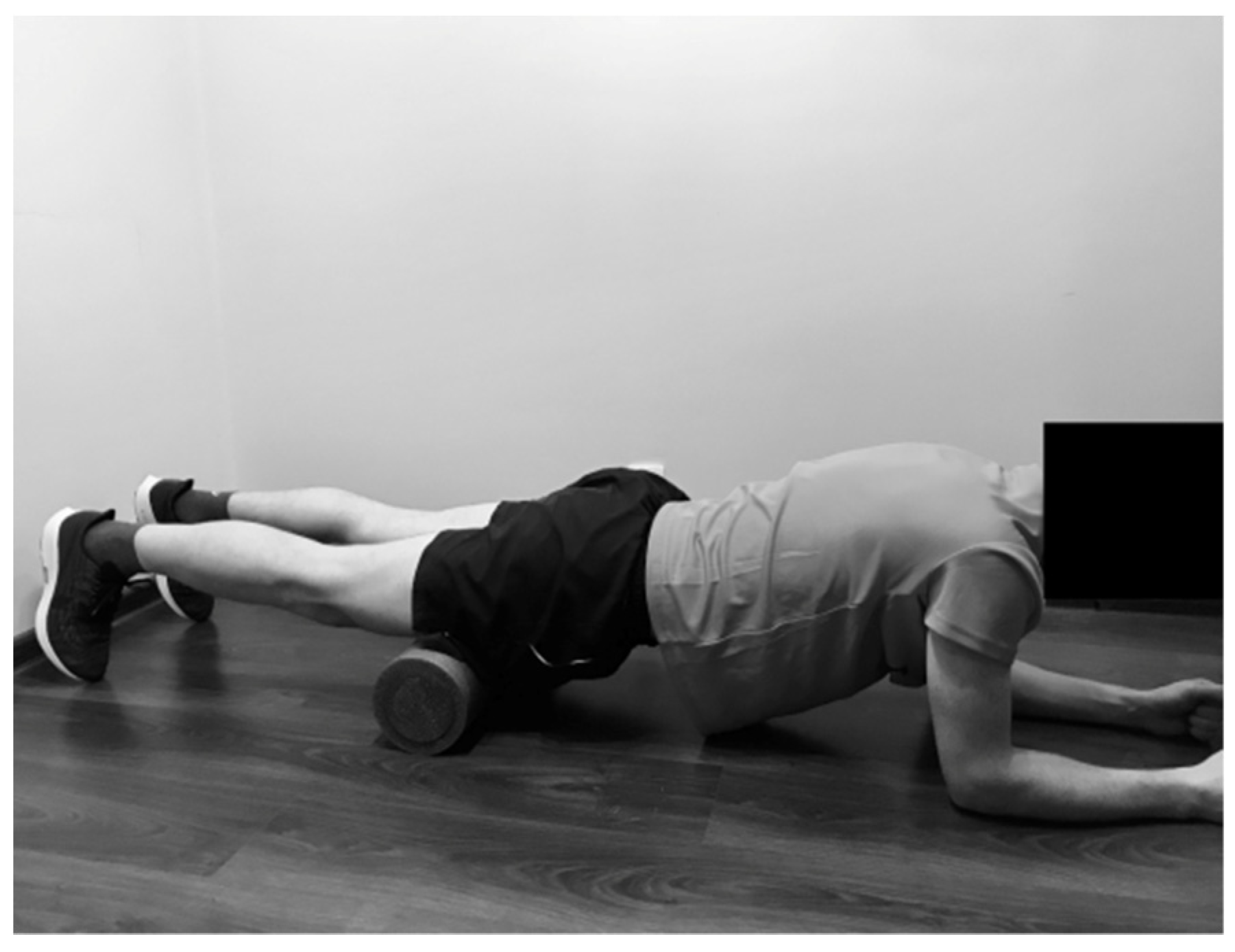
2.2.2. Rolling of the Gastrocnemius
2.2.3. Rolling of the Gluteus Maximus
2.2.4. Rolling of the Hip Adductors
2.2.5. Rolling of the Quadriceps
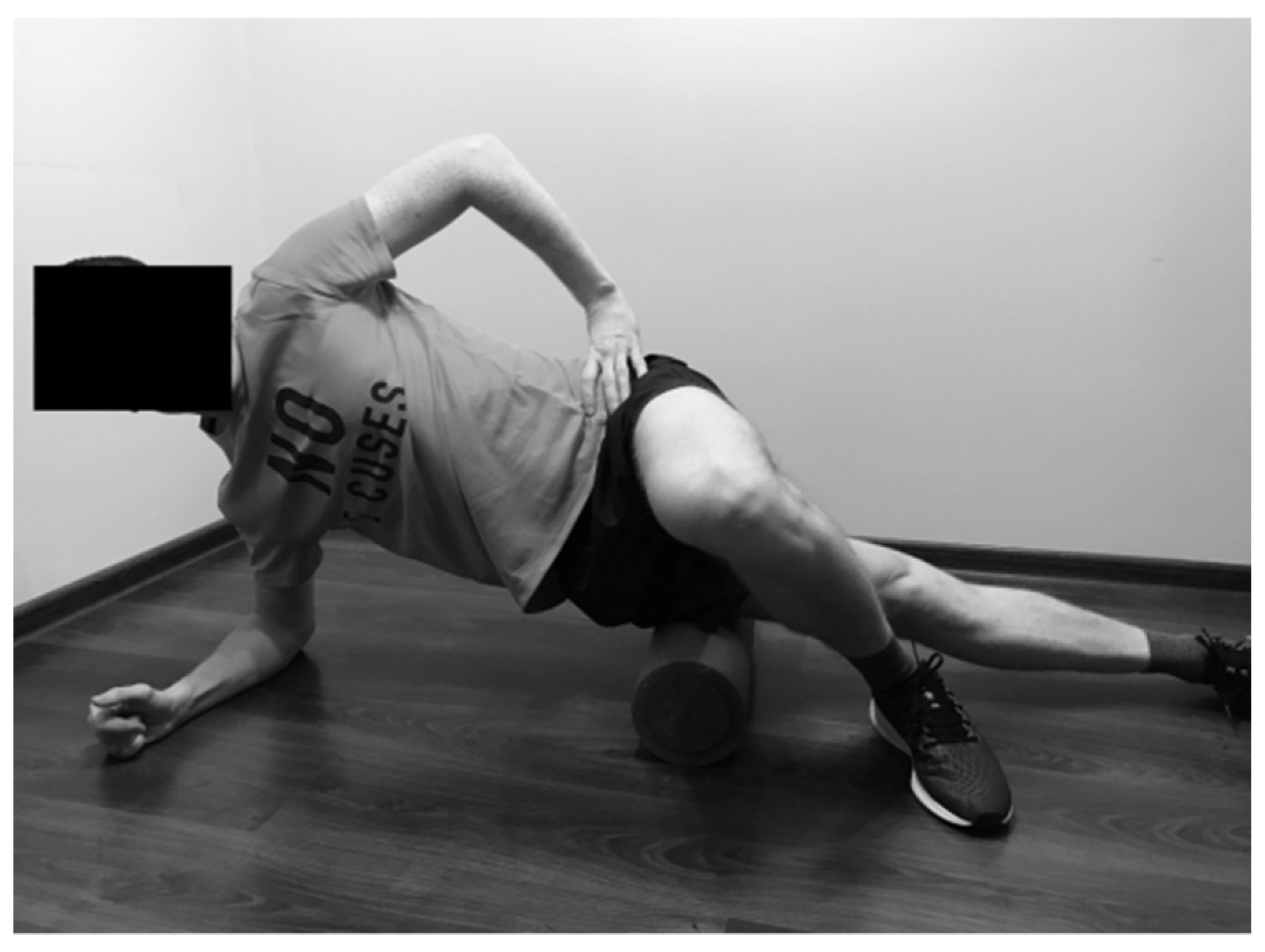
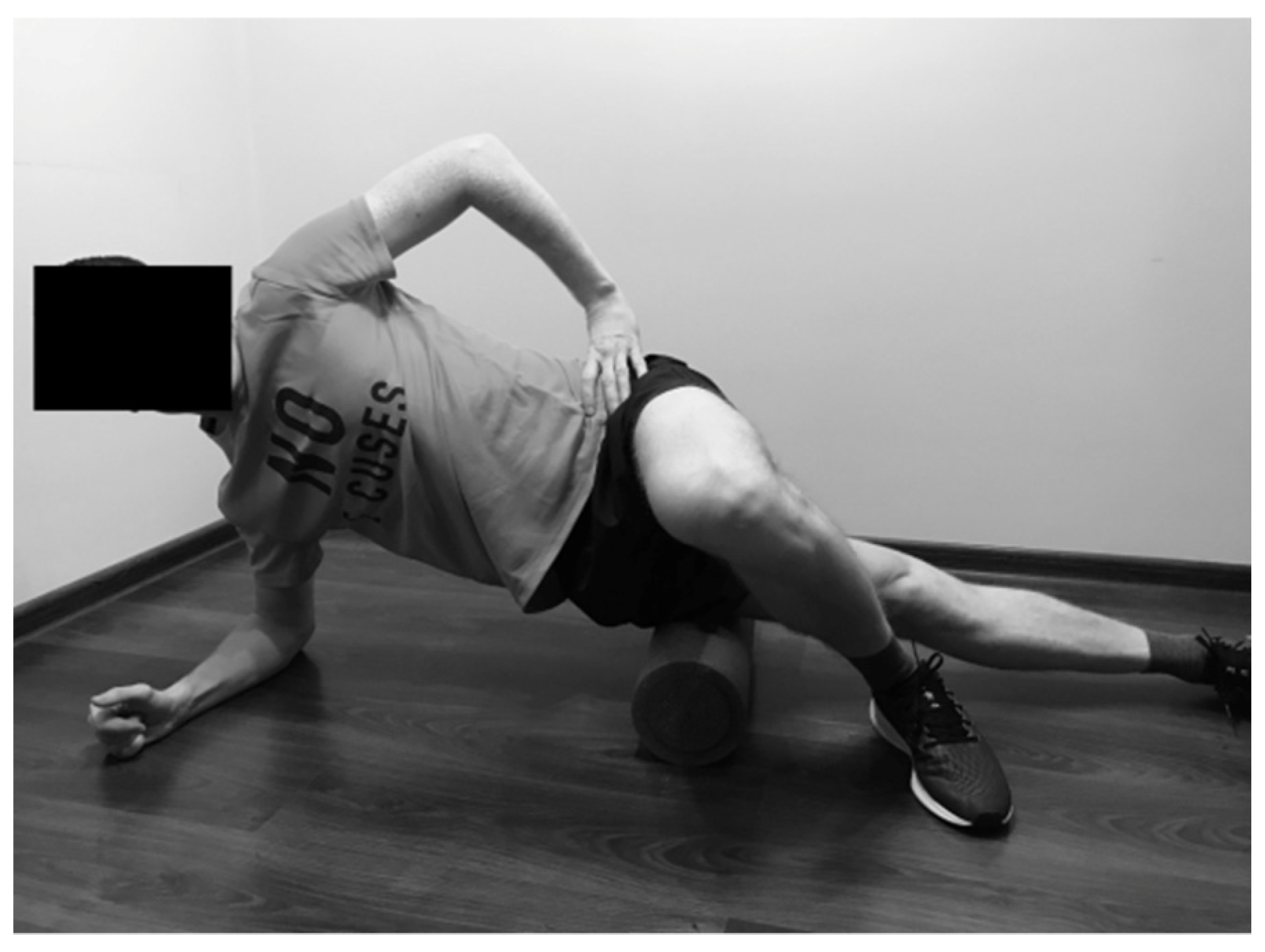
2.2.6. Rolling of the Tensor Fasciae Latae
2.3. Research Tool
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferber, R.; Hreljac, A.; Kendall, K.D. Suspected mechanisms in the cause of overuse running injuries: A clinical review. Sports Health 2009, 1, 242–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taunton, J.E.; Ryan, M.B.; Clement, D.B.; McKenzie, D.C.; Lloyd-Smith, D.R.; Zumbo, B.D. A retrospective case-control analysis of 2002 running injuries. Br. J. Sports Med. 2002, 36, 95–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Gent, R.N.; Siem, D.; van Middelkoop, M.; van Os, A.G.; Bierma-Zeinstra, S.M.; Koes, B.W. Incidence and determinants of lower extremity running injuries in long distance runners: A systematic review. Br. J. Sports Med. 2007, 41, 469–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croisier, J.L.; Forthomme, B.; Namurois, M.H.; Vanderthommen, M.; Crielaard, J.M. Hamstring muscle strain recurrence and strength performance disorders. Am. J. Sports Med. 2002, 30, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Heyward, V.H.; Gibson, A.L. Advanced Fitness Assessment and Exercise Prescription; Human Kinetics: Champaign, IL, USA, 2014. [Google Scholar]
- Thacker, S.B.; Gilchrist, J.; Stroup, D.F.; Kimsey, C.D., Jr. The impact of stretching on sports injury risk: A systematic review of the literature. Med. Sci. Sports Exerc. 2004, 36, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Shivalingaiah, J.; Vernekar, S.; Naik, A.; Goudar, S.S. Effect of training on agility, flexibility, its correlation, and also its correlation with skin fold thickness and body mass index among runners. Natl. J. Physiol. Pharm. Pharmacol. 2016, 6, 505–509. [Google Scholar] [CrossRef]
- Barnes, M.F. The basic science of myofascial release: Morphologic change in connective tissue. J. Bodyw. Mov. Ther. 1997, 1, 231–238. [Google Scholar] [CrossRef]
- Simmonds, N.; Miller, P.; Gemmell, H. A theoretical framework for the role of fascia in manual therapy. J. Bodyw. Mov. Ther. 2012, 16, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Ben David, C. Effect of self-myofascial release on myofascial pain, muscle flexibility, and strength: A narrative review. J. Bodyw. Mov. Ther. 2017, 21, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Riggs, A. Deep Tissue Massage, Revised: A Visual Guide to Technique; North Atlantic Books: Berkeley, CA, USA, 2007. [Google Scholar]
- Sefton, J.M. Myofascial release for athletic trainers, part I: Theory and session guidelines. Athl. Ther. Today 2004, 9, 48–49. [Google Scholar] [CrossRef]
- Couture, G.; Karlik, D.; Glass, S.C.; Hatzel, B.M. The Effect of Foam Rolling Duration on Hamstring Range of Motion. Open Orthop. J. 2015, 9, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weerapong, P.; Hume, P.A.; Kolt, G.S. The mechanisms of massage and effects on performance, muscle recovery and injury prevention. Sports Med. 2005, 35, 235–256. [Google Scholar] [CrossRef] [PubMed]
- Paolini, J. Review of myofascial release as an effective massage therapy technique. Athl. Ther. Today 2009, 14, 30–34. [Google Scholar] [CrossRef]
- MacDonald, G.Z.; Penney, M.D.; Mullaley, M.E.; Cuconato, A.L.; Drake, C.D.; Behm, D.G.; Button, D.C. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J. Strength Cond. Res. 2013, 27, 812–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaitow, L. Research in water and fascia. Micro-tornadoes, hydrogenated diamonds and nanocrystals. Massage Today 2009, 9, 1–3. [Google Scholar]
- Schleip, R.; Findley, T.W.; Chaitow, L.; Huijing, P.A. Fascia: The Tensional Network of the Human Body; Elsevier: London, UK, 2012. [Google Scholar]
- Aguilera, F.J.; Martin, D.P.; Masanet, R.A.; Botella, A.C.; Soler, L.B.; Morell, F.B. Immediate effect of ultrasound and ischemic compression techniques for the treatment of trapezius latent myofascial trigger points in healthy subjects: A randomized controlled study. J. Manip. Physiol. Ther. 2009, 32, 515–520. [Google Scholar] [CrossRef]
- Lavelle, E.D.; Lavelle, W.; Smith, H.S. Myofascial trigger points. Anesthesiol. Clin. 2007, 25, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Montañez-Aguilera, F.J.; Valtueña-Gimeno, N.; Pecos-Martín, D.; Arnau-Masanet, R.; Barrios-Pitarque, C.; Bosch-Morell, F. Changes in a patient with neck pain after application of ischemic compression as a trigger point therapy. J. Back Musculoskelet. Rehabil. 2010, 23, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Robertson, M. Self-Myofascial Release: Purpose, Methods, and Techniques; Robertson Training Systems: Indianapolis, IN, USA, 2008. [Google Scholar]
- Bradbury-Squires, D.J.; Noftall, J.C.; Sullivan, K.M.; Behm, D.G.; Power, K.E.; Button, D.C. Roller-massager application to the quadriceps and knee-joint range of motion and neuromuscular efficiency during a lunge. J. Athl. Train. 2015, 50, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halperin, I.; Aboodarda, S.J.; Button, D.C.; Andersen, L.L.; Behm, D.G. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int. J. Sports Phys. Ther. 2014, 9, 92–102. [Google Scholar] [PubMed]
- Mauntel, T.C.; Clark, M.A.; Padua, D. Effectiveness of myofascial release therapies on physical performance measurements: A systematic review. Athl. Train. Sports Health Care 2014, 6, 189–196. [Google Scholar] [CrossRef]
- Schleip, R. Fascial plasticity—A new neurobiological explanation: Part 1. J. Bodyw. Mov. Ther. 2003, 7, 11–19. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Kolber, M.J.; Cain, M.; Lee, M. The effects of self-myofascial release using a foam roll or roller massager on joint range of motion, muscle recovery, and performance: A systematic review. Int. J. Sports Phys. Ther. 2015, 10, 827–838. [Google Scholar] [PubMed]
- MacDonald, G.Z.; Button, D.C.; Drinkwater, E.J.; Behm, D.G. Foam rolling as a recovery tool after an intense bout of physical activity. Med. Sci. Sports Exerc. 2014, 46, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostiak, W.; Kaczmarek-Maciejewska, M.; Kasprzak, P. Foot and shin in terms of Anatomy Trains. J. Orthop. Trauma Surg. Rel. Res. 2011, 5, 38–46. [Google Scholar]
- Jones, A.M. Running economy is negatively related to sit-and-reach test performance in international-standard distance runners. Int. J. Sports Med. 2002, 23, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P.P.; Rosemann, T.; Knechtle, B. Force-velocity characteristics, muscle strength, and flexibility in female recreational marathon runners. Front. Physiol. 2018, 9, 1563. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Nosaka, K.; Chen, H.L.; Lin, M.J.; Tseng, K.W.; Chen, T.C. Effects of flexibility training on eccentric exercise-induced muscle damage. Med. Sci. Sports Exerc. 2011, 43, 491–500. [Google Scholar] [CrossRef]
- Del Coso, J.; Moreno, V.; Gutiérrez-Hellín, J.; Baltazar-Martins, G.; Ruíz-Moreno, C.; Aguilar-Navarro, M.; Lara, B.; Lucía, A. ACTN3 R577X genotype and exercise phenotypes in recreational marathon runners. Genes 2019, 10, 413. [Google Scholar] [CrossRef] [Green Version]
- Andersen, J.J. The State of Running 2019. Available online: https://racemedicine.org/the-state-of-running-2019 (accessed on 15 April 2020).
- Sports Medicine Institute. A Guide to the Foam Roller. Available online: http://smiweb.org/wp-content/uploads/2012/04/roller.pdf (accessed on 7 January 2021).
- Chaitow, L. Muscle Energy Techniques; Elsevier Health Sciences: London, UK, 2013. [Google Scholar]
- Skarabot, J.; Beardsley, C.; Stirn, I. Comparing the effects of self-myofascial release with static stretching on ankle range-of-motion in adolescent athletes. Int. J. Sports Phys. Ther. 2015, 10, 203–212. [Google Scholar] [PubMed]
- Mohr, A.R.; Long, B.C.; Goad, C.L. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J. Sport Rehabil. 2014, 23, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Roylance, D.S.; George, J.D.; Hammer, A.M.; Rencher, N.; Gellingham, G.W.; Hager, R.L.; Myrer, W.J. Evaluating acute changes in joint range-of-motion using self-myofascial release, postural alignment exercises, and static stretches. Int. J. Exerc. Sci. 2013, 6, 310–319. [Google Scholar]
- Sullivan, K.M.; Silvey, D.B.; Button, D.C.; Behm, D.G. Roller-massage application to the hamstrings increases sit-and reach range of motion within five to ten seconds without performance impairments. Int. J. Sports Phys. Ther. 2013, 8, 228–236. [Google Scholar] [PubMed]
- Morton, R.W.; Oikawa, S.Y.; Phillips, S.M.; Devries, M.C.; Mitchell, C.J. Self-myofascial release: No improvement of functional outcomes in ’tight’ hamstrings. Int. J. Sports Physiol. Perform. 2016, 11, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Peacock, C.A.; Krein, D.D.; Silver, T.A.; Sanders, G.J.; von Carlowitz, K.P.A. An acute bout of self-myofascial release in the form of foam rolling improves performance testing. Int. J. Exerc. Sci. 2014, 7, 202–211. [Google Scholar] [PubMed]
- Clapis, P.A.; Davis, S.M.; Davis, R.O. Reliability of inclinometer and goniometric measurements of hip extension flexibility using the modified Thomas test. Physiother. Theory Pract. 2008, 24, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Corkery, M.; Briscoe, H.; Ciccone, N.; Foglia, G.; Johnson, P.; Kinsman, S.; Legere, L.; Lum, B.; Canavan, P.K. Establishing normal values for lower extremity muscle length in college-age students. Phys. Ther. Sport. 2007, 8, 66–74. [Google Scholar] [CrossRef]
- Kendall, F.P.; McCreary, E.K.; Provance, P.G. Muscles: Testing and Function with Posture and Pain; Lippincott Williams & Wilkins: Baltimore, MA, USA, 2005. [Google Scholar]
- McGee, D.J. Orthopedic Physical Assessment; Saunders: Philadelphia, PA, USA, 2007. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 1 (n = 32) Mean ± SD | Group 2 (n = 30) Mean ± SD | |
|---|---|---|
| Age | 34.09 ± 7.73 | 33.46 ± 7.33 |
| Males | 22 | 18 |
| Females | 10 | 12 |
| High [cm] | 175.81 ± 8.73 | 177.60 ± 7.63 |
| Body mass [kg] | 69.88 ± 9.55 | 70.70 ± 8.79 |
| Total distance covered per week [km] | 47.34 ± 16.10 | 49.00 ± 17.91 |
| Outcome Measure | Group with FR (n = 32) Mean ± SD | pa | Group without FR (n = 30) Mean ± SD | pa | pb | |
|---|---|---|---|---|---|---|
| External rotation | Baseline | 60.07 ± 9.21 | 59.53 ± 8.96 | 0.776 | ||
| After | 60.77 ± 8.49 | <0.001 | 60.06 ± 8.40 | 0.742 | 0.342 | |
| Iliopsoas L | Baseline | 6.87 ± 3.74 | 6.93 ± 3.70 | 0.684 | ||
| After | 5.45 ± 3.73 | <0.001 | 5.48 ± 3.72 | <0.001 | 0.120 | |
| Iliopsoas R | Baseline | 6.60 ± 3.22 | 6.70 ± 3.12 | 0.599 | ||
| After | 5.38 ± 3.55 | <0.001 | 5.48 ± 3.49 | 0.001 | 0.178 | |
| Tensor fasciae latae L | Baseline | 18.60 ± 9.17 | 17.87 ± 9.19 | 0.849 | ||
| After | 21.03 ± 8.63 | 0.010 | 18.27 ± 8.76 | 0.331 | 0.598 | |
| Tensor fasciae latae R | Baseline | 18.82 ± 9.11 | 17.75 ± 8.68 | 0.715 | ||
| After | 21.53 ± 8.63 | 0.009 | 17.76 ± 8.11 | 0.964 | 0.851 | |
| Rectus femoris L | Baseline | 27.02 ± 3.51 | 27.38 ± 3.20 | 0.833 | ||
| After | 26.17 ± 3.28 | <0.001 | 26.50 ± 2.91 | 0.192 | 0.608 | |
| Rectus femoris R | Baseline | 26.92 ± 3.36 | 27.32 ± 3.09 | 0.801 | ||
| After | 25.90 ± 3.04 | <0.001 | 26.33 ± 2.80 | 0.296 | 0.432 | |
| Adductors | Baseline | 73.03 ± 13.21 | 72.87 ± 13.35 | 0.848 | ||
| After | 73.83 ± 13.37 | 0.061 | 73.77 ± 13.31 | 0.627 | 0.488 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sulowska-Daszyk, I.; Skiba, A. The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners. Int. J. Environ. Res. Public Health 2022, 19, 457. https://doi.org/10.3390/ijerph19010457
Sulowska-Daszyk I, Skiba A. The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners. International Journal of Environmental Research and Public Health. 2022; 19(1):457. https://doi.org/10.3390/ijerph19010457
Chicago/Turabian StyleSulowska-Daszyk, Iwona, and Agnieszka Skiba. 2022. "The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners" International Journal of Environmental Research and Public Health 19, no. 1: 457. https://doi.org/10.3390/ijerph19010457
APA StyleSulowska-Daszyk, I., & Skiba, A. (2022). The Influence of Self-Myofascial Release on Muscle Flexibility in Long-Distance Runners. International Journal of Environmental Research and Public Health, 19(1), 457. https://doi.org/10.3390/ijerph19010457