
Spanish Adaptation of the Overall Anxiety and Depression Severity and Impairment Scales in University Students

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Data
3.2. Validity Evidence Based on OASIS Internal Structure
3.3. Validity Evidence Based on ODSIS Internal Structure
3.4. Reliability
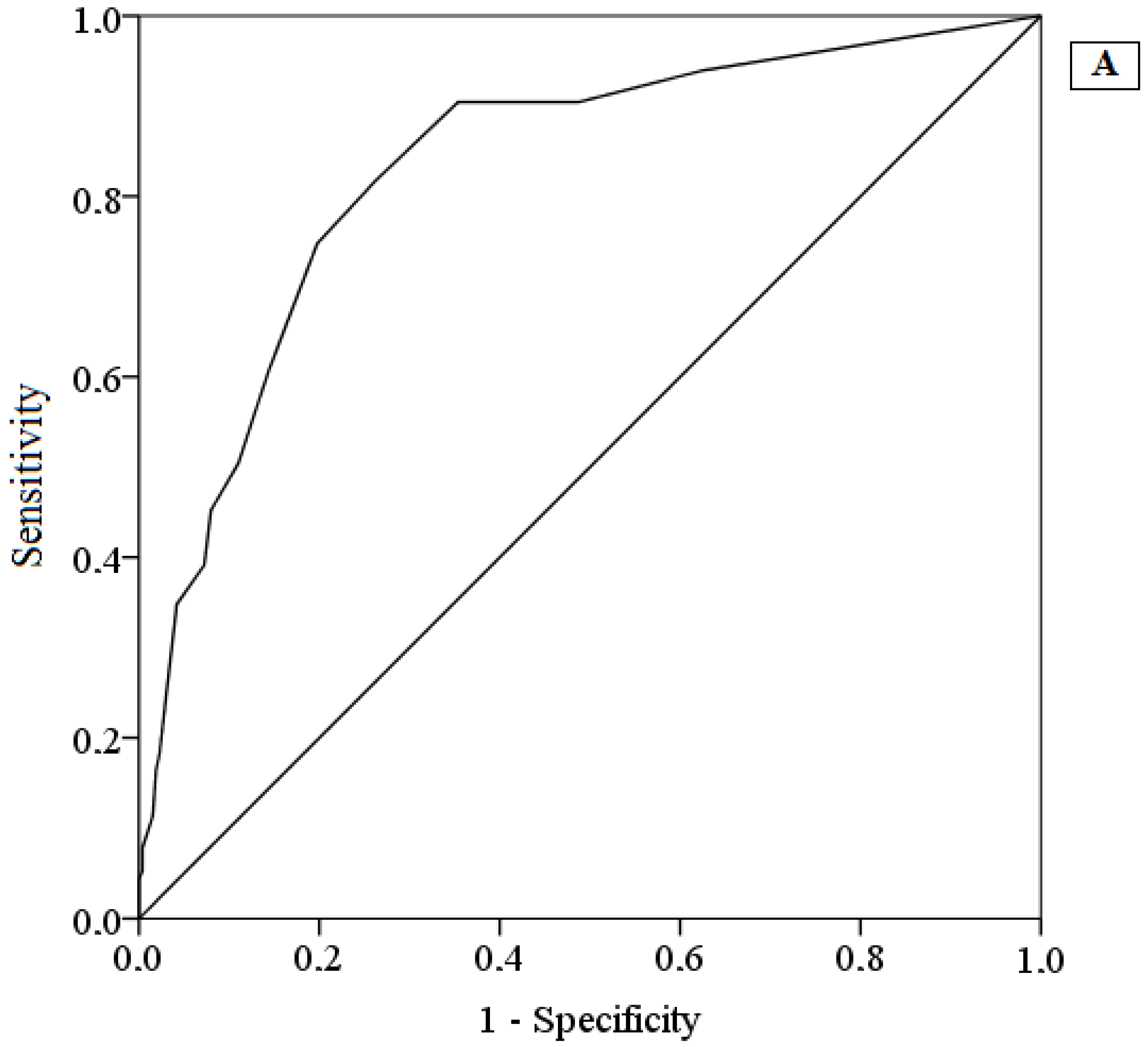
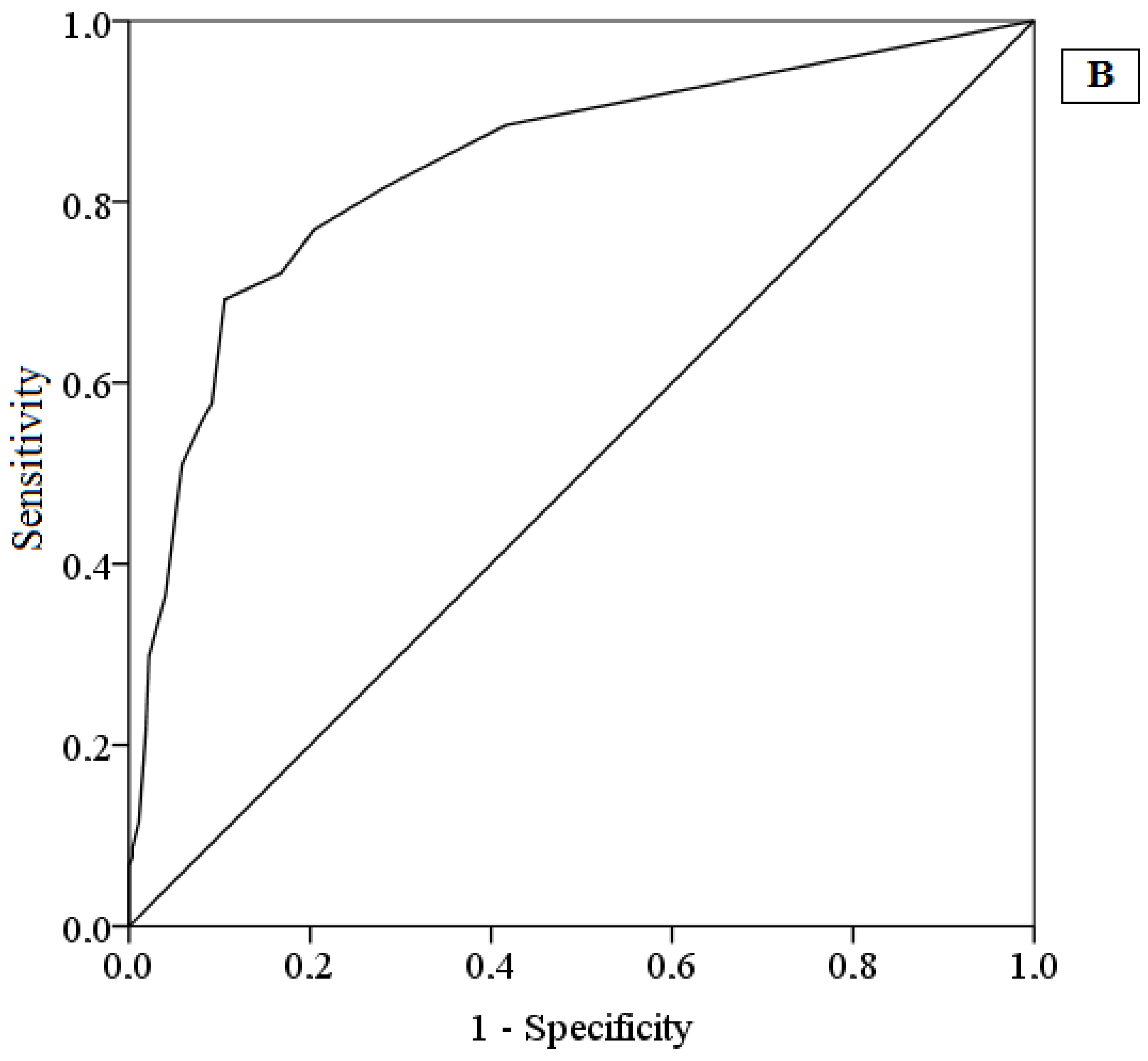
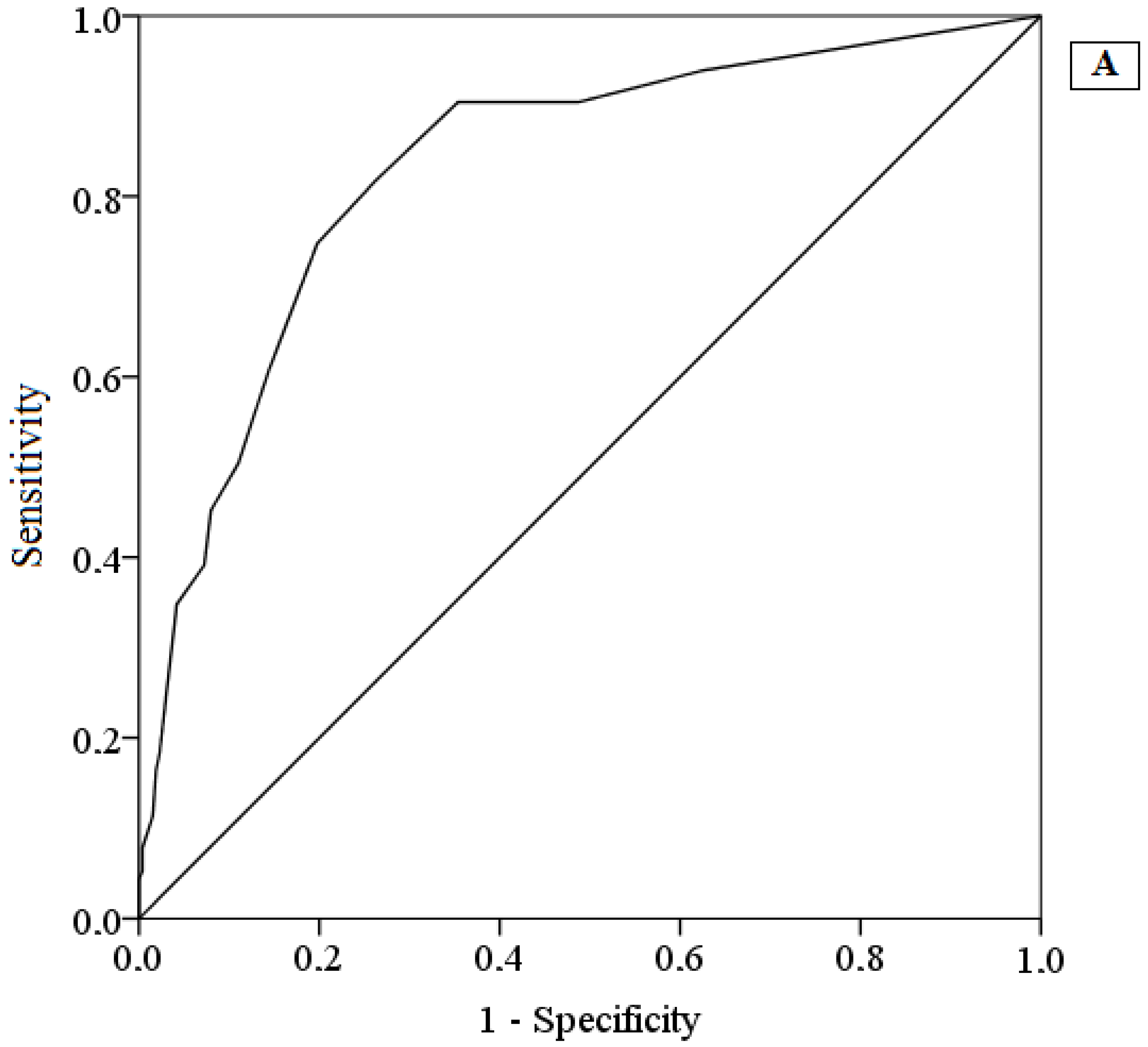
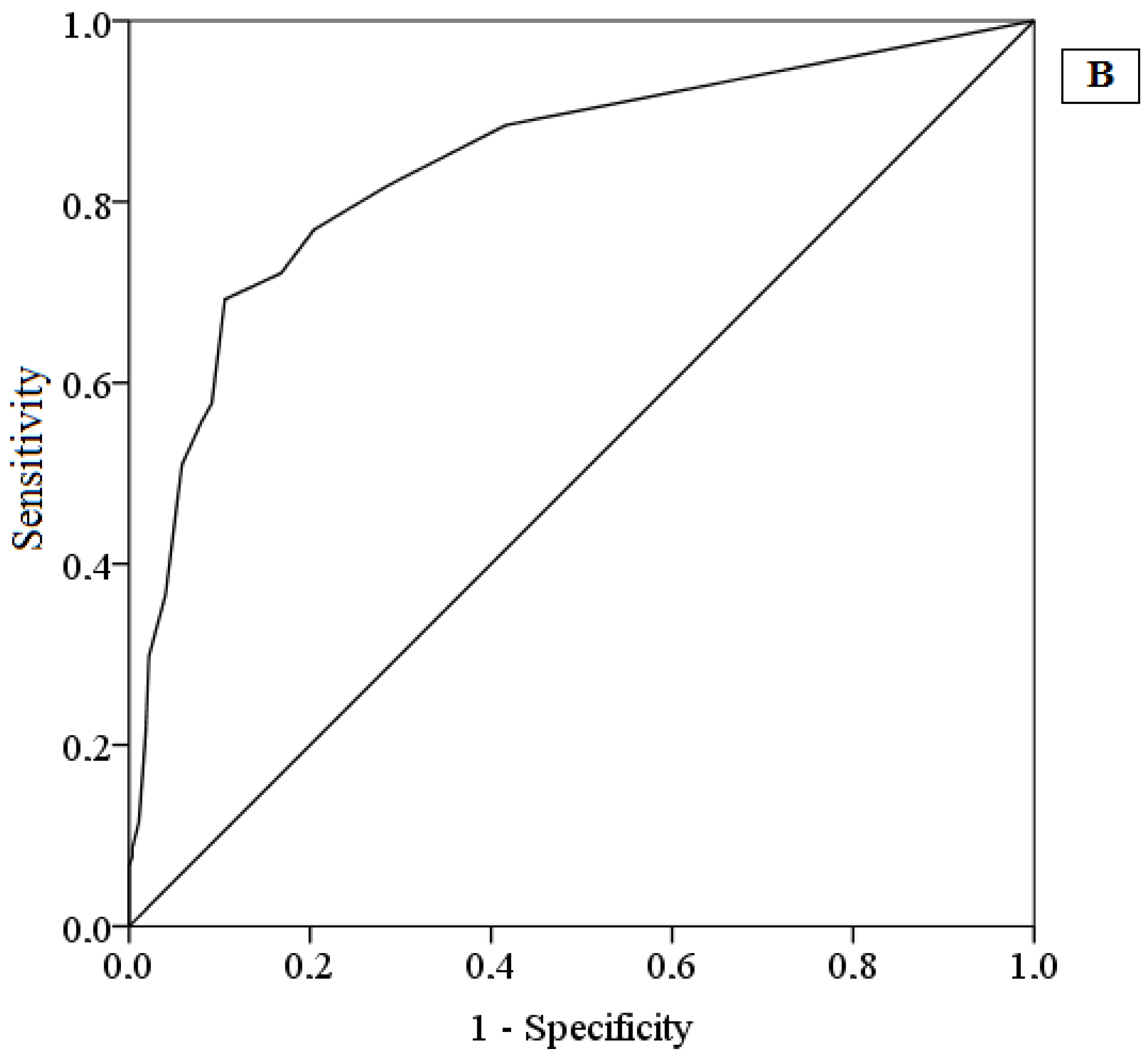
3.5. Validity Evidence Based on Relationships with Other Variables
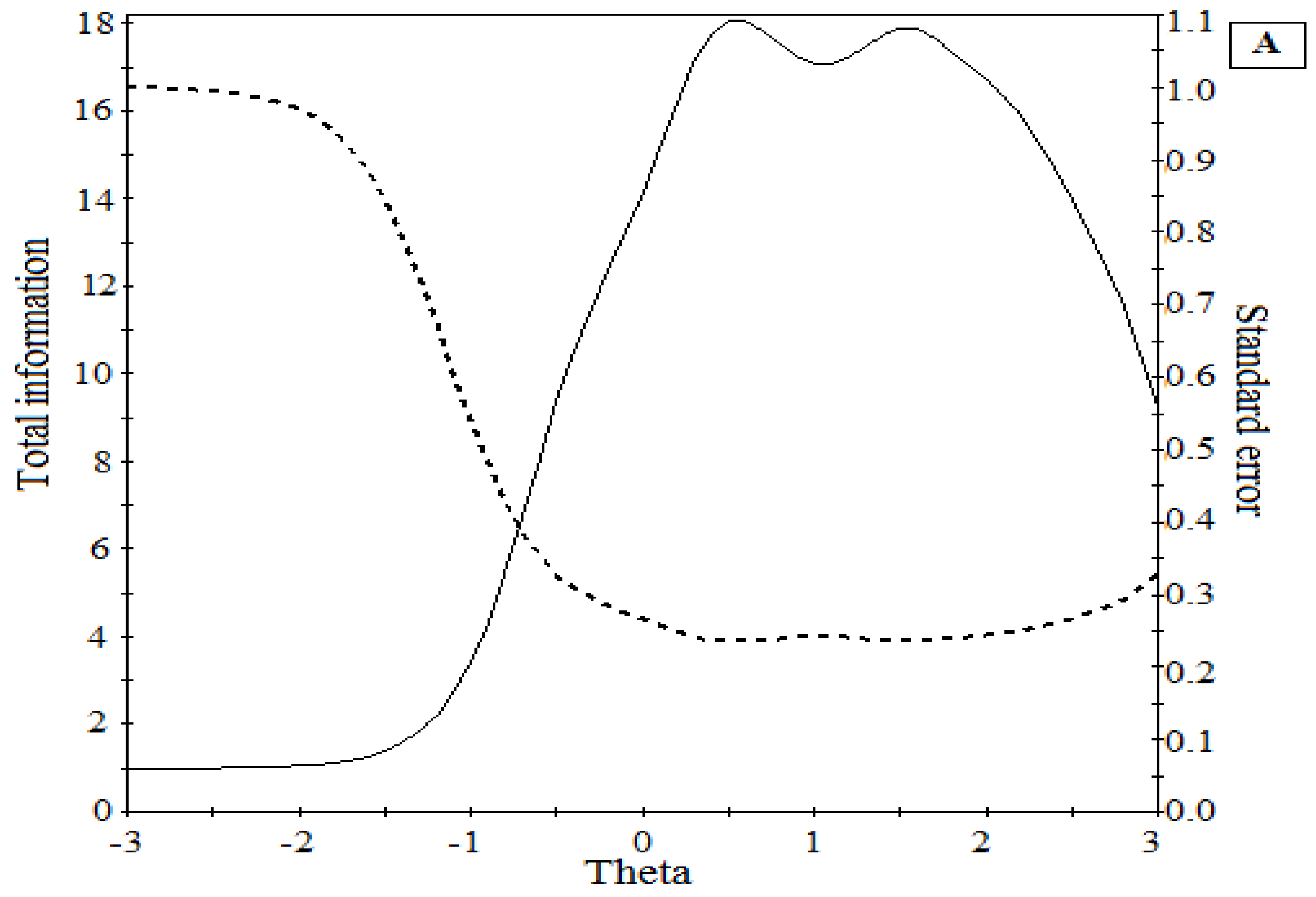
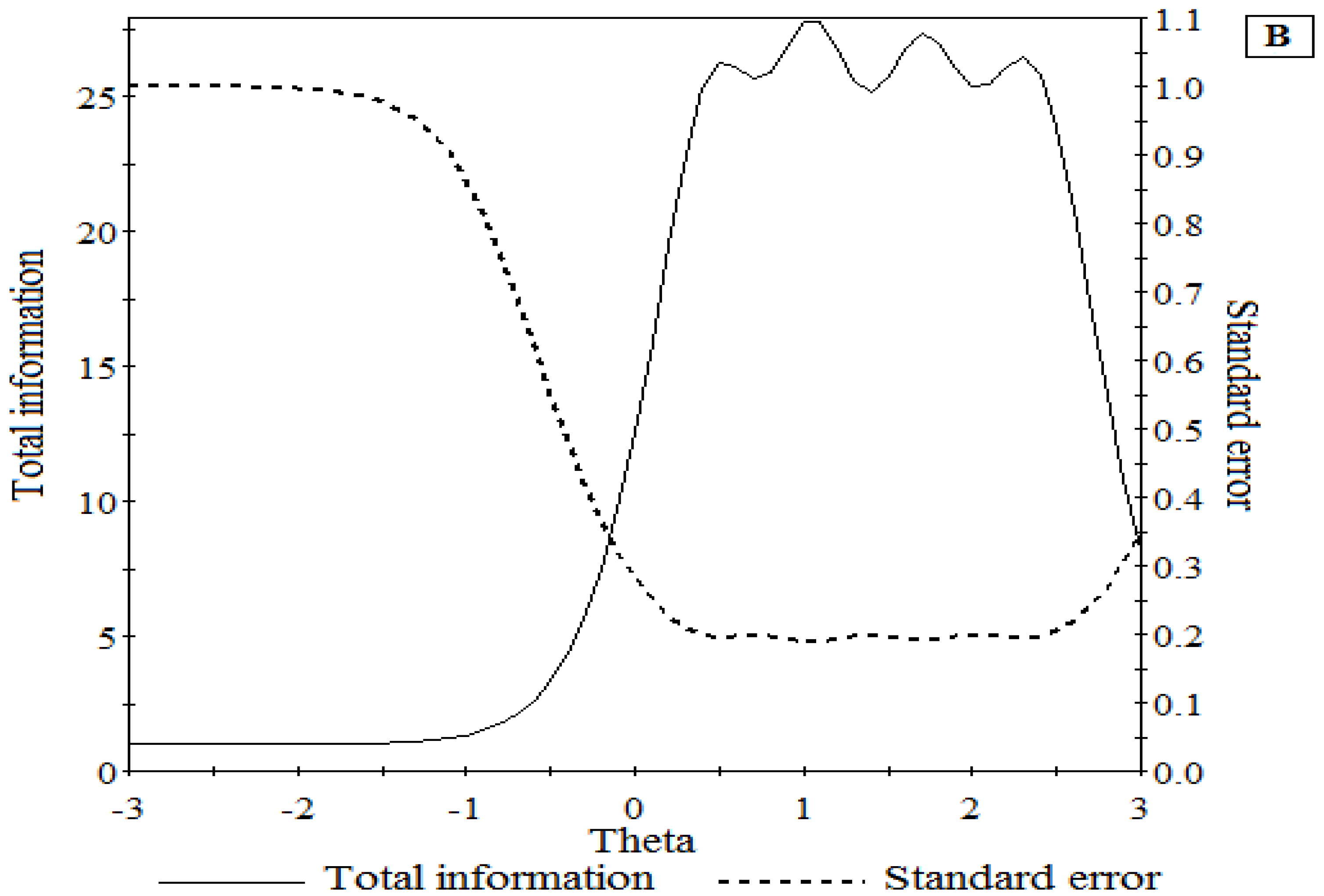
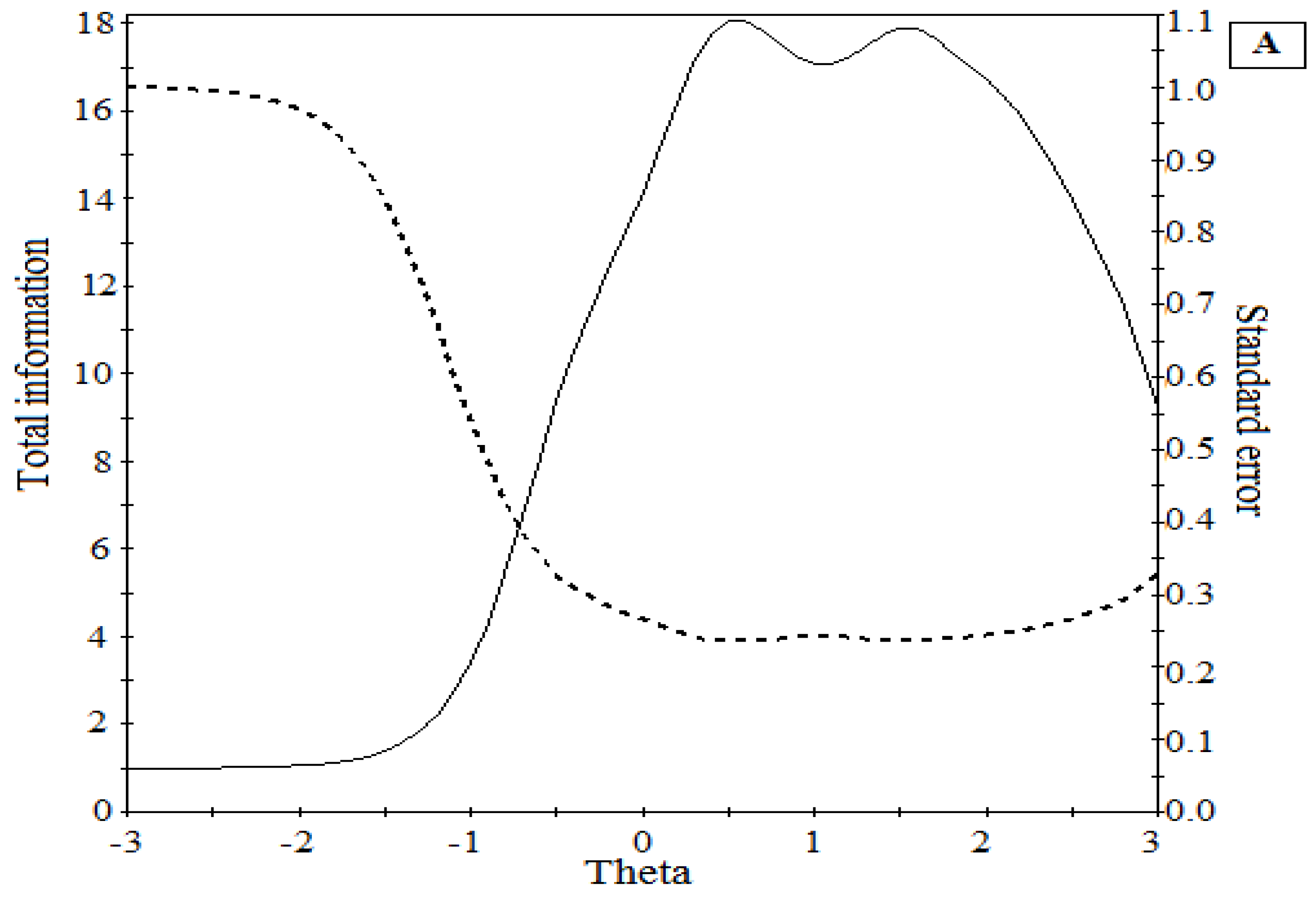
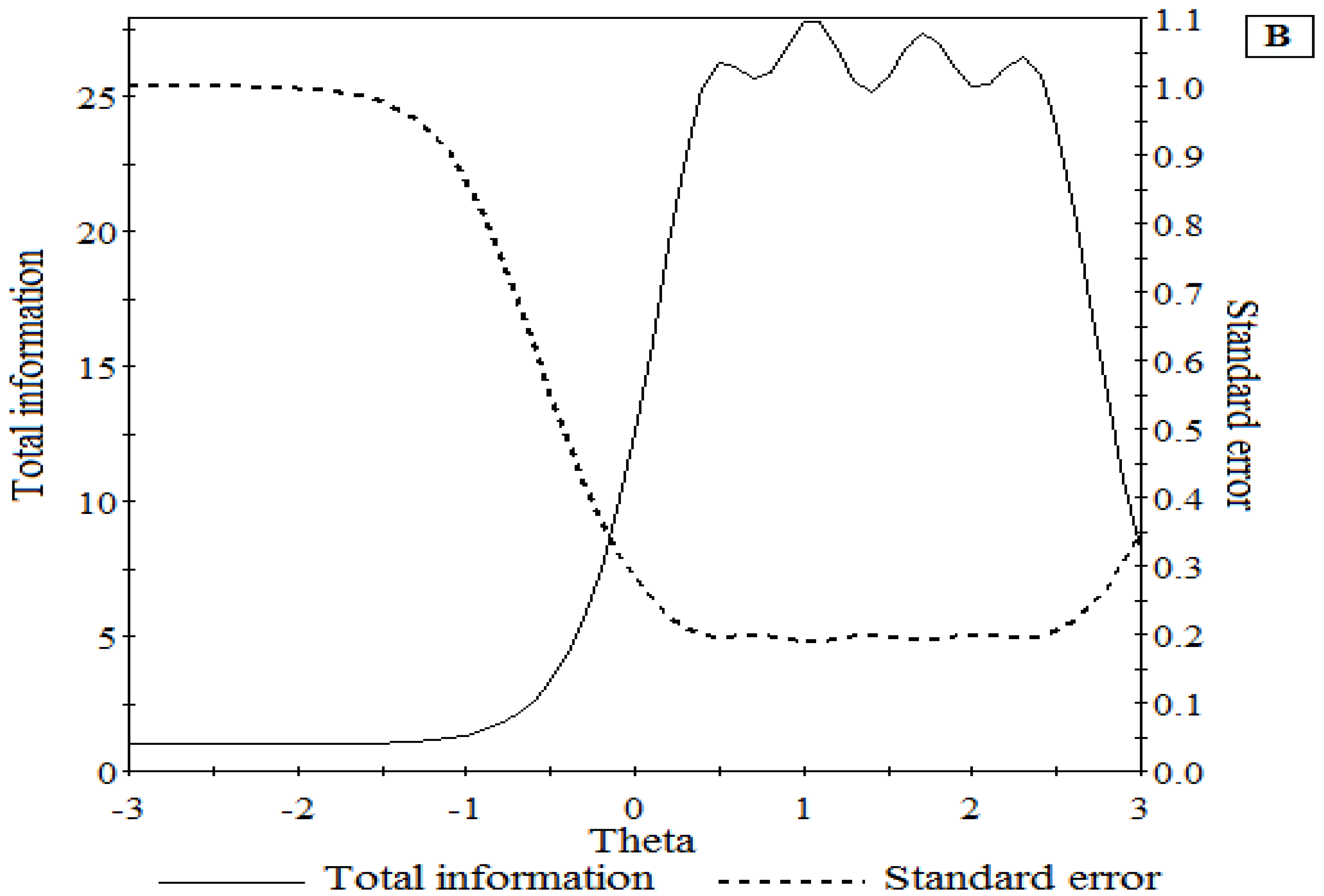
3.6. Item Response Theory Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bullis, J.R.; Boettcher, H.; Sauer-Zavala, S.; Farchione, T.J.; Barlow, D.H. What is an emotional disorder? A transdiagnostic mechanistic definition with implications for assessment, treatment, and prevention. Clin. Psychol. Sci. Pract. 2019, 26, e12278. [Google Scholar] [CrossRef]
- World Health Organization. Depression and other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global prevalence of anxiety disorders: A systematic review and meta-regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Cisler, J.M.; Tolin, D.F. Quality of life in the anxiety disorders: A meta-analytic review. Clin. Psychol. Rev. 2007, 27, 572–581. [Google Scholar] [CrossRef]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.L.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdollahi, M.; Abedi, P.; Abedi, A.; Abolhassani, H.; et al. Five insights from the Global Burden of Disease Study 2019. Lancet 2020, 396, 1135–1159. [Google Scholar] [CrossRef]
- Cooke, R.; Bewick, B.M.; Barkham, M.; Bradley, M.; Audin, K. Measuring, monitoring and managing the psychological well-being of first year university students. Br. J. Guid. Couns. 2006, 34, 505–517. [Google Scholar] [CrossRef]
- Harvey, S.B.; Glozier, N.; Henderson, M.; Allaway, S.; Litchfield, P.; Holland-Elliott, K.; Hotopf, M. Depression and work performance: An ecological study using web-based screening. Occup. Med. 2011, 61, 209–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hysenbegasi, A.; Hass, S.L.; Rowland, C.R. The impact of depression on the academic productivity of university students. J. Ment. Health Policy Econ. 2005, 8, 145. [Google Scholar]
- Ribeiro, Í.J.S.; Pereira, R.; Freire, I.V.; de Oliveira, B.G.; Casotti, C.A.; Boery, E.N. Stress and Quality of Life Among University Students: A Systematic Literature Review. Health Prof. Educ. 2018, 4, 70–77. [Google Scholar] [CrossRef]
- Adlaf, E.M.; Gliksman, L.; Demers, A.; Newton-Taylor, B. The Prevalence of Elevated Psychological Distress Among Canadian Undergraduates: Findings from the 1998 Canadian Campus Survey. J. Am. Coll. Health 2001, 50, 67–72. [Google Scholar] [CrossRef]
- Bayram, N.; Bilgel, N. The prevalence and socio-demographic correlations of depression, anxiety and stress among a group of university students. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Al-Naggar, R.A.; Al-Naggar, D.H. Prevalence and associated factors of emotional disorder among Malaysian University students. Int. J. Collab. Res. Intern. Med. Public Health 2012, 4, 1401–1411. [Google Scholar]
- Duffy, A.; Keown-Stoneman, C.; Goodday, S.; Horrocks, J.; Lowe, M.; King, N.; Saunders, K.E.A. Predictors of mental health and academic outcomes in first-year university students: Identifying prevention and early-intervention targets. BJPsych Open 2020, 6, e46. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, R.P.; Alonso, J.; Axinn, W.G.; Cuijpers, P.; Ebert, D.D.; Green, J.G.; Hwang, I.; Kessler, R.C.; Liu, H.; Mortier, P. Mental disorders among college students in the World Health Organization world mental health surveys. Psychol. Med. 2016, 46, 2955–2970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuijpers, P.; Cristea, I.A.; Ebert, D.D.; Koot, H.M.; Auerbach, R.P.; Bruffaerts, R.; Kessler, R.C. Psychological treatment of depression in college students: A metaanalysis. Depress. Anxiety 2016, 33, 400–414. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.K.; Kelly, S.J.; Adams, C.E.; Glazebrook, C. A systematic review of studies of depression prevalence in university students. J. Psychiatr. Res. 2013, 47, 391–400. [Google Scholar] [CrossRef]
- Weitzman, E.R. Poor Mental Health, Depression, and Associations with Alcohol Consumption, Harm, and Abuse in a National Sample of Young Adults in College. J. Nerv. Ment. Dis. 2004, 192, 269–277. [Google Scholar] [CrossRef]
- Finlay-Jones, R.A.; Burvill, P.W. The prevalence of minor psychiatric morbidity in the community. Psychol. Med. 1977, 7, 475–489. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Houck, P.R.; Spiegel, D.A.; Shear, M.K.; Rucci, P. Reliability of the self-report version of the panic disorder severity scale. Depress. Anxiety 2002, 15, 183–185. [Google Scholar] [CrossRef]
- Mattick, R.P.; Clarke, J.C. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav. Res. Ther. 1998, 36, 455–470. [Google Scholar] [CrossRef]
- Meyer, T.J.; Miller, M.L.; Metzger, R.L.; Borkovec, T.D. Development and validation of the penn state worry questionnaire. Behav. Res. Ther. 1990, 28, 487–495. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Norman, S.B.; Craske, M.G.; Sulivan, G.; Lang, A.J.; Chavira, D.A.; Bystritsky, A.; Sherbourne, C.; Roy-Byrne, P.; Stein, M.B. Validation of a brief measure of anxiety-related severity and impairment: The Overall Anxiety Sensitivity and Impairment Scale (OASIS). J. Affect. Disord. 2009, 112, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlow, D.H.; Allen, L.B.; Choate, M.L. Toward a unified treatment for emotional disorders. Behav. Ther. 2016, 47, 838–853. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, M.; Kemper, C.J.; Kruyen, P. Short Scales–Five Misunderstandings and Ways to Overcome Them. J. Individ Differ. 2014, 35, 185–189. [Google Scholar] [CrossRef]
- Norman, S.B.; Cissel, S.H.; Means-Christensen, A.J.; Stein, M.B. Development and validation of an Overall Anxiety Severity and Impairment Scale. Depress. Anxiety 2006, 23, 245–249. [Google Scholar] [CrossRef]
- Bentley, K.H.; Gallagher, M.W.; Carl, J.R.; Barlow, D.H. Development and validation of the Overall Depression Severity and Impairment Scale. Psychol. Assess. 2014, 26, 815–830. [Google Scholar] [CrossRef] [PubMed]
- Osma, J.; Castellano, C.; Crespo, E.; García-Palacios, A. The unified protocol for transdiagnostic treatment of emotional disorders in group format in a spanish public mental health setting. Behav. Psychol. 2015, 23, 447–466. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Oe, Y.; Kato, N.; Nakajima, S.; Fujisato, H.; Miyamae, M.; Kanie, A.; Horikoshi, M.; Norman, S.B. Validity and clinical interpretability of Overall Anxiety Severity and Impairment Scale (OASIS). J. Affect. Disord. 2015, 170, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Hermans, M.; Korrelboom, K.; Visser, S. A Dutch version of the Overall Anxiety Severity and Impairment Scale (OASIS): Psychometric properties and validation. J. Affect. Disord. 2015, 172, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Farrahi, H.; Gharraee, B.; Oghabian, M.A.; Pirmoradi, M.R.; Najibi, S.M.; Batouli, S.A.H. Psychometric Properties of the Persian Version of the Overall Anxiety Severity and Impairment Scale (OASIS). Iran. J. Psychiatry Behav. Sci. 2020, 14. Available online: http://eprints.iums.ac.ir/id/eprint/38973 (accessed on 16 November 2021). [CrossRef]
- Sandora, J.; Novak, L.; Brnka, R.; van Dijk, J.P.; Tavel, P.; Malinakova, K. The abbreviated overall anxiety severity and impairment scale (Oasis) and the abbreviated overall depression severity and impairment scale (odsis): Psychometric properties and evaluation of the czech versions. Int. J. Environ. Res. Public Health 2021, 18, 10337. [Google Scholar] [CrossRef] [PubMed]
- Ito, M.; Bentley, K.H.; Oe, Y.; Nakajima, S.; Fujisato, H.; Kato, N.; Miyamae, M.; Kanie, A.; Horikoshi, M.; Barlow, D.H. Assessing depression related severity and functional impairment(warning) the Overall Depression Severity and Impairment Scale (ODSIS). PLoS ONE 2015, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- González-Robles, A.; Mira, A.; Miguel, C.; Molinari, G.; Díaz-García, A.; García-Palacios, A.; Bretón-López, J.M.; Quero, S.; Baños, R.M.; Botella, C. A brief online transdiagnostic measure: Psychometric properties of the Overall Anxiety Severity and Impairment Scale (OASIS) among Spanish patients with emotional disorders. PLoS ONE 2018, 13, e0206516. [Google Scholar] [CrossRef] [PubMed]
- Osma, J.; Quilez-Orden, A.; Suso-Ribera, C.; Peris-Baquero, O.; Norman, S.B.; Bentley, K.H.; Sauer-Zavala, S. Psychometric properties and validation of the Spanish versions of the overall anxiety and depression severity and impairment scales. J. Affect. Disord. 2019, 252, 9–18. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.A.; Welch, S.S.; Michonski, J.; Poquiz, J.; Osborne, T.L.; Sayrs, J.; Spanos, A. Psychometric evaluation of the Overall Anxiety Severity and Impairment Scale (OASIS) in individuals seeking outpatient specialty treatment for anxiety-related disorders. J. Affec. Disord. 2015, 175, 463–470. [Google Scholar] [CrossRef]
- Norman, S.B.; Campbell-Sills, L.; Hitchcock, C.A.; Sullivan, S.; Rochlin, A.; Wilkins, K.C.; Stein, M.B. Psychometrics of a brief measure of anxiety to detect severity and impairment: The overall anxiety severity and impairment scale (OASIS). J. Psychiatr. Res. 2011, 45, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Bragdon, L.B.; Diefenbach, G.J.; Hannan, S.; Tolin, D.F. Psychometric properties of the Overall Anxiety Severity and Impairment Scale (OASIS) among psychiatric outpatients. J. Affect. Disord. 2016, 201, 112–115. [Google Scholar] [CrossRef] [PubMed]
- Mira, A.; Gonzalez-Robles, A.; Miguel, C. Capturing the Severity and Impairment Associated with Depression: The Overall Depression Severity and Impairment Scale (ODSIS) Validation in a Spanish Clinical Sample. Front. Psychiatry 2019, 10, 180. [Google Scholar] [CrossRef]
- Norman, S.B.; Allard, C.B.; Trim, R.S.; Thorp, S.R.; Behrooznia, M.; Masino, T.T.; Stein, M.B. Psychometrics of the overall anxiety severity and impairment scale (OASIS) in a sample of women with and without trauma histories. Arch. Women Ment. Health 2013, 16, 123–129. [Google Scholar] [CrossRef]
- Brooks, R. EuroQol: The current state of play. Health Policy 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. La versión española del EuroQol: Descripción y aplicaciones [EuroQol Spanish Version: Description and Aplications]. Med. Clín. 1999, 112, 79–86. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The estructure of negative emotional states: Comparison of the depression anxiety stress scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Bados, A.; Solanas, A.; Andrés, R. Psycometric Properties of the Spanish Version of Depression, Anxiety and Stress Scales (DASS). Psicothema 2005, 17, 679–683. [Google Scholar]
- Qualtrics; Version 2.16; Computer Program; Qualtrics: Provo, UT, USA, 2017.
- Commission, I.T. ITC Guidelines for Translating and Adapting Tests (Second Edition). Int. J. Test. 2018, 18, 101–134. [Google Scholar] [CrossRef]
- Timmerman, M.E.; Lorenzo-Seva, U. Dimensionality assessment of ordered polytomous items with parallel analysis. Psychol. Methods 2011, 16, 209. [Google Scholar] [CrossRef] [PubMed]
- Abad, F.J.; Olea, J.; Ponsoda, V.; García, C. Medición en Ciencias Sociales y de la Salud [Measurement in Social and Health Sciences]; Síntesis: Madrid, Spain, 2011. [Google Scholar]
- Ferrando, P.J.; Lorenzo-Seva, U. Assessing the quality and appropriateness of factor solutions and factor score estimates in exploratory item factor analysis. Educ. Psychol. Meas. 2018, 78, 762–780. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Haeberlein, K.; Chang, A.; Handal, P. Convergent Validity and Preliminary Cut-Off Scores for the Anxiety and Depression Subscales of the DASS-21 in US Adolescents. Child. Psychiatry Hum. Dev. 2020, 52, 579–585. [Google Scholar] [CrossRef]
- Roman, F.; Santibañez, P.; Vinet, V. Use of the Depression Anxiety Stress Scales (DASS-21) as Screening Tests in Clinical Youngsters. Acta Investig. Psicol. 2016, 6, 2325–2336. [Google Scholar]
- Samejima, F. Estimation of latent ability using a response pattern of graded scores. Psychom. Monogr. Suppl. 1969, 34, 100. [Google Scholar] [CrossRef]
- Universitat Rovira i Virgili, FACTOR 10.10.03; Universitat Rovira I Virgili: Tarrazona, Spain, 2020.
- Muthén, L.K.; Muthén, B.O. Growth Modeling with Latent Variable Using Mplus: Advanced Growth Models, Survival Analysis and Missing Data; Mplus Short Courses: Los Angeles, CA, USA, 2010. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows; Version 26.0; IBM Corp.: Armonk, NY, USA, 2019. [Google Scholar]
- Vector Psychometric Group, LLC. IRTPRO 4.2; Group LLC.: Chapel Hill, NC, USA, 2013. [Google Scholar]
- Kim, H.-Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Socio-Demographic Characteristics | n | % |
|---|---|---|
| Marital status | ||
| Single | 256 | 67.7 |
| Married or with a partner | 117 | 31 |
| Divorced | 5 | 1.3 |
| Employment situation | ||
| Not active (retired, unemployed, on sick leave) | 256 | 67.7 |
| Active | 122 | 32.3 |
| Ongoing university studies | ||
| Psychology | 211 | 55.8 |
| Master in General Health Psychology | 52 | 13.8 |
| Doctorate | 26 | 6.9 |
| Nursing | 19 | 5.0 |
| Teacher training | 14 | 3.7 |
| Medicine | 9 | 2.4 |
| Other | 47 | 12.4 |
| Past psychological treatment | ||
| No | 252 | 66.7 |
| Yes | 126 | 33.3 |
| Items | Loading | DI | a |
|---|---|---|---|
| 1. | 0.893 | 0.808 | 4.15 |
| 2. | 0.863 | 0.787 | 3.80 |
| 3. | 0.832 | 0.721 | 2.77 |
| 4. | 0.853 | 0.752 | 3.07 |
| 5. | 0.888 | 0.797 | 3.90 |
| Items | Loading | DI | a |
|---|---|---|---|
| 1. | 0.859 | 0.802 | 3.85 |
| 2. | 0.885 | 0.839 | 4.56 |
| 3. | 0.888 | 0.810 | 4.01 |
| 4. | 0.931 | 0.866 | 5.38 |
| 5. | 0.865 | 0.820 | 4.29 |
| 2 | 3 | 4 | 5 | |
|---|---|---|---|---|
| 1. OASIS | 0.653 * | 0.663 * | 0.599 * | −0.338 * |
| 2. ODSIS | 1 | 0.510 * | 0.738 * | −0.401 * |
| 3. DASS-14-A | 1 | 0.616 * | −0.304 * | |
| 4. DASS-14-D | 1 | −0.381 * | ||
| 5. VAS-EuroQol | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osma, J.; Martínez-Loredo, V.; Díaz-García, A.; Quilez-Orden, A.; Peris-Baquero, Ó. Spanish Adaptation of the Overall Anxiety and Depression Severity and Impairment Scales in University Students. Int. J. Environ. Res. Public Health 2022, 19, 345. https://doi.org/10.3390/ijerph19010345
Osma J, Martínez-Loredo V, Díaz-García A, Quilez-Orden A, Peris-Baquero Ó. Spanish Adaptation of the Overall Anxiety and Depression Severity and Impairment Scales in University Students. International Journal of Environmental Research and Public Health. 2022; 19(1):345. https://doi.org/10.3390/ijerph19010345
Chicago/Turabian StyleOsma, Jorge, Víctor Martínez-Loredo, Amanda Díaz-García, Alba Quilez-Orden, and Óscar Peris-Baquero. 2022. "Spanish Adaptation of the Overall Anxiety and Depression Severity and Impairment Scales in University Students" International Journal of Environmental Research and Public Health 19, no. 1: 345. https://doi.org/10.3390/ijerph19010345
APA StyleOsma, J., Martínez-Loredo, V., Díaz-García, A., Quilez-Orden, A., & Peris-Baquero, Ó. (2022). Spanish Adaptation of the Overall Anxiety and Depression Severity and Impairment Scales in University Students. International Journal of Environmental Research and Public Health, 19(1), 345. https://doi.org/10.3390/ijerph19010345