
Vitamin D and Depressive Symptoms in Adults with Multiple Sclerosis: A Scoping Review

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
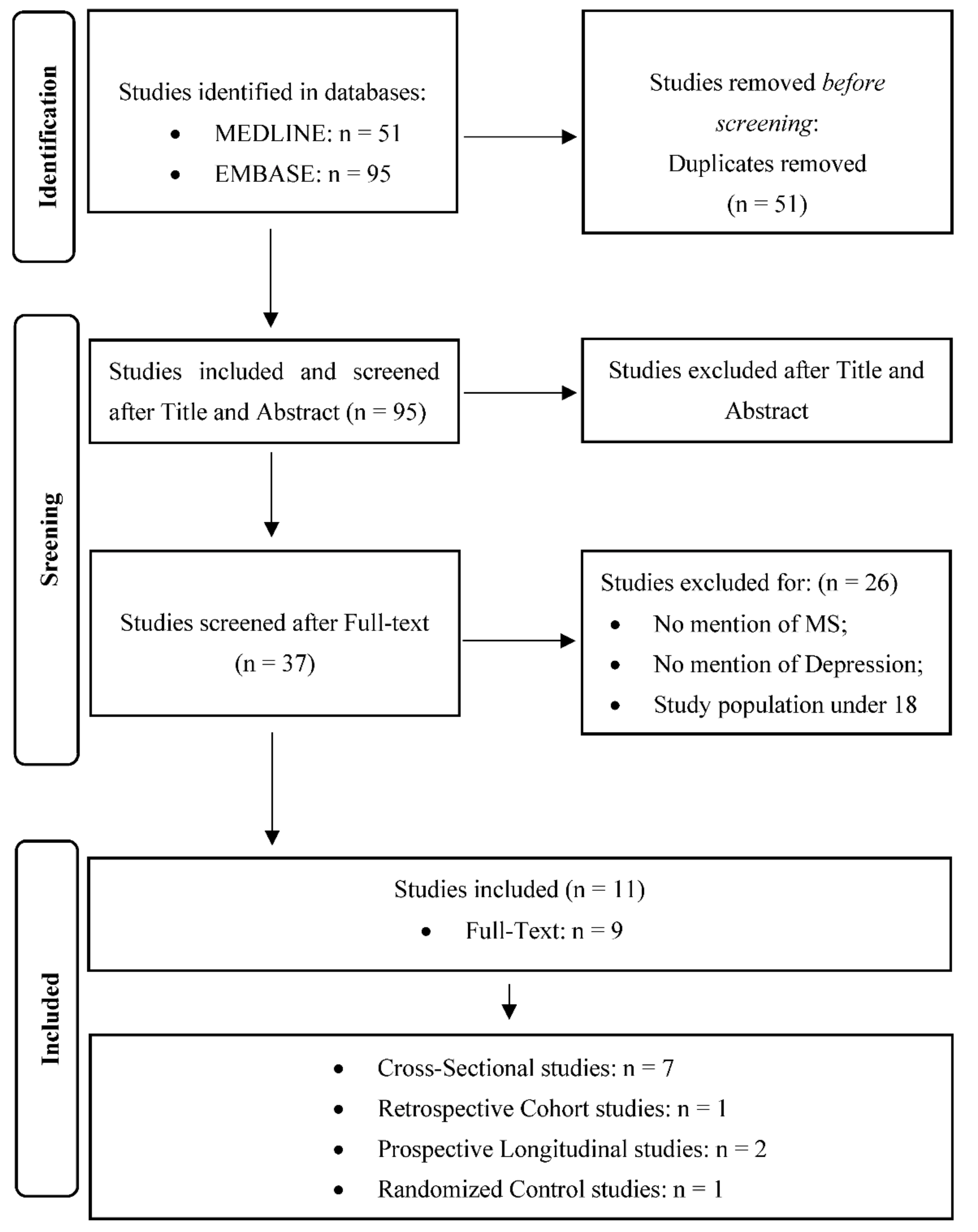
2. Methods
2.1. Search Strategy
2.2. Search and Studies Selection
Quality Assessment
3. Results
3.1. What Is the Association between Circulating Levels of Vitamin D and Symptoms of Depression?
3.2. What Is the Association between Vitamin D Supplementation or Sun Exposure on Depression Symptoms?
3.3. Study Design Cross-Sectional Studies
Longitudinal Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Patti, F.; Zanghì, A.; Chisari, C.G.; Lo Fermo, S.; Zappia, M. Late-onset and young-onset relapsing-remitting multiple sclerosis: Evidence from a retrospective long-term follow-up study. Eur. J. Neurol. 2018, 25, 1425–1431. [Google Scholar] [CrossRef] [PubMed]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- D’Amico, E.; Zanghì, A.; Serra, A.; Murabito, P.; Zappia, M.; Patti, F.; Cocuzza, S. Management of dysphagia in multiple sclerosis: Current best practice. Expert Rev. Gastroenterol. Hepatol. 2019, 13, 47–54. [Google Scholar] [CrossRef]
- D’Amico, E.; Patti, F.; Zanghì, A.; Zappia, M. A Personalized Approach in Progressive Multiple Sclerosis: The Current Status of Disease Modifying Therapies (DMTs) and Future Perspectives. Int. J. Mol. Sci. 2016, 17, 1725. [Google Scholar] [CrossRef] [Green Version]
- Zanghì, A.; Cimino, S.; Urzì, D.; Privitera, S.; Zagari, F.; Lanza, G.; Patti, F.; D’Amico, E. Pharmacotherapeutic management of lower urinary tract symptoms in Multiple Sclerosis patients. Expert Opin. Pharmacother. 2020, 21, 1449–1454. [Google Scholar] [CrossRef]
- Alvino, B.; Arianna, F.; Assunta, B.; Antonio, C.; Emanuele, D.; Giorgia, M.; Leonardo, S.; Daniele, S.; Renato, D.; Buscarinu, M.C.; et al. Prevalence and predictors of bowel dysfunction in a large multiple sclerosis outpatient population: An Italian multicenter study. J. Neurol. 2021. Online ahead of print. [Google Scholar] [CrossRef]
- Biernacki, T.; Sandi, D.; Kincses, Z.T.; Füvesi, J.; Rózsa, C.; Mátyás, K.; Vécsei, L.; Bencsik, K. Contributing factors to health-related quality of life in multiple sclerosis. Brain Behav. 2019, 9, e01466. [Google Scholar] [CrossRef]
- Solaro, C.; Gamberini, G.; Masuccio, F.G. Depression in Multiple Sclerosis: Epidemiology, Aetiology, Diagnosis and Treatment. CNS Drugs 2018, 32, 117–133. [Google Scholar] [CrossRef]
- Feinstein, A.; Magalhaes, S.; Richard, J.F.; Audet, B.; Moore, C. The link between multiple sclerosis and depression. Nat. Rev. Neurol. 2014, 10, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J.; Group, M.S.; European Multiple Sclerosis, P. New insights into the burden and costs of multiple sclerosis in Europe. Mult. Scler. 2017, 23, 1123–1136. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Forte, A.; Palermo, M.; Stefani, H.; Lamis, D.A.; Serafini, G.; Amore, M.; Girardi, P. Suicide risk in multiple sclerosis: A systematic review of current literature. J. Psychosom. Res. 2012, 73, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Patti, F.; Leone, C.; D’Amico, E. Treatment options of cognitive impairment in multiple sclerosis. Neurol. Sci. 2010, 31 (Suppl. 2), 265–269. [Google Scholar] [CrossRef]
- Zanghì, A.; D’Amico, E.; Lo Fermo, S.; Patti, F. Exploring polypharmacy phenomenon in newly diagnosed relapsing-remitting multiple sclerosis: A cohort ambispective single-centre study. Ther. Adv. Chronic Dis. 2021, 12, 2040622320983121. [Google Scholar] [CrossRef]
- Zanghì, A.; D’Amico, E.; Patti, F. Immunosuppression in relapsing remitting multiple sclerosis: Moving towards personalized treatment. Expert Rev. Neurother. 2020, 20, 771–782. [Google Scholar] [CrossRef]
- D’Amico, E.; Chisari, C.G.; Arena, S.; Zanghì, A.; Toscano, S.; Lo Fermo, S.; Maimone, D.; Castaing, M.; Sciacca, S.; Zappia, M.; et al. Cancer Risk and Multiple Sclerosis: Evidence From a Large Italian Cohort. Front. Neurol. 2019, 10, 337. [Google Scholar] [CrossRef] [Green Version]
- D’Amico, E.; Leone, C.; Zanghì, A.; Fermo, S.L.; Patti, F. Lateral and escalation therapy in relapsing-remitting multiple sclerosis: A comparative study. J. Neurol. 2016, 263, 1802–1809. [Google Scholar] [CrossRef]
- Munger, K.L.; Hongell, K.; Åivo, J.; Soilu-Hänninen, M.; Surcel, H.M.; Ascherio, A. 25-Hydroxyvitamin D deficiency and risk of MS among women in the Finnish Maternity Cohort. Neurology 2017, 89, 1578–1583. [Google Scholar] [CrossRef]
- Yadav, V.; Narayanaswami, P. Complementary and alternative medical therapies in multiple sclerosis--the American Academy of Neurology guidelines: A commentary. Clin. Ther. 2014, 36, 1972–1978. [Google Scholar] [CrossRef] [PubMed]
- Mojaverrostami, S.; Bojnordi, M.N.; Ghasemi-Kasman, M.; Ebrahimzadeh, M.A.; Hamidabadi, H.G. A Review of Herbal Therapy in Multiple Sclerosis. Adv. Pharm. Bull. 2018, 8, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Concerto, C.; Boo, H.; Hu, C.; Sandilya, P.; Krish, A.; Chusid, E.; Coira, D.; Aguglia, E.; Battaglia, F. Hypericum perforatum extract modulates cortical plasticity in humans. Psychopharmacology 2018, 235, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Concerto, C.; Infortuna, C.; Muscatello, M.R.A.; Bruno, A.; Zoccali, R.; Chusid, E.; Aguglia, E.; Battaglia, F. Exploring the effect of adaptogenic Rhodiola Rosea extract on neuroplasticity in humans. Complement. Ther. Med. 2018, 41, 141–146. [Google Scholar] [CrossRef]
- Mineo, L.; Concerto, C.; Patel, D.; Mayorga, T.; Paula, M.; Chusid, E.; Aguglia, E.; Battaglia, F. Valeriana officinalis Root Extract Modulates Cortical Excitatory Circuits in Humans. Neuropsychobiology 2017, 75, 46–51. [Google Scholar] [CrossRef]
- El-Salem, K.; Khalil, H.; Al-Sharman, A.; Al-Mistarehi, A.H.; Yassin, A.; Alhayk, K.A.; Qawasmeh, M.A.; Bashayreh, S.Y.; Kofahi, R.M.; Obeidat, A.Z. Serum vitamin d inversely correlates with depression scores in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 48, 102732. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, C.; Souberbielle, J.C. Vitamin D and multiple sclerosis: An update. Mult. Scler. Relat. Disord. 2017, 14, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Peelen, E.; Knippenberg, S.; Muris, A.H.; Thewissen, M.; Smolders, J.; Tervaert, J.W.; Hupperts, R.; Damoiseaux, J. Effects of vitamin D on the peripheral adaptive immune system: A review. Autoimmun. Rev. 2011, 10, 733–743. [Google Scholar] [CrossRef]
- Haroon, E.; Raison, C.L.; Miller, A.H. Psychoneuroimmunology meets neuropsychopharmacology: Translational implications of the impact of inflammation on behavior. Neuropsychopharmacology 2011, 37, 137–162. [Google Scholar] [CrossRef]
- Yuan, X.; Guo, L.; Jiang, C.; Yang, X.; Huang, J. The Effect of Different Administration Time and Dosage of Vitamin D Supplementation in Patients with Multiple Sclerosis: A Meta-Analysis of Randomized Controlled Trials. Neuroimmunomodulation 2021, 28, 118–128. [Google Scholar] [CrossRef]
- Zech, L.D.; Scherf-Clavel, M.; Daniels, C.; Schwab, M.; Deckert, J.; Unterecker, S.; Herr, A.S. Patients with higher vitamin D levels show stronger improvement of self-reported depressive symptoms in psychogeriatric day-care setting. J. Neural Transm. 2021, 128, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Berridge, M.J. Vitamin D and Depression: Cellular and Regulatory Mechanisms. Pharmacol. Rev. 2017, 69, 80–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elrayah, E.E.; Rogers, L.; Doggui, R.; Al-Jawaldeh, A. Vitamin D Insufficiency and Deficiency in the Eastern Mediterranean Region (EMR)-Misconceptions in Public Health Practice: A Scoping Review 2019–2020. J. Nutr. Sci. Vitaminol. 2020, 66, 389–395. [Google Scholar] [CrossRef]
- Kubera, M.; Lin, A.H.; Kenis, G.; Bosmans, E.; van Bockstaele, D.; Maes, M. Anti-Inflammatory effects of antidepressants through suppression of the interferon-gamma/interleukin-10 production ratio. J. Clin. Psychopharmacol. 2001, 21, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Dogan-Sander, E.; Mergl, R.; Willenberg, A.; Baber, R.; Wirkner, K.; Riedel-Heller, S.G.; Röhr, S.; Schmidt, F.M.; Schomerus, G.; Sander, C. Inflammation and the Association of Vitamin D and Depressive Symptomatology. Nutrients 2021, 13, 1972. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Sneve, M.; Figenschau, Y.; Svartberg, J.; Waterloo, K. Effects of vitamin D supplementation on symptoms of depression in overweight and obese subjects: Randomized double blind trial. J. Intern. Med. 2008, 264, 599–609. [Google Scholar] [CrossRef]
- Ju, S.Y.; Lee, Y.J.; Jeong, S.N. Serum 25-hydroxyvitamin D levels and the risk of depression: A systematic review and meta-analysis. J. Nutr. Health Aging 2012, 17, 447–455. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2000. [Google Scholar]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health. National Institutes of Health (NIH) Quality Assessment Tool for before-after (Pre-Post). Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 16 December 2021).
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Ashtari, F.; Ajalli, M.; Shaygannejad, V.; Akbari, M.; Hovsepian, S. The relation between Vitamin D status with fatigue and depressive symptoms of multiple sclerosis. J. Res. Med. Sci. 2013, 18, 193–197. [Google Scholar]
- Freitas, R.A.C. Clinical Correlates Of Fatigue In Multiple Sclerosis. 2017. Available online: https://repositorio-aberto.up.pt/handle/10216/104113 (accessed on 10 October 2021).
- Silva, B.; Merino, A.; Eizaguirre, B.; Yastremiz, C.; Pita, C.; Alonso, R.; Vanotti, S.; Garcea, O. Relationship between Vitamin D levels and cognitive impairment, depression and fatigue in relapsing remitting multiple sclerosis patients. Mult. Scler. J. 2016, 22, 266. [Google Scholar]
- Tiu, C.; Terecoasa, E.; Tiu, V.; Grigore, A.; Gavan, C.; Bajenaru, O. Patient-based outcome measures of the impact of disease in patients with multiple sclerosis and vitamin D deficiency. Mult. Scler. J. 2017, 23, 735–736. [Google Scholar]
- Taylor, K.L.; Hadgkiss, E.J.; Jelinek, G.A.; Weiland, T.J.; Pereira, N.G.; Marck, C.H.; van der Meer, D.M. Lifestyle factors, demographics and medications associated with depression risk in an international sample of people with multiple sclerosis. BMC Psychiatry 2014, 14, 327. [Google Scholar] [CrossRef]
- Knippenberg, S.; Bol, Y.; Damoiseaux, J.; Hupperts, R.; Smolders, J. Vitamin D status in patients with MS is negatively correlated with depression, but not with fatigue. Acta Neurol. Scand. 2010, 124, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.L.; Simpson, S., Jr.; Jelinek, G.A.; Neate, S.L.; De Livera, A.M.; Brown, C.R.; O’Kearney, E.; Marck, C.H.; Weiland, T.J. Longitudinal Associations of Modifiable Lifestyle Factors With Positive Depression-Screen Over 2.5-Years in an International Cohort of People Living With Multiple Sclerosis. Front. Psychiatry 2018, 9, 526. [Google Scholar] [CrossRef]
- Kotb, M.A.; Kamal, A.M.; Aldossary, N.M.; Bedewi, M.A. Effect of vitamin D replacement on depression in multiple sclerosis patients. Mult. Scler. Relat. Disord. 2019, 29, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Knippenberg, S.; Damoiseaux, J.; Bol, Y.; Hupperts, R.; Taylor, B.V.; Ponsonby, A.L.; Dwyer, T.; Simpson, S.; van der Mei, I.A. Higher levels of reported sun exposure, and not vitamin D status, are associated with less depressive symptoms and fatigue in multiple sclerosis. Acta Neurol. Scand. 2014, 129, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Rolf, L.; Muris, A.H.; Bol, Y.; Damoiseaux, J.; Smolders, J.; Hupperts, R. Vitamin D3 supplementation in multiple sclerosis: Symptoms and biomarkers of depression. J. Neurol. Sci. 2017, 378, 30–35. [Google Scholar] [CrossRef]
- Hanaei, S.; Sahraian, M.A.; Mohammadifar, M.; Ramagopalan, S.V.; Ghajarzadeh, M. Effect of Vitamin D Supplements on Relapse Rate and Expanded Disability Status Scale (EDSS) in Multiple Sclerosis (MS): A Systematic Review and Meta-Analysis. Int. J. Prev. Med. 2021, 12, 42. [Google Scholar] [CrossRef]
- Honarmand, K.; Feinstein, A. Validation of the Hospital Anxiety and Depression Scale for use with multiple sclerosis patients. Mult. Scler. J. 2009, 15, 1518–1524. [Google Scholar] [CrossRef]
- Maretzke, F.; Bechthold, A.; Egert, S.; Ernst, J.B.; Melo van Lent, D.; Pilz, S.; Reichrath, J.; Stangl, G.I.; Stehle, P.; Volkert, D.; et al. Role of Vitamin D in Preventing and Treating Selected Extraskeletal Diseases-An Umbrella Review. Nutrients 2020, 12, 969. [Google Scholar] [CrossRef] [Green Version]
- Geng, C.; Shaikh, A.S.; Han, W.; Chen, D.; Guo, Y.; Jiang, P. Vitamin D and depression: Mechanisms, determination and application. Asia Pac. J. Clin. Nutr. 2019, 28, 689–694. [Google Scholar] [CrossRef]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowda, U.; Mutowo, M.P.; Smith, B.J.; Wluka, A.E.; Renzaho, A.M. Vitamin D supplementation to reduce depression in adults: Meta-analysis of randomized controlled trials. Nutrients 2015, 31, 421–429. [Google Scholar] [CrossRef]
- Crupi, R.; Cambiaghi, M.; Spatz, L.; Hen, R.; Thorn, M.; Friedman, E.; Vita, G.; Battaglia, F. Reduced adult neurogenesis and altered emotional behaviors in autoimmune-prone B-cell activating factor transgenic mice. Biol. Psychiatry 2010, 67, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Crupi, R.; Cambiaghi, M.; Deckelbaum, R.; Hansen, I.; Mindes, J.; Spina, E.; Battaglia, F. n-3 fatty acids prevent impairment of neurogenesis and synaptic plasticity in B-cell activating factor (BAFF) transgenic mice. Prev. Med. 2012, 54, S103–S108. [Google Scholar] [CrossRef] [PubMed]
- Gold, S.M.; Irwin, M.R. Depression and immunity: Inflammation and depressive symptoms in multiple sclerosis. Immunol. Allergy Clin. N. Am. 2009, 29, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Shirazi, H.A.; Rasouli, J.; Ciric, B.; Rostami, A.; Zhang, G.X. 1,25-Dihydroxyvitamin D3 enhances neural stem cell proliferation and oligodendrocyte differentiation. Exp. Mol. Pathol. 2015, 98, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Björkholm, C.; Monteggia, L.M. BDNF—A key transducer of antidepressant effects. Neuropharmacology 2015, 102, 72–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuningas, M.; Mooijaart, S.P.; Jolles, J.; Slagboom, P.E.; Westendorp, R.G.; van Heemst, D. VDR gene variants associate with cognitive function and depressive symptoms in old age. Neurobiol. Aging 2009, 30, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Concerto, C.; Lanza, G.; Cantone, M.; Ferri, R.; Pennisi, G.; Bella, R.; Aguglia, E. Repetitive transcranial magnetic stimulation in patients with drug-resistant major depression: A six-month clinical follow-up study. Int. J. Psychiatry Clin. Pr. 2015, 19, 252–258. [Google Scholar] [CrossRef]
- Concerto, C.; Al Sawah, M.; Chusid, E.; Trepal, M.; Taylor, G.; Aguglia, E.; Battaglia, F. Anodal transcranial direct current stimulation for chronic pain in the elderly: A pilot study. Aging Clin. Exp. Res. 2015, 28, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhou, R.; Yang, R.; Zhang, Z.; Bai, Y.; Chang, F.; Li, L.; Sokabe, M.; Goltzman, D.; Miao, D.; et al. Abnormal neurogenesis in the dentate gyrus of adult mice lacking 1,25-dihydroxy vitamin D3 (1,25-(OH)2 D3). Hippocampus 2012, 22, 421–433. [Google Scholar] [CrossRef]
- Mineo, L.; Concerto, C.; Patel, D.; Mayorga, T.; Chusid, E.; Infortuna, C.; Aguglia, E.; Sarraf, Y.; Battaglia, F. Modulation of sensorimotor circuits during retrieval of negative Autobiographical Memories: Exploring the impact of personality dimensions. Neuropsychology 2018, 110, 190–196. [Google Scholar] [CrossRef]
- Zhang, H.; Kim, Y.; Ro, E.J.; Ho, C.; Lee, D.; Trapp, B.D.; Suh, H. Hippocampal Neurogenesis and Neural Circuit Formation in a Cuprizone-Induced Multiple Sclerosis Mouse Model. J. Neurosci. 2020, 40, 447–458. [Google Scholar] [CrossRef]
- Cambiaghi, M.; Crupi, R.; Bautista, E.L.; Elsamadisi, A.; Malik, W.; Pozdniakova, H.; Han, Z.; Buffelli, M.; Battaglia, F. The Effects of 1-Hz rTMS on Emotional Behavior and Dendritic Complexity of Mature and Newly Generated Dentate Gyrus Neurons in Male Mice. Int. J. Environ. Res. Public Health 2020, 17, 4074. [Google Scholar] [CrossRef]
- Cambiaghi, M.; Cherchi, L.; Masin, L.; Infortuna, C.; Briski, N.; Caviasco, C.; Hazaveh, S.; Han, Z.; Buffelli, M.; Battaglia, F. High-frequency repetitive transcranial magnetic stimulation enhances layer II/III morphological dendritic plasticity in mouse primary motor cortex. Behav. Brain Res. 2021, 410, 113352. [Google Scholar] [CrossRef] [PubMed]
- Infortuna, C.; Gratteri, F.; Benotakeia, A.; Patel, S.; Fleischman, A.; Muscatello, M.R.A.; Bruno, A.; Zoccali, R.A.; Chusid, E.; Han, Z.; et al. Exploring the Gender Difference and Predictors of Perceived Stress among Students Enrolled in Different Medical Programs: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 6647. [Google Scholar] [CrossRef]
- Van Heugten, C.; Köhler, S.; Francke, M.; Bol, Y. The association between executive functioning, coping styles and depressive symptoms in patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2019, 36, 101392. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year (Country) Study Design (D) Recruitment Timing (RT ) Followup (FU) Study Population Characteristics | Vitamin D Measurements | Depression Measuremnts | Other Measured Variables | Study Aim(s) Results Cofounder Quality Assessment |
|---|---|---|---|---|
| Ashtari F. et al., 2013 (Iran) D: Cross-sectional study RT: March 2011 to September 2011 FU: NR Participants: 200 Mean Age (SD): 33.5 (8.4) Female/Male: 154/46 MS Diagnosis: McDonald’s criteria Clinical status: 94% of patients have a RR MS, relapse free for more than 8 weeks prior to the study selected. | Analyzed fluid: venous blood Analythical methodology: radioimmunoassay (RIA) method using Biosource kit Vit. D concentration (nmol/L): 76 (IQR: 35.5–100.7) Vit. D status: 51.5% normal vit. D level (>75 mmol/L), 49.5% low vit. D level (<75 mmol/L) Dietary vit. D intake: NA | Evaluation of depressive symptoms: Beck Depression Inventory for Primary Care (BDI-PC) Depressive symptoms severity: 4 (3–7) in the overall sample | Sun exposure: Not Measured Fatigue Diagnosis: Fatigue Severity Scale (FFS) Degree of disability: Expanded Disability Status Score (EDSS) | Aim: To investigate the relation between vitamin D status with fatigue and depressive symptoms Results: Vitamin D status was inversely associated with depressive symptoms. Effect size: correlation, β = −0.16, p-value = 0.02 Controlled cofounders: not considered Quality asessment (NOS—cross sectional studies adaptation):Selection (max 5): 3
Outcome (max 3): 2
|
| Knippenberg et al., 2011 (The Netherlands) D: Cross-sectional study RT: 2005–2007 FU: NR Participants: 59 Mean Age (SD): 44.2 (9.2) Female/Male: 16/43 MS Diagnosis: McDonald’s criteria Clinical status: Participants had not used corticosteroids for ≥ 4 weeks and were relapse free for ≥4 weeks prior to assessment. | Analyzed fluid: serum Analythical methodology: NA Vit. D concentration (nmol/L): 62.3 (SD 27.8) Vit. D status: 23% normal vit. D level (>75 mmol/L), 73% low vit. D level (<75 mmol/L) Dietary vit. D intake: NA | Evaluation of depressive symptoms: Hospital Anxiety and Depression Scale, depression subscale (HADS-D) Depressive symptoms severity: 6.2 (SD 4.4) | Sun exposure: Not Measured Fatigue Diagnosis: Multidimensional Fatigue Inventory (MFI) Degree of disability: Expanded Disability Status Score (EDSS) | Aim: To assess whether vitamin D status contributes to the presence of depressive symptoms and fatigue in MS. Results: Vitamin D status correlated negatively with depression. In a multiple regression model, vitamin D status was not a significant contributor to depression. Effect size: correlation, β = −0.33, p-value = 0.006 Controlled cofounders: age, EDSS and MFI scors Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5): 2
Outcome (max 3): 2
|
| Silva et al., 2016 * (Argentina) D: Cross-sectional study RT: NA FU: NR Participants: 61 Mean Age (SD): 42.8 (12.4) Female/Male: 44/17 MS Diagnosis: NA Clinical Status: Relapsing Remitting MS (RRMS). | Analyzed fluid: serum Analythical methodology: chemiluminescence Vit. D mean (SD) (nmol/L): NA Vit. D status: 34% vit. D level (≤49.92 mmol/L), 66% low vit. D level (>49.92 mmol/L) Dietary vit. D intake: NA | Evaluation of depressive symptoms: Beck Depression Inventory II (BDI II). Depressive symptoms severity: NA | Sun exposure: Not Measured Neuropsychological status: Brief Repeatable Neuropsychological Battery (BNS-EM) Fatigue Diagnosis: Fatigue Severity Scale (FSS) Degree of disability: Expanded Disability Status Score (EDSS) | Aim: To evaluate the relationship between serum vitamin D levels and cognitive impairment, depression and fatigue Results: [An association between depression severity and vitamin D levels was observed (p < 0.01, X2 = 30.7). Effect size: odds ratio not reported Controlled cofounders: not considered Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5): 2
Outcome (max 3): 3
|
| Freitas et al., 2017 (Portugal) D: Cross-sectional study RT: May 2016–January 2017 FU: NR Participants: 54 (78 study participants, 24 without vit. D data) Mean Age: NA Female/Male: NA MS Diagnosis: McDonald’s criteria Clinical Status: 55% RR MS. | Analyzed fluid: serum Analythical methodology: NA Vit. D mean (SD) (nmol/L): 78.7 (SD 48.9) Vit. D status: 27.8% vit. D level deficiency (≤49.92 mmol/L), 42.6% low vit. D level (49.92–72.4 mmol/L), 29.6% normal vit. D levels (>72.4 mmol/L) Dietary vit. D intake: 34.6% were taking vit. D continuing supplement | Evaluation of depressive symptoms: Hospital Anxiety and Depression questionnaire (HADS-D) Depressive symptoms severity: NA | Sun exposure: recall questionnaire assessing daily time in sun and skin exposure (face, limbs, body) for the previous week Fatigue Diagnosis: Modified Fatigue Impact Scale (MFIS) Daytime sleepiness: Epworth Sleepiness Scale (ESS) Degree of disability: Expanded Disability Status Score (EDSS) | Aim: To evaluate the prevalence and severity of fatigue and its relationship with other clinical variables. Results: No association between 25-OH-D levels and depression. Effect size: correlation not reported Controlled cofounders: not considered Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5): 2
Outcome (max 3): 1
|
| Tiu et al., 2017 * (Romania) D: Cross-sectional Study RT: NA FU: NR Participants: 106 Mean Age (SD): 38.7 (10.1) Female/Male: 72/34 Clinical Status: patients treated with immunomodulatory drugs. | Analyzed fluid: serum Analythical methodology: chemiluminescence Vit. D mean (SD) (nmol/L): 57.9 (SD 29.5) Vit. D status: 81.1% vit. D level deficiency (≤74.9 mmol/L) Dietary vit. D intake: NA | Evaluation of depressive symptoms: Beck Depression Inventory for Primary Care (BDI-PC) Depressive symptoms severity: NA | Sun exposure: Not Measured | Aim: To investigate the relationship between vitamin D status, depression and self-reported impact of disease Results: no significant association between low vitamin D levels and depression Effect size: odds ratio not reported Controlled cofounders: not considered Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5):
Outcome (max 3): 3
|
| El Salem et al., 2021 (Jordan) D: Cross-sectional study RT: October 2018–June 2019 FU: NR Participants: 88 Mean Age (SD): 36 (10.69) Female/Male: 64/24 MS Diagnosis: 2017 revised McDonald MS diagnostic Clinical Status: Being relapse-free for 30 days prior to participation. | Analyzed fluid: blood Analythical methodology: Enzyme-Linked Immunosorbent Assay (ELISA) Vit. D mean (SD) (nmol/L): 60.2 (SD 25.9) Vit. D status: 40.9% vit. D level deficiency (≤49.9 mmol/L), 27.3% low vit. D level (49.9–74.9 mmol/L), 31.8% normal vit. D levels (>74.9 mmol/L) Dietary vit. D intake: NA | Evaluation of depressive symptoms: Hospital Anxiety and Depression Scale (HADS-D); Beck Depression Inventory-II rating scale(BDI-II) Depressive symptoms severity: HADS-D: 8.45 (SD 5.28); BDI-II: 17.93 (SD 11.82) | Sun exposure: Not Measured Degree of disability: Expanded Disability Status Score (EDSS) Perceived level of motor disability: Patient-determined disease steps (PDDS) | Aim: To evaluate vitamin D levels and its correlation with validated depression scales. Results: Serum Vit. D levels significantly correlated with scores of depression scales regardless of sex. The HADS depression score significantly correlated with serum Vit. D levels. Similarly, a significant inverse association between BDI-II score and Vit. D level was noted. Effect size: Pearson correlation coefficient, r = −0.513, p < 0.001 (for HADS), r = −0.401, p < 0.001 (for BDI-II) Controlled cofounders: age, sex, BMI, duration of disease, type of MS, and EDSS Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5): 2
Outcome (max 3): 3
|
| Taylor et al., 2014 (Australia) D: Cross-sectional study RT: NA FU: NR Participants: 2225 Median Age (IQR): 45 (38–53) Female/Male: 388/1813 MS Diagnosis: self-report Clinical Status: Being relapse-free for 30 days prior to participation, the majority (61.3%) had RR MS. | Analyzed fluid: not measured Analythical methodology: NA Vit. D mean (SD) (nmol/L): NA Vit. D status: NA Dietary vit. D intake: 30.1% no daily vit. D consumption, 17.4% 1–5000 IU daily vit. D consumption, >5000 IU vit. D consumption. | Evaluation of depressive symptoms: Patient Health Questionnaire depression module short version (PHQ-2) Depressive symptoms severity: NA | Sun exposure: Not Measured Fatigue Diagnosis: The Fatigue Severity Scale (FSS) Perceived level of disability: Patient-determined disease steps (PDDS) Habits Description: Diet Habits Questionnaire (DHQ) removed four items assessing salt use and alcohol intake; International Physical Activity Questionnaire (IPAQ) Comorbidities Assessment: Self-Administered Comorbidity Questionnaire (SCQ) | Aim: To examine depression and its association with modifiable lifestyle risk factors In the lifestyle factors: Vitamin D supplementation. Results: Taking any vitamin D supplement was associated with lower odds of screening positive for depression, but taking at least 5000 IU daily was associated with the greatest odds. Effect size: adjusted odds ratio 0.57 (0.43–0.77) for 1–5000 IU, 0.47 (0.32–0.70) for >5000 IU. Controlled cofounders: years since diagnosis, number of comorbidities, level of disability, clinically significant fatigue, age, gender, marital status and level of education. Quality asessment (NOS—cross sectional studies adaptation): Selection (max 5): 2
Outcome (max 3): 2
|
| Kotb et al., 2019 (Saudi Arabia) D: Prospective cohort study RT: 5 years (2013–2018) FU: All patients were regularly followed up every 2 months for 25-OH-D serum levels. EDSS scores and BDI scores. Participants: 35 Mean Age (SD): 27 (4). Female/Male: 19/16 MS: Diagnosis: McDonald’s criteria Clinical Status: Clinical Status: Being relapse-free for 30 days prior to participation, not receiving any corticosteroid therapy within four weeks prior to recruitment. | Analyzed fluid: serum Analythical methodology: NA Vit. D mean (SD) (nmol/L): baseline 23.4 (SD 9.8); endpoint 86.3 (SD 7.3) Vit. D status: NA Dietary vit. D intake: daily intake 1000 IU, for 3 months NB: patients with current MS treatment other than interferon, received high-dose vitamin D (daily intake 1000 IU) before inclusion to the study. | Evaluation of depressive symptoms: Beck Depression Inventory (BDI) Depressive symptoms severity: baseline 21.3 (SD 3.4); endpoint 16.8 (SD 2.9) | Sun exposure: Not Measured Degree of disability: Expanded Disability Status Score (EDSS) | Aim: evaluate the relation between vitamin D levels and depression scores, and the effect of vitamin D replacement on the depressive symptoms in patients with MS. Results: A significant negative correlation was observed between vitamin 25 (OH) D levels and Beck’s depression inventory scores at baseline (p < 0.001), eighth, tenth, and twelfth month (p = 0.001). Effect size: Pearson correlation coefficient r = −0.432 (p-value = 0.011) Controlled cofounders: EDSS Quality assessment (NIH quality assessment tool for before-after (Pre-Post) study with no control group):
|
| Taylor et al., 2018 (Australia) SD: Retrospective cohort study RT: NA FU: 2.5 years Participants: 1401 Mean Age (SD): 48.4 (10.5) Female/Male: 1150/241 Diagnosis MS: Clinical Status: Being relapse-free for 30 days prior to participation, the majority (59.3%) had RR MS. | Analyzed fluid: NA Analythical methodology: NA Vit. D mean (SD) (nmol/L): NA Vit. D status: NA Dietary vit. D intake: Vitamin D supplementation self-reported. | Evaluation of depressive symptoms: patient Health Questionnaire-2 (PHQ-2) at baseline, and Patient Health Questionnaire-9 (PHQ-9) at follow-up Depressive symptoms severity: NA | Sun exposure: Not Measured Fatigue Diagnosis: The Fatigue Severity Scale (FSS) Perceived level of disability: Patient-determined disease steps (PDDS) Habits Description: Diet Habits Questionnaire (DHQ) removed four items assessing salt use and alcohol intake; International Physical Activity Questionnaire (IPAQ) Severity of disease: Patient Determined Multiple Sclerosis Severity Score (P-MSSS) | Aim: Evaluating whether modifiable lifestyle factors were associated with screening positive for depression 2.5 years after our baseline study and the predictors of change in depression screen during follow-up. In the lifestyle factors: Vit D supplementation. Results: Vitamin D supplementation was associated with lower frequencies of depression risk by both PHQ-2 and PHQ-9. Effect size: adjusted odds ratio 0.70 (0.56–0.87) (p-value = 0.002) Controlled cofounders: age, P-MSSS, FSS, and use of antidepressant medication Quality assessment (NOS): Selection (max 4): 3
Outcome (max 3): 2
|
| Knippenberg et al., 2013 (The Netherlands) D: Prospective longitudinal study RT: (2002–2005) FU: 2.3 years Participants: 198 Mean Age (SD): 48.2 (11.4) Female/Male: 137/ 61 Diagnosis MS: McDonald’s criteria Clinical Status: Being relapse-free for 30 days prior to participation, 75.3% have RR MS. | Analyzed fluid: serum Analythical methodology: radioimmunoassay Vit. D mean (SD) (nmol/L): Summer 65,5 (SD 25,2); Winter 39.2 (SD 14.4) Vit. D status: NA Dietary vit. D intake: categorized as none, 0–200 IU/day, 201–750 IU/day. | Evaluation of depressive symptoms: Hospital Anxiety and Depression Scale (HADS-D) Depressive symptoms severity: NA | Sun exposure: Not Measured Fatigue Diagnosis: The Fatigue Severity Scale (FSS) Degree of disability: Expanded Disability Status Score (EDSS) Cognitive Performance: 3-s Paced Auditory Serial Addition Test (PASAT-3) | Aim: Examining the associations between personal sun exposure and serum 25- hydroxyvitamin D (25(OH)D), and depression, anxiety, fatigue and cognition. Results: 25(OH)D levels were not associated with depression scores. Higher levels of reported personal sun exposure in the current season were associated with lower depression score. Effect size: correlation, β = −0.05 (−0.12–0.02) (p-value = 0.186) Controlled cofounders: sex, age, initial EDSS score, initial disease duration, immunomodulatory therapies, BMI and season Quality assessment (NOS): Selection (max 4): 2
Outcome (max 3): 2
|
| Rolf et al., 2017 (The Netherlands) D: Randomized Placebo controlled trial (RCT) RT: FU: 48 weeks Participants: 40 (20 with vitD; 20 with Placebo) Female/Male: 26/14 (VitD 12/8; Placebo 14/6) Mean Age (SD): VitD 37.6 (9.6); placebo 38.5 (7.8) Diagnosis MS: McDonald’s criteria Clinical Status: Being relapse-free for 30 days prior to participation, having had their first clinical event in the previous 5 years, not active in the 30 days prior to inclusion, RR MS, treated with interferon-β1α. | Analyzed fluid: serum Analythical methodology: radioimmunoassay Vit. D median (Q1–Q3) (nmol/L): baseline control 53 (Q1-Q3 43–63), baseline case 58 (Q1–Q3 38–82); endpoint: control 61 (44–84), case 226 (159–250) Vit. D status: NA Dietary vit. D intake: NA NB: D3 supplementation in the vit D group cholecalciferol dosed at 7000 IU/day in the first 4 week, followed by 14,000 IU/day up to endpoint. | Evaluation of depressive symptoms: Hospital Anxiety and Depression Scale (HADS-D) Depressive symptoms severity: baseline control 3.0 (Q1–Q3 2.0–7.0), baseline case 4.0 (Q1–Q3 2.0–5.0) | Sun exposure: participants quantified how much time they spent in the sun during weekends and holidays in the current and preceding 3-month intervals using validated questions Fatigue Diagnosis: The Fatigue Severity Scale (FSS) Inflammation Status: assessment of TNFα and IL-10 concentrations | Aim: Exploring the effect of high dose vitamin D3 supplementation on depressive symptoms in MS. Fatigue was assessed as a potential confounder. Results: High dose vitamin D supplementation does not decrease depression and fatigue scores. Effect size: non significant, effect size not reported Controlled cofounders: HADS-D at baseline and FSS at T1 Quality assessment (Cochrane Risk of Bias 2.0): Randomization process: Some concerns Deviations from intended interventions: High risk Mising outcome data: Some concerns Measurement of the outcome: High risk Selection of the reported result: Some concerns Overall Bias: High risk |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Concerto, C.; Rodolico, A.; Ciancio, A.; Messina, C.; Natale, A.; Mineo, L.; Battaglia, F.; Aguglia, E. Vitamin D and Depressive Symptoms in Adults with Multiple Sclerosis: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 199. https://doi.org/10.3390/ijerph19010199
Concerto C, Rodolico A, Ciancio A, Messina C, Natale A, Mineo L, Battaglia F, Aguglia E. Vitamin D and Depressive Symptoms in Adults with Multiple Sclerosis: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(1):199. https://doi.org/10.3390/ijerph19010199
Chicago/Turabian StyleConcerto, Carmen, Alessandro Rodolico, Alessia Ciancio, Christian Messina, Antimo Natale, Ludovico Mineo, Fortunato Battaglia, and Eugenio Aguglia. 2022. "Vitamin D and Depressive Symptoms in Adults with Multiple Sclerosis: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 1: 199. https://doi.org/10.3390/ijerph19010199
APA StyleConcerto, C., Rodolico, A., Ciancio, A., Messina, C., Natale, A., Mineo, L., Battaglia, F., & Aguglia, E. (2022). Vitamin D and Depressive Symptoms in Adults with Multiple Sclerosis: A Scoping Review. International Journal of Environmental Research and Public Health, 19(1), 199. https://doi.org/10.3390/ijerph19010199