
Twenty-Four Week, Randomized, Double-Blind, Placebo-Controlled Trial of Metformin for Antipsychotic-Induced Weight Gain in Patients with First-Episode Psychosis: A Pilot Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Procedures
2.4. Assessments
2.5. Outcomes
2.6. Statistical Analysis
3. Results
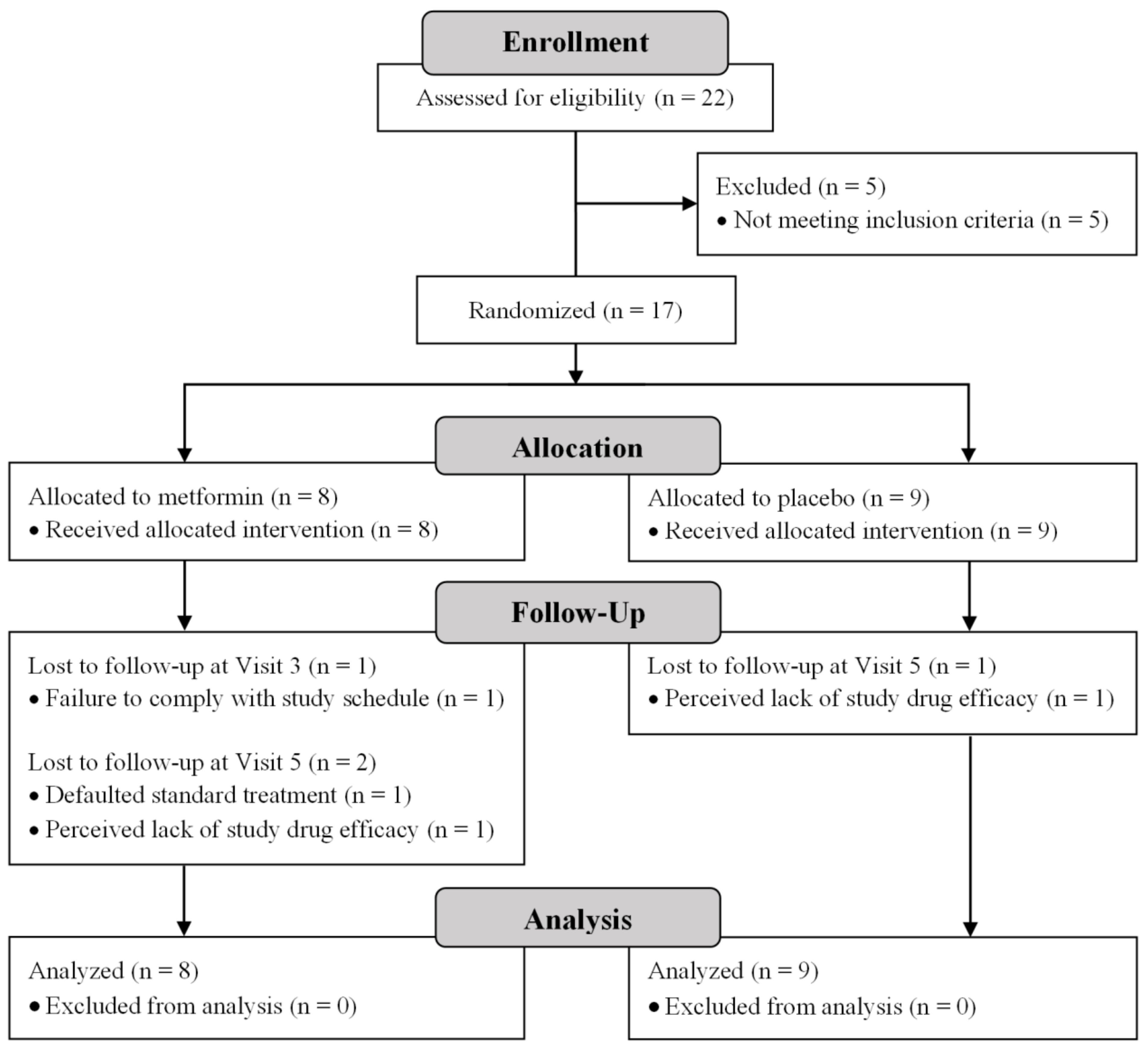
3.1. Participants
3.2. Safety and Tolerability
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perkins, D.O.; Gu, H.; Boteva, K.; Lieberman, J.A. Relationship between duration of untreated psychosis and outcome in first-episode schizophrenia: A critical review and meta-analysis. Am. J. Psychiatry 2005, 162, 1785–1804. [Google Scholar] [CrossRef]
- Robinson, D.G.; Woerner, M.G.; Alvir, J.M.J.; Geisler, S.; Koreen, A.; Sheitman, B.; Chakos, M.; Mayerhoff, D.; Bilder, R.; Goldman, R.; et al. Predictors of treatment response from a first episode of schizophrenia or schizoaffective disorder. Am. J. Psychiatry 1999, 156, 544–549. [Google Scholar] [CrossRef]
- Bak, M.; Drukker, M.; Cortenraad, S.; Vandenberk, E.; Guloksuz, S. Antipsychotics result in more weight gain in antipsychotic naive patients than in patients after antipsychotic switch and weight gain is irrespective of psychiatric diagnosis: A meta-analysis. PLoS ONE 2021, 16, e0244944. [Google Scholar] [CrossRef] [PubMed]
- Grajales, D.; Ferreira, V.; Valverde, Á.M. Second Generation Antipsychotics and Dysregulation of Glucose Metabolism: Beyond Weight Gain. Cells 2019, 8, 1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, D.B.; Mentore, J.L.; Heo, M.; Chandler, L.P.; Cappelleri, J.C.; Infante, M.C.; Weiden, P.J. Antipsychotic-Induced Weight Gain: A Comprehensive Research Synthesis. Am. J. Psychiatry 1999, 156, 1686–1696. [Google Scholar] [PubMed]
- Perkins, D.O.; Gu, H.; Weiden, P.J.; McEvoy, J.P.; Hamer, R.M.; Lieberman, J.A. Predictors of treatment discontinuation and medication nonadherence in patients recovering from a first episode of schizophrenia, schizophreniform disorder, or schizoaffective disorder: A randomized, double-blind, flexible-dose, multicenter study. J. Clin. Psychiatry 2008, 69, 106–113. [Google Scholar] [CrossRef]
- Tiihonen, J.; Lönnqvist, J.; Wahlbeck, K.; Klaukka, T.; Niskanen, L.; Tanskanen, A.; Haukka, J. 11-year follow-up of mortality in patients with schizophrenia: A population-based cohort study (FIN11 study). Lancet 2009, 374, 620–627. [Google Scholar] [CrossRef]
- Firth, J.; Siddiqi, N.; Koyanagi, A.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F.; et al. The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019, 6, 675–712. [Google Scholar] [CrossRef] [Green Version]
- Verma, S.K.; Liew, A.; Subramaniam, M.; Poon, L.Y. Effect of treatment on weight gain and metabolic abnormalities in patients with first-episode psychosis. Aust. N. Z. J. Psychiatry 2009, 43, 812–817. [Google Scholar] [CrossRef]
- Verma, S.K.; Subramaniam, M.; Liew, A.; Poon, L.Y. Metabolic risk factors in drug-naive patients with first-episode psychosis. J. Clin. Psychiatry 2009, 70, 997–1000. [Google Scholar] [CrossRef]
- Awad, A.G.; Voruganti, L.N.P. Body weight, image and self-esteem evaluation questionnaire: Development and validation of a new scale. Schizophr. Res. 2004, 70, 63–67. [Google Scholar] [CrossRef]
- Dayabandara, M.; Hanwella, R.; Ratnatunga, S.; Seneviratne, S.; Suraweera, C.; de Silva, V.A. Antipsychotic-associated weight gain: Management strategies and impact on treatment adherence. Neuropsychiatr. Dis. Treat. 2017, 13, 2231–2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiden, P.J. Switching Antispcyhotic Medications: Not Enough, Too Often, or Just Right? Am. J. Psychiatry 2011, 168, 882–884. [Google Scholar] [CrossRef]
- Hasnain, M.; Fredrickson, S.K.; Vieweg, W.V.R. Metformin for obesity and glucose dysregulation in patients with schizophrenia receiving antipsychotic drugs. J. Psychopharmacol. 2011, 25, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.I.G.; Gossage-Worrall, R.; Hind, D.; Bradburn, M.J.; McCrone, P.; Morris, T.; Edwardson, C.; Barnard, K.; Carey, M.E.; Davies, M.J.; et al. Structured lifestyle education for people with schizophrenia, schizoaffective disorder and first-episode psychosis (STEPWISE): Randomised controlled trial. Br. J. Psychiatry 2019, 214, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.H.; Mackin, P.; Chaudhry, I.; Farooqi, A.; Gadsby, R.; Heald, A.; Hill, J.; Millar, H.; Peveler, R.; Rees, R.; et al. Minimising metabolic and cardiovascular risk in schizophrenia: Diabetes, obesity and dyslipidaemia. J. Psychopharmacol. 2007, 21, 357–373. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Massey, S.; Story, D.; Li, L. Metformin: An old drug with new applications. Int. J. Mol. Sci. 2018, 19, 2863. [Google Scholar] [CrossRef] [Green Version]
- Hundal, R.S.; Inzucchi, S.E. Metformin: New understandings, new uses. Drugs 2003, 63, 1879–1894. [Google Scholar] [CrossRef] [PubMed]
- Kirpichnikov, D.; Mcfarlane, S.I.; Sowers, J.R. Metformin: An Update. Ann. Intern. Med. 2002, 137, 25–33. [Google Scholar] [CrossRef]
- Mannucci, E.; Ognibene, A.; Cremasco, F.; Bardini, G.; Mencucci, A.; Pierazzuoli, E.; Ciani, S.; Messeri, G.; Rotella, C.M. Effect of metformin on glucagon-like peptide 1 (GLP-1) and leptin levels in obese nondiabetic subjects. Diabetes Care 2001, 24, 489–494. [Google Scholar] [CrossRef] [Green Version]
- Correll, C.U.; Sikich, L.; Reeves, G.; Riddle, M. Metformin for antipsychotic-related weight gain and metabolic abnormalities: When, for whom, and for how long? Am. J. Psychiatry 2013, 170, 947–952. [Google Scholar] [CrossRef]
- Wu, R.R.; Zhao, J.P.; Jin, H.; Shao, P.; Fang, M.S.; Guo, X.F.; He, Y.Q.; Liu, Y.J.; Chen, J.D.; Li, L.H. Lifestyle Intervention and Metformin for Treatment of Antipsychotic-Induced Weight Gain: A Randomized Controlled Trial. JAMA 2008, 299, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Björkhem-Bergman, L.; Asplund, A.B.; Lindh, J.D. Metformin for weight reduction in non-diabetic patients on antipsychotic drugs: A systematic review and meta-analysis. J. Psychopharmacol. 2011, 25, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Maayan, L.; Vakhrusheva, J.; Correll, C.U. Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: A systematic review and meta-analysis. Neuropsychopharmacology 2010, 35, 1520–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Silva, V.A.; Suraweera, C.; Ratnatunga, S.S.; Dayabandara, M.; Wanniarachchi, N.; Hanwella, R. Metformin in prevention and treatment of antipsychotic induced weight gain: A systematic review and meta-analysis. BMC Psychiatry 2016, 16, 341. [Google Scholar] [CrossRef] [Green Version]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV); American Psychiatric Press: Washington, DC, USA, 1997. [Google Scholar]
- Guy, W. ECDEU Assessment Manual for Psychopharmacology; U.S. Department of Health, Education, and Welfare: Rockville, MD, USA, 1976.
- Overall, J.E.; Tex, G.; Hollister, L.E.; Alto, P.; Pichot, P. Major Psychiatric Disorders: A Four-Dimensional Model. Arch. Gen. Psychiatry 1967, 16, 146–151. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Board. Report of the National Nutrition Survey 2004; Health Promotion Board: Singapore, 2005. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Shafer, A. Meta-analysis of the brief psychiatric rating scale factor structure. Psychol. Assess. 2005, 17, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Startup, M.; Jackson, M.C.; Bendix, S. The concurrent validity of the Global Assessment of Functioning (GAF). Br. J. Clin. Psychol. 2002, 41, 417–422. [Google Scholar] [CrossRef]
- Beard, C.; Hsu, K.J.; Rifkin, L.S.; Busch, A.B.; Björgvinsson, T. Validation of the PHQ-9 in a psychiatric sample. J. Affect. Disord. 2016, 193, 267–273. [Google Scholar] [CrossRef]
- Kim, Y.; Park, I.; Kang, M. Convergent validity of the International Physical Activity Questionnaire (IPAQ): Meta-analysis. Public Health Nutr. 2013, 16, 440–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; De Hert, M.; Myin-Germeys, I.; Rosenbaum, S.; Stubbs, B.; Van Damme, T.; Probst, M. Validity and correlates of the International Physical Activity Questionnaire in first-episode psychosis. Early Interv. Psychiatry 2017, 562–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wantland, D.J.; Holzemer, W.L.; Moezzi, S.; Willard, S.S.; Arudo, J.; Kirksey, K.M.; Portillo, C.J.; Corless, I.B.; Rosa, M.E.; Robinson, L.L.; et al. A Randomized Controlled Trial Testing the Efficacy of an HIV/AIDS Symptom Management Manual. J. Pain Symptom Manag. 2008, 36, 235–246. [Google Scholar] [CrossRef]
- Prince, S.A.; Cardilli, L.; Reed, J.L.; Saunders, T.J.; Kite, C.; Douillette, K.; Fournier, K.; Buckley, J.P. A comparison of self-reported and device measured sedentary behaviour in adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 31. [Google Scholar] [CrossRef]
- Celis-Morales, C.A.; Perez-Bravo, F.; Ibañez, L.; Salas, C.; Bailey, M.E.S.; Gill, J.M.R. Objective vs. self-reported physical activity and sedentary time: Effects of measurement method on relationships with risk biomarkers. PLoS ONE 2012, 7, e36345. [Google Scholar] [CrossRef]

{kind=link}
| Screening Phase | Intervention Phase | Discontinuation Phase | Early Termination | |||||
|---|---|---|---|---|---|---|---|---|
| Visit | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Week | −1 | 0 | 3 | 6 | 12 | 24 | 36 | |
| Procedures/Assessments | ||||||||
| Informed consent | 🗸 | |||||||
| Sociodemographic and clinical characteristics | 🗸 | |||||||
| Concomitant medication(s) review | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Anthropometric measurements: Body weight (kg); height (m); body mass index (kg/m2); waist circumference (cm) | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 |
| Vital signs: Systolic and diastolic blood pressure (mmHg); pulse rate (bpm) | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | |
| Physical examination | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | ||
| 12-lead electrocardiogram | 🗸 | 🗸 | 🗸 | |||||
| Serum pregnancy test (for females of childbearing potential only) | 🗸 | 🗸 | 🗸 | |||||
| Laboratory blood tests: Serum creatinine and estimated glomerular filtration rate; serum insulin; lactic acid level; liver function test; serum fasting glucose | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Thyroid Function Test | 🗸 | |||||||
| Hemoglobin A1c (HbA1c) | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Total cholesterol, high-density and low-density lipoprotein, triglycerides | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Clinician-rated questionnaires: BPRS; GAF | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Participant-rated questionnaires: PHQ-9; DPQ; IPAQ | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Randomization | 🗸 | |||||||
| Study drug dispensed | 🗸 | 🗸 | 🗸 | 🗸 | ||||
| Adverse events monitoring | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | |||
| Drug accountability and adherence check | 🗸 | 🗸 | 🗸 | 🗸 | 🗸 | |||
| Metformin (n = 8) | Placebo (n = 9) | p-Value | |
|---|---|---|---|
| Age—years, mean (SD) | 25.0 (3.9) | 24.0 (6.0) | 0.593 |
| Gender—no. (%) | |||
| - Male - Female | 4 (50.0) 4 (50.0) | 5 (55.6) 4 (44.4) | 0.819 |
| Ethnicity—no. (%) | |||
| - Chinese - Malay - Indian - Others | 4 (50.0) 1 (12.5) 1 (12.5) 2 (25.0) | 6 (66.7) 2 (22.2) 1 (11.1) 0 (0.0) | 0.443 |
| Diagnosis—no. (%) | |||
| - Schizophrenia - Schizophreniform disorder - Schizoaffective disorder - Psychotic disorder not otherwise specified - Mood disorders with psychotic features | 5 (62.5) 1 (12.5) 2 (25.0) 0 (0.0) 0 (0.0) | 4 (44.4) 1 (11.1) 1 (11.1) 1 (11.1) 2 (22.2) | 0.494 |
| Body weight—kg, mean (SD) | 82.3 (17.1) | 87.1 (11.5) | 0.471 |
| Height—m, mean (SD) | 1.7 (0.1) | 1.7 (0.1) | 0.413 |
| Body mass index—kg/m2, mean (SD) | 27.9 (6.4) | 30.7 (4.8) | 0.229 |
| Waist circumference—cm, mean (SD) | 94.9 (11.2) | 97.2 (9.1) | 0.596 |
| Systolic blood pressure—mmHg, mean (SD) | 116.3 (11.3) | 119.6 (13.6) | 0.500 |
| Diastolic blood pressure—mmHg, mean (SD) | 73.9 (8.2) | 63.2 (9.0) | 0.030 * |
| Pulse rate—bpm, mean (SD) | 78.9 (20.0) | 86.7 (11.1) | 0.163 |
| Concurrent medications—no. (%) | |||
| - Typical antipsychotics | |||
| Flupentixol | 1 (12.5) | 2 (22.2) | |
| - Atypical antipsychotics | |||
| Amisulpride Aripiprazole Clozapine Olanzapine Paliperidone Risperidone | 1 (12.5) 1 (12.5) 0 (0.0) 0 (0.0) 2 (25.0) 3 (37.5) | 0 (0.0) 2 (22.2) 1 (11.1) 1 (11.1) 1 (11.1) 3 (33.3) | - |
| - Anticholinergics - Antidepressants - Mood stabilizers - Benzodiazepines | 1 (12.5) 2 (25.0) 2 (25.0) 0 (0.0) | 0 (0.0) 3 (33.3) 1 (11.1) 1 (11.1) |
| Visit 1 Week −1 (Metformin n = 8; Placebo n = 9) | Visit 2 Week 0 (Metformin n = 8; Placebo n = 9) | Visit 3 Week 3 (Metformin n = 7; Placebo n = 9) | Visit 4 Week 6 (Metformin n = 7; Placebo n = 9) | Visit 5 Week 12 (Metformin n = 7; Placebo n = 9) | Visit 6 Week 24 (Metformin n = 5; Placebo n = 8) | Visit 7 Week 36 (Metformin n = 5; Placebo n = 8) | |
|---|---|---|---|---|---|---|---|
| Weight—kg Metformin Placebo | 82.3 (17.1) 87.1 (11.5) | 82.6 (17.3) 87.5 (11.7) | 82.4 (18.9) 88.2 (11.7) | 82.6 (18.9) 89.0 (11.5) | 81.6 (19.5) 90.2 (12.0) | 84.8 (21.6) 90.7 (13.9) | 85.9 (22.2) 92.3 (13.3) |
| BMI—kg/m2 Metformin Placebo | 27.9 (6.4) 30.7 (4.8) | 28.2 (6.5) 30.9 (4.7) | 27.6 (7.3) 31.2 (4.5) | 27.6 (7.0) 31.5 (4.7) | 27.3 (6.9) 31.8 (5.0) | 28.7 (8.0) 31.0 (4.6) | 28.9 (8.0) 31.7 (5.1) |
| Waist circumference—cm Metformin Placebo | 94.9 (11.2) 97.2 (9.1) | 95.5 (11.2) 99.6 (9.0) | 96.6 (14.8) 99.6 (7.7) | 93.3 (13.7) 101.0 (8.8) | 95.3 (13.5) 100.7 (9.8) | 95.6 (14.5) 101.1 (9.8) | 96.4 (19.9) 98.8 (14.0) |
| Systolic BP—mmHg Metformin Placebo | 116.3 (11.3) 119.6 (13.6) | 111.9 (13.5) 120.1 (12.4) | 117.7 (18.3) 117.4 (14.4) | 116.7 (17.5) 120.0 (15.2) | 119.7 (14.4) 116.4 (9.1) | 112.2 (23.2) 121.6 (12.5) | - |
| Diastolic BP—mmHg Metformin Placebo | 73.9 (8.2) 63.2 (9.0) | 64.3 (7.8) 68.1 (9.6) | 69.6 (12.1) 70.9 (9.5) | 68.7 (10.3) 69.0 (11.5) | 70.1 (10.5) 67.8 (7.3) | 62.2 (11.4) 67.9 (6.6) | - |
| Pulse rate—bpm Metformin Placebo | 78.9 (20.0) 86.7 (11.1) | 82.0 (14.9) 90.3 (14.2) | 76.9 (9.2) 93.1 (15.9) | 77.0 (5.2) 89.6 (18.1) | 82.1 (9.1) 88.0 (17.3) | 75.2 (13.7) 82.4 (14.9) | - |
| BPRS total score Metformin Placebo | - | 22.8 (4.1) 24.4 (3.5) | - | - | - | 21.0 (2.6) 23.3 (4.5) | 22.6 (4.7) 20.3 (3.8) |
| GAF score Metformin Placebo | - | 71.5 (6.0) 70.7 (3.0) | - | - | - | 76.5 (10.8) 77.4 (8.0) | 75.2 (11.1) 81.4 (8.3) |
| PHQ-9 total score Metformin Placebo | - | 2.9 (2.5) 6.4 (4.3) | - | - | - | 3.8 (3.0) 5.0 (5.6) | 3.8 (3.8) 6.3 (4.4) |
| Fasting glucose—mmol/L Metformin Placebo | 4.6 (0.3) 4.7 (0.2) | - | - | - | 4.6 (0.3) 4.9 (0.4) | 4.5 (0.2) 5.0 (0.6) | - |
| Serum insulin—mU/L Metformin Placebo | 11.0 (4.6) 16.6 (11.6) | - | - | - | 17.8 (12.5) 17.6 (13.6) | 10.3 (10.3) 24.3 (25.1) | - |
| Triglycerides—mmol/L Metformin Placebo | 1.6 (1.0) 1.9 (1.0) | - | - | - | 1.6 (1.0) 1.8 (1.0) | 1.0 (0.4) 2.4 (1.7) | - |
| Total cholesterol—mmol/L Metformin Placebo | 4.7 (0.7) 5.1 (0.7) | - | - | - | 4.4 (1.0) 5.1 (1.2) | 4.6 (1.4) 5.2 (1.2) | - |
| HDL cholesterol—mmol/L Metformin Placebo | 1.1 (0.2) 1.2 (0.3) | - | - | - | 1.1 (0.1) 1.1 (0.3) | 1.2 (0.3) 1.0 (0.2) | - |
| LDL cholesterol—mmol/L Metformin Placebo | 2.9 (0.6) 3.4 (0.9) | - | - | - | 2.6 (0.6) 3.2 (0.9) | 2.8 (1.2) 3.1 (0.8) | - |
| Serum creatinine—µmol/L Metformin Placebo | 73.6 (14.4) 67.4 (14.1) | - | - | - | 72.4 (11.2) 67.2 (12.1) | 66.6 (12.0) 73.1 (13.0) | - |
| Lactic acid—mmol/L Metformin Placebo | 1.5 (0.7) 1.7 (0.7) | - | - | - | 1.4 (0.4) 1.5 (0.5) | 1.4 (0.3) 1.5 (0.4) | - |
| AST—U/L Metformin Placebo | 29.5 (16.5) 27.7 (7.2) | - | - | - | 28.0 (12.8) 31.7 (13.8) | 47.2 (51.6) 32.8 (16.1) | - |
| ALT—U/L Metformin Placebo | 41.8 (38.0) 34.3 (19.4) | - | - | - | 41.3 (24.9) 49.8 (50.5) | 86.8 (127.1) 50.5 (58.0) | - |
| HbA1c—% Metformin Placebo | 5.2 (0.5) 5.3 (0.3) | - | - | - | 5.1 (0.2) 5.5 (0.6) | 5.0 (0.4) 5.6 (0.7) | - |
| Mixed Model Fixed Effects (Intervention Phase) | Unconditional Means Model: Model A | Unconditional Growth Model: Model B | Growth Model: Model C |
|---|---|---|---|
| Initial status—Intercept (Status error SE) | 86.0 (3.6) ** | 84.8 (3.4) ** | 86.3 (4.8) ** |
| Initial status—Intervention/control | −3.0 (7.0) | ||
| Rate of change—Intercept | 0.4 (0.2) | 0.8 (0.2) ** | |
| Rate of change—Intervention/control | −1.2 (0.5) ** | ||
| Variance components | |||
| - Level 1 Within person | 3.6 (0.7) ** | 1.2 (0.3) ** | 1.2 (0.2) ** |
| - Level 2 In initial status | 216.3 (76.7) ** | 200.2 (71.2) ** | 210.0 (77.1) ** |
| - Level 2 In rate of change | 1.1 (0.5) ** | 0.7 (0.3) * | |
| Pseudo R2 statistics | |||
| - Level 1 Within person | 0.7 | ||
| - Level 2 Rate of change | 0.3 | ||
| Goodness of fit | |||
| - −2 Res Log Likelihood | 411.1 | 378.7 | 366.2 |
| - AIC | 415.1 | 384.7 | 372.2 |
| - BIC | 416.7 | 387.2 | 374.7 |
| RMANOVA (Intervention phase) | F value (df) | ||
| Within Subjects | 0.659 (1.8) a | ||
| Between Groups | 0.108 (1) | ||
| Group × Time Effect | 4.780 (1.8) a* | ||
| RMANOVA (Discontinuation phase) | Fvalue (df) | ||
| Within Subjects | 3.974 (1) | ||
| Between Groups | 0.407 (1) | ||
| Group × Time Effect | 0.124 (1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, C.; Chua, Y.C.; Abdin, E.; Subramaniam, M.; Verma, S. Twenty-Four Week, Randomized, Double-Blind, Placebo-Controlled Trial of Metformin for Antipsychotic-Induced Weight Gain in Patients with First-Episode Psychosis: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 137. https://doi.org/10.3390/ijerph19010137
Tang C, Chua YC, Abdin E, Subramaniam M, Verma S. Twenty-Four Week, Randomized, Double-Blind, Placebo-Controlled Trial of Metformin for Antipsychotic-Induced Weight Gain in Patients with First-Episode Psychosis: A Pilot Study. International Journal of Environmental Research and Public Health. 2022; 19(1):137. https://doi.org/10.3390/ijerph19010137
Chicago/Turabian StyleTang, Charmaine, Yi Chian Chua, Edimansyah Abdin, Mythily Subramaniam, and Swapna Verma. 2022. "Twenty-Four Week, Randomized, Double-Blind, Placebo-Controlled Trial of Metformin for Antipsychotic-Induced Weight Gain in Patients with First-Episode Psychosis: A Pilot Study" International Journal of Environmental Research and Public Health 19, no. 1: 137. https://doi.org/10.3390/ijerph19010137
APA StyleTang, C., Chua, Y. C., Abdin, E., Subramaniam, M., & Verma, S. (2022). Twenty-Four Week, Randomized, Double-Blind, Placebo-Controlled Trial of Metformin for Antipsychotic-Induced Weight Gain in Patients with First-Episode Psychosis: A Pilot Study. International Journal of Environmental Research and Public Health, 19(1), 137. https://doi.org/10.3390/ijerph19010137