
Developing and Evaluating a Continuous Education Program for Healthcare Assistants in Macao: A Cluster-Randomized Trial


Abstract
1. Introduction
1.1. Literature Review
1.1.1. Overview of Health Auxiliary Training
1.1.2. Healthcare Assistants in Macao
2. Materials and Methods
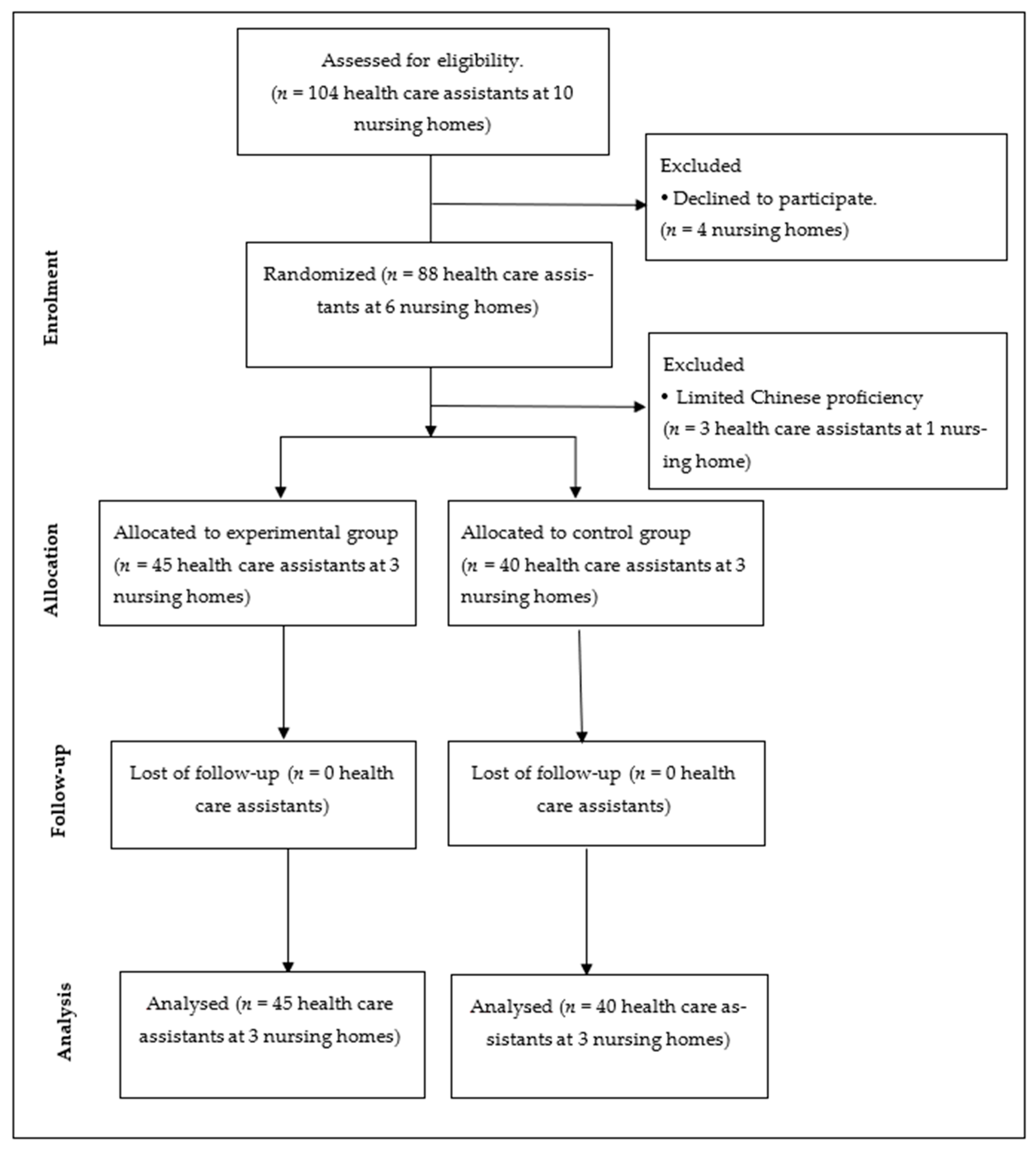
2.1. Participants
2.2. Continuous Education Program
2.3. Instruments
2.3.1. Demographic Data
2.3.2. Healthcare Assistants Care Knowledge Test
2.3.3. Healthcare Assistants Care Competence Self-Assessment
2.4. Sample Size
2.5. Data Analysis
2.6. Ethics Consideration
3. Results
3.1. Demographic Data
3.2. Descriptive Statistics
3.3. Inferential Statistics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- A Universal Truth: No Health without a Workforce. Available online: https://www.who.int/workforcealliance/knowledge/resources/GHWA-a_universal_truth_report.pdf?ua=1 (accessed on 10 March 2021).
- Buchan, J.; Poz, M.R. Skill mix in the healthcare workforce: Reviewing the evidence. Bull. World Health Organ. 2002, 80, 575–580. [Google Scholar] [PubMed]
- WHO Recommendations Optimizing Health Worker Roles to Improve Access to Key Maternal and New Born Health Interventions through Task Shifting. Available online: http://apps.who.int/iris/bitstream/10665/77764/1/9789241504843_eng.pdf (accessed on 10 March 2021).
- Policy on Assistants in Nursing. Available online: http://www.nswnma.asn.au/wp-content/uploads/2013/07/NSWNMA-Policy-on-Assistants-in-Nursing.pdf (accessed on 10 March 2021).
- Stute, M.; Hurwood, A.; Hulcombe, J.; Kuipers, P. Pilot implementation of allied health assistant roles within publicly funded health services in Queensland, Australia: Results of a workplace audit. BMC Health Serv. Res. 2014, 14, 258. [Google Scholar] [CrossRef] [PubMed]
- State Nurse Aide Training: Program Information and Data. Available online: http://www.canhr.org/reports/2002/oei-05-01-00030.pdf (accessed on 10 March 2021).
- Community Services and Health Industry Skills Council of Commonwealth of Australia: Certificate III in Health Services Assistance. Available online: https://training.gov.au/Training/Details/HLT33115# (accessed on 10 March 2021).
- Fletcher, M. Continuing education for healthcare professionals: Time to prove its worth. PriMarch y Care Respir. J. 2007, 16, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Continuing Education for Health. Available online: https://www.who.int/genomics/professionals/education/en/ (accessed on 10 March 2021).
- Raza, A.; CooMarch Asamy, A.; Khan, K.S. Best evidence continuous medical education. Arch. Gynecol. Obstet. 2006, 280, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.C.; Konrad, T.R. A mixed-method evaluation of a workforce development intervention for nursing assistants in nursing home: The case of WIN A STEP UP. Gerontologist 2008, 49, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Lerner, N.B.; Resnick, B.; Galik, E.; Russ, K.G. Advanced nursing assistant education program. J. Contin. Educ. Nurs. 2010, 41, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Goodridge, D.; Johnston, P.; Thomson, M. Impact of a nursing assistant training program on job performance, attitudes, and relationships with residents. Educ. Gerontol. 1997, 23, 37–51. [Google Scholar] [CrossRef]
- Resnick, B.; Cayo, J.; Galik, E.; Pretzer-Aboff, I. Implementation of the 6-week educational component in the res-care intervention: Process and outcomes. J. Contin. Educ. Nurs. 2009, 40, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Pitmen, S. Evaluating a self-directed palliative care learning package for rural age care workers: A pilot study. Int. J. Palliat. Nurs. 2013, 19, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Bluestone, J.; Johnson, P.; Fullerton, J.; Carr, C.; Alderman, J.; BonTempo, J. Effective in-service training design and delivery: Evidence from an integrative literature review. Hum. Resour. Health 2013, 11, 51. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Coto-Yglesias, F.; Varkey, P.; Prokop, L.J.; Murad, A.L. The effectiveness of self-directed learning in health professions education: A systematic review. Med. Educ. 2010, 44, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- 2016–2036 Macao Population Projection. Available online: https://www.dsec.gov.mo/Statistic.aspx?lang=en-US&NodeGuid=ec391696-f920-49ed-b539-e1cfabff1d84 (accessed on 10 March 2021).
- Health Statistics 2019. Available online: https://www.dsec.gov.mo/en-US/Statistic?id=202 (accessed on 10 March 2021).
- Health at a Glance 2019. Available online: https://www.oecd-ilibrary.org/docserver/4dd50c09-en.pdf?expires=1580546775&id=id&accname=guest&checksum=F53B57E61ED3C1E64B0A3BF1ACAB6077 (accessed on 10 March 2021).
- Social Welfare Bureau of Macao. The Practice and Duty of Registered Nurses, Healthcare Assistants and Personal Caregivers; Social Welfare Bureau of Macao: Macao, China, 2001; pp. 1–8.
- Organisation for Economic Co-Operation and Development. Education and training policy. In Qualifications Systems-Bridges to Lifelong Learning; Organization for Economic Co-operation and Development Publishing: Paris, France, 2007; pp. 198–229. [Google Scholar]
- Cheong, P.L.; Hsu, N.L. An action plan of developing nurse assistant competence standard for elderly healthcare organizations in Macao. J. Health Archit. 2017, 4, 9–16. [Google Scholar]
- The Care Certificate Framework Guidance Document. Available online: https://www.skillsforcare.org.uk/Documents/Learning-and-development/Care-Certificate/The-Care-Certificate-Guidance.pdf (accessed on 10 March 2021).
- Leung, M.F. Manual of Professional Health Services for Nursing Homes for the Elderly; Cosmos Books Ltd: Hong Kong, China, 2008; pp. 1–554. [Google Scholar]
- Course Content Introduction: Fundamental Healthcare Training Programme. Available online: http://www2.kwnc.edu.mo/?page_id=5950 (accessed on 10 March 2021).
- Report of Findings from the 2014 Nurse Aide Job Analysis and Knowledge, Skill and Ability Study. Available online: https://www.ncsbn.org/15_2014NNAAP_Job_Analysis_vol65.pdf (accessed on 10 March 2021).
- Stewart, J.; O’Halloran, C.; Barton, J.R.; Singleton, S.J.; Harrigan, P.; Spencer, J. Clarifying the concepts of confidence and competence to produce appropriate self-evaluation measurement scales. Med Educ. 2008, 34, 11. [Google Scholar] [CrossRef] [PubMed]
- Oltean, H.; Gagnier, J.J. Use of clustering analysis in randomized controlled trials in orthopaedic surgery. BMC Med. Res. Methodol. 2015, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.C. To Develop a Perceived Caring Ability Assessment Scale of Nurse- Aide in the Long- Term Care Facilities. Master’s Thesis, Department Healthcare Administration and Medical Informatics, Kaohsiung. Medical University, Kaohsiung, Taiwan, 2013. [Google Scholar]
- Munn, Z.; Tufanaru, C.; Aromataris, E.; Pearson, A. Clinical Education and Training for Health Assistants: A Systematic Review to Support an External Evaluation of Clinical Education and Training for Allied Health Assistants; Clinical Education and Training Queensland, Queensland Health: Brisbane, Australia, 2010; pp. 19–29.


{kind=link}
| Themes | Teaching Content | Teaching Methods |
|---|---|---|
| 1. Role and Task |
| Lecture, case sharing |
| 2. Caring and Respect |
| Lecture, discussion |
| 3. Emergency Event |
| Lecture, demonstration, and practice |
| 4. Safety |
| Lecture, discussion, case sharing |
| 5. Hygiene |
| Experiential learning |
| 6. Infection Control |
| Lecture, demonstration, and practice |
| 7. Nutrition and Elimination |
| Lecture, discussion |
| 8. Activities and Rest |
| Lecture, demonstration, and practice |
| 9. Symptom Control |
| Lecture, case studies |
| 10. Special Care |
| Lecture, case sharing |
| Variable | Items | Experimental Group (n = 45) | Control Group (n = 40) | p |
|---|---|---|---|---|
| Number (%) | Number (%) | |||
| Age | 25 years or below | 23 (51.1) | 6 (15.0) | 0.002 ** |
| 26–35 years | 15 (33.3) | 22 (55.0) | ||
| 36 years or above | 7 (15.6) | 12 (30.0) | ||
| Educational level | Secondary | 11 (24.4) | 8 (20.0) | 0.116 |
| Diploma | 30 (66.7) | 21 (52.5) | ||
| Bachelor | 4 (8.9) | 11 (27.5) | ||
| Working years in a nursing home | Less than 1 year | 10 (22.2) | 9 (22.5) | 0.002 ** |
| 1–3 years | 28 (62.2) | 10 (25.0) | ||
| 4–7 years | 4 (8.9) | 12 (30.0) | ||
| More than 7 years | 3 (6.7) | 9 (22.5) | ||
| Other health service working experience | No | 7 (15.6) | 4 (10.0) | 0.529 |
| Yes | 38 (84.4) | 36 (90.0) | ||
| Overall dependency of residents from the nursing home | High dependency | 33 (73.3) | 35 (87.5) | 0.173 |
| Middle dependency | 12 (26.7) | 5 (12.5) | ||
| In-service training in last year | No | 6 (13.3) | 13 (32.5) | 0.040 * |
| Yes | 39 (86.7) | 27 (67.5) |
| Instruments | Domains | Experimental Group (n = 45) | Control Group (n = 40) | ||||
|---|---|---|---|---|---|---|---|
| Pre (M ± SD) | Post (M ± SD) | Difference | Pre (M ± SD) | Post (M ± SD) | Difference | ||
| Care knowledge | Daily living care | 0.55 ± 0.20 | 0.76 ± 0.21 | 0.21 | 0.50 ± 0.23 | 0.50 ± 0.25 | 0.00 |
| Clinical care skills | 0.58 ± 0.19 | 0.64 ± 0.15 | 0.06 | 0.49 ± 0.18 | 0.45 ± 0.14 | −0.04 | |
| Healthcare promotion | 0.58 ± 0.30 | 0.67 ± 0.32 | 0.09 | 0.63 ± 0.27 | 0.51 ± 0.33 | −0.12 | |
| Psychosocial support | 0.73 ± 0.29 | 0.88 ± 0.22 | 0.15 | 0.66 ± 0.32 | 0.56 ± 0.34 | −0.10 | |
| Residents’ rights and interests | 0.56 ± 0.39 | 0.73 ± 0.36 | 0.17 | 0.44 ± 0.36 | 0.51 ± 0.37 | 0.07 | |
| Taking the role of health care assistants | 0.40 ± 0.27 | 0.86 ± 0.25 | 0.46 | 0.35 ± 0.28 | 0.69 ± 0.27 | 0.34 | |
| Overall care knowledge | 0.57 ± 0.15 | 0.72 ± 0.12 | 0.15 | 0.51 ± 0.13 | 0.51 ± 0.14 | 0.00 | |
| Care competence | Daily living care | 4.45 ± 0.49 | 4.47 ± 0.49 | 0.02 | 4.18 ± 0.44 | 4.18 ± 0.41 | 0.00 |
| Clinical care skills | 4.52 ± 0.34 | 4.58 ± 0.34 | 0.06 | 4.20 ± 0.43 | 4.15 ± 0.50 | −0.04 | |
| Healthcare promotion | 3.84 ± 0.79 | 4.02 ± 0.68 | 0.18 | 3.71 ± 0.71 | 3.78 ± 0.67 | 0.07 | |
| Psychosocial support | 4.21 ± 0.54 | 4.43 ± 0.42 | 0.22 | 4.04 ± 0.47 | 4.08 ± 0.49 | 0.05 | |
| Residents’ rights and interests | 4.48 ± 0.48 | 4.67 ± 0.34 | 0.19 | 4.23 ± 0.53 | 4.35 ± 0.54 | 0.13 | |
| Taking the role of health care assistants | 3.95 ± 0.77 | 4.24 ± 0.58 | 0.29 | 3.74 ± 0.71 | 3.83 ± 0.58 | 0.09 | |
| Overall care competence | 4.37 ± 0.38 | 4.48 ± 0.36 | 0.11 | 4.10 ± 0.41 | 4.11 ± 0.45 | 0.01 | |
| Variable | Parameters | β | SE | Wald χ2 | 95% CI | p |
|---|---|---|---|---|---|---|
| Care knowledge | Intercept | 0.410 | 0.036 | 127.28 | (0.339, 0.482) | <0.001 *** |
| Group (Experimental vs. Control) | 0.057 | 0.029 | 3.848 | (0.000, 0.114) | 0.049 * | |
| Time (Post-test vs. Pre-test) | 0.003 | 0.019 | 0.021 | (−0.034, 0.040) | 0.885 | |
| Group X Time | 0.149 | 0.032 | 21.138 | (0.086, 0.213) | <0.001 *** | |
| Care competence | Intercept | 4.077 | 0.162 | 633.099 | (3.759, 4.394) | <0.001 *** |
| Group (Experimental vs. Control) | 0.349 | 0.095 | 13.361 | (−0.37, 0.238) | <0.001 *** | |
| Time (Post-test vs. Pre-test) | 0.006 | 0.439 | 0.017 | (−0.080, 0.092) | 0.897 | |
| Group X Time | 0.100 | 0.070 | 2.045 | (−0.037, 0.238) | 0.153 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheong, P.-L.; Hsu, N. Developing and Evaluating a Continuous Education Program for Healthcare Assistants in Macao: A Cluster-Randomized Trial. Int. J. Environ. Res. Public Health 2021, 18, 4990. https://doi.org/10.3390/ijerph18094990
Cheong P-L, Hsu N. Developing and Evaluating a Continuous Education Program for Healthcare Assistants in Macao: A Cluster-Randomized Trial. International Journal of Environmental Research and Public Health. 2021; 18(9):4990. https://doi.org/10.3390/ijerph18094990
Chicago/Turabian StyleCheong, Pak-Leng, and Nanly Hsu. 2021. "Developing and Evaluating a Continuous Education Program for Healthcare Assistants in Macao: A Cluster-Randomized Trial" International Journal of Environmental Research and Public Health 18, no. 9: 4990. https://doi.org/10.3390/ijerph18094990
APA StyleCheong, P.-L., & Hsu, N. (2021). Developing and Evaluating a Continuous Education Program for Healthcare Assistants in Macao: A Cluster-Randomized Trial. International Journal of Environmental Research and Public Health, 18(9), 4990. https://doi.org/10.3390/ijerph18094990