
Loneliness, Wellbeing, and Social Activity in Scottish Older Adults Resulting from Social Distancing during the COVID-19 Pandemic

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
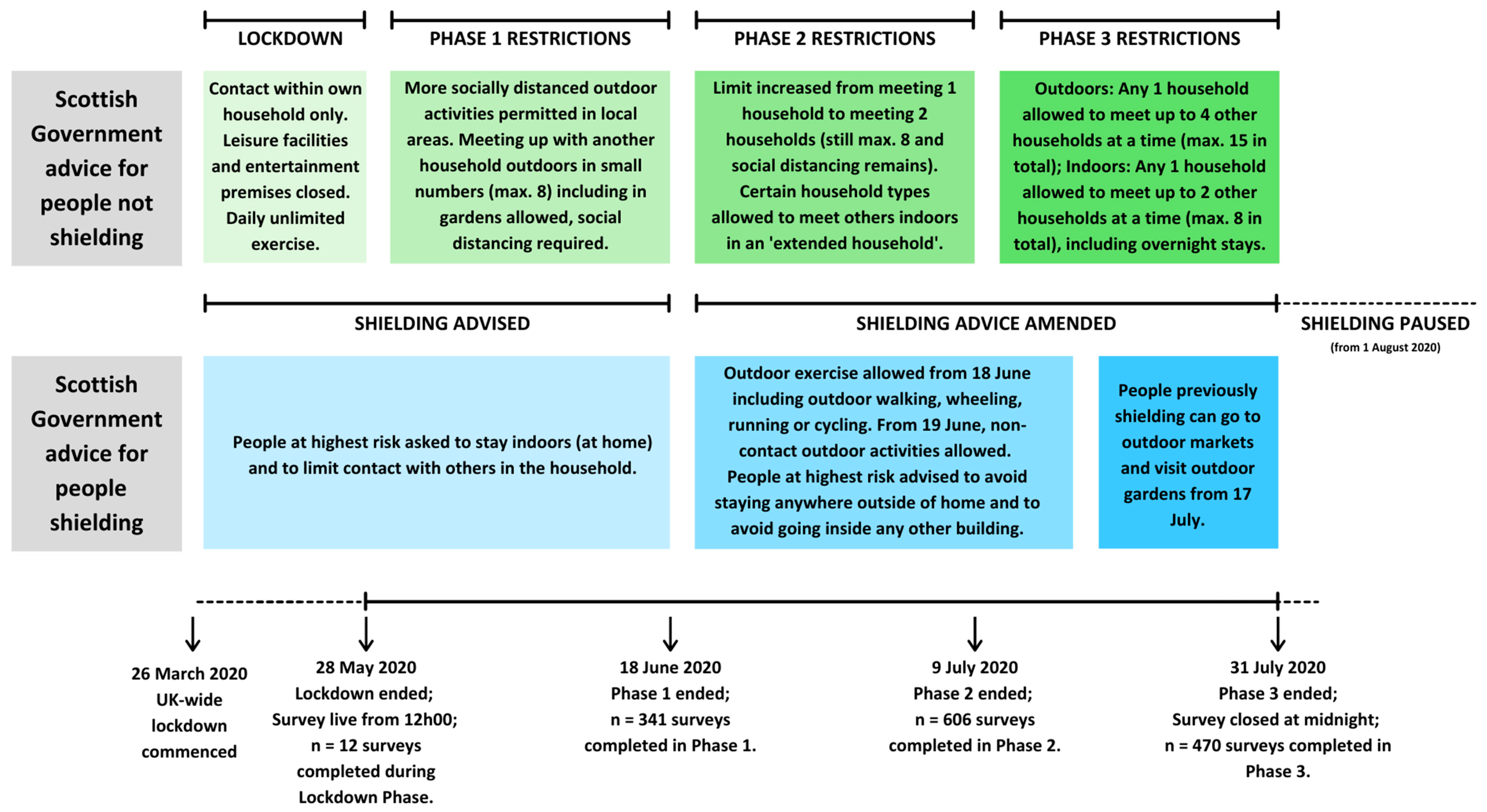
2.1. Design
2.2. Participants and Procedure
2.3. Measures
2.3.1. Sociodemographics
2.3.2. Health and Health Behaviours
2.3.3. Loneliness, Wellbeing, and Social Activity including Social Support
2.3.4. Strategies to Maintain Social Contact and Additional Contextual Factors of the Lived Experience of during Social Distancing
2.4. Data Analysis
3. Results
3.1. Data Missingness and Representativeness
3.2. Sociodemographics
3.3. Health and Health Behaviours
3.4. Loneliness, Wellbeing, and Social Activity Including Social Support
3.5. Change in Loneliness, Wellbeing, and Social Activity Including Social Support
3.6. Associations between Loneliness, Wellbeing, and Social Activity Including Social Support
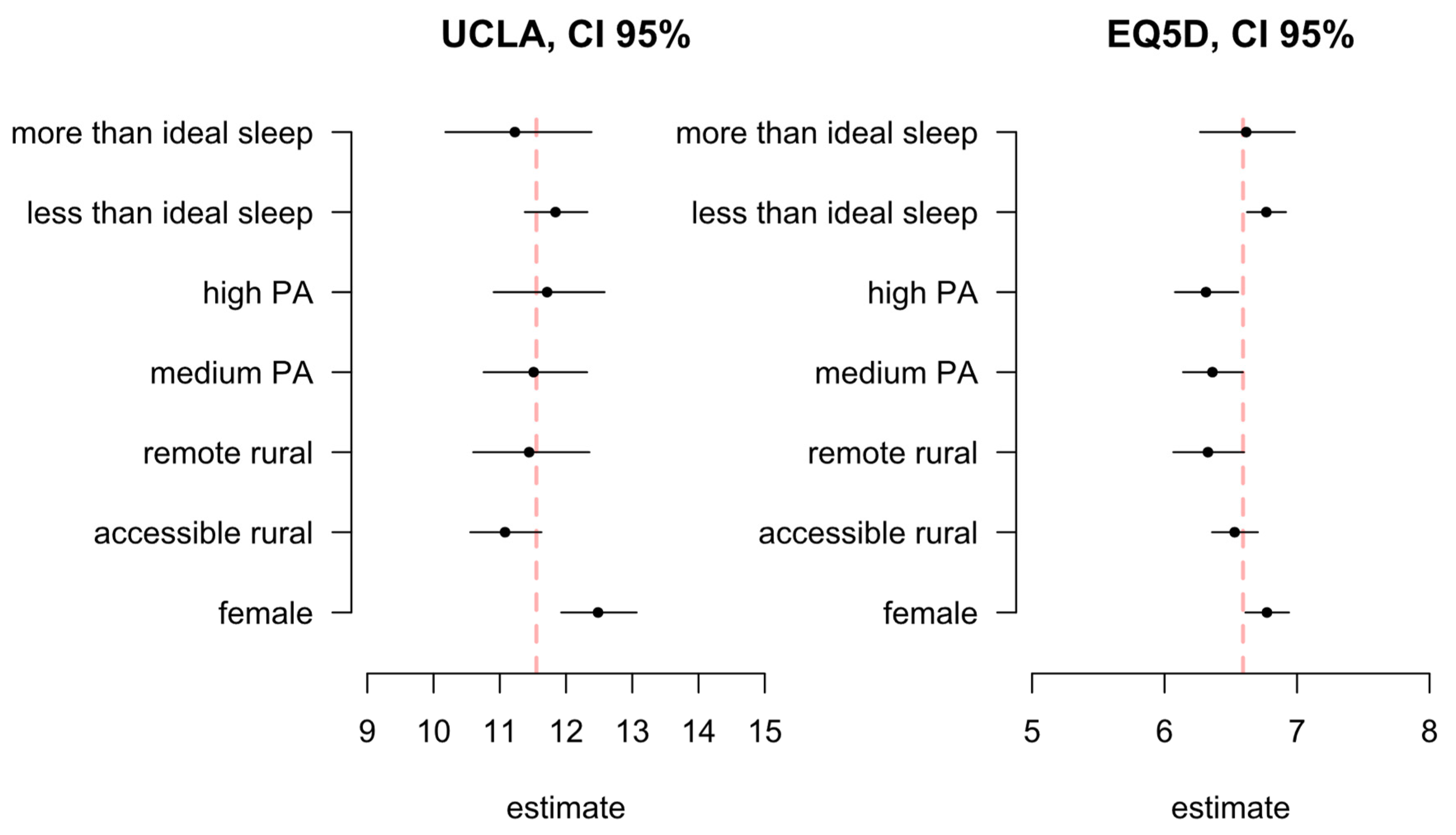
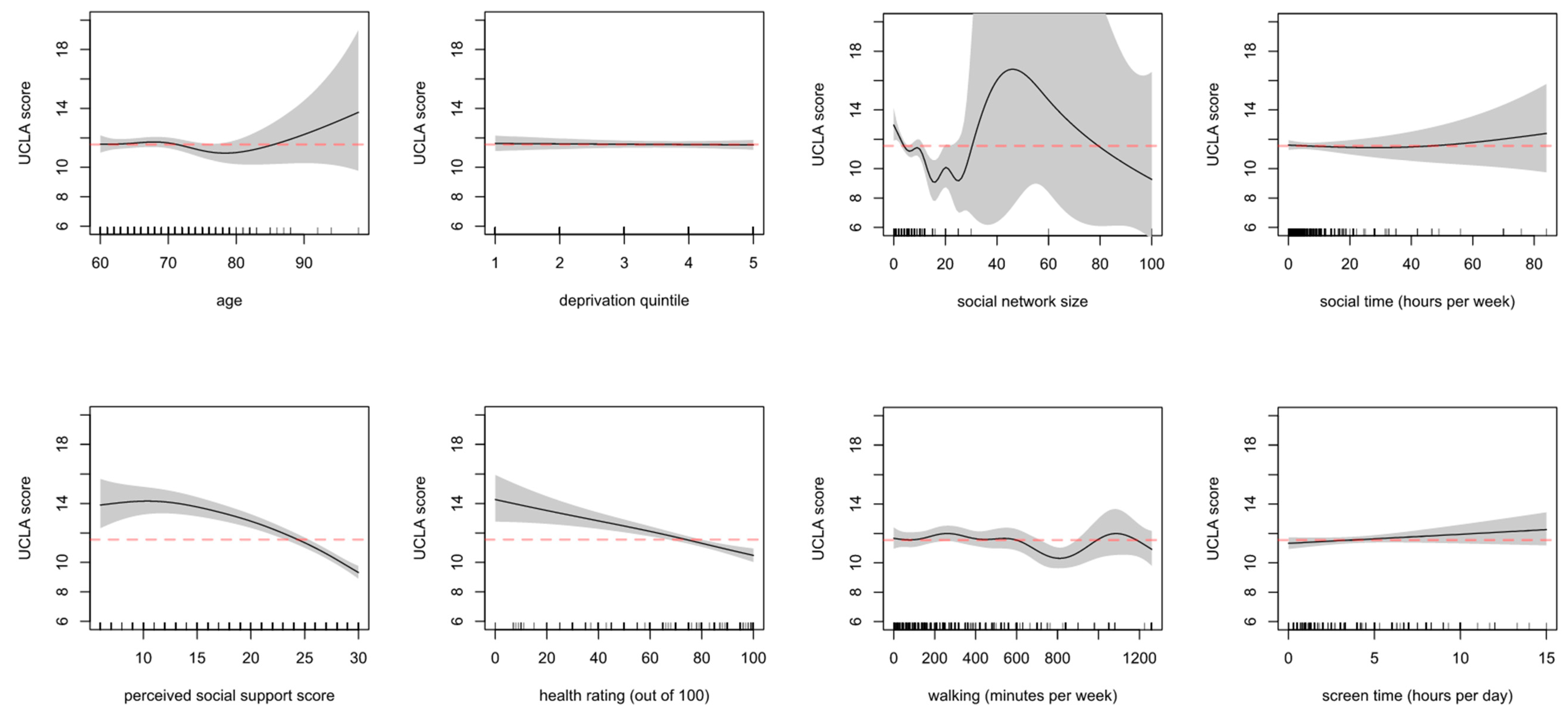
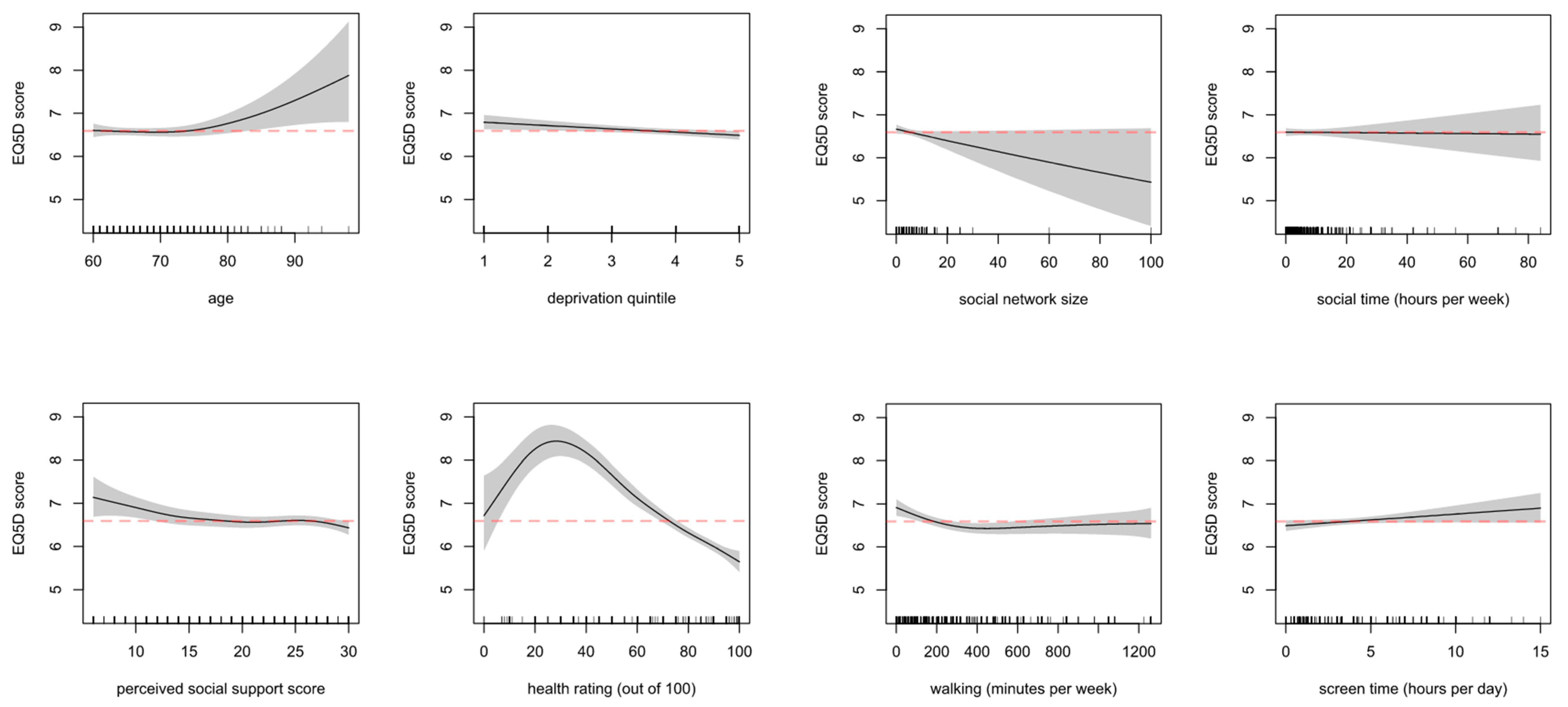
3.7. Associations with Loneliness and Wellbeing and Sociodemographic and Behavioural Variables
3.8. Strategies to Maintain Social Contact
Daily phone calls with son and daughter. Son lives a distance away and takes me for virtual walks with 2 dogs every day. As I am very familiar with the beautiful park he goes to—woodland, grassy areas, riverside, I almost feel I am there. Wider family facetime three times a week minimum. Daughter visiting at my door while socially distancing several times a week.—Female, 72 years, ‘rest of Scotland’
During lockdown I rang old friends more frequently and reconnected with people I hadn’t spoken to for a while. It was hard not having close contact with family but we FaceTimed daily.—Female, 68 years, ‘rest of Scotland’
Video calls with work and family. Work 2–3 times a week, family—once a week Social videos with work colleagues every week WhatsApp chat with colleagues daily—except weekends.—Female, 61 years, ‘accessible rural’
I spend all day at my window and have lots of chats with friends, neighbours and innocent passers-by!—Female, 70 years, ‘rest of Scotland’
The whole village is at home and out doing stuff in their gardens. We talk more than before. We talk longer than before.—Male, 66 years, ‘remote rural’
Since lockdown has eased I have been walking with friends, but now maintaining social distance.—Female, 64 years, ‘accessible rural’
Constantly meeting & chatting with people whilst out walking—especially those whose dogs come running to me, … chatting with neighbours more.—Female, 64 years, ‘rest of Scotland’
3.9. Additional Contextual Factors of the Lived Experience of during the Pandemic
I get frustrated that rules and regulations are so prescriptive, not allowing room for common sense. This leads to great feelings of guilt if one takes a calculated risk to care for a vulnerable relative who needs care…—Female, 68 years, ‘rest of Scotland’
…Angry about being asked by my doctor [if] we wanted to be resuscitated if required, made to feel that although family and friends care society as a whole thinks we are not important in the overall scheme of things.—Female, 70 years, [no postcode provided]
When I was sick I called NHS24 who advised me to call my doctor and on phoning my doctor I was advised to call NHS24. I had symptoms … The reason I was not given any attention was because I could not prove I had a fever. … I have been extremely tired since I had the virus. I phoned my doctor and the nurse said “You’ve told me all this before. You’re suffering from post viral fatigue but you’ve only had the flu”.—Female, 66 years, ‘rest of Scotland’
At the start of lockdown I felt I was going to have panic attacks again. Lost faith in other human beings the way they behaved.—Female, 65 years, ‘rest of Scotland’
As a frontline professional who has had no respite since the onset of the pandemic; the expectation that I will be able to adapt to a change of working and take on considerable more responsibility is expected; regardless of my family circumstances, which are also in disarray. The support from my organization is superficial no more than ticking boxes and the expectation is great to be present for others actually, emotionally and 24/7. I feel undervalued, patronized and exhausted.—Female, 62 years, ‘rest of Scotland’
As a single person living alone I was used to being on my own but did have a reasonable social life. I have missed the personal contact with people most but have found zoom meetings very helpful. I have 2 main problems—a lack of motivation to achieve anything domestically, and days when I feel very down and lonely. I tend not to contact anyone to discuss that preferring to get through the day on my own and trying to get out for some exercise which usually helps!—Female, 73 years, ‘rest of Scotland’
It has been hell. My son who has Down’s syndrome, autism and epilepsy has had no support since the pandemic started, day services stopped and not knowing when they will restart is awful. I feel abandoned by the system and exhausted as I am unable to do anything for me.—Female, 61 years, ‘rest of Scotland’
Not being able to work, and not qualifying for any government schemes causes anxiety. I had a part-time, self-employed job cleaning 3 times a week for 3 elderly ladies. (Because not my MAIN source income, but very important one, I don’t qualify for financial support. I am VERY angry about this) These 3 jobs gave me a lot of social contact and emotional support from the kindly [old] ladies I cleaned for. This has now gone.—Female, 62 years, ‘rest of Scotland’
At first I was happy in my bubble but now I’m feeling fed up and a bit frightened as I don’t know how it’s all going to end.—Female, 75 years, [no postcode provided]
There is no doubt that at times I have felt very isolated and lonely. Anxiety has a lot to play into feeling this way … not knowing when or if life will return to some normal. Not knowing when I will see close family that live over 500 miles away…—Female, 64 years, ‘accessible rural’
The biggest thing for me is not being able to spend time with my grandchildren and go out with my friends. No amount of online activities can replace that.—Female, 66 years, ‘rest of Scotland’
Felt loss of husband suddenly two years ago more acutely as no overnight stays from grandchildren or visits from family and friends.—Female, 76 years, ‘accessible rural’
I am a carer for elderly parents, one has dementia and one has cancer. I am shopping for them and their only source of support at the present time. Pre Covid they had home help, gardener and my sisters and other family members were visiting regularly. The isolation has had a huge impact on their wellbeing and consequently on mine. The time involved in supporting them has increased significantly.—Female, 60 years, ‘remote rural’
We have been caring for [daughter] for 47 years. Her Care package was dramatically cut To one and a half hours per week from day one. She did not make the shielding list!! Couldn’t get shopping. Feel the learning disabled abandoned by government planning…—Female, 68 years, ‘accessible rural’
I take care of my husband, who has been disabled for the past 22 years. There is no respite during the COVID-19 epidemic, so I have no free time, and feel my mental health is suffering, with no clear optimism for the future—Female, 71 years, ‘rest of Scotland’
I felt fine with social distancing and was not in any hurry to participate in any easing of lockdown but now that I have started meeting friends whilst remaining physically distanced it is absolutely wonderful. Really enjoying simple pleasures in life.—Female, 62 years, ‘rest of Scotland’
… Far from being awful, this time has been like having a gift that I couldn’t have anticipated and has made me reflect on how I will live my life moving forwards to reduce stress and have a lasting impact on health and wellbeing—Female, 60 years, [no postcode provided]
I am very lucky that I am in lockdown with a loving husband in beautiful surroundings with plenty of open space. Fortunately, all my family, including my 94 year old mother and 86 year old father in law, are keeping well so this pandemic has been a positive experience for me personally. I’m aware that this is not the case for many people.—Female, 60 years, ‘accessible rural’
4. Discussion
4.1. Strengths and Limitations
4.2. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://webarchiveorg/web/20200502133342/https:/wwwwhoint/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---1-march-2020 (accessed on 12 May 2020).
- WHO. Coronavirus Disease (COVID-19) Situation Report—2020 Situation in Numbers (by WHO Region); WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Guidance for the Public on the Mental Health and Wellbeing Aspects of Coronavirus (COVID-19)—GOV.UK. Available online: https://www.gov.uk/government/publications/covid-19-guidance-for-the-public-on-mental-health-and-wellbeing/guidance-for-the-public-on-the-mental-health-and-wellbeing-aspects-of-coronavirus-covid-19 (accessed on 15 September 2020).
- Masi, C.M.; Chen, H.Y.; Hawkley, L.C.; Cacioppo, J.T. A meta-analysis of interventions to reduce loneliness. Personal. Soc. Psychol. Rev. 2011, 15, 219–266. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. USA 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Mann, F.; Lloyd-Evans, B.; Ma, R.; Johnson, S. Associations between loneliness and perceived social support and outcomes of mental health problems: A systematic review. BMC Psychiatry 2018, 18, 156. [Google Scholar] [CrossRef]
- Cruwys, T.; Haslam, C.; Steffens, N.K.; Haslam, S.A.; Fong, P.; Lam, B.C.P. Friendships that money can buy: Financial security protects health in retirement by enabling social connectedness. BMC Geriatry 2019, 19, 319. [Google Scholar] [CrossRef]
- Choi, Y.J.; Ailshire, J.A.; Crimmins, E.M. Living alone, social networks in neighbourhoods, and daily fruit and vegetable consumption among middle-aged and older adults in the USA. Public Health Nutr. 2020, 23, 3315. [Google Scholar] [CrossRef] [PubMed]
- Ellwardt, L.; Wittek, R.P.M.; Hawkley, L.C.; Cacioppo, J.T. Social Network Characteristics and Their Associations With Stress in Older Adults: Closure and Balance in a Population-Based Sample. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 1573–1584. [Google Scholar] [CrossRef]
- Lindsay Smith, G.; Banting, L.; Eime, R.; O’Sullivan, G.; van Uffelen, J.G.Z. The association between social support and physical activity in older adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 56. [Google Scholar] [CrossRef] [PubMed]
- Poscia, A.; Stojanovic, J.; La Milia, D.I.; Duplaga, M.; Grysztar, M.; Moscato, U.; Onder, G.; Collamati, A.; Ricciardi, W.; Magnavita, N. Interventions targeting loneliness and social isolation among the older people: An update systematic review. Exp. Gerontol. 2018, 102, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Chalise, H.N.; Saito, T.; Takahashi, M.; Kai, I. Relationship specialization amongst sources and receivers of social support and its correlations with loneliness and subjective well-being: A cross sectional study of Nepalese older adults. Arch. Gerontol. Geriatr. 2007, 44, 299–314. [Google Scholar] [CrossRef]
- Green, L.R.; Richardson, D.S.; Lago, T.; Schatten-Jones, E.C. Network Correlates of Social and Emotional Loneliness in Young and Older Adults. Personal. Soc. Psychol. Bull. 2001, 27, 281–288. [Google Scholar] [CrossRef]
- Kemperman, A.; van den Berg, P.; Weijs-Perrée, M.; Uijtdewillegen, K. Loneliness of Older Adults: Social Network and the Living Environment. Int. J. Environ. Res. Public Health 2019, 16, 406. [Google Scholar] [CrossRef]
- Mellor, K.S.; Edelmann, R.J. Mobility, social support, loneliness and well-being amongst two groups of older adults. Pers. Individ. Dif. 1988, 9, 1–5. [Google Scholar] [CrossRef]
- Schnittger, R.I.B.; Wherton, J.; Prendergast, D.; Lawlor, B.A. Risk factors and mediating pathways of loneliness and social support in community-dwelling older adults. Aging Ment. Health 2012, 16, 335–346. [Google Scholar] [CrossRef]
- Winningham, R.G.; Pike, N.L. A cognitive intervention to enhance institutionalized older adults’ social support networks and decrease loneliness. Aging Ment. Health 2007, 11, 716–721. [Google Scholar] [CrossRef]
- Merz, E.M.; De Jong Gierveld, J. Childhood memories, family ties, sibling support and loneliness in ever-widowed older adults: Quantitative and qualitative results. Ageing Soc. 2016, 36, 534–561. [Google Scholar] [CrossRef]
- Rodrigues, M.M.S.; De Jong Gierveld, J.; Buz, J. Loneliness and the exchange of social support among older adults in Spain and the Netherlands. Ageing Soc. 2014, 34, 330–354. [Google Scholar] [CrossRef]
- Kang, H.W.; Park, M.; Wallace Hernandez, J.P. The impact of perceived social support, loneliness, and physical activity on quality of life in South Korean older adults. J. Sport Health Sci. 2016, 7, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Feeley, T.H. Social support, social strain, loneliness, and well-being among older adults. J. Soc. Pers. Relat. 2014, 31, 141–161. [Google Scholar] [CrossRef]
- Bai, X.; Yang, S.; Knapp, M. Sources and directions of social support and life satisfaction among solitary Chinese older adults in Hong Kong: The mediating role of sense of loneliness. Clin. Interv. Aging 2018, 13, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef]
- Scottish Health Survey 2019—Volume 1: Main Report—gov.scot. Available online: https://www.gov.scot/publications/scottish-health-survey-2019-volume-1-main-report/pages/10/ (accessed on 5 February 2021).
- UK Chief Medical Officers’ Physical Activity Guidelines. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 15 September 2020).
- Fox, K.R.; Stathi, A.; McKenna, J.; Davis, M.G. Physical activity and mental well-being in older people participating in the Better Ageing Project. Eur. J. Appl. Physiol. 2007, 100, 591–602. [Google Scholar] [CrossRef]
- Shvedko, A.; Whittaker, A.C.; Thompson, J.L.; Greig, C.A. Physical activity interventions for treatment of social isolation, loneliness or low social support in older adults: A systematic review and meta-analysis of randomised controlled trials. Psychol. Sport Exerc. 2018, 34. [Google Scholar] [CrossRef]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Tackling Loneliness|Age Scotland. Available online: https://www.ageuk.org.uk/scotland/what-we-do/tackling-loneliness/# (accessed on 28 September 2020).
- Hubbard, G.; den Daas, C.; Johnston, M.; Dixon, D. Sociodemographic and Psychological Risk Factors for Anxiety and Depression: Findings from the Covid-19 Health and Adherence Research in Scotland on Mental Health (CHARIS-MH) Cross-sectional Survey. Int. J. Behav. Med. 2021, 3, 1–13. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Smith, L.; Jacob, L.; Yakkundi, A.; McDermott, D.; Armstrong, N.C.; Barnett, Y.; López-Sánchez, G.F.; Martin, S.; Butler, L.; Tully, M.A. Correlates of symptoms of anxiety and depression and mental wellbeing associated with COVID-19: A cross-sectional study of UK-based respondents. Psychiatry Res. 2020, 291, 113138. [Google Scholar] [CrossRef] [PubMed]
- WMA—The World Medical Association. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 11 September 2020).
- United Nations, The Population Division of the Department of Economic and Social Affairs. World Population Ageing 2019; United Nations: Geneva, Switzerland, 2019. [Google Scholar]
- The Easy Read Photo Library—Photosymbols. Available online: https://www.photosymbols.com/ (accessed on 5 November 2020).
- Accessible Communication Formats—GOV.UK. Available online: https://www.gov.uk/government/publications/inclusive-communication/accessible-communication-formats (accessed on 10 February 2021).
- Scottish Government Urban Rural Classification. Available online: https://www2.gov.scot/Topics/Statistics/About/Methodology/UrbanRuralClassification# (accessed on 21 September 2020).
- Cummins, S.; Smith, D.M.; Taylor, M.; Dawson, J.; Marshall, D.; Sparks, L.; Anderson, A.S. Variations in fresh fruit and vegetable quality by store type, urban–rural setting and neighbourhood deprivation in Scotland. Publ. Health Nutr. 2009, 12, 2044–2050. [Google Scholar] [CrossRef][Green Version]
- Scottish Index of Multiple Deprivation 2020—gov.scot. Available online: https://www.gov.scot/collections/scottish-index-of-multiple-deprivation-2020/ (accessed on 27 October 2020).
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National sleep foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Davies, D.S.C.; Atherton, F.; McBride, M.; Calderwood, C. UK Chief Medical Officers’ Physical Activity Guidelines; Scottish Government: Edinburgh, UK, 2019.
- Neto, F. Psychometric analysis of the short-form UCLA Loneliness Scale (ULS-6) in older adults. Eur. J. Ageing 2014, 11, 313–319. [Google Scholar] [CrossRef]
- EuroQol Group Eq-5D-3L—Eq-5D. Available online: https://euroqol.org/eq-5d-instruments/eq-5d-3l-about/ (accessed on 28 September 2020).
- Sherbourne, C.D.; Stewart, A.L. The MOS social support survey. Soc. Sci. Med. 1991, 32, 705–714. [Google Scholar] [CrossRef]
- Kliem, S.; Mößle, T.; Rehbein, F.; Hellmann, D.F.; Zenger, M.; Brähler, E. A brief form of the Perceived Social Support Questionnaire (F-SozU) was developed, validated, and standardized. J. Clin. Epidemiol. 2015, 68, 551–562. [Google Scholar] [CrossRef]
- Lin, M.; Hirschfeld, G.; Margraf, J. Brief form of the perceived social support questionnaire (F-SozU K-6): Validation, norms, and cross-cultural measurement invariance in the USA, Germany, Russia, and China. Psychol. Assess. 2019, 31, 609–621. [Google Scholar] [CrossRef]
- R Core Team, R. A Language and Environment for Statistical Computing; R Core Team R: Vienna, Austria, 2020. [Google Scholar]
- Durante, F.; Sempi, C. Copula Theory: An Introduction; Springer: Berlin/Heidelberg, Germany, 2010; pp. 3–31. [Google Scholar]
- Wood, S.N. Generalized Additive Models: An Introduction With R, 2nd ed.; Routledge: London, UK, 2017; ISBN 9781498728348. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Davern, M.; Rodin, H.; Beebe, T.J.; Call, K.T. The effect of income question design in health surveys on family income, poverty and eligibility estimates. Health Serv. Res. 2005, 40, 1534–1552. [Google Scholar] [CrossRef] [PubMed]
- National Records of Scotland (NRS). Scotland’s Population 2011. The Registrar General’s Annual Review of Demographic Trends, 157th ed.; National Records of Scotland: Edinburgh, UK, 2012; Volume 1. [Google Scholar]
- Warriner, K.; Goyder, J.; Miller, S. Evaluating Socio-economic Status (SES) Bias in Survey Nonresponse. J. Off. Stat. 2002, 18, 1–12. [Google Scholar]
- Scotland: Ethnicity 2018|Statista. Available online: https://www.statista.com/statistics/367842/scotland-ethnicity-of-population/ (accessed on 28 September 2020).
- Szende, A.; Janssen, B.; Cabasés, J. Self-Reported Population Health: An International Perspective Based on EQ-5D; Springer: Amsterdam, The Netherlands, 2014; ISBN 9789400775961. [Google Scholar]
- Van Eijk, B.W.J.H.; Penninx, T.; Van Tilburg, D.M.W.; Kriegsman, A.; Joan, P.; Boeke, D.J.H.; Deeg, J.; Th, M. Social Network, Social Support, and Loneliness in Older Persons with Different Chronic Diseases. J. Aging Health 2011, 11, 151–168. [Google Scholar] [CrossRef]
- McHugh, J.E.; Kenny, R.A.; Lawlor, B.A.; Steptoe, A.; Kee, F. The discrepancy between social isolation and loneliness as a clinically meaningful metric: Findings from the Irish and English longitudinal studies of ageing (TILDA and ELSA). Int. J. Geriatr. Psychiatry 2017, 32, 664–674. [Google Scholar] [CrossRef] [PubMed]
- Menec, V.H.; Newall, N.E.; Mackenzie, C.S.; Shooshtari, S.; Nowicki, S. Examining social isolation and loneliness in combination in relation to social support and psychological distress using Canadian Longitudinal Study of Aging (CLSA) data. PLoS ONE 2020, 15, e0230673. [Google Scholar] [CrossRef]
- El-Tallawy, S.N.; Nalamasu, R.; Pergolizzi, J.V.; Gharibo, C. Pain Management During the COVID-19 Pandemic. Pain Ther. 2020, 9, 453–466. [Google Scholar] [CrossRef]
- Curran, E.; Rosato, M.; Ferry, F.; Leavey, G. Prevalence and factors associated with anxiety and depression in older adults: Gender differences in psychosocial indicators. J. Affect. Disord. 2020, 267, 114–122. [Google Scholar] [CrossRef]
- Magee, C.A.; Caputi, P.; Iverson, D.C. Relationships between self-rated health, quality of life and sleep duration in middle aged and elderly Australians. Sleep Med. 2011, 12, 346–350. [Google Scholar] [CrossRef]
- Faubel, R.; Lopez-Garcia, E.; Guallar-Castillón, P.; Balboa-Castillo, T.; Gutiérrez-Fisac, J.L.; Banegas, J.R.; Rodríguez-Artalejo, F. Sleep Duration and Health-Related Quality of Life among Older Adults: A Population-Based Cohort in Spain. Sleep 2009, 32, 1059–1068. [Google Scholar] [CrossRef][Green Version]
- Stathi, A.; Fox, K.R.; McKenna, J. Physical activity and dimensions of subjective well-being in older adults. J. Aging Phys. Act. 2002, 10, 76–92. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The Impact of COVID-19 on Physical Activity Behavior and Well-Being of Canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Lee, M.-A.; Ferraro, K.F.; Kim, G. Digital technology use and depressive symptoms among older adults in Korea: Beneficial for those who have fewer social interactions? Aging Ment. Health 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ryan, J.; Lopian, L.; Le, B.; Edney, S.; Van Kessel, G.; Plotnikoff, R.; Vandelanotte, C.; Olds, T.; Maher, C. It’s not raining men: A mixed-methods study investigating methods of improving male recruitment to health behaviour research. BMC Public Health 2019, 19, 814. [Google Scholar] [CrossRef] [PubMed]
- Denny, C.C.; Grady, C. Clinical research with economically disadvantaged populations. J. Med. Ethics 2007, 33, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Pels, F.; Kleinert, J. Loneliness and physical activity: A systematic review. Int. Rev. Sport Exerc. Psychol. 2016, 9, 231–260. [Google Scholar] [CrossRef]
- Chalise, H.; Kai, I.; Saito, T. Social support and its correlation with loneliness: A cross-cultural study of Nepalese older adults. Int. J. Aging Hum. Dev. 2010, 71, 115–138. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n | Mean (SD)/n (%) | |
|---|---|---|---|
| Sex | Female | 1196 | 920 (77) |
| Age (years) | 1198 | 67.3 (5.4) | |
| Relationship | Single | 1191 | 78 (7) |
| Divorced/widowed | 306 (26) | ||
| In a Relationship | 53 (4) | ||
| Married/cohabiting | 754 (63) | ||
| Health condition | Yes | 1198 | 624 (52) |
| Carer | Yes | 1198 | 149 (12) |
| Education | Did not complete | 1168 | 72 (6) |
| GCSE/O-levels 1 | 113 (10) | ||
| Post-16 vocational course | 40 (3) | ||
| Highers/A-levels 1 | 121 (10) | ||
| Undergraduate degree 1 | 545 (47) | ||
| Postgraduate degree | 277 (24) | ||
| SIMD deprivation quintile 2 | 1 (most deprived) | 1094 | 89 (8) |
| 2 | 142 (13) | ||
| 3 | 229 (21) | ||
| 4 | 282 (26) | ||
| 5 (least deprived) | 351 (32) | ||
| Urban/rural 3-fold classification 2 | ‘Rest of Scotland’ 3 | 1094 | 826 (69) |
| Accessible rural | 199 (17) | ||
| Remote rural | 69 (6) | ||
| Walking (min/week) | 1193 | 336.2 (307.6) | |
| Sleep category | Short sleeper | 1187 | 520 (44) |
| Ideal sleeper | 616 (52) | ||
| Long sleeper | 51 (4) | ||
| Physical Activity category | Low active | 1193 | 252 (21) |
| Moderately active | 426 (36) | ||
| Highly active | 515 (43) | ||
| Screen time (hr/day) | 1193 | 3.7 (2.6) |
| Variable | Mean (SD)/n (%) |
|---|---|
| UCLA loneliness score | 12.7 (4.70) |
| Social network size | 5.5 (5.06) |
| Social contact (days per week) | 5.4 (1.92) |
| Social time (hours per week) | 7.0 (8.68) |
| Perceived social support (BPSSQ) | 3.8 (1.04) |
| EQ5D-3L total score 1 | 6.7 (1.60) |
| Mobility | |
| I have no problems in walking about | 919 (77) |
| I have some problems in walking about | 278 (23) |
| I am confined to bed | 1 (<1) |
| Self-care | |
| I have no problems with self-care | 1103 (92) |
| I have some problems washing or dressing myself | 92 (8) |
| I am unable to wash or dress myself | 3 (<1) |
| Usual activities | |
| I have no problems with performing my usual activities | 879 (73) |
| I have some problems with performing my usual activities | 289 (24) |
| I am unable to perform my usual activities | 30 (3) |
| Pain/discomfort | |
| I have no pain or discomfort | 547 (46) |
| I have moderate pain or discomfort | 598 (50) |
| I have extreme pain or discomfort | 53 (4) |
| Anxiety/depression | |
| I am not anxious or depressed | 646 (54) |
| I am moderately anxious or depressed | 510 (43) |
| I am extremely anxious or depressed | 42 (4) |
| Current health rating (out of 100) 2 | 72.5 (19.91) |
| Variable | n | n (%) | ||
|---|---|---|---|---|
| Less | Same | More | ||
| Loneliness 1 | 1198 | 51 (4) | 495 (41) | 652 (54) |
| Health rating 2 | 1198 | 357 (30) | 762 (64) | 79 (7) |
| Anxiety/Depression 1,2 | 1198 | 48 (4) | 733 (61) | 417 (35) |
| Social network size | 1194 | 690 (58) | 373 (31) | 131 (11) |
| Social contact frequency | 1177 | 823 (69) | 247 (21) | 107 (9) |
| Social contact time | 1176 | 835 (70) | 243 (20) | 98 (8) |
| Social support quality | 1175 | 252 (21) | 803 (67) | 120 (10) |
| Giving social support | 1174 | 227 (19) | 516 (43) | 431 (36) |
| Perceived Social support | 1198 | 222 (19) | 897 (75) | 79 (7) |
| Walking | 1198 | 572 (40) | 480 (34) | 377 (26) |
| Screen time | 1198 | 42 (4) | 416 (35) | 740 (62) |
| Sleep volume | 1198 | 433 (30) | 915 (64) | 81 (6) |
| 2. | 3. | 4. | 5. | 6. | |
|---|---|---|---|---|---|
| 1. Loneliness | −0.44 ** | −0.17 * | −0.22 ** | 0.34 ** | −0.31 ** |
| 2. Perceived Social support | 0.40 ** | 0.27 ** | −0.32 ** | 0.20 ** | |
| 3. Social network size | 0.13 * | −0.16 * | 0.02 | ||
| 4. Social contact time | −0.08 | 0.12 | |||
| 5. EQ5D-3L total score | −0.55 ** | ||||
| 6. Health rating | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomaz, S.A.; Coffee, P.; Ryde, G.C.; Swales, B.; Neely, K.C.; Connelly, J.; Kirkland, A.; McCabe, L.; Watchman, K.; Andreis, F.; et al. Loneliness, Wellbeing, and Social Activity in Scottish Older Adults Resulting from Social Distancing during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4517. https://doi.org/10.3390/ijerph18094517
Tomaz SA, Coffee P, Ryde GC, Swales B, Neely KC, Connelly J, Kirkland A, McCabe L, Watchman K, Andreis F, et al. Loneliness, Wellbeing, and Social Activity in Scottish Older Adults Resulting from Social Distancing during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(9):4517. https://doi.org/10.3390/ijerph18094517
Chicago/Turabian StyleTomaz, Simone A., Pete Coffee, Gemma C. Ryde, Bridgitte Swales, Kacey C. Neely, Jenni Connelly, Andrew Kirkland, Louise McCabe, Karen Watchman, Federico Andreis, and et al. 2021. "Loneliness, Wellbeing, and Social Activity in Scottish Older Adults Resulting from Social Distancing during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 9: 4517. https://doi.org/10.3390/ijerph18094517
APA StyleTomaz, S. A., Coffee, P., Ryde, G. C., Swales, B., Neely, K. C., Connelly, J., Kirkland, A., McCabe, L., Watchman, K., Andreis, F., Martin, J. G., Pina, I., & Whittaker, A. C. (2021). Loneliness, Wellbeing, and Social Activity in Scottish Older Adults Resulting from Social Distancing during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(9), 4517. https://doi.org/10.3390/ijerph18094517