
Prediction Models for Public Health Containment Measures on COVID-19 Using Artificial Intelligence and Machine Learning: A Systematic Review

 ,
, 
 ,
, 
Abstract
1. Introduction
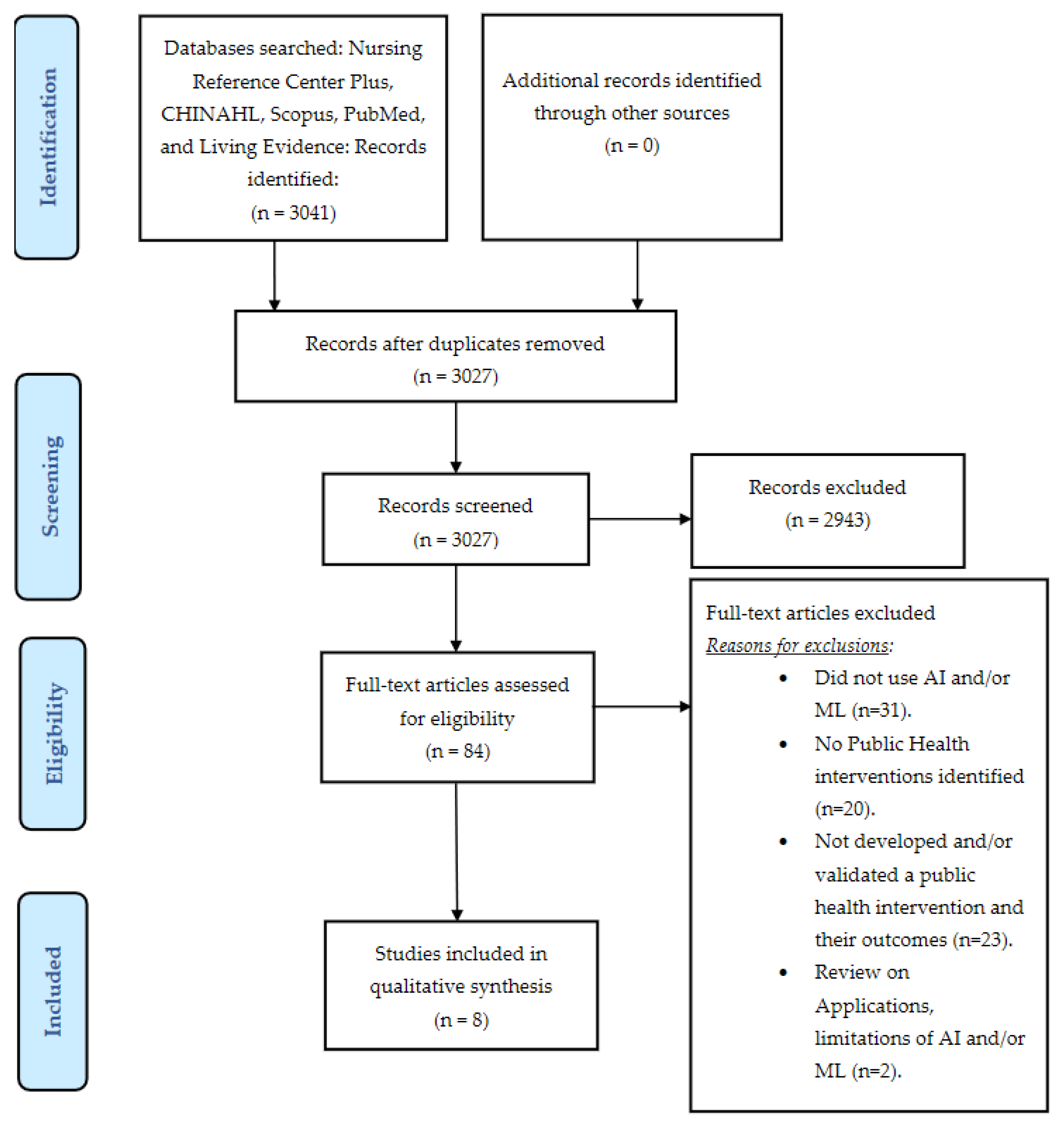
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Definition of the Interventions
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Handelman, G.S.; Kok, H.K.; Chandra, R.V.; Razavi, A.H.; Lee, M.J.; Asadi, H. eDoctor: Machine learning and the future of medicine. J. Intern. Med. 2018, 284, 603–619. [Google Scholar] [CrossRef]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: A practical introduction. BMC Med. Res. Methodol. 2019, 19, 1–18. [Google Scholar] [CrossRef]
- Wynants, L.; Van Calster, B.; Collins, G.S.; Riley, R.D.; Heinze, G.; Schuit, E.; Bonten, M.M.J.; Dahly, D.L.; A Damen, J.; A Debray, T.P.; et al. Prediction models for diagnosis and prognosis of covid-19: Systematic review and critical appraisal. BMJ 2020, 369, m1328. [Google Scholar] [CrossRef] [PubMed]
- Riley, P.; Riley, A.; Turtle, J.; Ben-Nun, M. COVID-19 deaths: Which explanatory variables matter the most? medRxiv 2020, 1–21. [Google Scholar] [CrossRef]
- Mollalo, A.; Rivera, K.M.; Vahedi, B. Artificial Neural Network Modeling of Novel Coronavirus (COVID-19) Incidence Rates across the Continental United States. Int. J. Environ. Res. Public Health 2020, 17, 4204. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, Z.; Cao, W.; Liu, Y.; Du, B.; Chen, C.; Liu, Q.; Uddin, N.; Jiang, S.; Chen, C.; et al. Identifying novel factors associated with COVID-19 transmission and fatality using the machine learning approach. Sci. Total Environ. 2021, 764, 142810. [Google Scholar] [CrossRef]
- Alsayed, A.; Sadir, H.; Kamil, R.; Sari, H. Prediction of Epidemic Peak and Infected Cases for COVID-19 Disease in Malaysia, 2020. Int. J. Environ. Res. Public Health 2020, 17, 4076. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, M.; Ortuondo, E.M.; Van-Dierdonck, J.B.; Mar, J.; Stollenwerk, N. Modelling COVID 19 in the Basque Country from introduction to control measure response. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef]
- Kannan, S.; Subbaram, K.; Ali, S.; Kannan, H. The Role of Artificial Intelligence and Machine Learning Techniques: Race for COVID-19 Vaccine. Arch. Clin. Infect. Dis. 2020, 15, e103232. [Google Scholar] [CrossRef]
- Mohamed, S.; Giabbanelli, P.; Alvarez-Lopez, F.; Adly, A.S.; Adly, A.S.; Adly, M.S. Approaches Based on Artificial Intelligence and the Internet of Intelligent Things to Prevent the Spread of COVID-19: Scoping Review. J. Med. Internet Res. 2020, 22, e19104. [Google Scholar] [CrossRef]
- Lalmuanawma, S.; Hussain, J.; Chhakchhuak, L. Applications of machine learning and artificial intelligence for Covid-19 (SARS-CoV-2) pandemic: A review. Chaos Solitons Fractals 2020, 139, 110059. [Google Scholar] [CrossRef] [PubMed]
- WHO. Non-Pharmaceutical Public Health Measures for Mitigating the Risk and Impact of Epidemic and Pandemic Influenza. A Checklist for Pandemic Influenza Risk and Impact Management: Building Capacity for Pandemic Response. 2019. Available online: https://www.who.int/publications/i/item/non-pharmaceutical-public-health-measuresfor-mitigating-the-risk-and-impact-of-epidemic-and-pandemic-influenza (accessed on 1 July 2020).
- Porgo, T.V.; Norris, S.L.; Salanti, G.; Johnson, L.F.; Simpson, J.A.; Low, N.; Egger, M.; Althaus, C.L. The use of mathematical modeling studies for evidence synthesis and guideline development: A glossary. Res. Synth. Methods 2019, 10, 125–133. [Google Scholar] [CrossRef]
- Godio, A.; Pace, F.; Vergnano, A. SEIR Modeling of the Italian Epidemic of SARS-CoV-2 Using Computational Swarm Intelligence. Int. J. Environ. Res. Public Health 2020, 17, 3535. [Google Scholar] [CrossRef]
- Parham, P.E.; Michael, E. Outbreak properties of epidemic models: The roles of temporal forcing and stochasticity on pathogen invasion dynamics. J. Theor. Biol. 2011, 271, 1–9. [Google Scholar] [CrossRef]
- WHO. Action Plan to Strengthen the Use of Evidence, Information and Research for Policy-Making in the WHO European Region. Regional Committee for Europe 66th session: Copenhagen, Denmark. 2016, pp. 12–15. Available online: http://www.euro.who.int/en/who-we-are/governance (accessed on 13 July 2020).
- Blessing, V.; Davé, A.; Varnai, P. Evidence on Mechanisms and Tools for Use of Health Information for Decision-Making; Evid Mech Tools Use Heal Inf Decis Published Online First: 2017. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29300440 (accessed on 13 July 2020).
- Living Evidence on COVID-19. Available online: https://ispmbern.github.io/covid-19/living-review/index.html (accessed on 1 February 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Odusanya, O.O.; Odugbemi, B.A.; Odugbemi, T.O.; Ajisegiri, W.S. January–March 2018 an Official Publication of the National Postgraduate Medical College of Nigeria. Niger. Postgrad. Med. J. 2018, 19–26. [Google Scholar] [CrossRef]
- Kumar, A.; Khan, F.M.; Gupta, R.; Puppala, H. Preparedness and Mitigation by projecting the risk against COVID-19 transmission using Machine Learning Techniques. medRxiv 2020. published online first. [Google Scholar] [CrossRef]
- Zengul, F.; Erraguntla, M.; Delen, D.; Eryarsoy, E.; Davazdahemami, B. No Place Like Home: Cross-National Data Analysis of the Efficacy of Social Distancing During the COVID-19 Pandemic. JMIR Public Health Surveill. 2020, 6, e19862. [Google Scholar] [CrossRef]
- Shao, P.; Shan, Y. Beware of asymptomatic transmission: Study on 2019-nCoV prevention and control measures based on extended SEIR model. bioRxiv 2020, 16, 224. [Google Scholar] [CrossRef]
- Pasayat, A.K.; Pati, S.N.; Maharana, A. Predicting the COVID-19 positive cases in India with concern to lockdown by using mathematical and machine learning based models. medRxiv 2020. published online first. [Google Scholar] [CrossRef]
- Marini, M.; Chokani, N.; Abhari, R.S. COVID-19 Epidemic in Switzerland: Growth Prediction and Containment Strategy Using Artificial Intelligence and Big Data. medRxiv 2020, 1–10. [Google Scholar] [CrossRef]
- Qiu, Y.; Chen, X.; Shi, W. Impacts of social and economic factors on the transmission of coronavirus disease 2019 (COVID-19) in China. J. Popul. Econ. 2020, 33, 1127–1172. [Google Scholar] [CrossRef]
- Wang, S.; Ramkrishna, D. On the spread of coronavirus infection. A mechanistic model to rate strategies for disease management. medRxiv 2020, 1–15. [Google Scholar] [CrossRef]
- Dandekar, R.; Barbastathis, G. Quantifying the effect of quarantine control in Covid-19 infectious spread using machine learning. medRxiv 2020, 2020, 1–13. [Google Scholar] [CrossRef]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions With the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1915. [Google Scholar] [CrossRef] [PubMed]
- Bo, Y.; Guo, C.; Lin, C.; Zeng, Y.; Li, H.B.; Zhang, Y.; Hossain, S.; Chan, J.W.; Yeung, D.W.; Kwok, K.O.; et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int. J. Infect. Dis. 2021, 102, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef]
- Singh, B.B.; Lowerison, M.; Lewinson, R.T.; Vallerand, I.A.; Deardon, R.; Gill, J.P.S.; Singh, B.; Barkema, H.W. Public health interventions slowed but did not halt the spread of COVID-19 in India. Transbound. Emerg. Dis. 2020, 2, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kissler, S.; Tedijanto, C.; Lipsitch, M.; Grad, Y. Social distancing strategies for curbing the COVID-19 epidemic. medRxiv 2020. prepr published online first. [Google Scholar] [CrossRef]
- Ludvigsson, J.F. The first eight months of Sweden’s COVID-19 strategy and the key actions and actors that were involved. Acta Paediatr. 2020, 109, 2459–2471. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J.H.; Tibshirani, R.; Hastie, T. The Elements of Statistical Learning; Springer: Berlin/Heidelberg, Germany, 2001; Available online: https://web.stanford.edu/~hastie/Papers/ESLII.pdf (accessed on 8 April 2021).
- Nielsen, T.; Jensen, F. Bayesian Networks and Decision Graphs; Springer: Berlin/Heidelberg, Germany, 2007; Available online: https://www.springer.com/gp/book/9780387682815 (accessed on 8 April 2021).
- Emerging SARS-CoV-2 Variants. Available online: https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/scientific-brief-emerging-variants.html (accessed on 10 March 2021).
- Schiermeier, Q.; Klimek, P. Deducing which pandemic policies work best. Nature 2021, 591, 189. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Title | Author | Setting | Outcome | Model Development | Model Characteristic | Typology of Data |
|---|---|---|---|---|---|---|
| On the Spread of Coronavirus Infection. A Mechanistic Model to Rate Strategies for Disease Management. | Shiyan Wang | United States | Control of the epidemic spread, reduce spike. | New | Mechanistic | Empirical |
| No Place Like Home: Cross-National Data Analysis of the Efficacy of Social Distancing During the COVID-19 Pandemic. | Dursun Delen | 26 countries | Control of the epidemic spread, reduce spike. | Existing | Susceptible–infected–recovered (SIR) | Empirical |
| Predicting the COVID-19 positive cases in India with concern to Lockdown by using Mathematical and Machine Learning based models. | Ajit Kumar Pasayat | India | Control of the epidemic spread, reduce spike. | Existing | Exponential Growth, Linear Regression | Simulation |
| Preparedness and Mitigation by projecting the risk against COVID-19 transmission using Machine Learning Techniques. | Akshay Kumar | India | Risk of hotspot formation. | New | Technique for Order of Preference by Similarity to Ideal Solution (TOPSIS) | Simulation |
| Quantifying the effect of quarantine control in COVID-19 infectious spread using machine learning. | Raj Dandekar | Wuhan, Italy, South Korea, USA | Control of the epidemic spread. | New | Neural network augmented | Empirical |
| COVID-19 Epidemic in Switzerland: Growth Prediction and Containment Strategy Using Artificial Intelligence and Big Data. | Marcello Marini | Switzerland | Outbreak prediction evolution of spread, rate of recovery. | Existing | Agent-based simulation framework, EnerPol | Simulation |
| Impacts of Social and Economic Factors on the Transmission of Coronavirus Disease 2019 (COVID-19) in China. | Yun Qiuy | China | Reduce the transmission rate. | Existing | Empirical | Empirical |
| Beware of asymptomatic transmission: Study on 2019-nCoV prevention and control measures based on extended SEIR model. | Peng Shao | China | Control of the epidemic spread. | Existing | Susceptible–Exposed–Infectious–Recovered (SEIR) | Simulation |
| Author | Outbreak Phase | Intervention Type | Description of Intervention | Results |
|---|---|---|---|---|
| Shiyan Wang | All the stages of the epidemic | Multiple | (i.) Stay at home order. (ii.) Easing social distancing measures. (iii.) Mandatory quarantine for travelers. (iv.) Non-essential business closure. (v.) Gathering ban. (vi.) School closure. (vii.) Restaurant limits. | The study suggested that non-essential business closure, a gathering ban and school closure could have a strong impact on eventual infection fraction—if the interventions were implemented before the peak infection rate. |
| Dursun Delen | All the stages of the epidemic | Single | Social Distancing. | Social distancing policies could help in slowing the spread of COVID-19 (approximately 47% of the variation in the disease transmission rates) as well as in flattening the epidemic curve. |
| Ajit Kumar Pasayat | All the stages of the epidemic | Single | (i.) Lockdown is not continuing strictly after May 18th, 2020. (ii.) Lockdown continues. | Partial lockdown could play a positive role in preventing the spread of the disease. |
| Akshay Kumar | Beginning of the epidemic | Single | Adaption of lockdown measures according to the risk (low, moderate, and high) of new hot spots. | The study suggested to: (i) Release all constraints except mass gatherings and travel out of district in low-risk areas. (ii) Release partial constraints, i.e., (i) + markets with essential commodities in moderate-risk areas. (iii) Seal the districts with essential commodities at doorsteps in high-risk areas. |
| Raj Dandekar | All the stages of the epidemic | Single | Quarantine and isolation. | Strong correlation between strengthening of the quarantine, actions taken by governments, and a decrease in effective reproductive number (Rt). |
| Marcello Marini | Beginning of the epidemic | Multiple | (i.) Closure of schools. (ii.) Closure of activities. (iii.) Limitation of public transport. (iv.) Social distancing. | The study estimated that, in the absence of interventions, 42.7% of the Swiss population would have been infected. |
| Yun Qiuy | Beginning of the epidemic | Multiple | (i.) Stringent quarantine. (ii.) Massive lockdown. (iii.) Other public health measures. | The interventions significantly reduced the transmission rate of COVID-19. The study also demonstrated that the actual population flow from the outbreak source poses a higher risk to the destination than geographic proximity and similarity in economic conditions. |
| Peng Shao | Beginning of the epidemic | Multiple | (i.) Quarantine of infected people. (ii.) Reduction in movement of people. | The measures could help in controlling the spread of the epidemic. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Payedimarri, A.B.; Concina, D.; Portinale, L.; Canonico, M.; Seys, D.; Vanhaecht, K.; Panella, M. Prediction Models for Public Health Containment Measures on COVID-19 Using Artificial Intelligence and Machine Learning: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4499. https://doi.org/10.3390/ijerph18094499
Payedimarri AB, Concina D, Portinale L, Canonico M, Seys D, Vanhaecht K, Panella M. Prediction Models for Public Health Containment Measures on COVID-19 Using Artificial Intelligence and Machine Learning: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(9):4499. https://doi.org/10.3390/ijerph18094499
Chicago/Turabian StylePayedimarri, Anil Babu, Diego Concina, Luigi Portinale, Massimo Canonico, Deborah Seys, Kris Vanhaecht, and Massimiliano Panella. 2021. "Prediction Models for Public Health Containment Measures on COVID-19 Using Artificial Intelligence and Machine Learning: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 9: 4499. https://doi.org/10.3390/ijerph18094499
APA StylePayedimarri, A. B., Concina, D., Portinale, L., Canonico, M., Seys, D., Vanhaecht, K., & Panella, M. (2021). Prediction Models for Public Health Containment Measures on COVID-19 Using Artificial Intelligence and Machine Learning: A Systematic Review. International Journal of Environmental Research and Public Health, 18(9), 4499. https://doi.org/10.3390/ijerph18094499