
Different Domains of Dengue Research in Malaysia: A Systematic Review and Meta-Analysis of Questionnaire-Based Studies

 , ,
, ,  , , ,
, , ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
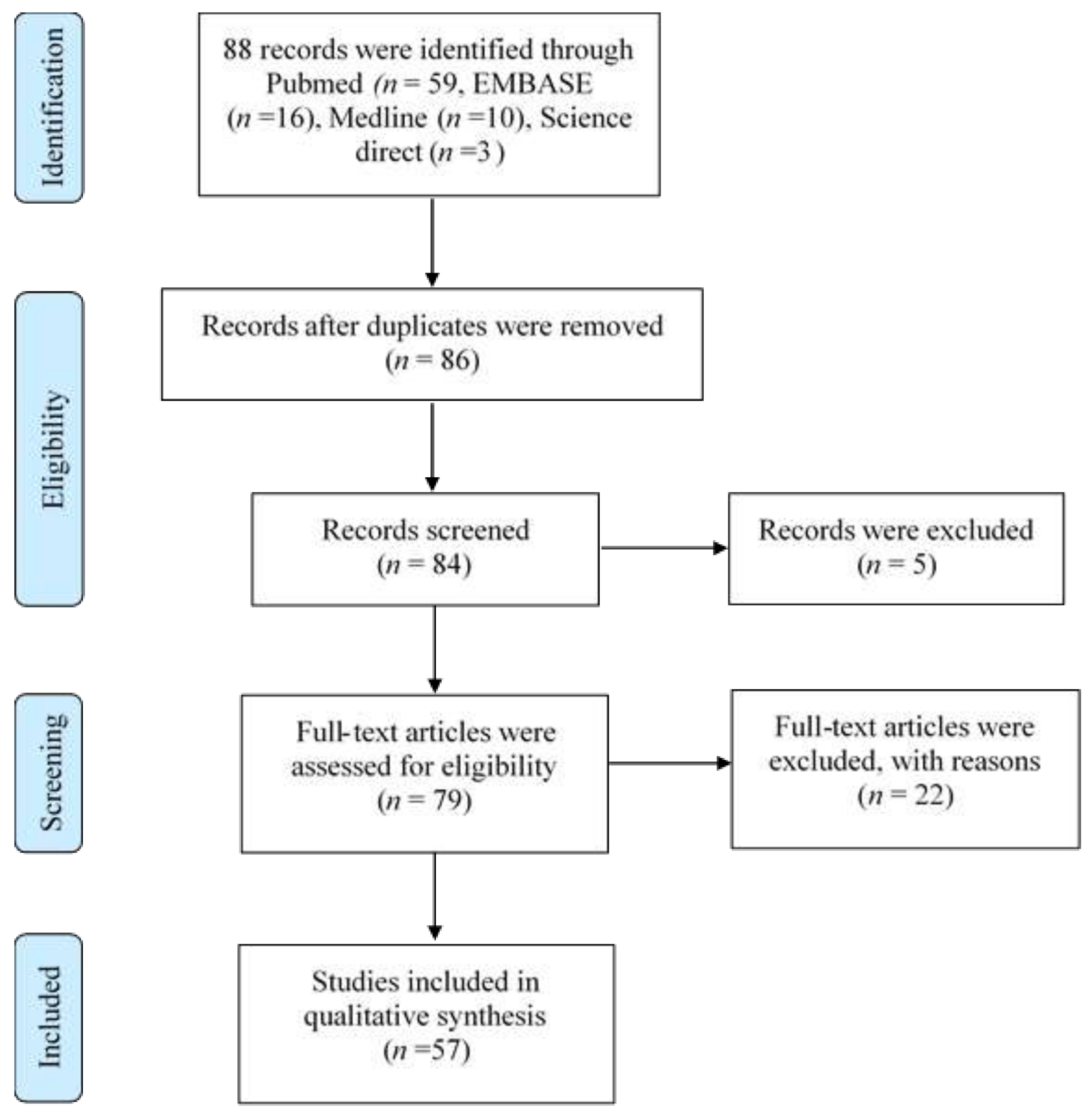
2.1.1. Identification and Selection of Studies
2.1.2. Selection Criteria
2.1.3. Data Extraction and Management
3. Results
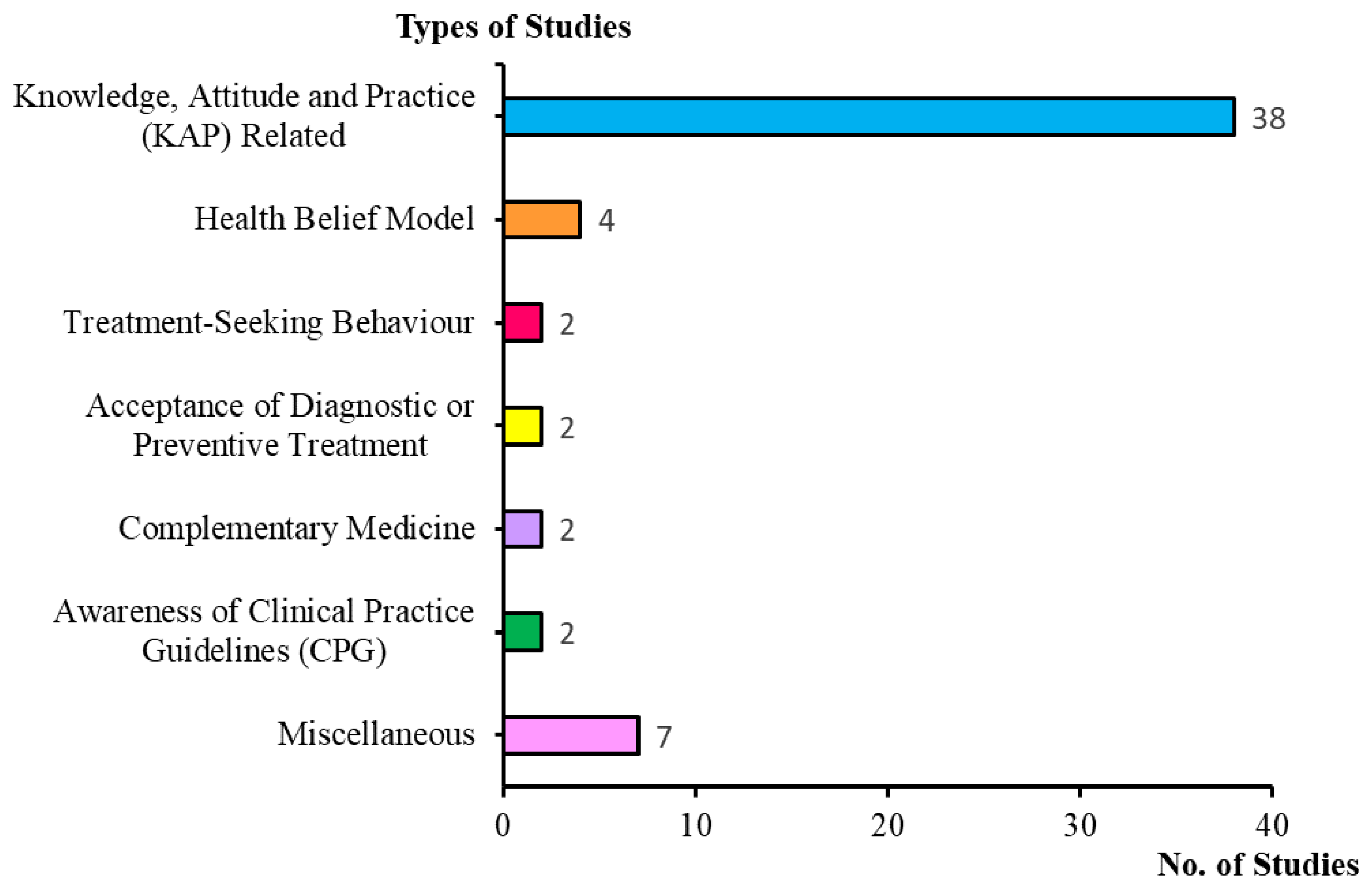
3.1. Quantitative Analysis and Comparison of Recruited Questionnaire-Based Dengue Studies in Malaysia
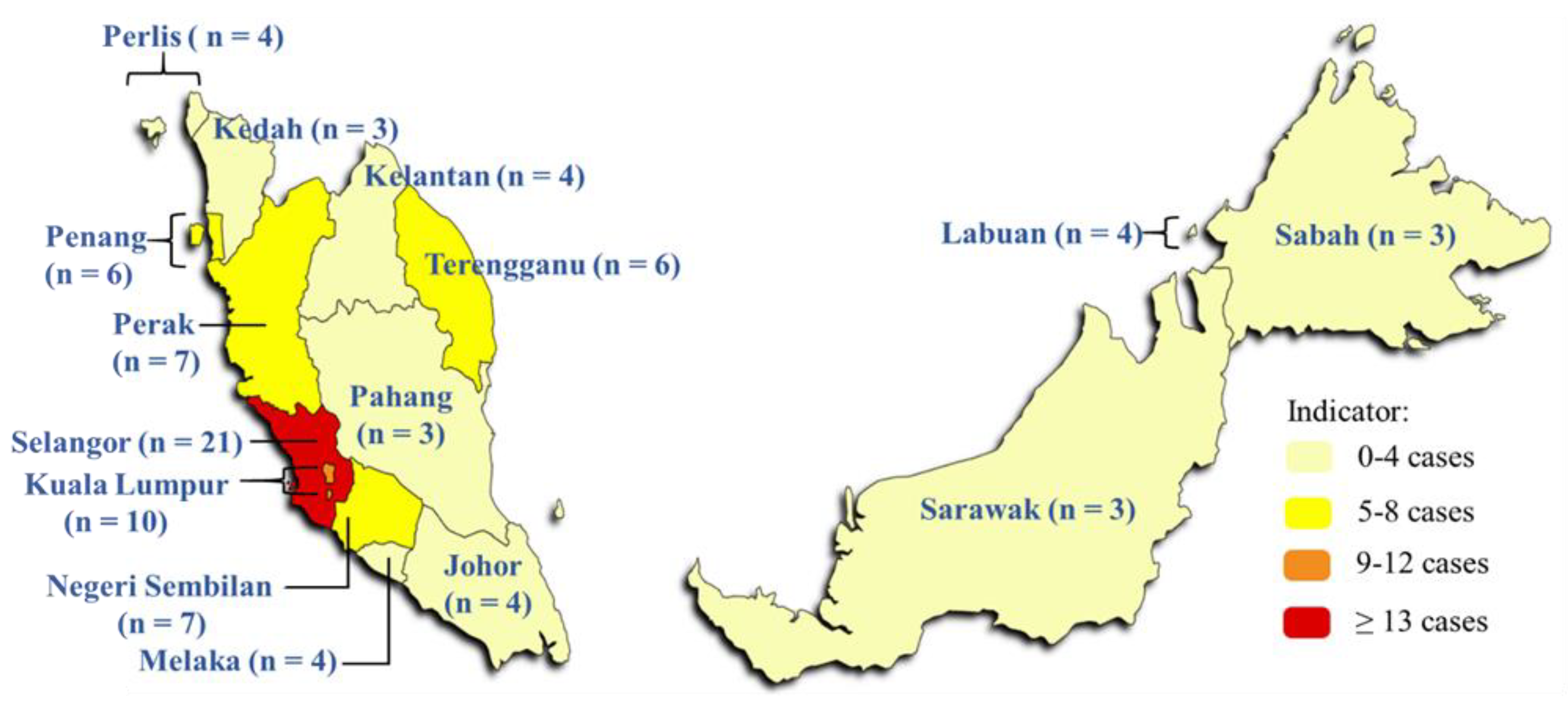
3.2. Location of Study
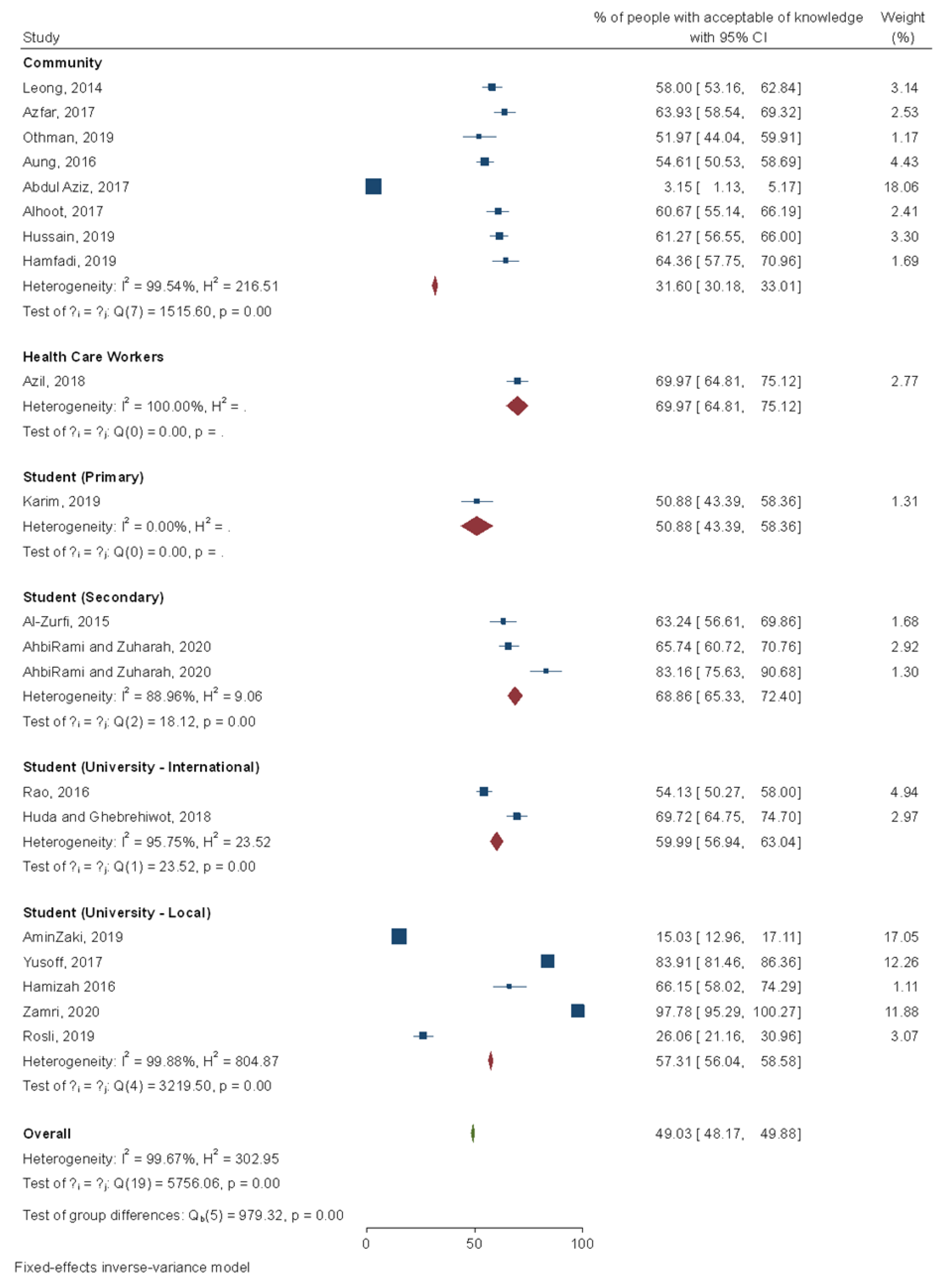
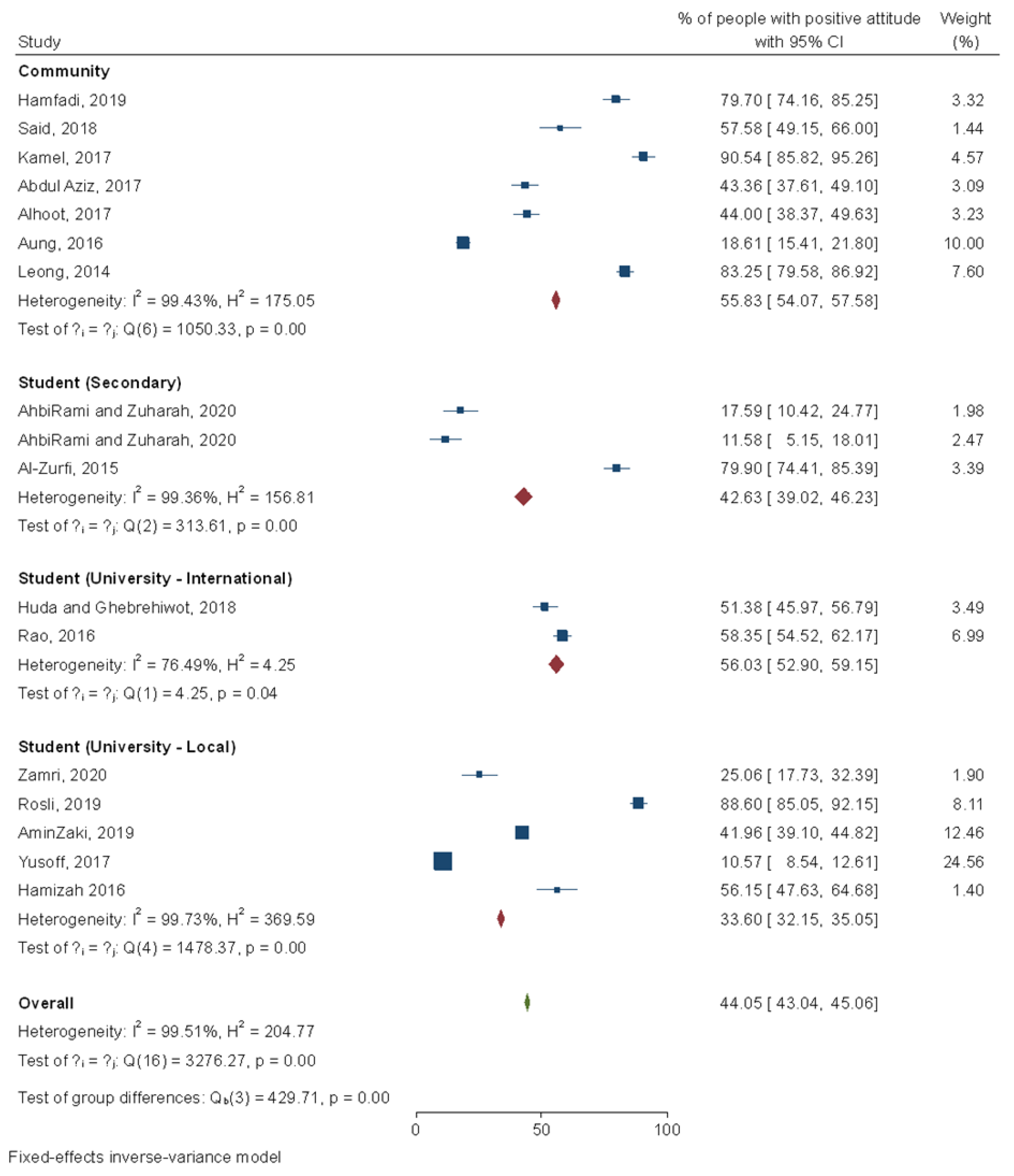
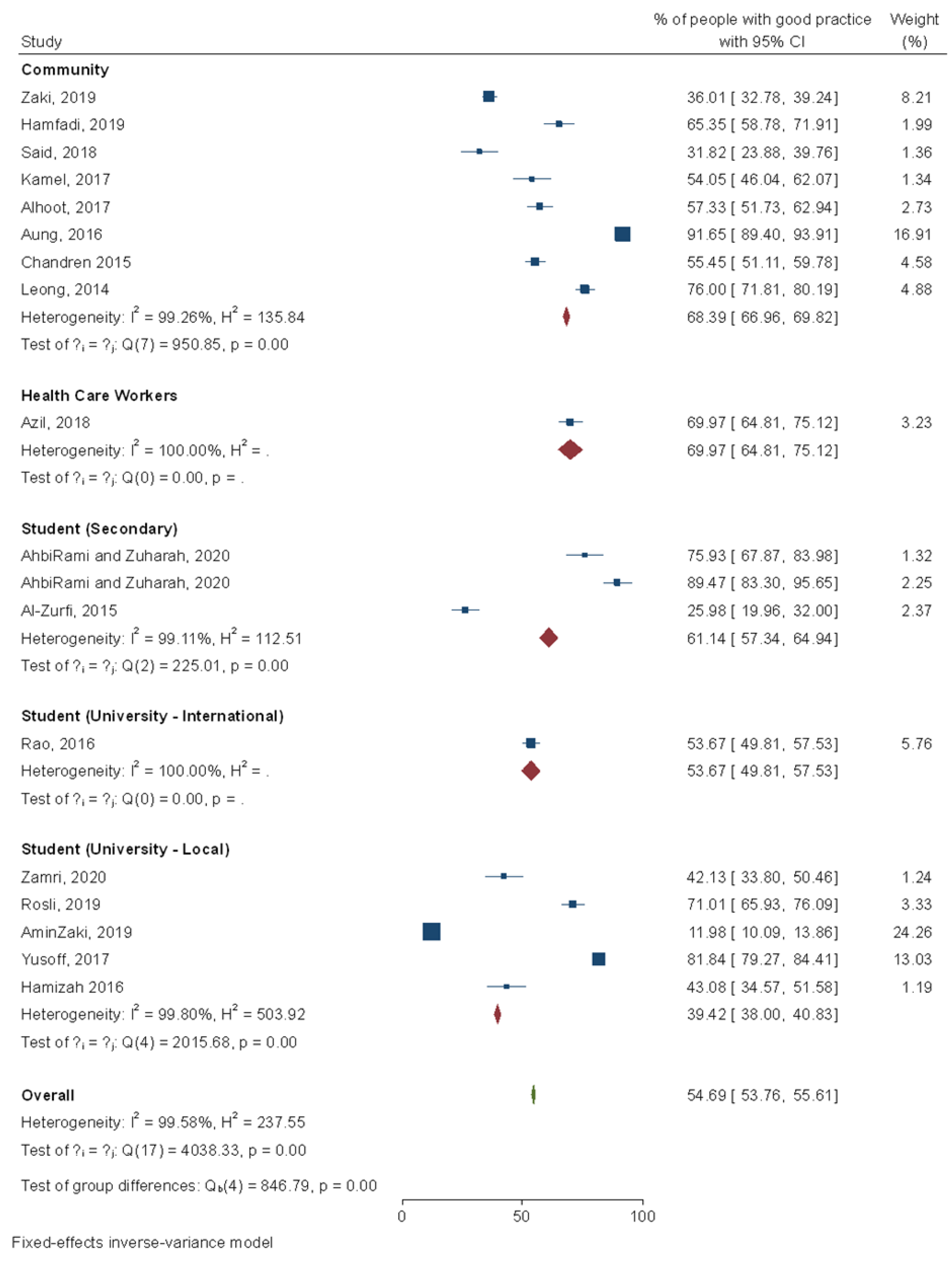
3.3. KAP towards Dengue Infection
3.4. Treatment-Seeking Behaviour
3.5. Acceptance of Diagnostic and Preventive Treatment
3.6. CAM for Dengue Prevention
3.7. Health Belief Association with Dengue Infection
3.8. Awareness and Utilization of Clinical Practice Guidelines (CPG)
3.9. Sources of Information on Dengue
3.10. Reliability and Validity of the Questionnaire
4. Discussion
4.1. Knowledge, Attitude, and Practice towards Dengue Infection
4.2. Treatment-Seeking Behaviour
4.3. Acceptance of Diagnostic and Preventive Treatment
4.4. CAM as Dengue Treatment
4.5. HBM Construct Association with Dengue Prevention Practices
4.6. Awareness and Utilization of Clinical Practice Guidelines (CPG)
4.7. Sources of Information on Dengue
4.8. Lack of Evidence in the Questionnaire’s Reliability and Validity
Strength and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andaya, B.W.; Andaya, L.Y. A History of Malaysia: Macmillan International Higher Education; Palgrave Macmillan, Saffron House, 6-10 Kirby Street: London, UK, 2016. [Google Scholar]
- Jomo, K.S. Southeast Asia’s Misunderstood Miracle: Industrial Policy and Economic Development in Thailand, Malaysia and Indonesia; Routledge: Oxfordshire, UK, 2019. [Google Scholar]
- Hatta, Z.A.; Ali, I. Poverty reduction policies in Malaysia: Trends, strategies and challenges. Asian Cult. Hist. 2013, 5, 48. [Google Scholar] [CrossRef]
- Tee, E.S.; Yap, R.W.K. Type 2 diabetes mellitus in Malaysia: Current trends and risk factors. Eur. J. Clin. Nutr. 2017, 71, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Chia, Y.C.; Kario, K. Asian management of hypertension: Current status, home blood pressure, and specific concerns in Malaysia. J. Clin. Hypertens. 2020, 22, 497–500. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases Country Profiles 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Yang, L.; Liu, C.; Bi, P.; Vardoulakis, S.; Huang, C. Local actions to health risks of heatwaves and dengue fever under climate change: Strategies and barriers among primary healthcare professionals in Southern China. Environ. Res. 2020, 187. [Google Scholar] [CrossRef]
- Harapan, H.; Michie, A.; Yohan, B.; Shu, P.Y.; Mudatsir, M.; Sasmono, R.T.; Imrie, A. Dengue viruses circulating in Indonesia: A systematic review and phylogenetic analysis of data from five decades. Rev. Med. Virol. 2019, 29, e2037. [Google Scholar] [CrossRef]
- Ryan, S.J.; Carlson, C.J.; Mordecai, E.A.; Johnson, L.R. Global expansion and redistribution of Aedes-borne virus transmission risk with climate change. PLoS Negl. Trop. Dis. 2019, 13, e0007213. [Google Scholar] [CrossRef]
- Mohd-Zaki, A.H.; Brett, J.; Ismail, E.; L’Azou, M. Epidemiology of dengue disease in Malaysia (2000–2012): A systematic literature review. PLoS Negl. Trop. Dis. 2014, 8, e3159. [Google Scholar] [CrossRef]
- Undurraga, E.A.; Halasa, Y.A.; Shepard, D.S. Use of expansion factors to estimate the burden of dengue in Southeast Asia: A systematic analysis. PLoS Negl. Trop. Dis. 2013, 7, e2056. [Google Scholar] [CrossRef]
- Bank, W. Who Is Keeping Score? Estimating the Number of Foreign Workers in Malaysia; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Allerton, C. Invisible children? Non-recognition, humanitarian blindness and other forms of ignorance in Sabah, Malaysia. Crit. Anthropol. 2020, 40, 455–470. [Google Scholar] [CrossRef]
- Carruthers, A.M. Clandestine Movement in the Indonesia-Malaysia Migration Corridor: Roots, Routes, and Realities; ISEAS Yusof Ishak Institute: Singapore, 2017. [Google Scholar]
- Grange, L.; Simon-Loriere, E.; Sakuntabhai, A.; Gresh, L.; Paul, R.; Harris, E. Epidemiological risk factors associated with high global frequency of inapparent dengue virus infections. Front. Immunol. 2014, 5. [Google Scholar] [CrossRef]
- Zulfikar, A. The Dynamics of Bugis Diaspora in the Development of Work Migration to Sabah Malaysia. arxiv 2019. [Google Scholar]
- Dollah, R.; Abdullah, K. The securitization of migrant workers in Sabah, Malaysia. J. Int. Migr. Integr. 2018, 19, 717–735. [Google Scholar] [CrossRef]
- Teng, A.K.; Singh, S. Epidemiology and new initiatives in the prevention and control of dengue in Malaysia. Dengue Bull. 2001, 25, 7–14. [Google Scholar]
- Chong, Z.L.; Sekaran, S.D.; Soe, H.J.; Peramalah, D.; Rampal, S.; Ng, C.W. Diagnostic accuracy and utility of three dengue diagnostic tests for the diagnosis of acute dengue infection in Malaysia. BMC Infect. Dis. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Chrostek, E.; Hurst, G.D.; McGraw, E.A. Infectious diseases: Antiviral Wolbachia limits dengue in malaysia. Curr. Biol. 2020, 30, R30–R32. [Google Scholar] [CrossRef]
- Taherdoost, H. Validity and reliability of the research instrument. How Test Valid. Quest. Surv. Res. 2016. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef]
- Zeng, X.; Zhang, Y.; Kwong, J.S.; Zhang, C.; Li, S.; Sun, F.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid. Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- Zamri, S.; Rahman, N.A.A.; Haque, M. Knowledge, attitude, and practice regarding dengue among Kuantan medical campus students of international Islamic university of Malaysia. Bangladesh J. Med. Sci. 2020, 19, 245–253. [Google Scholar] [CrossRef]
- AhbiRami, R.; Zuharah, W.F. School-based health education for dengue control in Kelantan, Malaysia: Impact on knowledge, attitude and practice. PLoS Negl. Trop. Dis. 2020, 14, e0008075. [Google Scholar] [CrossRef]
- Fenga, H.S.; Hashim, N.A.; Kamaruddin, N.A.; Syahida, N.; Kamarudin, W.; Basari, N.A. Preliminary survey on the level of awareness of dengue control programmes among residences in Kuala Terengganu. Univ. Malays. Teren. J. Undergrad. Res. 2020, 2, 55–60. [Google Scholar]
- Othman, H.; Karim, N.; Abd Rashid, N.A.; Abas, M.B.H.; Sahani, M.; Hod, R.; Daud, F.; Nordin, S.A.; Nor, N.A.M. Applying health belief model for the assessment of community knowledge, attitude and prevention practices following a dengue epidemic in a township in Selangor, Malaysia. Int. J. Commun. Med. Public Health 2019, 6, 958–970. [Google Scholar] [CrossRef]
- Zaki, R.; Roffeei, S.N.; Hii, Y.L.; Yahya, A.; Appannan, M.; Said, M.A.; Wan, N.C.; Aghamohammadi, N.; Hairi, N.N.; Bulgiba, A.; et al. Public perception and attitude towards dengue prevention activity and response to dengue early warning in Malaysia. PLoS ONE 2019, 14. [Google Scholar] [CrossRef]
- Rosli, W.R.W.; Rahman, S.A.; Parhar, J.K.; Suhaimi, M.I. Positive impact of educational intervention on knowledge, attitude, and practice towards dengue among university students in Malaysia. J. Public Health 2019, 27, 461–471. [Google Scholar] [CrossRef]
- Mahalingam, S.R.; Abdullah, A.H.; Tiong, C.S.; Arshad, K.; Ming, L.C.; Lean, Q.Y. Mobile health interventions for vector control in dengue prone areas in Malaysia. J. Sustain. Sci. Manag. 2019, 14, 87–97. [Google Scholar]
- Abas, B.H.; Sahani, M.A.Z.R.U.R.A.; Nordin, R.H.; Azlan, S. Knowledge and practices regarding Aedes control amongst residents of dengue hotspot areas in Selangor: A cross-sectional study. Sains Malays. 2019, 48, 841–849. [Google Scholar]
- Fatimah, S.; WO, W.N.A.; AZ, M.A.; Razif, D. Knowledge, Attitude and Practice towards Dengue Fever among University Students. KnE Life Sci. 2019, 53–63. [Google Scholar]
- Kai, L.Y.; Yu, C.Y.; Yee, K.P.; Abdullah, S.N.; Hang, T.Q.; Rahimi, A.; Yusop, M.S.; Ismail, F.Z.; Farid, N.D.N.; How, L.S.; et al. Perceptions, attitudes, and responses to dengue early warning among urban community in Kuala Lumpur. Malays. J. Public Health Med. 2019, 19, 149–159. [Google Scholar] [CrossRef]
- Karim, N.; Ishak, I.; Hum, W.L.; Othman, H. Knowledge About Aedes Mosquitoes, Dengue Fever and Zika Virus among Primary School Students in the Dengue Cluster Areas of Hulu Langat, Selangor. Malays. J. Health Sci. 2019, 17. [Google Scholar] [CrossRef]
- Hussain, R.S.; Davinder, S.; Rahul, S.; Ahmad, H.; Aqila, M.N.; Zharif, R. Study on knowledge, practice of preventive measures and its effectiveness on health promotion on dengue among the residents of a village in Ipoh, Perak. Asian J. Med. Health Sci. 2019, 2, 31. [Google Scholar]
- Ghani, N.A.; Shohaimi, S.; Hee, A.K.W.; Chee, H.Y.; Emmanuel, O.; Alaba Ajibola, L.S. Comparison of knowledge, attitude, and practice among communities living in hotspot and non-hotspot areas of dengue in Selangor, Malaysia. Trop. Med. Infect. Dis. 2019, 4, 37. [Google Scholar] [CrossRef]
- Maung, T.M.; Fernandez, K. Knowledge and Attitude on Dengue Fever and Practice on Preventive Measures among Malaysia Medical Students. IOSR J. Dent. Med. Sci. 2019, 18, 53–59. [Google Scholar]
- Hamfadi, N.S.; Rasudin, N.S.; Ghafar, N.A. Household survey on attitude and practice toward dengue infection among rural dwellers. Int. J. Commun. Med. Public Health 2019, 6, 4651. [Google Scholar] [CrossRef]
- Azil, A.H.; Ahmad, N.; Rosam, A.N.R.; Ru, W.M.; Atira, N.; Norizan, F.L.S.; Firdaus, M.Z.M.; Sharip, S. Knowledge and practice regarding dengue fever and acceptance towards wolbachia among Universiti Kebangsaan Malaysia Medical Centre healthcare staff. Malays. J. Public Health Med. 2018, 69–76. [Google Scholar]
- Huda, B.Z.; Ghebrehiwot, L. Factors associated with knowledge and attitude on prevention of dengue fever among international postgraduate students in a Malaysian university. Int. J. Public Health Clin. Sci. 2018, 5, 123–132. [Google Scholar]
- Yeo, H.Y.; Shafie, A.A. The acceptance and willingness to pay (WTP) for hypothetical dengue vaccine in Penang, Malaysia: A contingent valuation study. Cost Effect. Resour. Alloc. 2018, 16, 1–10. [Google Scholar] [CrossRef]
- Boo, Y.L.; Liam, C.C.K.; Lim, S.Y.; Look, M.L.; Tan, M.H.; Ching, S.M.; Wan, J.L.; Chin, P.W.; Hoo, F.K. Stress and burnout syndrome in health-care providers treating dengue infection: A cross-sectional study. Med. J. Malays. 2018, 73, 371. [Google Scholar]
- Amanah, M.; Abdullah, H.; Ghafar, N. Knowledge attitude and practice on dengue among university students. Int. J. Commun. Med. Public Health 2018, 5, 4720–4724. [Google Scholar] [CrossRef]
- Said, M.F.F.; Abdullah, H.; Ghafar, N.A. Dengue prevention practices among community in dengue hotspot area. Int. J. Commun. Med. Public Healh 2018, 5, 4664. [Google Scholar] [CrossRef]
- Kamel, M.N.A.M.; Gnanakkan, B.D.; Fauzi, F.Z.; Hanafi, M.I.; Selvarajah, G.; Jabar, S.A.; Abd Hamid, S. The KAP study on dengue among community in Taman Salak Baiduri, Sepang, Selangor. Int. J. Sci. Healthc. Res. 2017, 18, 2. [Google Scholar]
- Yussof, F.M.; Hassan, A.; Zin, T.; Hussin, T.M.A.R.; Kadarman, N.; Umar, R. Knowledge of dengue among students in Universiti Sultan Zainal Abidin (UNISZA), Terengganu, Malaysia and the influence of knowledge of dengue on attitude and practice. J. Fundam. Appl. Sci. 2017, 9, 199–216. [Google Scholar] [CrossRef]
- Firdous, J.; Mohamed, A.; Al Amin, M.; Ihsan, M.; Faris’Imadi, M.; Hakim, M.K.; Afiq, M.; Muhamad, N. Knowledge, attitude and practice regarding dengue infection among Ipoh community, Malaysia. J. Appl. Pharm. Sci. 2017, 7, 99–103. [Google Scholar]
- Lugova, H.; Wallis, S. Cross-sectional survey on the dengue knowledge, attitudes and preventive practices among students and staff of a public university in Malaysia. J. Commun. Health 2017, 42, 413–420. [Google Scholar] [CrossRef]
- Azfar, M.; Omarulharis, S.; Azfar, H.; Maryam, A.; Hafizah, S.; Adibah, B.A.H.; Akmal, N. Knowledge, attitude and practice of dengue prevention among sub urban community in Sepang, Selangor. Int. J. Public Health Clin. Sci. 2017, 4, 73–83. [Google Scholar]
- AA, K.H.; Razman, M.R.; Jamalludin, A.R.; Nasreen, E.H.; Phyu, H.M.; SweSwe, L.; Hafizah, P. Knowledge, attitude and practice on dengue among adult population in Felda Sungai Pancing Timur, Kuantan, Pahang. IIUM Med. J. Malays. 2017, 16. [Google Scholar] [CrossRef]
- Alhoot, M.A.; Baobaid, M.F.; Al-Maleki, A.R.; Abdelqader, M.A.; Paveetran, A.; Bathmanathan, L.; Murugan, A.; Maniam, L. Knowledge, attitude, and practice towards dengue fever among patients in Hospital Taiping. Malays. J. Public Health Med. 2017, 17, 66–75. [Google Scholar] [CrossRef]
- Fatini, N.; Mangantig, E.; Soon, L.K. Factors associated with dengue knowledge of signs and symptoms, and treatment-seeking behavior among community in a dengue hotspot area in Malaysia. Int. J. Public Health Clin. Sci. 2017, 4, 64–75. [Google Scholar]
- Ariff, M.I.; Yahya, A.; Zaki, R.; Sarimin, R.; Mohamed Ghazali, I.M.; Gill, B.S.; Suli, Z.; Mohd Yusof, M.A.; Ahmad Lutfi, N.; Thye, S.L.; et al. Evaluation of awareness & utilisation of clinical practise guideline for management of adult Dengue infection among Malaysia doctors. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Mia, M.S.; Begum, R.A.; Er, A.C.; Pereira, J.J. Assessing the cost burden of dengue infection to households in Seremban, Malaysia. Southeast Asian J. Trop. Med. Public Health 2016, 47, 1167–1176. [Google Scholar]
- Rao, G.; Minhat, H.S.; Hayati, K.S. Predictors of practices related to dengue fever prevention among international students in Universiti Putra Malaysia, Serdang. Int. J. Public Health Clin. Sci. 2016, 3, 36–47. [Google Scholar]
- Danial, M.; Subramaniam, S.; Kin, Y.C.; Meng, O.L. External Factors Governing Dengue Outbreaks and Practices Associated in Curbing Dengue Infections among Population in Northern Malaysia. Age 2016, 18, 185. [Google Scholar]
- Aung, M.M.T.; Hassan, A.B.; Kadarman, N.B.; Hussin, T.M.; Barman, A.; Ismail, S.B.; Hashim, S.E. Knowledge, attitude, practices related to dengue fever among rural population in Terengganu, Malaysia. Malays. J. Public Health Med. 2016, 16, 15–23. [Google Scholar]
- Mahyiddin, N.S.; Mohamed, R.; Mohamed, H.J.J.; Ramly, N. High knowledge on dengue but low preventive practices among residents in a low cost flat in Ampang, Selangor. Malays. J. Nurs. 2016, 8, 39–48. [Google Scholar]
- Sumayyah, A.; Fadzly, N.; Zuharah, W.F. Current observation on Aedes mosquitoes: A survey on implication of dengue infection, human lifestyle and preventive measure among Malaysia resident in urban and sub-urban areas. Asian Pac. J. Trop. Dis. 2016, 6, 841–849. [Google Scholar] [CrossRef]
- Wong, L.P.; Atefi, N.; AbuBakar, S. Nationwide study of factors associated with public’s willingness to use home self-test kit for dengue fever in Malaysia. BMC Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef]
- Ng, S.W.; Lim, S.Y.; Beth, M. A study to determine the effectiveness of health education on knowledge of dengue fever and preventive measures among high school students in a selected private school, Malaysia. Int. J. Contemp. Pediatr. 2016, 3, 553–558. [Google Scholar] [CrossRef][Green Version]
- Hamizah, K.; Olivia, L.J.; Anita, A.R.; BB, M.R. Risk Assessment on Dengue among UPM students. Int. J. Public Health Clin. Sci. 2016, 3, 132–140. [Google Scholar]
- Juni, M.H.; Hayati, K.S.; Cheng, C.M.; Pyang, G.S.; Abd Samad, N.H.B.; Bt, Z.S.B.Z.A.; Abidin, Z. Risk behaviour associated with dengue fever among rural population in Malaysia. Int. J. Public Health Clin. Sci. 2015, 2, 114–127. [Google Scholar]
- Chandren, J.R.; Wong, L.P.; AbuBakar, S. Practices of dengue fever prevention and the associated factors among the Orang Asli in Peninsular Malaysia. PLoS Negl. Trop. Dis. 2015, 9. [Google Scholar] [CrossRef]
- Al-Zurfi, B.M.; Fuad, M.D.; Abdelqader, M.A.; Baobaid, M.F.; Elnajeh, M.; Ghazi, H.F.; Ibrahim, M.H.; Abdullah, M.R. Knowledge, attitude and practice of dengue fever and health education programme among students of Alam Shah Science School, Cheras, Malaysia. Practice 2015, 15, 69–74. [Google Scholar]
- Hamid, M.; Lugova, H.; Mon, A.; Knight, V. Awareness and practice related to dengue infection among military cadets in Malaysia. J. Behav. Health 2015, 4, 1. [Google Scholar] [CrossRef]
- Ching, S.; Ramachandran, V.; Gew, L.T.; Lim, S.M.S.; Sulaiman, W.A.W.; Foo, Y.L.; Zakaria, Z.A.; Samsudin, N.H.; Lau, P.C.M.C.; Veettil, S.K.; et al. Complementary alternative medicine use among patients with dengue fever in the hospital setting: A cross-sectional study in Malaysia. BMC Complement. Altern. Med. 2015, 16, 1–7. [Google Scholar] [CrossRef]
- Wong, L.P.; AbuBakar, S.; Chinna, K. Community knowledge, health beliefs, practices and experiences related to dengue fever and its association with IgG seropositivity. PLoS Negl. Trop. Dis. 2014, 8, 2789. [Google Scholar] [CrossRef]
- Ariffin, F.; Ramli, A.S.; Nuratifah, N.A.I.M.; Selamat, M.I.; Syed-Jamal, S.J. Recognizing Life-threatening Features of Dengue in Children and Health Seeking Behavior in Dengue Emergency Amongst Parents and Carers: A Cross-sectional study in Gombak District, Malaysia. Med. J. Malays. 2014, 69, 211. [Google Scholar]
- Abd Rahman, A.; Zainuddin, H.; Minhat, H.S.; Juni, M.H.; Mazeli, M.I. Community perception towards Dengue and Dengue Prevention Program among residences of a rural settlement in Jempol, Negeri Sembilan. Int. J. Public Health Clin. Sci. 2014, 1, 13–26. [Google Scholar]
- Leong, T.K. Knowledge, attitude and practice on dengue among rural communities in Rembau and Bukit Pelanduk, Negeri Sembilan, Malaysia. Int. J. Trop. Dis. Health 2014, 4, 841–848. [Google Scholar] [CrossRef]
- Mohamad, M.; Selamat, M.I.; Ismail, Z. Factors associated with larval control practices in a dengue outbreak prone area. J. Environ. Public Health 2014, 2014. [Google Scholar] [CrossRef]
- Ken, C.C.; Aan, G.J.; Hamdi, C.H.H.; Ibrahim, O.A.M.; Maskon, O. Impact on Knowledge in Dengue Management among Medical and Paramedical Personnel Following Attendance to Educational Lectures; 2014. [Google Scholar]
- Al-Dubai, S.A.; Ganasegeran, K.; Mohanad Rahman, A.; Alshagga, M.A.; Saif-Ali, R. Factors affecting dengue fever knowledge, attitudes and practices among selected urban, semi-urban and rural communities in Malaysia. Southeast Asian J. Trop. Med. Public Health 2013, 44, 37–49. [Google Scholar]
- Isa, A.; Loke, Y.K.; Smith, J.R.; Papageorgiou, A.; Hunter, P.R. Mediational effects of self-efficacy dimensions in the relationship between knowledge of dengue and dengue preventive behaviour with respect to control of dengue outbreaks: A structural equation model of a cross-sectional survey. PLoS Negl. Trop. Dis. 2013, 7, 2401. [Google Scholar] [CrossRef]
- Burhanuddin, M.A.; Abdullah, M.N.; Azib, W.N.H.W.; Harun, M.F.M. Comparison of Mean Knowledge on Age, Location and Education Level towards Dengue Fever Prevention. Methodology 2013, 3. [Google Scholar]
- Naing, C.; Ren, W.Y.; Man, C.Y.; Fern, K.P.; Qiqi, C.; Ning, C.N.; Ee, C.W.S. Awareness of dengue and practice of dengue control among the semi-urban community: A cross sectional survey. J. Commun. Health 2011, 36, 1044–1049. [Google Scholar] [CrossRef] [PubMed]
- Ang, K.T.; Rohani, I.; Look, C.H. Role of primary care providers in dengue prevention and control in the community. Med. J. Malays. 2010, 65, 58–62. [Google Scholar]
- Wan Rozita, W.M.; Yap, B.W.; Veronica, S.; Muhammad, A.K.; Lim, K.H.; Sumarni, M.G. Knowledge, attitude and practice (KAP) survey on dengue fever in an urban Malay residential area in Kuala Lumpur. Malays. J. Public Health Med. 2006, 6, 62–67. [Google Scholar]
- Hairi, F.; Ong, C.H.; Suhaimi, A.; Tsung, T.W.; Bin Anis Ahmad, M.A.; Sundaraj, C.; Soe, M.M. A Knowledge, Attitude and Practices (KAP) Study on Dengue among Selected Rural Communities in the Kuala Kangsar District; Sage Publications Sage CA: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Thomas, S.J.; Yoon, I.K. A review of Dengvaxia®: Development to deployment. Human Vaccine Immunother. 2019, 15, 2295–2314. [Google Scholar] [CrossRef]
- Yboa, B.C.; Labrague, L.J. Dengue knowledge and preventive practices among rural residents in Samar province, Philippines. Am. J. Public Health Res. 2013, 1, 47–52. [Google Scholar] [CrossRef]
- Harapan, H.; Rajamoorthy, Y.; Anwar, S.; Bustamam, A.; Radiansyah, A.; Angraini, P.; Fasli, R.; Salwiyadi, S.; Bastian, R.A.; Oktiviyari, A.; et al. Knowledge, attitude, and practice regarding dengue virus infection among inhabitants of Aceh, Indonesia: A cross-sectional study. BMC Infect. Dis. 2018, 18, 1–16. [Google Scholar] [CrossRef]
- Koenraadt, C.J.; Tuiten, W.; Sithiprasasna, R.; Kijchalao, U.; Jones, J.W.; Scott, T.W. Dengue knowledge and practices and their impact on Aedes aegypti populations in Kamphaeng Phet, Thailand. Am. J. Trop. Med. Hyg. 2006, 74, 692–700. [Google Scholar] [CrossRef]
- Prashar, P.K.; Dutta, S.; Neha, K.B.; Taylor-Robinson, A.W.; Singh, A. Knowledge, Attitude and Practices of Univer-sity Students towards Prevention of Dengue in Northern India: A Questionnaire-Based Study. Emerg. Infect. Dis. Diag. J. 2019. [Google Scholar]
- Xu, J.W.; Liu, H.; Yaw, B.; Nbwi, H.S. The health beliefs, dengue knowledge and control behaviors among internally displaced persons versus local residents in Kachin Special Region II, Myanmar. PLoS Negl. Trop. Dis. 2020, 14, 0008321. [Google Scholar] [CrossRef]
- Santhi, H.; Marsaulina, I. Knowledge, Attitudes, Income and Implementation Regarding the Dengue Fever Prevention Program in Medan, Indonesia. Br. Int. Exact Sci. J. 2020, 2, 77–83. [Google Scholar]
- Wijayanti, S.P.M.; Octaviana, D.; Asti, A.D. Lack of knowledge and false perception on space spraying against dengue in endemic area. Int. J. Public Health 2020, 9, 207–213. [Google Scholar]
- Kaushik, S.C.; Singh, S.; Srivastava, P. Assessment of Knowledge, Attitude and Practices in different Socio-Economic Groups of Population on Control of Dengue and its Vectors in Delhi. J. Commun. Dis. 2019, 51, 16–21. [Google Scholar]
- Boonchutima, S.; Kachentawa, K.; Limpavithayakul, M.; Prachansri, A. Longitudinal study of Thai people media exposure, knowledge, and behavior on dengue fever prevention and control. J. Infect. Public Health 2017, 10, 836–841. [Google Scholar] [CrossRef]
- Dhimal, M.; Aryal, K.K.; Dhimal, M.L.; Gautam, I.; Singh, S.P.; Bhusal, C.L.; Kuch, U. Knowledge, attitude and practice regarding dengue fever among the healthy population of highland and lowland communities in central Nepal. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Murphy, A.; Rajahram, G.S.; Jilip, J.; Maluda, M.; William, T.; Hu, W.; Reid, S.; Devine, G.J.; Frentiu, F.D. Incidence and epidemiological features of dengue in Sabah, Malaysia. PLoS Negl. Trop. Dis. 2020, 14. [Google Scholar] [CrossRef]
- Department of Statistics Malaysia. Population Distribution and Basic Demographic Characteristics. In Population and Housing Census of Malaysia; Department of Statistics Malaysia: Putrajaya, Malaysia, 2010. [Google Scholar]
- Greenaway, C.; Castelli, F. Infectious diseases at different stages of migration: An expert review. J. Travel Med. 2019, 26. [Google Scholar] [CrossRef]
- Karmakar, P.R.; Saharay, S. Study on Knowledge and Practice Regarding Dengue among Medical Students in Kolkata, West Bengal. Vaccine 2020, 102, 64–115. [Google Scholar]
- Meena, J.S.; Mahore, R.; Sahay, A.; Sengar, S.S. Assessing level of pre and post interventional knowledge and attitude for dengue awareness among selected government school student of Bhopal, India. Int. J. Commun. Med. Public Health 2020, 7, 1095. [Google Scholar] [CrossRef][Green Version]
- Rahman, M.S.; Karamehic-Muratovic, A.; Baghbanzadeh, M.; Amrin, M.; Zafar, S.; Rahman, N.N.; Shirina, S.U.; Haque, U. Climate change and dengue fever knowledge, attitudes and practices in Bangladesh: A social media–based cross-sectional survey. Transact. R. Soc. Trop. Med. Hyg. 2021, 115, 85–93. [Google Scholar] [CrossRef]
- Nguyen, P.V.; Vo, T.Q.; Nguyen, T.D.; TT, C.P. Dengue fever in Southern of Vietnam: A survey of reported knowledge, attitudes, and practices. JPMA J. Pak. Med. Assoc. 2019, 69, 118–130. [Google Scholar]
- Khun, S.; Manderson, L. Community and school-based health education for dengue control in rural Cambodia: A process evaluation. PLoS Negl. Trop. Dis. 2007, 1, 143. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.V.; Than, P.Q.T.; Nguyen, T.H.; Vu, G.T.; Hoang, C.L.; Tran, T.T.; Truong, N.T.; Nguyen, S.H.; Do, H.P.; Ha, G.H.; et al. Knowledge, attitude and practice about dengue fever among patients experiencing the 2017 outbreak in Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 976. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Xu, J.W.; Ai, Z.; Yu, Y.; Yu, B. Treatment seeking behavior and associated factors of suspected dengue fever among Shan people in eastern Shan special region IV, Myanmar: A cross-sectional study. BMC Health Serv. Res. 2020, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Elsinga, J.; Lizarazo, E.F.; Vincenti, M.F.; Schmidt, M.; Velasco-Salas, Z.I.; Arias, L.; Bailey, A.; Tami, A. Health seeking behaviour and treatment intentions of dengue and fever: A household survey of children and adults in Venezuela. PLoS Negl. Trop. Dis. 2015, 9. [Google Scholar] [CrossRef]
- Cui, E.R.; Beja-Glasser, A.; Fernandez, A.R.; Grover, J.M.; Mann, N.C.; Patel, M.D. Emergency medical services time intervals for acute chest pain in the United States, 2015–2016. Prehosp. Emerg. Care 2020, 24, 557–565. [Google Scholar] [CrossRef]
- Krisnian, T.; Alisjahbana, B.; Afriandi, I. Treatment seeking patterns among dengue fever patients: A qualitative study. Althea Med. J. 2017, 4, 369–374. [Google Scholar]
- Khun, S.; Manderson, L. Health seeking and access to care for children with suspected dengue in Cambodia: An ethnographic study. BMC Public Health 2007, 7, 1–10. [Google Scholar] [CrossRef]
- Muzaffar, D.; Mahdey, H.M.; Sonjaya, D.; Zafar, M.S. Tendency of self-medication among various malaysian ethnicities. J. Pharm. Res. Int. 2016, 1–7. [Google Scholar] [CrossRef]
- Ismail, I.S.; Hairon, S.M.; Yaacob, N.M.; Besari, A.M.; Abdullah, S. Usage of Traditional and Complementary Medicine among Dengue Fever Patients in the Northeast Region of Peninsular Malaysia. Malays. J. Med. Sci. 2019, 26, 90. [Google Scholar] [CrossRef]
- Vasikasin, V.; Rojdumrongrattana, T.; Chuerboonchai, W.; Siriwiwattana, T.; Thongtaeparak, W.; Niyasom, S.; Lertliewtrakool, N.; Jitsiri, S.; Changpradub, D. Effect of standard dose paracetamol versus placebo as antipyretic therapy on liver injury in adult dengue infection: A multicentre randomised controlled trial. Lancet Glob. Health 2019, 7, 664–670. [Google Scholar] [CrossRef]
- Harapan, H.; Anwar, S.; Setiawan, A.M.; Sasmono, R.T. Dengue vaccine acceptance and associated factors in Indonesia: A community-based cross-sectional survey in Aceh. Vaccine 2016, 34, 3670–3675. [Google Scholar] [CrossRef]
- World Health Organization. Dengue vaccine: WHO position paper, July 2016–recommendations. Vaccine 2017, 35, 1200–1201. [Google Scholar] [CrossRef]
- Lenselink, C.H.; Schmeink, C.E.; Melchers, W.J.G.; Massuger, L.F.A.G.; Hendriks, J.C.M.; Van Hamont, D.; Bekkers, R.L.M. Young adults and acceptance of the human papillomavirus vaccine. Public Health 2008, 122, 1295–1301. [Google Scholar] [CrossRef]
- Eppes, C.; Wu, A.; Cameron, K.A.; Garcia, P.; Grobman, W. Does obstetrician knowledge regarding influenza increase HINI vaccine acceptance among their pregnant patients? Vaccine 2012, 30, 5782–5784. [Google Scholar] [CrossRef]
- Ministry of Health Republic of Indonesia. Indonesia Health Profile 2010; Center for data and information Jakarta Center for Data and Information, Ministry of Health Republic of Indonesia: Jakarta, Indonesia, 2011. [Google Scholar]
- Hopkins, T.G.; Wood, N. Female human papillomavirus (HPV) vaccination: Global uptake and the impact of attitudes. Vaccine 2013, 31, 1673–1679. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Raude, J.; Sagaon-Teyssier, L.; Constant, A.; Verger, P.; Beck, F. Attitudes toward vaccination and the H1N1 vaccine: Poor people’s unfounded fears or legitimate concerns of the elite? Soc. Sci. Med. 2014, 109, 10–18. [Google Scholar] [CrossRef]
- Taddei, C.; Ceccherini, V.; Niccolai, G.; Porchia, B.R.; Boccalini, S.; Levi, M.; Tiscione, E.; Santini, M.G.; Baretti, S.; Bonanni, P.; et al. Attitude toward immunization and risk perception of measles, rubella, mumps, varicella, and pertussis in health care workers working in 6 hospitals of Florence, Italy 2011. Human Vaccine Immunother. 2014, 10, 2612–2622. [Google Scholar] [CrossRef]
- Valido, E.M.; Laksanawati, I.S.; Utarini, A. Acceptability of the dengue vaccination among parents in urban poor communities of Quezon City, Philippines before and after vaccine suspension. BMC Res. Notes 2018, 11, 1–5. [Google Scholar] [CrossRef]
- Siti, Z.M.; Tahir, A.; Farah, A.I.; Fazlin, S.A.; Sondi, S.; Azman, A.H.; Maimunah, A.H.; Haniza, M.A.; Haslinda, M.S.; Zulkarnain, A.K.; et al. Use of traditional and complementary medicine in Malaysia: A baseline study. Complement. Ther. Med. 2009, 17, 292–299. [Google Scholar] [CrossRef]
- Yamashita, H.; Tsukayama, H.; Sugishita, C. Popularity of complementary and alternative medicine in Japan: A telephone survey. Complement. Ther. Med. 2002, 10, 84–93. [Google Scholar] [CrossRef]
- Seo, H.J.; Baek, S.M.; Kim, S.G.; Kim, T.H.; Choi, S.M. Prevalence of complementary and alternative medicine use in a community-based population in South Korea: A systematic review. Complement. Ther. Med. 2013, 21, 260–271. [Google Scholar] [CrossRef]
- Lim, M.K.; Sadarangani, P.; Chan, H.L.; Heng, J.Y. Complementary and alternative medicine use in multiracial Singapore. Complement. Ther. Med. 2005, 13, 16–24. [Google Scholar] [CrossRef]
- Rahayu, Y.Y.S.; Araki, T.; Rosleine, D. Factors affecting the use of herbal medicines in the universal health coverage system in Indonesia. J. Ethnopharmacol. 2020, 260. [Google Scholar] [CrossRef]
- Yunita, F.; Hanani, E.; Kristianto, J. The effect of Carica papaya L. leaves extract capsules on platelets count and hematocrit level in dengue fever patient. Int. J. Med. Aromat. Plants 2012, 2, 573–578. [Google Scholar]
- Madjos, G.G.; Luceño, A.M. Comparative cytotoxic properties of two varieties of Carica papaya leaf extracts from Mindanao, Philippines using brine shrimp lethality assay. Bull. Environ. Pharmacol. Life Sci. 2019, 8, 113–118. [Google Scholar]
- Gadhwal, A.K.; Ankit, B.S.; Chahar, C.; Tantia, P.; Sirohi, P.; Agrawal, R.P. Effect of Carica papaya leaf extract capsule on platelet count in patients of dengue fever with thrombocytopenia. J. Assoc. Phys. India 2016, 64, 22–26. [Google Scholar]
- Norahmad, N.A.; Abd Razak, M.R.M.; Misnan, N.M.; Jelas, N.H.M.; Sastu, U.R.; Muhammad, A.; Ho, T.C.D.; Jusoh, B.; Zolkifli, N.A.; Thayan, R.; et al. Effect of freeze-dried Carica papaya leaf juice on inflammatory cytokines production during dengue virus infection in AG129 mice. BMC Complement. Altern. Med. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Butthep, P.; Chunhakan, S.; Yoksan, S.; Tangnararatchakit, K.; Chuansumrit, A. Alteration of cytokines and chemokines during febrile episodes associated with endothelial cell damage and plasma leakage in dengue hemorrhagic fever. Pediatr. Infect. Dis. J. 2012, 31, 232–238. [Google Scholar] [CrossRef]
- Mesana, M.I.; Hilbig, A.; Androutsos, O.; Cuenca-García, M.; Dallongeville, J.; Huybrechts, I.; De Henauw, S.; Widhalm, K.; Kafatos, A.; Nova, E.; et al. Dietary sources of sugars in adolescents’ diet: The HELENA study. Eur. J. Nutr. 2018, 57, 629–641. [Google Scholar] [CrossRef]
- Kovendan, K.; Murugan, K.; Kumar, A.N.; Vincent, S.; Hwang, J.S. Bioefficacy of larvicdial and pupicidal properties of Carica papaya (Caricaceae) leaf extract and bacterial insecticide, spinosad, against chikungunya vector, Aedes aegypti (Diptera: Culicidae). Parasitol. Res. 2012, 110, 669–678. [Google Scholar] [CrossRef]
- Subenthiran, S.; Choon, T.C.; Cheong, K.C.; Thayan, R.; Teck, M.B.; Muniandy, P.K.; Afzan, A.; Abdullah, N.R.; Ismail, Z. Carica papaya leaves juice significantly accelerates the rate of increase in platelet count among patients with dengue fever and dengue haemorrhagic fever. Evid. Based Complement. Altern. Med. 2013. [Google Scholar] [CrossRef] [PubMed]
- Diptyanusa, A.; Kusumasari, R.A.; Satoto, T.B.T. Health Belief Model of Persistent Dengue Transmission in Klaten, Indonesia. Am. J. Health Behav. 2020, 44, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Tapera, R.; Senabye, P.K.; Mhaka-Mutepfa, M.; January, J.; Apau, S.G. The use of the Health Belief Model (HBM) in determining the factors associated with breast cancer screening among female students in Botswana. Int. J. Health Promot. Educ. 2019, 57, 203–216. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. The health belief model and HIV risk behavior change. In Preventing AIDS; Springer: Boston, MA, USA, 1994; pp. 5–24. [Google Scholar]
- Siddiqui, T.R.; Ghazal, S.; Bibi, S.; Ahmed, W.; Sajjad, S.F. Use of the health belief model for the assessment of public knowledge and household preventive practices in Karachi, Pakistan, a dengue-endemic city. PLoS Negl. Trop. Dis. 2016, 10. [Google Scholar] [CrossRef]
- Ahmedov, M.; Green, J.; Azimov, R.; Avezova, G.; Inakov, S.; Mamatkulov, B. Addressing the challenges of improving primary care quality in Uzbekistan: A qualitative study of chronic heart failure management. Health Policy Plan. 2013, 28, 458–466. [Google Scholar] [CrossRef][Green Version]
- Chandler, C.I.; Jones, C.; Boniface, G.; Juma, K.; Reyburn, H.; Whitty, C.J. Guidelines and mindlines: Why do clinical staff over-diagnose malaria in Tanzania? Qual. Stud. Malar. J. 2008, 7, 1–13. [Google Scholar] [CrossRef]
- Hobbs, F.R.; Erhardt, L. Acceptance of guideline recommendations and perceived implementation of coronary heart disease prevention among primary care physicians in five European countries: The Reassessing European Attitudes about Cardiovascular Treatment (REACT) survey. Fam. Pract. 2002, 19, 596–604. [Google Scholar] [CrossRef]
- Wharton-Smith, A.; Green, J.; Loh, E.C.; Gorrie, A.; Omar, S.F.S.; Bacchus, L.; Lum, L.C.S. Using clinical practice guidelines to manage dengue: A qualitative study in a Malaysian hospital. BMC Infect. Dis. 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Chiappelli, F.; Santos, S.M.E.; Brant, X.M.C.; Bakhordarian, A.; Thames, A.D.; Maida, C.A.; Du, A.M.; Jan, A.L.; Nahcivan, M.; Nguyen, M.T.; et al. Viral immune evasion in dengue: Toward evidence-based revisions of clinical practice guidelines. Bioinformation 2014, 10, 726. [Google Scholar] [CrossRef]
- Khan, J.I. Assessing the Readiness of Future Network Cyber Infrastructure in Malaysia—Part-2: Challenges, Opportunities and Recommendations; Kent State University: Kent, OH, USA, 2018. [Google Scholar]
- Schreiber, M.; Job, V.; Dohle, S. Is your health malleable or fixed? The influence of implicit theories on health-related attitudes and behaviour. Psychol. Health 2020, 35, 1421–1439. [Google Scholar] [CrossRef]
- Sundararajan, R.; Mwanga-Amumpaire, J.; King, R.; Ware, N.C. Conceptual model for pluralistic healthcare behaviour: Results from a qualitative study in southwestern Uganda. BMJ Open 2020, 10, 033410. [Google Scholar] [CrossRef]
- Ismail, A.; Nawi, A.M.; Mohamed, A. Communication for Behavioural Impact (COMBI) Program in Dengue Prevention Evaluation: Mixed Methods Approach. Int. Med. J. 2015, 22, 367–370. [Google Scholar]
- Bolarinwa, O.A. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger. Postgrad. Med. J. 2015, 22, 195. [Google Scholar] [CrossRef]
- Engellant, K.A.; Holland, D.D.; Piper, R.T. Assessing convergent and discriminant validity of the motivation construct for the technology integration education (TIE) model. J. High. Educ. Theory Prac. 2016, 16. [Google Scholar]
- Shroff, R.H.; Ting, F.S.T.; Lam, W.H. Development and validation of an instrument to measure students’ perceptions of technology-enabled active learning. Aust. J. Educ. Technol. 2019, 35. [Google Scholar] [CrossRef]
- Ajibola, L.S.A.; Shohaimi, S.; Adam, M.B.; Nadzir, M.N.H.M.; Segun, O.E. Systematic review of knowledge, attitude, and practices regarding dengue in Malaysia. J. Appl. Pharm. Sci. 2018, 8, 80–91. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref | Location of Study | Respondents (N) | Sampling Method and Data Collection Method | Outcome of the Study |
|---|---|---|---|---|
| [24] | IIUM, Kuantan, Pahang | University students (135) | Convenience sampling and self-administered |
|
| [25] | Pasir pekan & Kubang kerian, Kelantan | School students (203) | Convenience sampling and self-administered |
|
| [26] | Kuala Terengganu, Terengganu | Urban, rural residents and university students (286) | Simple random sampling and face-to-face interview |
|
| [27] | Bandar Baru Bangi, Selangor | Residential community (152) | Purposive sampling and self-administered |
|
| [28] | Petaling District, Selangor | Residential community (847) | Convenience sampling and self-administered |
|
| [29] | CUCMS, Selangor | University student (307) | Convenience sampling and self-administered |
|
| [30] | Perak state, Kedah state, Penang | Residential community (379) | Cluster sampling and face-to-face interview |
|
| [31] | Bandar Baru Bangi, Selangor | Residential community (152) | Purposive sampling and self-administered |
|
| [32] | Selangor & Negeri Sembilan | University students (1144) | Convenience sampling and self-administered |
|
| [33] | Titiwangsa district, Kuala Lumpur | Residential community (322) | Purposive sampling and face-to-face interview |
|
| [34] | Hulu Langat District, Selangor | Primary school students (171) | Purposive sampling and self-administered |
|
| [35] | Ipoh, Perak | Residential community (259) | Simple random sampling and self-administered |
|
| [36] | Selangor | Residential community (406) | Systematic random sampling and self-administered |
|
| [37] | AIMST University, Kedah | Medical university students (200) | Simple random sampling and self-administered |
|
| [38] | Besut, Terengganu | Residential community (202) | Simple random selection and self-administered |
|
| [39] | UKMC, Kuala Lumpur | Healthcare provider (330) | Purposive sampling and self-administered |
|
| [40] | UPM, Serdang, Selangor | Postgraduate international students (327) | Simple random sampling and self-administered |
|
| [41] | Penang | Residential community (415) | Convenience sampling and face-to-face interview |
|
| [42] | Malaysia | Medical doctor (313) | Universal sampling and self-administered |
|
| [43] | USM, Penang | University students (250) | Purposive sampling and self-administered |
|
| [44] | Tok Kenali village, Kelantan | Residential community (132) | Convenience sampling and self-administered |
|
| [45] | Sepang, Selangor | Residential community (148) | Universal and simple random sampling and face-to-face interview |
|
| [46] | UniSZA, Terengganu | Hostel residents (870) | Convenience sampling and self-administered |
|
| [47] | Ipoh, Perak | Residential community (86) | Simple random selection and self-administered |
|
| [48] | NDUM, Kuala Lumpur | Military cadet & staff (372) | Stratified random sampling and self-administered |
|
| [49] | Sepang, Selangor | Residential community (305) | Simple random sampling and self-administered |
|
| [50] | Kuantan, Pahang | Residential community (286) | Simple random sampling and face-to-face interview |
|
| [51] | Hospital Taiping, Perak | Inpatients & parents/caretakers (300) | Simple random sampling and self-administered |
|
| [52] | Kubang Kerian, Kelantan | Residential community (218) | Simple random sampling and self-administered |
|
| [53] | Malaysia | Medical doctor (864) | Proportionate multistage random sampling and self-administered |
|
| [54] | Seremban, Negeri Sembilan | Dengue patients (120) | Purposive random sampling and face-to-face interview |
|
| [55] | UPM Serdang, Selangor | International university students (641) | Cluster random sampling and self-administrated |
|
| [56] | Penang General Hospital, Penang | Hospital visitors (337) | Convenience sampling and face-to-face interview |
|
| [57] | Terengganu | Residential community (575) | Purposive sampling and face-to-face interview |
|
| [58] | Ampang, Selangor | Residential community (133) | Convenience sampling and self-administered |
|
| [59] | Penang Island, Penang | Residential community (urban, suburban) (202) | Purposive sampling and self-administered |
|
| [60] | Malaysia | Malaysian public (2512) | Simple random sampling and phone call interview |
|
| [61] | Kuala Lumpur | Secondary school students (123) | Convenience sampling and self-administered |
|
| [62] | UPM Serdang, Selangor | University students (320) | Purposive sampling and self-administered |
|
| [63] | Kuala Pilah District, Negeri Sembilan | Residential community (141) | Purposive and simple random selection and face-to-face interview |
|
| [64] | West Malaysia | Indigenous people (505) | Stratified random sampling and face-to-face interview |
|
| [65] | Selangor | School children (204) | Convenience sampling and self-administered |
|
| [66] | NDUM, Kuala Lumpur | Military cadet (183) | Convenience sampling and self-administered |
|
| [67] | Hospital Serdang, Kajang and Kuala Lumpur, Kuala Lumpur & Selangor | Dengue patients (326) | Purposive sampling and face-to-face interview |
|
| [68] | Kuala Lumpur | Residential community (1400) | Simple random sampling and telephone-interview |
|
| [69] | Gombak, Selangor | Parents or caretakers (866) | Universal sampling and self-administered |
|
| [70] | Jempol, Negeri Sembilan | Residential community (306) | Cluster random sampling and self-administrated |
|
| [71] | Rembau & Bukit Pelanduk district, Negeri Sembilan | Residential community (400) | Simple random sampling and face-to-face interview |
|
| [72] | Selangor | Residential community (322) | Cluster random sampling and face-to-face interview |
|
| [73] | UKMC, Banggi, Selangor | Health care providers (61) | Simple random sampling and self-administered |
|
| [74] | Selangor & Kuala Lumpur | Residential community (300) | Convenience sampling and self-administered |
|
| [75] | Terengganu | Residential community (280) | Simple random sampling and face-to-face interview |
|
| [76] | Perak Tengah district, Perak | Residential community (200) | Convenience sampling and self-administered |
|
| [77] | Seremban District, Negeri Sembilan | Residential community (321) | Convenience sampling and face-to-face interview |
|
| [78] | Klang Valley, Selangor | Suspected dengue patients (236) | Purposive random sampling and face-to-face interview |
|
| [79] | Kuala Lumpur | Residential community (133) | Stratified and systematic random sampling and face-to-face interview |
|
| [80] | Kuala Kangsar Perak | Residential community (200) | Simple random sampling and face-to-face interview |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guad, R.M.; Wu, Y.S.; Aung, Y.N.; Sekaran, S.D.; Wilke, A.B.B.; Low, W.Y.; Sim, M.S.; Carandang, R.R.; Jeffree, M.S.; Taherdoost, H.; et al. Different Domains of Dengue Research in Malaysia: A Systematic Review and Meta-Analysis of Questionnaire-Based Studies. Int. J. Environ. Res. Public Health 2021, 18, 4474. https://doi.org/10.3390/ijerph18094474
Guad RM, Wu YS, Aung YN, Sekaran SD, Wilke ABB, Low WY, Sim MS, Carandang RR, Jeffree MS, Taherdoost H, et al. Different Domains of Dengue Research in Malaysia: A Systematic Review and Meta-Analysis of Questionnaire-Based Studies. International Journal of Environmental Research and Public Health. 2021; 18(9):4474. https://doi.org/10.3390/ijerph18094474
Chicago/Turabian StyleGuad, Rhanye Mac, Yuan Seng Wu, Yin Nwe Aung, Shamala Devi Sekaran, André Barretto Bruno Wilke, Wah Yun Low, Maw Shin Sim, Rogie Royce Carandang, Mohammad Saffree Jeffree, Hamed Taherdoost, and et al. 2021. "Different Domains of Dengue Research in Malaysia: A Systematic Review and Meta-Analysis of Questionnaire-Based Studies" International Journal of Environmental Research and Public Health 18, no. 9: 4474. https://doi.org/10.3390/ijerph18094474
APA StyleGuad, R. M., Wu, Y. S., Aung, Y. N., Sekaran, S. D., Wilke, A. B. B., Low, W. Y., Sim, M. S., Carandang, R. R., Jeffree, M. S., Taherdoost, H., Sunggip, C., Lin, C. L. S., Murugaiah, C., Subramaniyan, V., & Azizan, N. (2021). Different Domains of Dengue Research in Malaysia: A Systematic Review and Meta-Analysis of Questionnaire-Based Studies. International Journal of Environmental Research and Public Health, 18(9), 4474. https://doi.org/10.3390/ijerph18094474