
Heat Acclimation Following Heat Acclimatization Elicits Additional Physiological Improvements in Male Endurance Athletes

 , ,
, , 
Abstract
1. Introduction
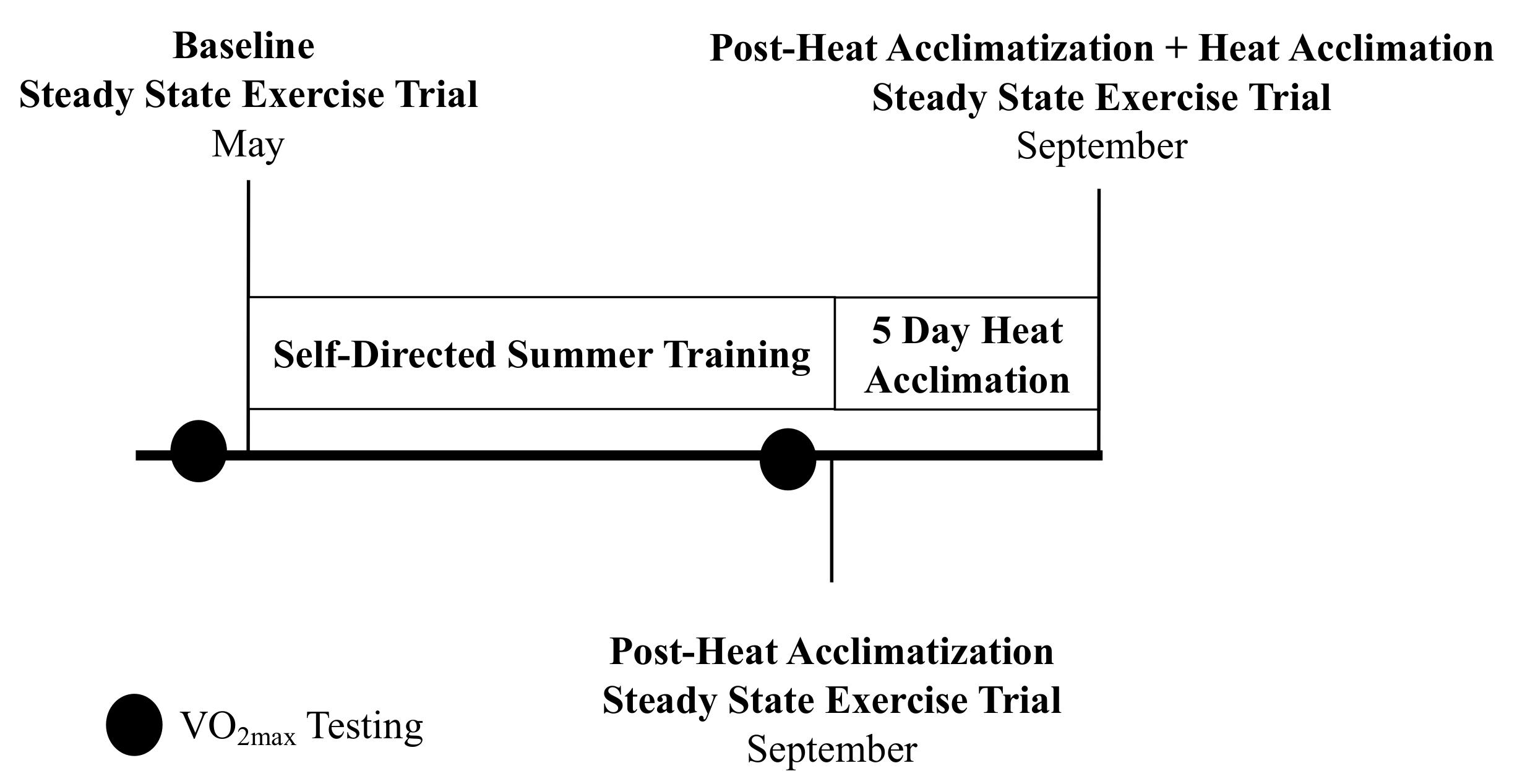
2. Materials and Methods
3. Results
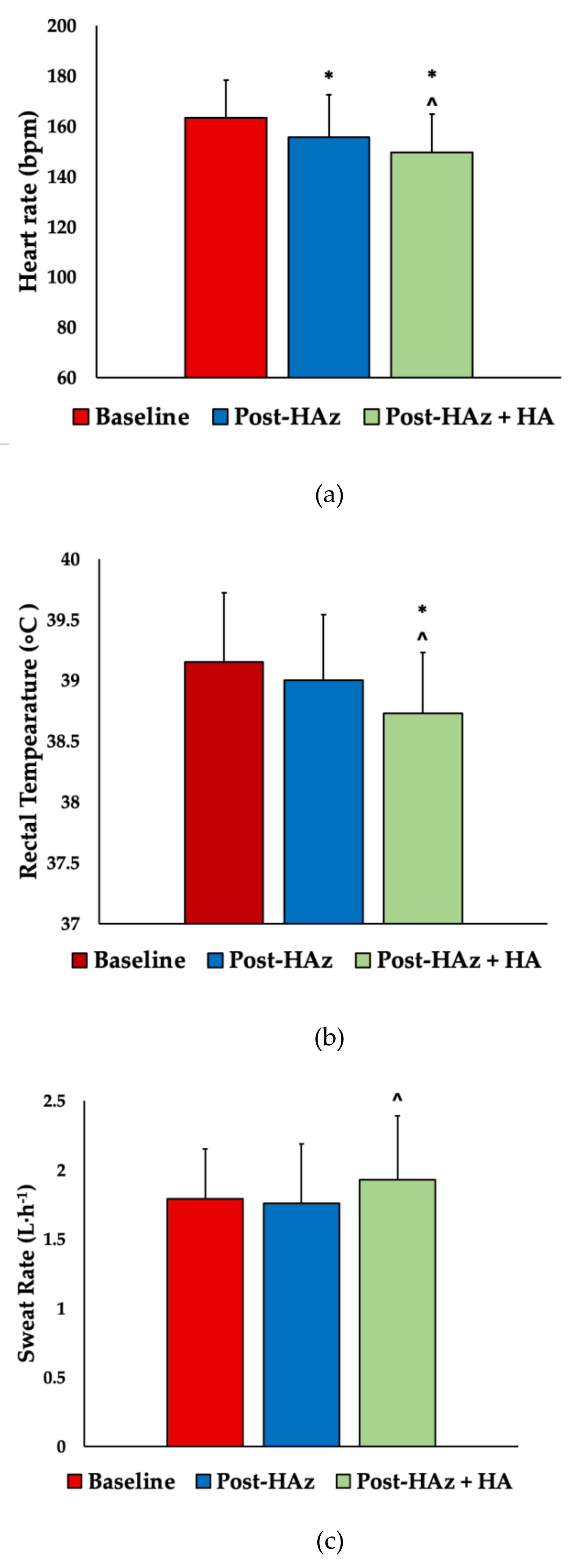
3.1. Heart Rate
3.2. Trec and Delta Trec
3.3. Skin Temperature and Sweat Rate
3.4. Sweat Electrolyte Concentration
3.5. Ratings of Perceived Exertion, Thermal Sensation, Thirst, and Fatigue
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Watanabe, N.; Wicker, P.; Yan, G. Weather conditions, travel distance, rest, and running performance: The 2014 FIFA World cup and implications for the future. J. Sport Manag. 2017, 31, 27–43. [Google Scholar] [CrossRef]
- Grundstein, A.; Williams, C.; Phan, M.; Cooper, E. Regional heat safety thresholds for athletics in the contiguous United States. Appl. Geogr. 2015, 56, 55–60. [Google Scholar] [CrossRef]
- Casadio, J.R.; Kilding, A.E.; Cotter, J.D.; Laursen, P.B. From lab to real world: Heat acclimation considerations for elite athletes. Sports Med. 2017, 47, 1467–1476. [Google Scholar] [CrossRef] [PubMed]
- Périard, J.D.; Racinais, S.; Sawka, M.N. Adaptations and mechanisms of human heat acclimation: Applications for competitive athletes and sports. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 1), 20–38. [Google Scholar] [CrossRef]
- Benjamin, C.L.; Sekiguchi, Y.; Fry, L.A.; Casa, D.J. Performance changes following heat acclimation and the factors that influence these changes: Meta-analysis and meta-regression. Front. Physiol. 2019, 10, 448. [Google Scholar] [CrossRef]
- Pandolf, K.B. Time course of heat acclimation and its decay. Int. J. Sports Med. 1998, 19 (Suppl. 2), S157–S160. [Google Scholar] [CrossRef]
- Tyler, C.J.; Reeve, T.; Hodges, G.J.; Cheung, S.S. The effects of heat adaptation on physiology, perception and exercise performance in the heat: A meta-analysis. Sports Med. 2016, 46, 1699–1724. [Google Scholar] [CrossRef]
- Keiser, S.; Flück, D.; Hüppin, F.; Stravs, A.; Hilty, M.P.; Lundby, C. Heat training increases exercise capacity in hot but not in temperate conditions: A mechanistic counter-balanced cross-over study. Am. J. Physiol. Heart Circ. Physiol. 2015, 309, H750–H761. [Google Scholar] [CrossRef]
- Taylor, N.A.S. Human heat adaptation. Compr. Physiol. 2014, 4, 325–365. [Google Scholar] [CrossRef]
- Pryor, J.L.; Johnson, E.C.; Roberts, W.O.; Pryor, R.R. Application of evidence-based recommendations for heat acclimation: Individual and team sport perspectives. Temperature 2019, 6, 37–49. [Google Scholar] [CrossRef]
- Racinais, S.; Moussay, S.; Nichols, D.; Travers, G.; Belfekih, T.; Schumacher, Y.O.; Periard, J.D. Core Temperature up to 41.5 °C during the UCI road cycling world championships in the heat. Br. J. Sports Med. 2018. [Google Scholar] [CrossRef]
- Daanen, H.A.M.; Jonkman, A.G.; Layden, J.D.; Linnane, D.M.; Weller, A.S. Optimising the acquisition and retention of heat acclimation. Int. J. Sports Med. 2011, 32, 822–828. [Google Scholar] [CrossRef]
- Ramanathan, N.L. New weighting system for mean surface temperature of the human body. J. Appl. Physiol. 1964, 19, 531–533. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Casa, D.J. Methods to evaluate electrolyte and water turnover of athletes. Athl. Train. Sports Health Care 2009, 1, 169–179. [Google Scholar] [CrossRef]
- Armstrong, L.E. Assessing hydration status: The elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef]
- Hongu, N.; Orr, B.; Roe, D.; Reed, R.; Going, S. Global positioning system watches for estimating energy expenditure. J. Strength Cond. Res. 2013, 27, 3216–3220. [Google Scholar] [CrossRef]
- Heat Stress Adviser. Available online: http://www.zunis.org/sports_p.htm (accessed on 5 March 2020).
- Liljegren, J.C.; Carhart, R.A.; Lawday, P.; Tschopp, S.; Sharp, R. Modeling the wet bulb globe temperature using standard meteorological measurements. J. Occup. Environ. Hyg. 2008, 5, 645–655. [Google Scholar] [CrossRef]
- Pryor, J.L.; Pryor, R.R.; Vandermark, L.W.; Adams, E.L.; VanScoy, R.M.; Casa, D.J.; Armstrong, L.E.; Lee, E.C.; DiStefano, L.J.; Anderson, J.M.; et al. Intermittent exercise-heat exposures and intense physical activity sustain heat acclimation adaptations. J. Sci. Med. Sport 2018, 22, 117–122. [Google Scholar] [CrossRef]
- Batterham, A.M.; Hopkins, W.G. Making meaningful inferences about magnitudes. Int. J. Sports Physiol. Perform. 2006, 1, 50–57. [Google Scholar] [CrossRef]
- Armstrong, L.E.; Hubbard, R.W.; DeLuca, J.P.; Christensen, E.L. Heat Acclimatization during summer running in the northeastern United States. Med. Sci. Sports Exerc. 1987, 19, 131–136. [Google Scholar] [CrossRef]
- Racinais, S.; Mohr, M.; Buchheit, M.; Voss, S.C.; Gaoua, N.; Grantham, J.; Nybo, L. Individual responses to short-term heat acclimatisation as predictors of football performance in a hot, dry environment. Br. J. Sports Med. 2012, 46, 810–815. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, S.; Esterman, A.; Eston, R.; Bowering, K.J.; Norton, K. Short-term heat acclimation training improves physical performance: A systematic review, and exploration of physiological adaptations and application for team sports. Sports Med. 2014, 44, 971–988. [Google Scholar] [CrossRef] [PubMed]
- Périard, J.D.; Travers, G.J.S.; Racinais, S.; Sawka, M.N. Cardiovascular adaptations supporting human exercise-heat acclimation. Auton. Neurosci. 2016, 196, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, Y.; McLellan, T.M.; Shephard, R.J. Interactions of physical training and heat acclimation. Sports Med. 1997, 23, 173–210. [Google Scholar] [CrossRef]
- Aoyagi, Y.; McLellan, T.M.; Shephard, R.J. Effects of endurance training and heat acclimation on psychological strain in exercising men wearing protective clothing. Ergonomics 1998, 41, 328–357. [Google Scholar] [CrossRef]
- Baker, L.B.; Barnes, K.A.; Anderson, M.L.; Passe, D.H.; Stofan, J.R. Normative data for regional sweat sodium concentration and whole-body sweating rate in athletes. J. Sports Sci. 2016, 34, 358–368. [Google Scholar] [CrossRef]
- Baker, L.B. Physiology of sweat gland function: The roles of sweating and sweat composition in human health. Temperature 2019, 6, 211–259. [Google Scholar] [CrossRef]
- Clark, B.; Costa, V.P.; O’Brien, B.J.; Guglielmo, L.G.; Paton, C.D. Effects of a seven day overload-period of high-intensity training on performance and physiology of competitive cyclists. PLoS ONE 2014, 9, e115308. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Exercise Type (# of Sessions) | Distance (km) | Heart Rate (bpm) | Duration (min) | Heat Index (°C) | WBGT (°C) | Time of Day (hh:mm) |
|---|---|---|---|---|---|---|
| Outdoor Running (n = 1692) | 10.28 ± 8.43 | 140 ± 15 | 56.38 ± 72.66 | 29.89 ± 2.42 | 22.31 ± 4.23 | 12:14 ± 4:42 |
| Outdoor Cycling (n = 364) | 32.74 ± 26.21 | 128 ± 16 | 91.67 ± 69.27 | 30.17 ± 2.41 | 23.68 ± 3.96 | 13:12 ± 3:52 |
| Multi-Sport (n = 18) | 27.88 ± 15.43 | 125 ± 6 | 90.71 ± 31.78 | 31.32 ± 1.51 | 22.03 ± 6.20 | 11:11 ± 4:33 |
| Hiking (n = 19) | 8.50 ± 8.95 | 94 ± 18 | 161.58 ± 170.58 | 30.77 ± 4.61 | 19.39 ± 6.84 | 11:50 ± 3:30 |
| - | HA#1 | HA#2 | HA#3 | HA#4 | HA#5 | Overall |
|---|---|---|---|---|---|---|
| Total Session | ||||||
| Duration (min) | 82 ± 6 | 81 ± 6 | 85 ± 6 | 83 ± 8 | 83 ± 8 | 83 ± 5 |
| Average HR (bpm) | 137 ± 13 | 132 ± 14 | 132 ± 11 | 130 ± 12 | 129 ± 12 | 132 ± 11 |
| Average Trec (°C) | 38.85 ± 0.42 | 38.93 ± 0.31 | 38.81 ± 0.38 | 38.80 ± 0.30 | 38.78 ± 0.31 | 38.83 ± 0.25 |
| Max HR (bpm) | 165 ± 13 | 164 ± 11 | 164 ± 13 | 162 ± 14 | 161 ± 15 | 163 ± 11 |
| Max Trec (°C) | 39.63 ± 0.34 | 39.65 ± 0.28 | 39.46 ± 0.30 | 39.50 ± 0.28 | 39.48 ± 0.29 | 39.55 ± 0.15 |
| AUC (°C·h−1) | 52 ± 4 | 51 ± 4 | 51 ± 3 | 52 ± 4 | 52 ± 5 | 52 ± 4 |
| Perceived Exertion | 10 ± 2 | 10 ± 2 | 10 ± 2 | 10 ± 2 | 10 ± 2 | 10 ± 2 |
| Thermal Sensation | 6.0 ± 1.0 | 6.0 ± 1.0 | 6.0 ± 1.0 | 6.0 ± 1.0 | 6.0 ± 0.5 | 6.0 ± 1.0 |
| Fatigue | 4 ± 2 | 3 ± 2 | 4 ± 2 | 3 ± 2 | 3 ± 2 | 3 ± 2 |
| Sweat Volume (L) | 2.40 ± 0.63 | 2.47 ± 0.59 | 2.72 ± 0.60 | 2.74 ± 0.56 | 2.77 ± 0.81 | 2.62 ± 0.52 |
| Session after 38.5 °C * | ||||||
| Average Trec (°C) | 39.16 ± 0.42 | 39.24 ± 0.22 | 39.16 ± 0.36 | 39.16 ± 0.30 | 39.11 ± 0.22 | 39.17 ± 0.17 |
| Average HR (bpm) | 138 ± 14 | 132 ± 14 | 131 ± 14 | 131 ± 14 | 128 ± 12 | 132 ± 12 |
| AUC (°C·h−1) | 46 ± 16 | 46 ± 12 | 42 ± 16 | 42 ± 15 | 38 ± 10 | 43 ± 13 |
| Physiological Outcome | Baseline vs. Post-HAz | Post-HAz vs. Post-HAz+HA | Baseline vs. Post-HAz+HA | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MD ± SE | ES | p-Value | MD ± SE | ES | p-Value | MD ± SE | ES | p-Value | |
| Average Heart Rate (bpm) | −5 ± 1 | 0.36 | 0.002 * | −4 ± 3 | 0.29 | 0.013 * | −8 ± 2 | 0.71 | <0.001 * |
| Max Heart Rate (bpm) | −8 ± 2 | 0.47 | 0.002 * | −6 ± 2 | 0.36 | 0.06 * | −14 ± 2 | 0.90 | <0.001 * |
| Average Trec (°C) | −0.04 ± 0.01 | 0.08 | 0.479 | −0.22 ± 0.08 | 0.54 | 0.009 * | −0.26 ± 0.08 | 0.68 | 0.005 * |
| Max Trec (°C) | −0.15 ± 0.07 | 0.27 | 0.059 | −0.27 ± 0.10 | 0.52 | 0.009 * | −0.42 ± 0.11 | 0.78 | 0.001 * |
| Minimum Trec (°C) | 0.04 ± 0.06 | 0.08 | 0.577 | −0.22 ± 0.10 | 0.59 | 0.016 * | −0.18 ± 0.10 | 0.49 | 0.067 |
| Delta Trec (°C) | −0.18 ± 0.08 | 0.34 | 0.025 * | −0.05 ± 0.05 | 0.11 | 0.337 | −0.23 ± 0.09 | 0.42 | 0.020 * |
| Average TSK (°C) | −0.45 ± 0.11 | 0.87 | 0.001 * | −0.37 ± 0.11 | 0.63 | 0.005 * | −0.81 ± 0.12 | 1.48 | <0.001 * |
| Sweat Rate (L·h−1) | −0.03 ± 0.05 | 0.08 | 0.533 | 0.16 ± 0.07 | 0.36 | 0.027 * | 0.13 ± 0.07 | 0.31 | 0.061 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benjamin, C.L.; Sekiguchi, Y.; Struder, J.F.; Szymanski, M.R.; Manning, C.N.; Grundstein, A.J.; Lee, E.C.; Huggins, R.A.; Armstrong, L.E.; Casa, D.J. Heat Acclimation Following Heat Acclimatization Elicits Additional Physiological Improvements in Male Endurance Athletes. Int. J. Environ. Res. Public Health 2021, 18, 4366. https://doi.org/10.3390/ijerph18084366
Benjamin CL, Sekiguchi Y, Struder JF, Szymanski MR, Manning CN, Grundstein AJ, Lee EC, Huggins RA, Armstrong LE, Casa DJ. Heat Acclimation Following Heat Acclimatization Elicits Additional Physiological Improvements in Male Endurance Athletes. International Journal of Environmental Research and Public Health. 2021; 18(8):4366. https://doi.org/10.3390/ijerph18084366
Chicago/Turabian StyleBenjamin, Courteney L., Yasuki Sekiguchi, Jeb F. Struder, Michael R. Szymanski, Ciara N. Manning, Andrew J. Grundstein, Elaine C. Lee, Robert A. Huggins, Lawrence E. Armstrong, and Douglas J. Casa. 2021. "Heat Acclimation Following Heat Acclimatization Elicits Additional Physiological Improvements in Male Endurance Athletes" International Journal of Environmental Research and Public Health 18, no. 8: 4366. https://doi.org/10.3390/ijerph18084366
APA StyleBenjamin, C. L., Sekiguchi, Y., Struder, J. F., Szymanski, M. R., Manning, C. N., Grundstein, A. J., Lee, E. C., Huggins, R. A., Armstrong, L. E., & Casa, D. J. (2021). Heat Acclimation Following Heat Acclimatization Elicits Additional Physiological Improvements in Male Endurance Athletes. International Journal of Environmental Research and Public Health, 18(8), 4366. https://doi.org/10.3390/ijerph18084366