
Vibration Exposure and Transmissibility on Dentist’s Anatomy: A Study of Micro Motors and Air-Turbines

 , ,
, ,  , ,
, ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Hand Held Tool
2.2. Handheld Dentistry Tools under Present Experimentation
2.3. Experimental Approach
2.4. Hand Piece Examination Research Methodology
2.5. Purpose of the Study
- To study the vibration amplitudes during Idling of micro motor and air-turbine hand pieces.
- To explore different grasp forces while drilling with irrigant injection by the dentists using different hand pieces.
- To study various vibration transmission of these hand pieces.
2.6. Null Hypotheses of the Study
3. Result Analysis and Discussion
3.1. Vibration Amplitudes during Idling
3.2. Drilling with Different Grip Force: Micro Motor and Air-Turbine
3.3. Vibration Transmissibility: Micro Motor and Air-Turbine
3.4. Discussion of the Results Extracted
- Result no. 1: The variance in average vibration amplitudes of twelve hand pieces did not show equality in independent observations of 1/3rd octave band vibration amplitudes with F (11, 252) = 54.017, p = 0.000, and α = 0.05. Later, the Welch ANOVA output showed a significant difference in means, and variance between the means are not equal with F (11, 98.842) =5.938, p = 0.000 and α = 0.05. A post-hoc comparison Games–Howell test showed that two used hand pieces coded as MUD and AUA show a difference in the average vibration amplitudes.Possible causes of disagreement: The reason for the difference in micro motor used hand piece (MUD) and used air-turbine hand piece (AUA) is the overuse of both hand pieces. The MUD was used for more than two and a half years. The AUA was used for more than three years, impacting the dental professionals’ overall professional idling efficiencies. This is why the idling efficiency of both used hand pieces were different from the other hand pieces under study.
- Result no. 2: The study found all grasping conditions of micro motor and air-turbine at 1/3–octave band vibration amplitude at 22 different frequencies testing homogeneity of variances in two hand pieces, p-value < 0.05 depicting equal variances were not assumed. The study has also shown that output is statistically significant in all grasping conditions with the help of an independent t-test on air-turbine and micro-motors. Hence, both devices differ from each other on the pretext of comparison of corresponding grasping style.The Levene test showed that computed variances for 1/3rd–octave band vibrations amplitudes for various hand pieces various grasping conditions are not equal with F (7, 168) = 20.922, p = 0.000, and α = 0.05. The Welch ANOVA output showed that there is a significant difference in means, and variances between the means are not equal with F (7, 70.486) = 10.788, p = 0.000, and α = 0.05. A post-hoc comparison Games–Howell test showed that the tight grasping style in the case of micro motor devices differs from the rest of the styles.Possible causes of disagreement: These electrically driven micro motors are edging over the air-turbine while grasping and drilling in dental operations. Electric micro motors, when held tightly, give a hand piece strength of 0.18 million rpm. Hence, it is reasonable that this particular grasping style will differ from others.
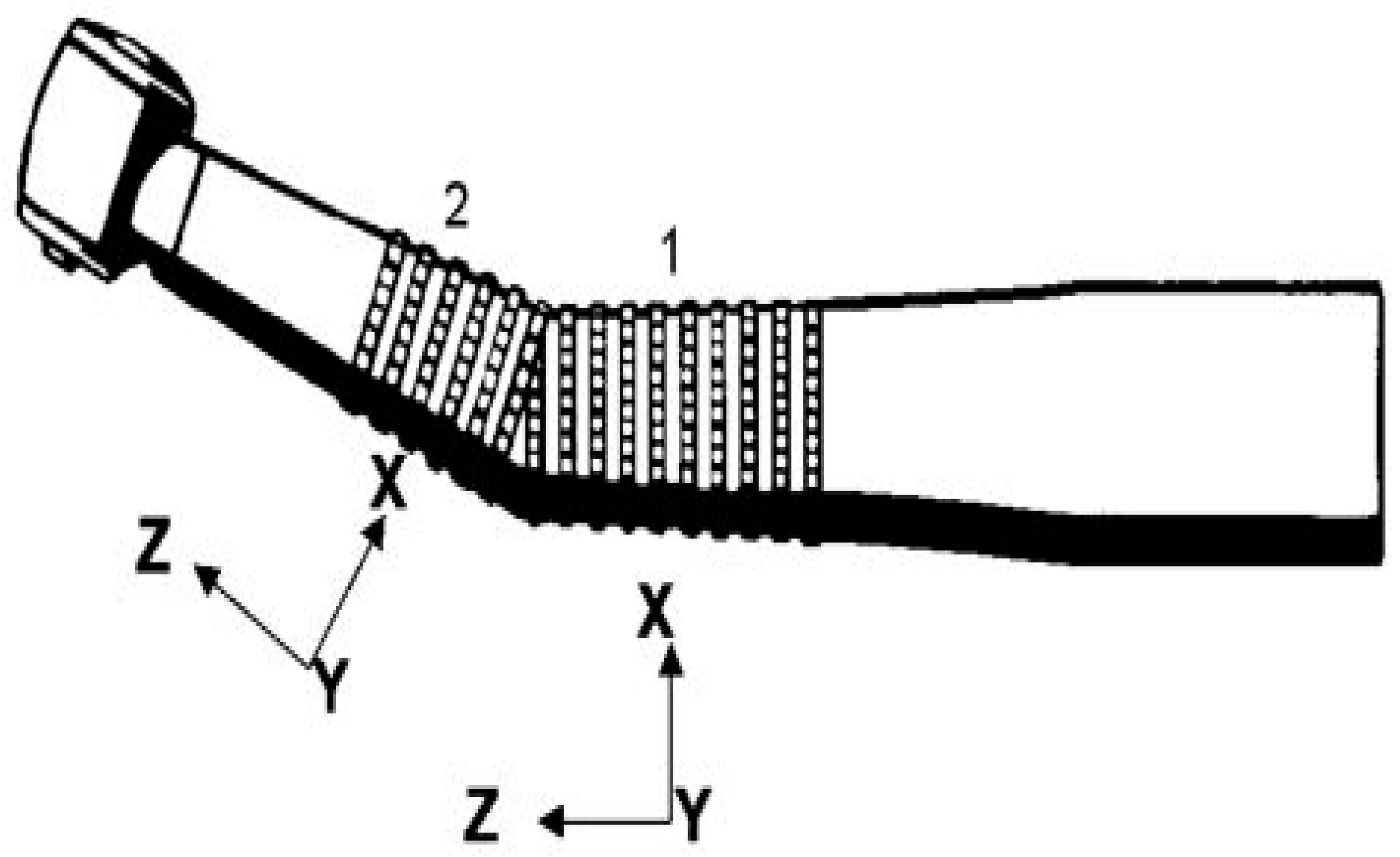
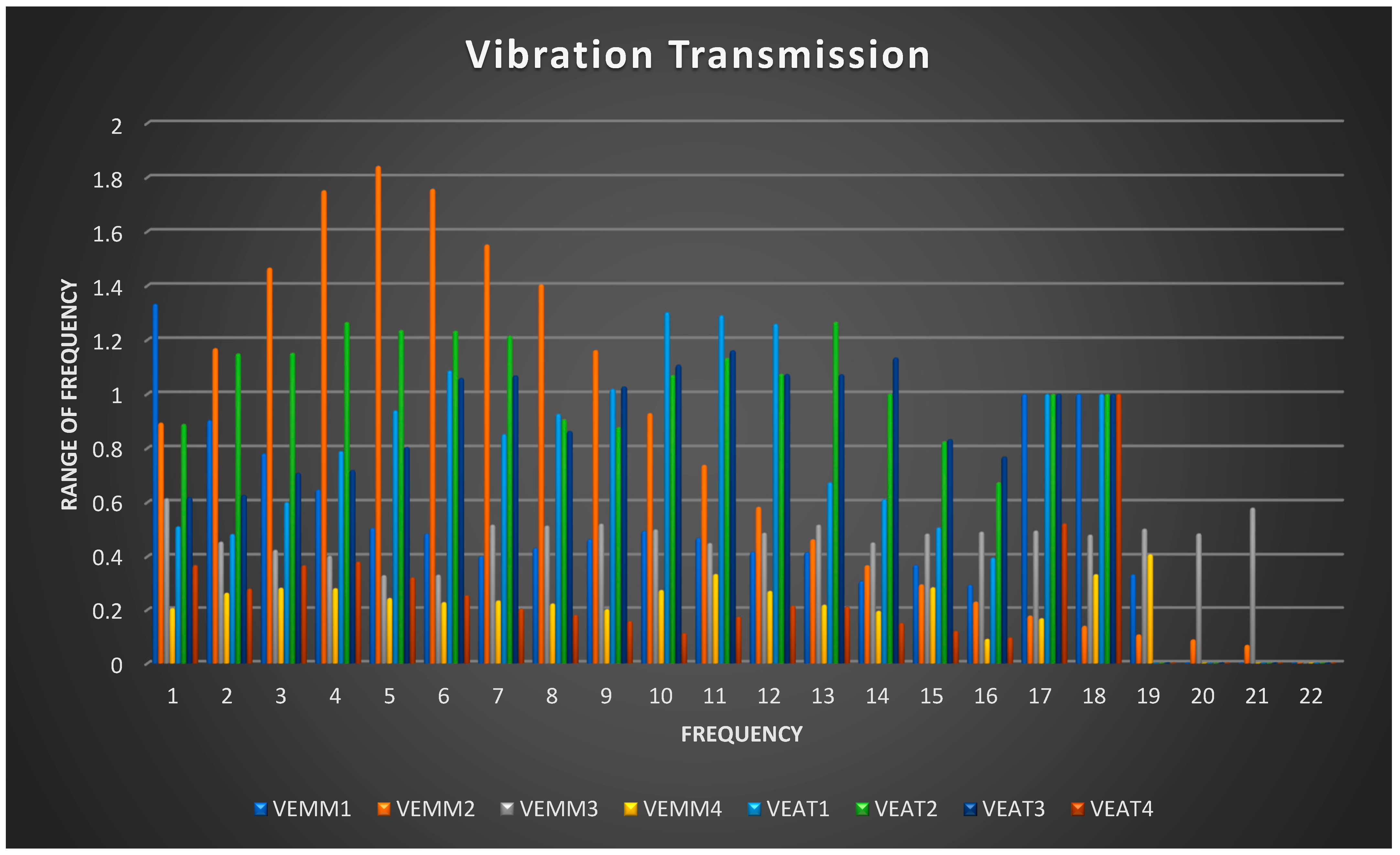
- Result no. 3: This is the main crux of the present investigation. The vibration transmissibility was evaluated on four different micro motors and 4 air-turbine hand pieces with 22 different frequencies. A study of eight hand pieces measuring 1/3rd–octave band vibrations transmissions during drilling with irrigant injection at position two for varying transmission points by the dentist showed a resonance frequency range less than unity. This indicates that most of the vibrations were absorbed through the dental workers’ fingers, palms, and hands. The lower the transmissibility range, the higher is the absorption by the body limbs of dental workers.The Levene test showed that computed variances for 1/3rd–octave band vibrations amplitudes for various grasping conditions of both hand pieces are not equal with F (7, 168) = 12.673, p = 0.000, and α = 0.05. The Welch ANOVA output showed that there is a significant difference in means, and variances between the means are not equal. F (7, 69.933) = 18.531, p = 0.000 and α = 0.05. A post-hoc comparison Games–Howell test showed that vibration transmissibility of used micro motor hand piece (VEMM4) differs from others.Possible causes of disagreement: The reason for the difference is the obsolete and old hand piece. This micro motor was observed to be old, overused, and noisy during experimentation. The vibrancy of offhand tools must remain declared according to after EC Machinery Directive. The lesson handbook concerning the desktop should contain the weighted RMS acceleration worth according to who the missile is subjected to if it exceeds 2.5 m/s2. If the acceleration price does not outdo 2.5 m/s2, it must be mentioned.As aforesaid, there are many alternative treatments, technologies, and instruments that can provide quick relief, less pain, and less discomfort for dentists and their patients. These include techniques like laser technology, digital impressions, and intraoral scanners. Drafting direct images with titanium dioxide powder-free intraoral scanning, gypsum models etc., are very usable alternatives in this area [41].
4. Conclusions
5. Policy Implications, Suggestions and Future Scope of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, V.; Kalra, P. A Study to Analyse the Vibration Transmissibility on Dental Hand pieces. i-Manag. J. Mech. Eng. 2017, 7, 24. [Google Scholar]
- Reitemeier, B.K.S. Exposure to vibration of parts of the body during dental work. Zent. Arb. Arb. Erg. 1993, 43, 187–193. [Google Scholar]
- Kinne, J.; Schenk, T.; Knoll, P. Automatic test stand for the measurement of the vibration emission of hand held machines. In Proceedings of the 8th International Conference on Hand-Arm Vibration, Umeå, Sweden, 9–12 June 1998; pp. 9–12. [Google Scholar]
- Wu, J.Z.; Dong, R.G.; Rakheja, S.; Schopper, A.W. Simulation of mechanical responses of fingertip to dynamic loading. Med. Eng. Phys. 2002, 24, 253–264. [Google Scholar] [CrossRef]
- Tarabini, M.; Mauri, N.; Gaudio, I.; Cinquemani, S.; Moorhead, A.; Bongiovanni, R.; Feletti, F. Hand-arm vibration in motocross: Measurement and mitigation actions. Muscles Ligaments Tendons J. 2020, 10, 280–289. [Google Scholar] [CrossRef]
- International Organization for Standardization. 5349-1: Mechanical Vibration—Measurement and Evaluation of Human Exposure to Hand-Transmitted Vibration—Part 1: General Requirements; International Organization for Standardization: Geneva, Switzerland, 2001; Volume 1, pp. 1–24. [Google Scholar]
- Rytkönen, E.; Sorainen, E.; Leino-Arjas, P.; Solovieva, S. Hand-arm vibration exposure of dentists. Int. Arch. Occup. Environ. Health 2006, 79, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Sorensson, A.; Burstrom, L. Energy Absorption in the Hand and Arm System Exposed to Impact Vibration with High Frequency Contents. Int. J. Acoust. Vib. 2000, 32, 35–36. [Google Scholar] [CrossRef]
- Gerhardsson, L.; Ahlstrand, C.; Ersson, P.; Gustafsson, E. Vibration-induced injuries in workers exposed to transient and high frequency vibrations. J. Occup. Med. Toxicol. 2020, 15, 18. [Google Scholar] [CrossRef]
- Bylund, S.H.; Burström, L. Power absorption in women and men exposed to hand–arm vibration. Int. Arch. Occup. Environ. Health 2003, 76, 313–317. [Google Scholar] [CrossRef]
- Jodalli, P.S.; Kurana, S.; Shameema, M.R.; Khed, J.; Prabhu, V. Posturedontics: How does dentistry fit you? J. Pharm. Bioallied Sci. 2015, 7, S393–S397. [Google Scholar] [CrossRef]
- Griffin, M.J.; Bovenzi, M.; Nelson, C.M. Dose-response patterns for vibration-induced white finger. Occup. Environ. Med. 2003, 60, 16–26. [Google Scholar] [CrossRef]
- Gupta, A.; Bhat, M.; Mohammed, T.; Bansal, N.; Gupta, G. Ergonomics in dentistry. Int. J. Clin. Pediatric Dent. 2014, 7, 30–34. [Google Scholar] [CrossRef]
- Singh, S.; Arora, R. Ergonomic Intervention for Preventing Musculoskeletal Disorders among Farm Women. J. Agric. Sci. 2010, 1. [Google Scholar] [CrossRef]
- Farges, J.-C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental pulp defence and repair mechanisms in dental caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef]
- Mm, J.; Nk, B.; Pathak, A. Minimal intervention dentistry—A new frontier in clinical dentistry. J. Clin. Diagn. Res. 2014, 8, ZE04–ZE08. [Google Scholar] [CrossRef] [PubMed]
- Nadanovsky, P.; Cohen-Carneiro, F.; Mello, F. Removal of Caries Using only Hand Instruments: A Comparison of Mechanical and Chemo-Mechanical Methods. Caries Res. 2001, 35, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Bhandary, N.; Desai, A.; Shetty, Y.B. High speed hand pieces. J. Int. Oral Health 2014, 6, 130–132. [Google Scholar]
- Lawson, I.; McGeoch, K. A medical assessment process for a large volume of medico-legal compensation claims for hand–arm vibration syndrome. Occup. Med. 2003, 53, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Sauni, R.; Toivio, P.; Pääkkönen, R.; Malmström, J.; Uitti, J. Work disability after diagnosis of hand-arm vibration syndrome. Int. Arch. Occup. Environ. Health 2015, 88, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Poole, C.J.M.; Bovenzi, M.; Nilsson, T.; Lawson, I.J.; House, R.; Thompson, A.; Youakim, S. International consensus criteria for diagnosing and staging hand–arm vibration syndrome. Int. Arch. Occup. Environ. Health 2019, 92, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Aarhus, L.; Veiersted, K.B.; Nordby, K.-C.; Bast-Pettersen, R. Neurosensory component of hand–arm vibration syndrome: A 22-year follow-up study. Occup. Med. 2019, 69, 215–218. [Google Scholar] [CrossRef]
- Vihlborg, P.; Bryngelsson, I.-L.; Lindgren, B.; Gunnarsson, L.G.; Graff, P. Association between vibration exposure and hand-arm vibration symptoms in a Swedish mechanical industry. Int. J. Ind. Erg. 2017, 62, 77–81. [Google Scholar] [CrossRef]
- Jaffar, N.; Abdul-Tharim, A.H.; Mohd-Kamar, I.F.; Lop, N.S. A Literature Review of Ergonomics Risk Factors in Construction Industry. Procedia Eng. 2011, 20, 89–97. [Google Scholar] [CrossRef]
- Ohlendorf, D.; Erbe, C.; Nowak, J.; Hauck, I.; Hermanns, I.; Ditchen, D.; Ellegast, R.; Groneberg, D.A. Constrained posture in dentistry—A kinematic analysis of dentists. BMC Musculoskelet. Disord. 2017, 18, 291. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.D.; Aggarwal, S.; Gupta, B.; Gupta, M.; Gupta, N. Effect of Deep Cervical Flexor Training vs. Conventional Isometric Training on Forward Head Posture, Pain, Neck Disability Index In Dentists Suffering from Chronic Neck Pain. J. Clin. Diagn. Res. 2013, 7, 2261–2264. [Google Scholar] [CrossRef]
- Mizrahi, J. Neuro-mechanical aspects of playing-related mobility disorders in orchestra violinists and upper strings players: A review. Eur. J. Transl. Myol. 2020, 30, 9095. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, T.H.; Yenealem, D.G.; Geberu, D.M. Physical environmental and occupational factors inducing work-related neck and shoulder pains among self-employed tailors of informal sectors in Ethiopia, 2019: Results from a community based cross-sectional study. BMC Public Health 2020, 20, 1265. [Google Scholar] [CrossRef] [PubMed]
- Mulimani, P.; Hoe, V.C.W.; Hayes, M.J.; Idiculla, J.J.; Abas, A.B.L.; Karanth, L. Ergonomic interventions for preventing musculoskeletal disorders in dental care practitioners. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef] [PubMed]
- Shivpaul, R.A. The Effects of a Visco-Elastic Polymer Glove on Hand-Arm Vibration, Muscle Activity, and Comfort during Simulated Power Tool Use; University of Ontario Institute of Technology: Oshawa, ON, Canada, 2017. [Google Scholar]
- Singh, A.K.; Meena, M.L.; Chaudhary, H.; Karmakar, S. Assessment of transmissibility of hand-arm vibration, noise exposure, and shift in hearing threshold among handicraft operatives’: A cross-sectional study. J. Ind. Prod. Eng. 2020, 37, 134–147. [Google Scholar] [CrossRef]
- Griffin, M. Handbook of Human Vibration; Academic Press: London, UK, 1996; Volume 1. [Google Scholar]
- Wojtkowska, A.; Zapolski, T.; Wysokińska-Miszczuk, J.; Wysokiński, A.P. The inflammation link between periodontal disease and coronary atherosclerosis in patients with acute coronary syndromes: Case–control study. BMC Oral Health 2021, 21, 1–17. [Google Scholar] [CrossRef]
- Zhang, J.T.; Zhou, B.; Guo, J.; Zhu, T. Two-sample Behrens–Fisher problems for high-dimensional data: A normal reference approach. J. Stat. Plann. Inference 2021, 213, 142–161. [Google Scholar] [CrossRef]
- Flick, T.R.; Wang, C.X.; Patel, A.H.; Hodo, T.W.; Sherman, W.F.; Sanchez, F.L. Arthrofibrosis after total knee arthroplasty: Patients with keloids at risk. J. Orthop. Traumatol. 2021, 22, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, N.; Kern, M.; Taylor, T.; Wille, S.; Passia, N. Retention and wear of resin matrix attachments for implant overdentures. J. Mech. Behav. Biomed. Mater. 2020, 110. [Google Scholar] [CrossRef] [PubMed]
- Busch, T. Generic third-octave band vibration spectra for construction equipment. Can Acoust 2019, 47, 42–43. [Google Scholar]
- Beerse, M.; Lelko, M.; Wu, J. Acute effect of whole-body vibration on acceleration transmission and jumping performance in children. Clin. Biomech. 2021, 81. [Google Scholar] [CrossRef]
- Chuang, L.R.; Yang, W.W.; Chang, P.L.; Chen, V.C.F.; Liu, C.; Shiang, T.Y. Managing vibration training safety by using knee flexion angle and rating perceived exertion. Sensors 2021, 21, 1158. [Google Scholar] [CrossRef]
- Shimoda, T.; Kokuyama, W.; Nozato, H. A low-acceleration measurement using anti-vibration table with low-frequency resonance. Acta Imeko 2021, 9, 369–373. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Gandini, P.; Malfatto, M.; Di Corato, F.; Trovati, F.; Scribante, A. Computerized Casts for Orthodontic Purpose Using Powder-Free Intraoral Scanners: Accuracy, Execution Time, and Patient Feedback. Biomed Res. Int. 2018, 2018, 4103232. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, Y.; Beyth, N.; Ram, D.; Mijiritsky, E.; Davidovich, E. Laser Tooth Preparation for Pit and Fissure Sealing. Int. J. Environ. Res. Public Health 2020, 17, 7813. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Type | Rotational Speed (rpm) | Restricted Rotational Speed (rpm) | |
|---|---|---|---|---|
| 1 | M * | New micro-motor Hand pieces | 25,000–40,000 | 35,000 |
| 2 | M | |||
| 3 | A * | New air-turbine Hand pieces | 35,000–400,000 | |
| 4 | A | |||
| 5 | M | Used micro-motor Hand pieces | 25,000–40,000 | |
| 6 | M | |||
| 7 | M | |||
| 8 | M | |||
| 9 | M | |||
| 10 | M | |||
| 11 | M | |||
| 12 | M | |||
| 13 | A | Used air-turbine Hand pieces | 35,000–400,000 | |
| 14 | A | |||
| 15 | A | |||
| 16 | A | |||
| 17 | A | |||
| 18 | A | |||
| 19 | A | |||
| 20 | A | |||
| Hand Piece | MM | AT | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Usage of Hand Piece | New | Used | New | Used | |||||||||
| Number of hand piece | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| Code assigned for hand piece | MNA | MNB | MUA | MUB | MUC | MUD | ANA | ANB | AUA | AUB | AUC | AUD | |
| Mean 1/3rd–octave band vibrations amplitudes | 0.080 | 0.059 | 0.046 | 0.024 | 0.030 | 0.686 | 0.043 | 0.024 | 0.358 | 0.058 | 0.032 | 0.044 | |
| Std. Deviation in 1/3rd–octave band vibrations amplitudes | 0.070 | 0.060 | 0.041 | 0.034 | 0.033 | 0.614 | 0.053 | 0.033 | 0.327 | 0.071 | 0.043 | 0.030 | |
| Std. Error in 1/3rd–octave band vibrations amplitudes | 0.015 | 0.013 | 0.009 | 0.007 | 0.007 | 0.131 | 0.011 | 0.007 | 0.070 | 0.015 | 0.009 | 0.006 | |
| 95% Confidence Interval for Mean | Lower Bound | 0.049 | 0.033 | 0.028 | 0.009 | 0.015 | 0.414 | 0.019 | 0.009 | 0.214 | 0.026 | 0.013 | 0.030 |
| Upper Bound | 0.112 | 0.086 | 0.065 | 0.039 | 0.044 | 0.958 | 0.066 | 0.038 | 0.503 | 0.090 | 0.051 | 0.057 | |
| Minimum vibrations amplitudes | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| Maximum1/3rd–octave band vibrations amplitudes | 0.202 | 0.185 | 0.120 | 0.103 | 0.119 | 10.71 | 0.150 | 0.091 | 0.927 | 0.209 | 0.127 | 0.090 | |
| Hand Piece | MM | AT | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Usage | New | Used | New | Used | ||||||||||
| Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | ||
| Hand piece description | Code | MNA | MNB | MUA | MUB | MUC | MUD | ANA | ANB | AUA | AUB | AUC | AUD | |
| MUD Post hoc Differences | Mean Difference (I–J) | 0.606 | 0.627 | 0.640 | 0.662 | 0.657 | - | 0.643 | 0.663 | 0.328 | 0.628 | 0.655 | 0.642 | |
| Std. Error | 0.132 | 0.131 | 0.131 | 0.131 | 0.131 | - | 0.131 | 0.131 | 0.148 | 0.132 | 0.131 | 0.131 | ||
| Sig. | 0.006 | 0.004 | 0.003 | 0.002 | 0.003 | - | 0.003 | 0.002 | 0.553 | 0.004 | 0.003 | 0.003 | ||
| 95% Confidence Interval | Lower Bound | 0.126 | 0.147 | 0.161 | 0.183 | 0.178 | - | 0.164 | 0.184 | −0.194 | 0.148 | 0.176 | 0.164 | |
| Upper Bound | 1.086 | 1.106 | 1.119 | 1.140 | 1.135 | - | 1.123 | 1.141 | 0.849 | 1.108 | 1.133 | 1.121 | ||
| AUA Post hoc Differences | Mean Difference (I–J) | 0.278 | 0.299 | 0.312 | 0.334 | 0.329 | −0.328 | 0.315 | 0.334 | - | 0.301 | 0.327 | 0.315 | |
| Std. Error | 0.071 | 0.071 | 0.070 | 0.070 | 0.070 | 0.148 | 0.071 | 0.070 | - | 0.071 | 0.070 | 0.070 | ||
| Sig. | 0.027 | 0.014 | 0.009 | 0.004 | 0.005 | 0.553 | 0.008 | 0.004 | - | 0.013 | 0.005 | 0.008 | ||
| 95% Confidence Interval | Lower Bound | 0.020 | 0.042 | 0.056 | 0.079 | 0.073 | −0.849 | 0.059 | 0.079 | - | 0.042 | 0.071 | 0.059 | |
| Upper Bound | 0.536 | 0.556 | 0.568 | 0.589 | 0.584 | 0.194 | 0.572 | 0.590 | - | 0.559 | 0.583 | 0.570 | ||
| S.No. | Frequency (Hz) | Mild Grasp | Gentle Grasp | Moderate Grasp | Tight Grasp | ||||
|---|---|---|---|---|---|---|---|---|---|
| MM | AT | MM | AT | MM | AT | MM | AT | ||
| 1 | 4 | 0.061102 | 0.02232 | 0.045358 | 0.022622 | 0.048273 | 0.022605 | 0.055188 | 0.022679 |
| 2 | 5 | 0.077492 | 0.014792 | 0.059547 | 0.014795 | 0.058292 | 0.013569 | 0.067697 | 0.02106 |
| 3 | 6.3 | 0.085361 | 0.020077 | 0.075257 | 0.015571 | 0.082418 | 0.016272 | 0.083462 | 0.033346 |
| 4 | 8 | 0.090946 | 0.02337 | 0.096737 | 0.018692 | 0.108857 | 0.018911 | 0.108265 | 0.039356 |
| 5 | 10 | 0.096186 | 0.017983 | 0.104106 | 0.019338 | 0.11251 | 0.019501 | 0.12911 | 0.042234 |
| 6 | 12.5 | 0.095075 | 0.014772 | 0.09945 | 0.018372 | 0.105408 | 0.017963 | 0.121874 | 0.035213 |
| 7 | 16 | 0.064613 | 0.011493 | 0.104221 | 0.012878 | 0.104044 | 0.014565 | 0.108744 | 0.021135 |
| 8 | 20 | 0.065636 | 0.004925 | 0.085852 | 0.007521 | 0.084231 | 0.009747 | 0.090106 | 0.017771 |
| 9 | 25 | 0.050784 | 0.003534 | 0.085755 | 0.004155 | 0.074222 | 0.005725 | 0.077805 | 0.013261 |
| 10 | 31.5 | 0.039617 | 0.003068 | 0.069618 | 0.002796 | 0.055338 | 0.003437 | 0.060045 | 0.00878 |
| 11 | 40 | 0.032447 | 0.002309 | 0.044357 | 0.002328 | 0.046594 | 0.002319 | 0.047724 | 0.004875 |
| 12 | 50 | 0.031231 | 0.002249 | 0.045057 | 0.002304 | 0.038382 | 0.002291 | 0.051721 | 0.003068 |
| 13 | 63 | 0.021891 | 0.001158 | 0.035641 | 0.001158 | 0.029066 | 0.001221 | 0.040975 | 0.001459 |
| 14 | 80 | 0.015031 | 0.000927 | 0.020398 | 0.000985 | 0.019231 | 0.000927 | 0.022152 | 0.0011 |
| 15 | 100 | 0.017962 | 0.000812 | 0.022426 | 0.000755 | 0.025223 | 0.000812 | 0.023977 | 0.000812 |
| 16 | 125 | 0.009328 | 0.000693 | 0.011679 | 0.000693 | 0.011516 | 0.000693 | 0.012676 | 0.000693 |
| 17 | 160 | 0.000245 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.0003 | 0.000173 |
| 18 | 200 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 |
| 19 | 250 | 0.001625 | 0 | 0.001797 | 0 | 0.001517 | 0 | 0.001625 | 0 |
| 20 | 315 | 0.000173 | 0 | 0.000173 | 0 | 0.000173 | 0 | 0.000173 | 0 |
| 21 | 400 | 0.000173 | 0.0001 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 | 0.000173 |
| 22 | 500 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Grasping Conditions | Type of Grip Force | N | Mean Vibration Amplitude | Std. Deviation Vibration Amplitude | Std. Error Mean of Vibration Amplitude | |
|---|---|---|---|---|---|---|
| Type of Hand Piece | Code Assigned to the Hand Piece | |||||
| Mild Grasping Position | MM | MMMG | 22 | 0.0390 | 0.0352 | 0.0075 |
| AT | ATMG | 22 | 0.0066 | 0.0083 | 0.0018 | |
| Gentle Grasping Position | MM | MMGG | 22 | 0.0458 | 0.0390 | 0.0083 |
| AT | ATGG | 22 | 0.0066 | 0.0080 | 0.0017 | |
| Moderate Grasping Position | MM | MMMoG | 22 | 0.0457 | 0.0404 | 0.0086 |
| AT | ATMoG | 22 | 0.0069 | 0.0080 | 0.0017 | |
| Tight Grasping Position | MM | MMTG | 22 | 0.0502 | 0.0436 | 0.0093 |
| AT | ATTG | 22 | 0.0122 | 0.0146 | 0.0031 | |
| Grasping Conditions | Levene’s Test for Equality of Variances | t-Test for Equality of Means | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | Sig. | t | df | Sig. (2-tailed) | MD * | SED * | 95% CID * | |||
| L * | U * | |||||||||
| Mild Grasping Position | Equal variance assumed | 45.44 | 0.000 (Not assumed) | 4.202 | 42.0 | 0.000 | 0.032 | 0.008 | 0.017 | 0.048 |
| Equal variance not assumed | 4.202 | 23.33 | 0.000 (Ho Not accepted) | 0.032 | 0.008 | 0.016 | 0.048 | |||
| Gentle Grasping Position | Equal variance assumed | 42.96 | 0.000 (Not assumed) | 4.620 | 42.0 | 0.000 | 0.039 | 0.008 | 0.022 | 0.056 |
| Equal variance not assumed | 4.620 | 22.75 | 0.000 (Ho Not accepted) | 0.039 | 0.008 | 0.022 | 0.057 | |||
| Moderate Grasping Position | Equal variance assumed | 39.55 | 0.000 (Not assumed) | 4.424 | 42.0 | 0.000 | 0.039 | 0.009 | 0.021 | 0.057 |
| Equal variance not assumed | 4.424 | 22.65 | 0.000 (Ho Not accepted) | 0.039 | 0.009 | 0.021 | 0.057 | |||
| Tight Grasping Position | Equal variance assumed | 23.24 | 0.000 (Not assumed) | 3.881 | 42.0 | 0.000 | 0.038 | 0.010 | 0.018 | 0.058 |
| Equal variance not assumed | - | - | 3.881 | 25.62 | 0.001 (Ho Not accepted) | 0.038 | 0.010 | 0.018 | 0.058 | |
| Hand Piece | MM | AT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Usage of Hand Piece | Mild | Gentle | Moderate | Tight | Mild | Gentle | Moderate | Tight | |
| Number of hand Piece | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Code assigned to hand piece | MMMG | MMGG | MMMoG | MMTG | ATMG | ATGG | ATMoG | ATTG | |
| Mean of 1/3rd-octave band vibration amplitude | 0.038959 | 0.045816 | 0.045719 | 0.050180 | 0.006588 | 0.006613 | 0.006867 | 0.012153 | |
| Std. Deviation of 1/3rd-octave band vibration amplitude | 0.0351685 | 0.0389952 | 0.0404009 | 0.0435919 | 0.0082956 | 0.0079690 | 0.0080147 | 0.0145510 | |
| Std. Error of 1/3rd-octave band vibration amplitude | 0.0074979 | 0.0083138 | 0.0086135 | 0.0092938 | 0.0017686 | 0.0016990 | 0.0017087 | 0.0031023 | |
| 95% Confidence Interval for Mean | Lower Bound | 0.023366 | 0.028526 | 0.027806 | 0.030853 | 0.002910 | 0.003080 | 0.003314 | 0.005701 |
| Upper Bound | 0.054551 | 0.063105 | 0.063632 | 0.069508 | 0.010266 | 0.010146 | 0.010421 | 0.018604 | |
| Minimum1/3rd-octave band vibration amplitude | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | |
| Maximum1/3rd-octave band vibration amplitude | 0.0962 | 0.1042 | 0.1125 | 0.1291 | 0.0234 | 0.0226 | 0.0226 | 0.0422 | |
| Hand Piece | MM | AT | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Usage of Hand Piece | Mild | Gentle | Moderate | Tight | Mild | Gentle | Moderate | Tight | ||
| Number of Hand Piece | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| Code Assigned to Hand Piece | MMMG | MMGG | MMMoG | MMTG | ATMG | ATGG | ATMoG | ATTG | ||
| MMMG | Mean Difference (I–J) | - | −0.007 | −0.007 | −0.011 | 0.032 | 0.032 | 0.032 | 0.027 | |
| Std. Error | - | 0.011 | 0.011 | 0.012 | 0.008 | 0.008 | 0.008 | 0.008 | ||
| Sig. | - | 0.999 | 0.999 | 0.980 | 0.007 | 0.007 | 0.007 | 0.046 | ||
| 95% Confidence Interval | Lower Bound | - | −0.043 | −0.043 | −0.049 | 0.007 | 0.007 | 0.007 | 0.000 | |
| Upper Bound | - | 0.029 | 0.030 | 0.027 | 0.058 | 0.058 | 0.058 | 0.053 | ||
| MMGG | Mean Difference (I–J) | 0.007 | - | 0.000 | −0.004 | 0.039 | 0.039 | 0.039 | 0.034 | |
| Std. Error | 0.011 | - | 0.012 | 0.012 | 0.008 | 0.008 | 0.008 | 0.009 | ||
| Sig. | 0.999 | - | 1.000 | 1.000 | 0.003 | 0.003 | 0.003 | 0.015 | ||
| 95% Confidence Interval | Lower Bound | −0.029 | - | −0.038 | −0.044 | 0.011 | 0.011 | 0.011 | 0.005 | |
| Upper Bound | 0.043 | - | 0.038 | 0.035 | 0.067 | 0.067 | 0.067 | 0.063 | ||
| MMMoG | Mean Difference (I–J) | 0.007 | 0.000 | - | −0.004 | 0.039 | 0.039 | 0.039 | 0.034 | |
| Std. Error | 0.011 | 0.012 | - | 0.013 | 0.009 | 0.009 | 0.009 | 0.009 | ||
| Sig. | 0.999 | 1.000 | - | 1.000 | 0.004 | 0.004 | 0.004 | 0.021 | ||
| 95% Confidence Interval | Lower Bound | −0.030 | −0.038 | - | −0.045 | 0.010 | 0.010 | 0.010 | 0.003 | |
| Upper Bound | 0.043 | 0.038 | - | 0.036 | 0.068 | 0.068 | 0.068 | 0.064 | ||
| MMGG | Mean Difference (I–J) | 0.011 | 0.004 | 0.004 | - | 0.043 | 0.044 | 0.044 | 0.038 | |
| Std. Error | 0.012 | 0.012 | 0.013 | - | 0.009 | 0.009 | 0.009 | 0.010 | ||
| Sig. | 0.980 | 1.000 | 1.000 | - | 0.003 | 0.003 | 0.003 | 0.013 | ||
| 95% Confidence Interval | Lower Bound | −0.027 | −0.035 | −0.036 | - | 0.012 | 0.012 | 0.012 | 0.006 | |
| Upper Bound | 0.049 | 0.044 | 0.045 | - | 0.075 | 0.075 | 0.075 | 0.070 | ||
| Hand Piece | MM | AT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Usage | New | Used | New | Used | |||||
| Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Code | VEMM1 | VEMM2 | VEMM3 | VEMM4 | VEAT1 | VEAT2 | VEAT3 | VEAT4 | |
| S. No. | Frequency (Hz) | 1 | 2 | 5 | 7 | 3 | 4 | 14 | 16 |
| 1 | 4 | 1.332623 | 0.893539 | 0.61474 | 0.205814 | 0.511174 | 0.888751 | 0.61867 | 0.367738 |
| 2 | 5 | 0.903326 | 1.168455 | 0.454325 | 0.263473 | 0.483062 | 1.149103 | 0.626443 | 0.279294 |
| 3 | 6.3 | 0.780509 | 1.465982 | 0.424118 | 0.282336 | 0.60051 | 1.151523 | 0.707801 | 0.367199 |
| 4 | 8 | 0.647043 | 1.751821 | 0.401938 | 0.280732 | 0.789163 | 1.264929 | 0.718729 | 0.380642 |
| 5 | 10 | 0.505716 | 1.841547 | 0.3298 | 0.243792 | 0.939132 | 1.235758 | 0.803602 | 0.321782 |
| 6 | 12.5 | 0.484758 | 1.75728 | 0.33136 | 0.22856 | 1.086217 | 1.232928 | 1.05872 | 0.254641 |
| 7 | 16 | 0.401497 | 1.551646 | 0.517135 | 0.234704 | 0.851565 | 1.214412 | 1.067767 | 0.204182 |
| 8 | 20 | 0.431736 | 1.404339 | 0.513706 | 0.223313 | 0.926529 | 0.906346 | 0.862737 | 0.181025 |
| 9 | 25 | 0.463981 | 1.16148 | 0.520726 | 0.201863 | 1.018485 | 0.876886 | 1.027158 | 0.157877 |
| 10 | 31.5 | 0.494685 | 0.928678 | 0.499663 | 0.274051 | 1.301875 | 1.069459 | 1.107523 | 0.11347 |
| 11 | 40 | 0.468912 | 0.737711 | 0.44934 | 0.33411 | 1.290452 | 1.132554 | 1.160653 | 0.174032 |
| 12 | 50 | 0.41766 | 0.582814 | 0.487399 | 0.270538 | 1.259204 | 1.07415 | 1.073087 | 0.215577 |
| 13 | 63 | 0.416147 | 0.462888 | 0.517069 | 0.218723 | 0.673837 | 1.265966 | 1.072193 | 0.211517 |
| 14 | 80 | 0.308406 | 0.36675 | 0.451595 | 0.195745 | 0.611718 | 1.00109 | 1.133893 | 0.150858 |
| 15 | 100 | 0.368654 | 0.295126 | 0.483951 | 0.284196 | 0.507438 | 0.824739 | 0.832641 | 0.121524 |
| 16 | 125 | 0.29405 | 0.230249 | 0.491351 | 0.091574 | 0.395968 | 0.673448 | 0.768315 | 0.097135 |
| 17 | 160 | 1 | 0.17764 | 0.495487 | 0.167836 | 1 | 1 | 1 | 0.522233 |
| 18 | 200 | 1 | 0.139386 | 0.480472 | 0.333333 | 1 | 1 | 1 | 1 |
| 19 | 250 | 0.333333 | 0.107947 | 0.502329 | 0.408248 | 0 | 0 | 0 | 0 |
| 20 | 315 | 0 | 0.089298 | 0.484931 | 0 | 0 | 0 | 0 | 0 |
| 21 | 400 | 0 | 0.068794 | 0.579865 | 0 | 0 | 0 | 0 | 0 |
| 22 | 500 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Hand Piece | MM | AT | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Usage | New | Used | New | Used | |||||
| Number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Code | VEMM1 | VEMM2 | VEMM3 | VEMM4 | VEAT1 | VEAT2 | VEAT3 | VEAT4 | |
| Mean | 0.502411 | 0.781062 | 0.455968 | 0.215588 | 0.693015 | 0.861911 | 0.756361 | 0.232760 | |
| Std. Deviation | 0.3353035 | 0.6354262 | 0.1213015 | 0.1083065 | 0.4244408 | 0.4431472 | 0.3998367 | 0.2207017 | |
| Std. Error | 0.0714869 | 0.1354733 | 0.0258616 | 0.0230910 | 0.0904911 | 0.0944793 | 0.0852455 | 0.0470538 | |
| 95% Confidence Interval for Mean | Lower Bound | 0.353746 | 0.499330 | 0.402186 | 0.167568 | 0.504828 | 0.665431 | 0.579083 | 0.134907 |
| Upper Bound | 0.651076 | 1.062794 | 0.509750 | 0.263609 | 0.881201 | 1.058391 | 0.933638 | 0.330614 | |
| Minimum | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | 0.0000 | |
| Maximum | 1.3326 | 1.8415 | 0.6147 | 0.4082 | 1.3019 | 1.2660 | 1.1607 | 1.0000 | |
| Hand Piece | MM | AT | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Usage of Hand Piece | New | Used | New | Used | ||||||
| Number of Hand Piece | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
| Code assigned to Hand Piece | VEMM1 | VEMM2 | VEMM3 | VEMM4 | VEAT1 | VEAT2 | VEAT3 | VEAT4 | ||
| VEMMI | Mean Difference (I–J) | - | −0.279 | 0.046 | 0.287 | −0.191 | −0.360 | −0.254 | 0.270 | |
| Std. Error | - | 0.153 | 0.076 | 0.075 | 0.115 | 0.118 | 0.111 | 0.086 | ||
| Sig. | - | 0.612 | 0.998 | 0.015 | 0.716 | 0.074 | 0.327 | 0.058 | ||
| 95% Confidence Interval | Lower Bound | - | −0.775 | −0.203 | 0.039 | −0.559 | −0.739 | −0.609 | −0.005 | |
| Upper Bound | - | 0.218 | 0.296 | 0.534 | 0.178 | 0.020 | 0.101 | 0.545 | ||
| VEMM2 | Mean Difference (I–J) | 0.279 | - | 0.325 | 0.565 | 0.088 | −0.081 | 0.025 | 0.548 | |
| Std. Error | 0.153 | - | 0.138 | 0.137 | 0.163 | 0.165 | 0.160 | 0.143 | ||
| Sig. | 0.612 | - | 0.308 | 0.009 | 0.999 | 1.000 | 1.000 | 0.015 | ||
| 95% Confidence Interval | Lower Bound | −0.218 | - | −0.134 | 0.107 | −0.435 | −0.611 | −0.491 | 0.077 | |
| Upper Bound | 0.775 | - | 0.785 | 1.024 | 0.611 | 0.449 | 0.540 | 1.020 | ||
| VEMM3 | Mean Difference (I–J) | −0.046 | −0.325 | - | 0.240 | −0.237 | −0.406 | −0.300 | 0.223 | |
| Std. Error | 0.076 | 0.138 | - | 0.035 | 0.094 | 0.098 | 0.089 | 0.054 | ||
| Sig. | 0.998 | 0.308 | - | 0.000 | 0.234 | 0.007 | 0.043 | 0.005 | ||
| 95% Confidence Interval | Lower Bound | −0.296 | −0.785 | - | 0.130 | −0.548 | −0.730 | −0.595 | 0.050 | |
| Upper Bound | 0.203 | 0.134 | - | 0.351 | 0.074 | −0.082 | −0.006 | 0.397 | ||
| VEMM4 | Mean Difference (I–J) | −0.287 | −0.565 | −0.240 | - | −0.477 | −0.646 | −0.541 | −0.017 | |
| Std. Error | 0.075 | 0.137 | 0.035 | - | 0.093 | 0.097 | 0.088 | 0.052 | ||
| Sig. | 0.015 | 0.009 | 0.000 | - | 0.001 | 0.000 | 0.000 | 1.000 | ||
| 95% Confidence Interval | Lower Bound | −0.534 | −1.024 | −0.351 | - | −0.787 | −0.969 | −0.833 | −0.187 | |
| Upper Bound | −0.039 | −0.107 | −0.130 | - | −0.168 | −0.324 | −0.248 | 0.153 | ||
| Factor | p-Value | Levene Test Ho | Equal Var. Assumed | Testing Method | p-Value | Ho | Go for Post-Hoc | Differing Parameter (Age Group) |
|---|---|---|---|---|---|---|---|---|
| Vibration exposure using different hand pieces | 0.000 | Not Accepted | Not Assumed | Welch Test | 0.000 | Not Accepted | Games–Howell Test | MUD and AUA |
| different grip positions on the vibration exposure of dentist | 0.000 | Not Accepted | Assumed | Welch Test | 0.000 | Not Accepted | Games–Howell Test | Micro Motor with Air-turbine |
| Vibration Transmissibility | 0.000 | Not Accepted | Assumed | Welch Test | 0.000 | Not Accepted | Games–Howell Test | VEMM4 with everyone except VEAT4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banga, H.K.; Goel, P.; Kumar, R.; Kumar, V.; Kalra, P.; Singh, S.; Singh, S.; Prakash, C.; Pruncu, C. Vibration Exposure and Transmissibility on Dentist’s Anatomy: A Study of Micro Motors and Air-Turbines. Int. J. Environ. Res. Public Health 2021, 18, 4084. https://doi.org/10.3390/ijerph18084084
Banga HK, Goel P, Kumar R, Kumar V, Kalra P, Singh S, Singh S, Prakash C, Pruncu C. Vibration Exposure and Transmissibility on Dentist’s Anatomy: A Study of Micro Motors and Air-Turbines. International Journal of Environmental Research and Public Health. 2021; 18(8):4084. https://doi.org/10.3390/ijerph18084084
Chicago/Turabian StyleBanga, Harish Kumar, Pankaj Goel, Raman Kumar, Vikas Kumar, Parveen Kalra, Sehijpal Singh, Sunpreet Singh, Chander Prakash, and Catalin Pruncu. 2021. "Vibration Exposure and Transmissibility on Dentist’s Anatomy: A Study of Micro Motors and Air-Turbines" International Journal of Environmental Research and Public Health 18, no. 8: 4084. https://doi.org/10.3390/ijerph18084084
APA StyleBanga, H. K., Goel, P., Kumar, R., Kumar, V., Kalra, P., Singh, S., Singh, S., Prakash, C., & Pruncu, C. (2021). Vibration Exposure and Transmissibility on Dentist’s Anatomy: A Study of Micro Motors and Air-Turbines. International Journal of Environmental Research and Public Health, 18(8), 4084. https://doi.org/10.3390/ijerph18084084