
Sadness and Other Health Complaints among Swedish Adolescents: A Cross-Sectional Study




Abstract
1. Introduction
1.1. Health Complaints among Adolescents
1.2. Developmental Changes during Adolescence
1.3. Theoretical Background
1.4. Aim
2. Materials and Methods
2.1. Study Design
2.2. Context
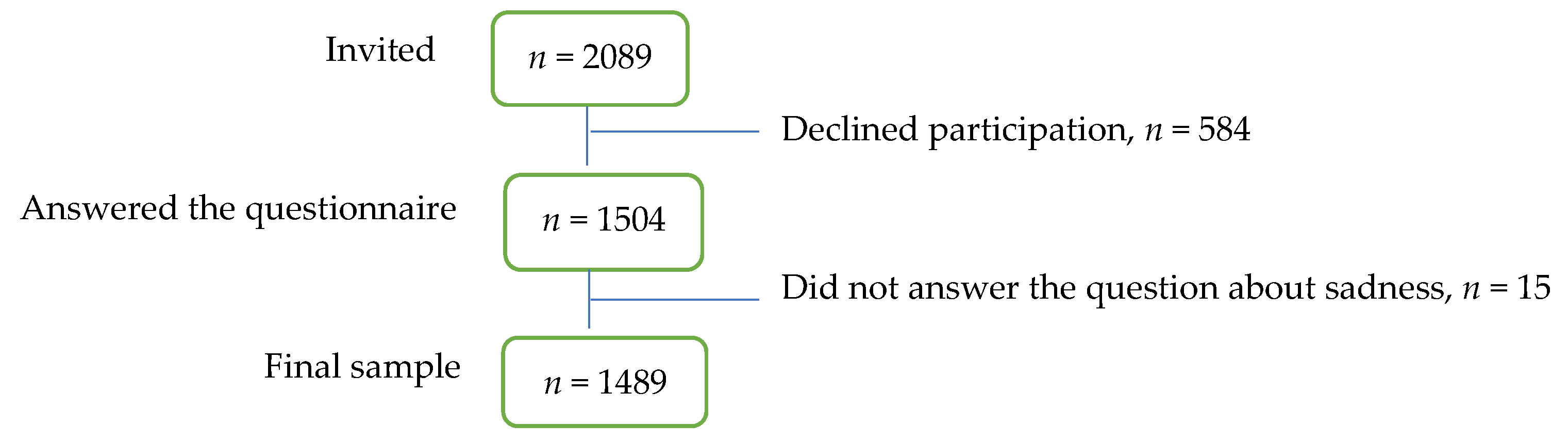
2.3. Sample and Data Collection
2.4. Data Analysis
3. Results
4. Discussion
4.1. The Prevalence of Sadness and Other Health Complaints
4.2. The Relationship between Sadness and Other Health Complaints
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Description of the Included Variables
References
- Inchley, J.; Currie, D.; Budisavljevic, S.; Torsheim, T.; Jåstad, A.; Cosma, A.; Kelly, C.; Már Arnarsson, Á. Spotlight on Adolescent Health and Well-Being: Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/332091/9789289055000-eng.pdf (accessed on 3 November 2020).
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and well-being. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef]
- Potrebny, T.; Wiium, N.; Lundegård, M.M.-I. Temporal trends in adolescents’ self-reported psychosomatic health complaints from 1980-2016: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0188374. [Google Scholar] [CrossRef]
- Breidablik, H.-J.; Meland, E.; Lydersen, S. Self-rated health in adolescence: A multifactorial composite. Scand. J. Public Health 2008, 36, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Shore, L.; Toumbourou, J.W.; Lewis, A.J.; Kremer, P. Review: Longitudinal trajectories of child and adolescent depressive symptoms and their predictors—A systematic review and meta-analysis. Child Adolesc. Ment. Health 2017, 23, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, A.W.; Wakefield, J.C. The Loss of Sadness: How Psychiatry Transformed Normal Sorrow into Depressive Disorder; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Bor, W.; Dean, A.J.; Najman, J.; Hayatbakhsh, R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Aust. N. Z. J. Psychiatry 2014, 48, 606–616. [Google Scholar] [CrossRef]
- Langton, E.G.; Collishaw, S.; Goodman, R.; Pickles, A.; Maughan, B. An emerging income differential for adolescent emotional problems. J. Child Psychol. Psychiatry 2011, 52, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Hagquist, C. Trends in adolescent mental health during economic upturns and downturns: A multilevel analysis of Swedish data 1988–2008. J. Epidemiol. Community Health 2017, 72, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Eckersley, R. A new narrative of young people’s health and well-being. J. Youth Stud. 2011, 14, 627–638. [Google Scholar] [CrossRef]
- Sweeting, H.; West, P.; Young, R.; Der, G. Can we explain increases in young people’s psychological stress over time? Soc. Sci. Med. 2010, 71, 1819–1830. [Google Scholar] [CrossRef]
- O’Keeffe, G.S.; Clarke-Pearson, K. The Impact of Social Media on Children, Adolescents and Families. Am. Acad. Pediatr. 2011, 127, 800–804. [Google Scholar] [CrossRef]
- Ottová-Jordan, V.; Smith, O.R.; Augustine, L.; Gobina, I.; Rathmann, K.; Torsheim, T.; Mazur, J.; Välimaa, R.; Cavallo, F.; Klanscek, H.J.; et al. Trends in health complaints from 2002 to 2010 in 34 countries and their association with health behaviours and social context factors at individual and macro-level. Eur. J. Public Health 2015, 25, 83–89. [Google Scholar] [CrossRef]
- Myrtveit Sæther, S.M.; Sivertsen, B.; Haugland, S.; Bøe, T.; Hysing, M. Health complaints in late adolescence; Frequency, factor structure and the association with socio-economic status. Scand. J. Public Health 2017, 46, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Hansson, E.; Garmy, P.; Vilhjálmsson, R.; Kristjánsdóttir, G. Bullying, health complaints, and self-rated health among school-aged children and adolescents. J. Int. Med. Res. 2020, 48, 1–9. [Google Scholar] [CrossRef]
- Brolin Låftman, S.; Östberg, V. The pros and cons of social relations: An analysis of adolescents’ health complaints. Soc. Sci. Med. 2006, 63, 611–623. [Google Scholar] [CrossRef]
- Gross, J.J. Emotion regulation: Taking stock and moving forward. Emotion 2013, 13, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Erikson, E.H. Ungdomens Identitetskriser [Youth Identity Crisis]; Natur & Kultur: Stockholm, Sweden, 1977. [Google Scholar]
- Arnett, J. Adolescent storm and stress, reconsidered. Am. Psychol. 1999, 54, 317–326. [Google Scholar] [CrossRef]
- Larson, R.W.; Moneta, G.; Richards, M.H.; Wilson, S. Continuity, Stability, and Change in Daily Emotional Experience across Adolescence. Child Dev. 2002, 73, 1151–1165. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Ogden, J. Making sense of children’s unexplained symptoms: Managing ambiguity, authenticity and responsibility. Psychol. Health Med. 2012, 17, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T. Ecology of the Brain: The Phenomenology and Biology of the Embodied Mind; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Merleau-Ponty, M. Kroppens Fenomenologi [The Phenomenology of the Body]; Daidalos: Göteborg, Sweden, 1999. [Google Scholar]
- SCB. Sverige har lägst andel i Materiell Fattigdom i Europa. Undersökningarna av Levnadsförhållanden (ULF/SILC) [Sweden has the Lowest Share of Material Poverty in Europe. The Living Conditions Surveys ULF/SILC]. Available online: https://www.scb.se/hitta-statistik/statistik-efter-amne/levnadsforhallanden/levnadsforhallanden/undersokningarna-av-levnadsforhallanden-ulf-silc/pong/statistiknyhet/undersokningarna-av-levnadsforhallanden-ulfsilc-2019/ (accessed on 11 November 2020).
- SCB. Högst Utbildningsnivå Bland Kvinnor och i våra Universitetsstäder. Befolkningens Utbildning 2019 [Highest Level of Edu-Cation among Women and in Our University Cities. Population Education 2019]. Available online: https://www.scb.se/hitta-statistik/statistik-efter-amne/utbildning-och-forskning/befolkningens-utbildning/befolkningens-utbildning/pong/statistiknyhet/befolkningens-utbildning-2019/ (accessed on 11 November 2020).
- SCB. Hur Försörjer sig Unga utan Gymnasieutbildning? [How Do Young People Earn a Living Without High School Education?]. Available online: https://www.scb.se/hitta-statistik/artiklar/2017/Hur-forsorjer-sig-unga-utan-gymnasieutbildning/ (accessed on 11 November 2020).
- SCB. Utbildningsnivån i Sverige. [The Level of Education in Sweden.] Statistiska Centralbyrån. Available online: https://www.scb.se/hitta-statistik/sverige-i-siffror/utbildning-jobb-och-pengar/utbildningsnivan-i-sverige/ (accessed on 11 November 2020).
- Norman, G.R.; Streiner, D.L. Biostatistics: The Bare Essentials, 4th ed.; PMPH USA: Shelton, CT, USA, 2014. [Google Scholar]
- Bauer, G.R.; Braimoh, J.; Scheim, A.I.; Dharma, C. Transgender-inclusive measures of sex/gender for population surveys: Mixed-methods evaluation and recommendations. PLoS ONE 2017, 12, e0178043. [Google Scholar] [CrossRef] [PubMed]
- Haugland, S.; Wold, B. Subjective health complaints in adolescence—Reliability and validity of survey methods. J. Adolesc. 2001, 24, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Voyer, D.; Voyer, S.D. Gender differences in scholastic achievement: A meta-analysis. Psychol. Bull. 2014, 140, 1174–1204. [Google Scholar] [CrossRef]
- Pekrun, R.; Lichtenfeld, S.; Marsh, H.W.; Murayama, K.; Goetz, T. Achievement Emotions and Academic Performance: Longitudinal Models of Reciprocal Effects. Child Dev. 2017, 88, 1653–1670. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F.; Bliss-Moreau, E. She’s emotional. He’s having a Bad Day: Attributional explanations for emotion stereo-types. Emotion 2009, 9, 649–658. [Google Scholar] [CrossRef]
- Callegari, J.; Levander, U. Kompetent aktör eller psykiskt skör? Barn- och flickdiskurser i konstruktionen av ungas psykiska ohälsa [Competent and agile, or mentally fragile? Child- and girlhood discourses shaping views of young peoples’ mental health.]. Tidskr. Genusvetenskap 2019, 40, 72–95. [Google Scholar]
- Burkitt, I. Emotions and Social Relations; SAGE Publications Ltd.: London, UK, 2014. [Google Scholar]
- Samulowitz, A.; Gremyr, I.; Eriksson, E.; Hensing, G. ”Brave men” and ”emotional women”: A theory guided literature review on gender bias in health care and gendered norms towards patients with chronic pain. Pain Res. Manag. 2018, 2018, 14. [Google Scholar] [CrossRef] [PubMed]
- Addis, M.E.; Mahalik, J.R. Men, masculinity and the context of help seeking. Am. Psychol. 2003, 58, 5–14. [Google Scholar] [CrossRef]
- The Public Health Agency of Sweden. Statistik om Suicid. [Suicide Statistics.]. Available online: https://www.folkhalsomyndigheten.se/suicidprevention/statistik-om-suicid/ (accessed on 20 November 2020).
- Miranda-Mendizabal, A.; Castellví, P.; Parés-Badell, O.; Alayo, I.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; et al. Gender differences in suicidal behavior in adolescents and young adults: Systematic review and meta-analysis of longitudinal studies. Int. J. Public Health 2019, 64, 265–283. [Google Scholar] [CrossRef]
- Connolly, M.D.; Zervos, M.J.; Barone II, C.J.; Johnson, C.C.; Joseph, C.L.M. The mental health of transgender youth: Advances in understanding. J. Adolesc. Health 2016, 59, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Plenty, S.; Mood, C. Money, peers and parents: Social and economic aspects in inequality in youth well-being. J. Youth Adolesc. 2016, 45, 1294–1308. [Google Scholar] [CrossRef]
- Heinrich, L.M.; Gullone, E. The clinical significance of loneliness: A literature review. Clin. Psychol. Rev. 2006, 26, 695–718. [Google Scholar] [CrossRef]
- Bohman, H.; Låftman, B.S.; Cleland, N.; Lundberg, M.; Päären, A.; Jonsson, U. Somatic symptoms in adolescence as a predictor of severe mental illness in adulthood: A long-term community-based follow-up study. Child Adolesc. Psychiatry Ment. Health 2018, 12, 42. [Google Scholar] [CrossRef]
- Borgman, S.; Ericsson, I.; Clausson, E.K.; Garmy, P. The Relationship Between Reported Pain and Depressive Symptoms Among Adolescents. J. Sch. Nurs. 2020, 36, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, M.T.; Graff, L.; Avery, L.; Palatnick, C.; Parnerowski, K.; Targownik, L. Gastrointestinal symptoms before and during menses in healthy women. BMC Women’s Health 2014, 14, 14. [Google Scholar] [CrossRef] [PubMed]
- Hoeppner, B.B.; Kelly, J.F.; Urbanoski, K.A.; Slaymaker, V. Comparative utility of a single-item versus multiple-item measure of self-efficacy in predicting relapse among young adults. J. Subst. Abus. Treat. 2011, 41, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, R.; Patalay, P.; Humphrey, N. A systematic literature review of existing conceptualization and measurement of mental health literacy in adolescent research: Current challenges and inconsistencies. BMC Public Health 2020, 20, 607. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Factors | Total n (%) | Sadness Often or Always n = 325 (21.8%) n (%) | Sadness Never, Rarely or Sometimes n = 1164 (78.2%) n (%) | ꭓ² | p-Value |
|---|---|---|---|---|---|
| Gender | 17.5 | <0.0001 | |||
| Male | 643 (43.2) | 172 (52.9) | 471 (40.5) | ||
| Female | 821 (55.1) | 146 (44.9) | 675 (58.0) | ||
| Other | 25 (1.7) | 7 (2.2) | 18 (1.5) | ||
| Perceived family financial situation | 14.7 | <0.0001 | |||
| Average/ not very good/not good at all | 394 (26.5) | 113 (34.8) | 281 (24.1) | ||
| Very good/quite good | 1095 (73.5) | 212 (65.2) | 883 (75.9) | ||
| Sleeping difficulties | 104.5 | <0.0001 | |||
| ≥ Once a week | 686 (46.1) | 231 (71.1) | 455 (39.1) | ||
| < Once a week | 803 (53.9) | 94 (28.9) | 709 (60.9) | ||
| Headache | 70.8 | <0.0001 | |||
| Often/always | 241 (16.2) | 102 (31.4) | 139 (11.9) | ||
| Never/rarely/sometimes | 1248 (83.8) | 223 (68.6) | 1025 (88.1) | ||
| Abdominal pain | 55.1 | <0.0001 | |||
| Often/always | 174 (11.7) | 76 (23.4) | 98 (8.4) | ||
| Never/rarely/sometimes | 1315 (88.3) | 249 (76.6) | 1066 (91.6) | ||
| Reduced appetite | 133.6 | <0.0001 | |||
| Often/always | 193 (13.0) | 104 (32.0) | 89 (7.6) | ||
| Never/rarely/sometimes | 1296 (87.0) | 221 (68.0) | 1075 (92.4) | ||
| Tension | 161.3 | <0.0001 | |||
| Often/always | 393 (26.4) | 150 (46.2) | 218 (18.7) | ||
| Never/rarely/sometimes | 1096 (73.6) | 175 (53.8) | 946 (81.3) | ||
| Concentration difficulties | 167.8 | <0.0001 | |||
| Often/always | 468 (31.4) | 198 (60.9) | 270 (23.2) | ||
| Never/rarely/sometimes | 1021 (68.6) | 127 (39.1) | 894 (76.8) |
| Independent Variables | OR | (95% Cl for OR) | p-Value |
|---|---|---|---|
| Sleeping difficulties every week | 2.04 | (1.52–2.76) | <0.0001 |
| Headache often or always | 1.56 | (1.20–2.22) | 0.013 |
| Abdominal pain often or always | 1.27 | (0.85–1.90) | 0.238 |
| Reduced appetite often or always | 2.56 | (1.77–3.69) | <0.0001 |
| Tension often or always | 2.47 | (1.83–3.34) | <0.0001 |
| Concentration difficulties often or always | 2.82 | (2.10–3.77) | <0.0001 |
| Independent Variables | OR 1 | (95% Cl for OR) | p-Value |
|---|---|---|---|
| Sleeping difficulties every week | 2.00 | (1.48–2.70) | <0.0001 |
| Headache often or always | 1.58 | (1.11–2.24) | 0.011 |
| Abdominal pain often or always | 1.33 | (0.89–1.99) | 0.168 |
| Reduced appetite often or always | 1.43 | (1.68–3.51) | <0.0001 |
| Tension often or always | 2.44 | (1.80–3.29) | <0.0001 |
| Concentration difficulties often or always | 2.75 | (2.05–3.69) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garnow, T.; Einberg, E.-L.; Edberg, A.-K.; Garmy, P. Sadness and Other Health Complaints among Swedish Adolescents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 3999. https://doi.org/10.3390/ijerph18083999
Garnow T, Einberg E-L, Edberg A-K, Garmy P. Sadness and Other Health Complaints among Swedish Adolescents: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(8):3999. https://doi.org/10.3390/ijerph18083999
Chicago/Turabian StyleGarnow, Tide, Eva-Lena Einberg, Anna-Karin Edberg, and Pernilla Garmy. 2021. "Sadness and Other Health Complaints among Swedish Adolescents: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 8: 3999. https://doi.org/10.3390/ijerph18083999
APA StyleGarnow, T., Einberg, E.-L., Edberg, A.-K., & Garmy, P. (2021). Sadness and Other Health Complaints among Swedish Adolescents: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 18(8), 3999. https://doi.org/10.3390/ijerph18083999