
Lessons Learned from Replicating a Randomized Control Trial Evaluation of an App-Based Sexual Health Program



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Procedures
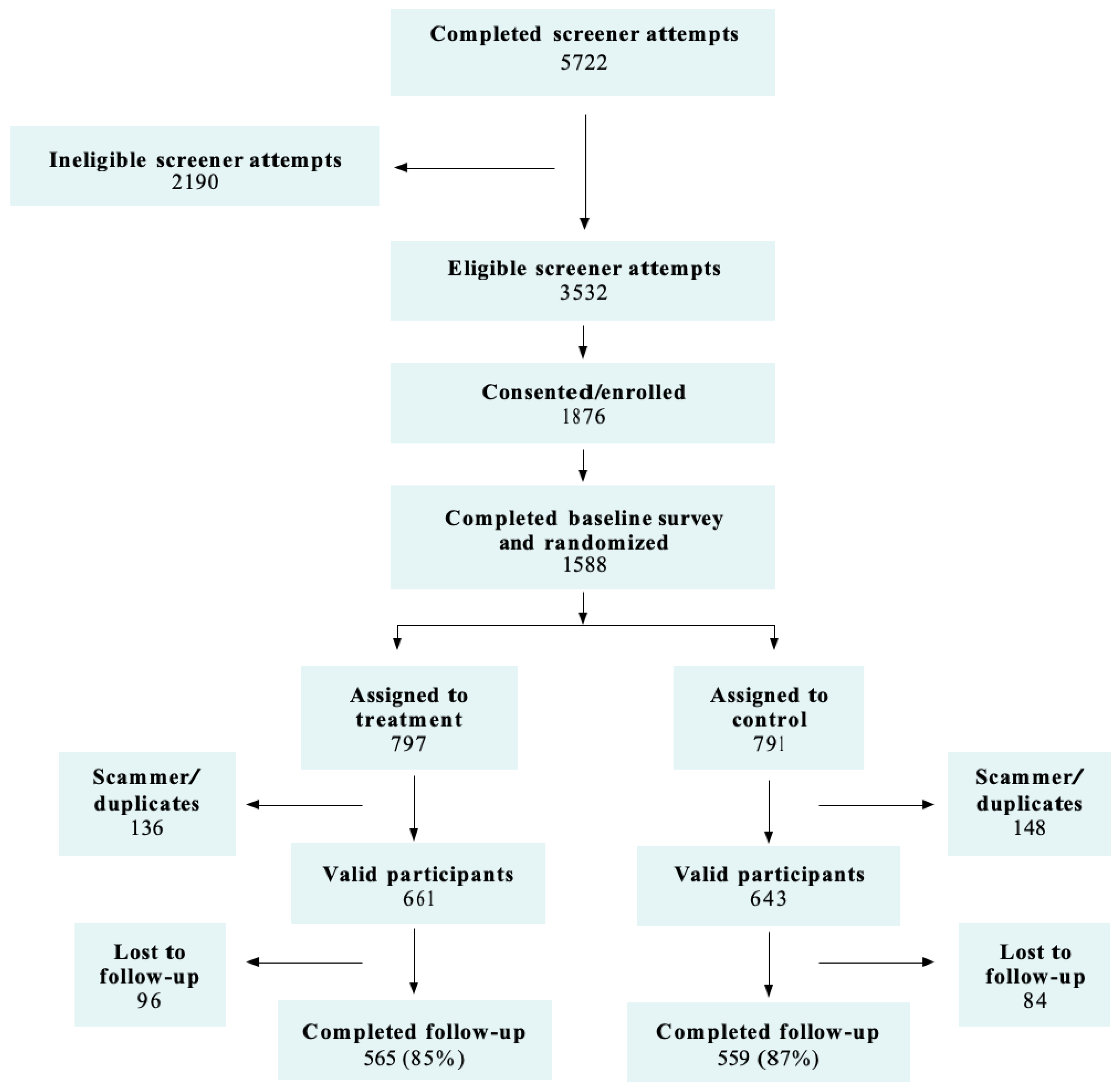
2.1.1. Enrollment and Randomization
2.1.2. Scammers and Duplicate Accounts
2.1.3. Intervention and Control Apps
2.1.4. Text Messages
2.2. Data Collection
2.3. Survey Instruments and Measures
2.4. App Usage
2.5. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Widman, L.; Nesi, J.; Kamke, K.; Choukas-Bradley, S.; Stewart, J. Technology-based interventions to reduce sexually transmitted infections and unintended pregnancy among youth. J. Adolesc. Health 2018, 62, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Noar, S.; Fitts Willoughby, J. eHealth interventions for HIV prevention. AIDS Care 2012, 24, 945–952. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Noar, S.; Black, H.; Pierce, L. Efficacy of computer technology-based HIV prevention interventions: A meta-analysis. AIDS Care 2009, 23, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.; Hamilton, B.; Osterman, M.; Driscoll, A. Births: Final Data for 2018; National Center for Health Statistics: Hyattsville, MD, USA, 2019.
- Finer, L.; Zolna, M. Declines in unintended pregnancy in the United States, 2008–2011. N. Engl. J. Med. 2016, 374, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Guse, K.; Levine, D.; Martins, S.; Lira, A.; Gaarde, J.; Westmorland, W.; Gilliam, M. Interventions using new digital media to improve adolescent sexual health: A systematic review. J. Adolesc. Health 2012, 51, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Noar, S. Computer technology-based interventions in HIV prevention: State of the evidence and future directions for research. AIDS Care 2011, 23, 525–533. [Google Scholar] [CrossRef]
- Blackstock, O.; Patel, V.; Cunningham, C. Use of technology for HIV prevention among adolescent and adult women in the United States. Curr. HIV/AIDS Rep. 2015, 12, 489–499. [Google Scholar] [CrossRef]
- Steinberg, A.; Griffin-Tomas, M.; Abu-Odeh, D.; Whitten, A. Evaluation of a mobile phone app for providing adolescents with sexual and reproductive health information, New York City, 2013–2016. Public Health Rep. 2018, 133, 234–239. [Google Scholar] [CrossRef]
- Antonishak, J.; Kaye, K.; Swiader, L. Impact of an online birth control support network on unintended pregnancy. Soc. Mark. Q. 2015, 21, 23–36. [Google Scholar] [CrossRef]
- Lugo-Gil, J.; Lee, A.; Vohra, D.; Harding, J.; Ochoa, L.; Goesling, B. Updated Findings from the HHS Teen Pregnancy Prevention Evidence Review: August 2015 through October 2016; U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation: Washington, DC, USA, 2018.
- Downing, R.; LaVeist, T.; Bullock, H. Intersections of ethnicity and social class in provider advice regarding reproductive health. Am. J. Public Health 2007, 97, 1803–1807. [Google Scholar] [CrossRef]
- Dehlendorf, C.; Ruskin, R.; Grumbach, K.; Vittinghoff, E.; Bibbins-Domingo, K.; Schillinger, D.; Steinauer, J. Recommendations for intrauterine contraception: A randomized trial of the effects of patients’ race/ethnicity and socioeconomic status. Am. J. Obstet. Gynecol. 2010, 203, 319.e311–319.e318. [Google Scholar] [CrossRef]
- Rocca, C.; Harper, C. Do racial and ethnic differences in contraceptive attitudes and knowledge explain disparities in method use? Sex. Reprod. Health 2012, 44, 150–158. [Google Scholar] [CrossRef]
- Higgins, J.; Kramer, R.; Ryder, K. Provider bias in long-acting reversible contraception (LARC) promotion and removal: Perceptions of young adult women. Am. J. Public Health 2016, 106, 1932–1937. [Google Scholar] [CrossRef]
- Manlove, J.; Cook, E.; Whitfield, B.; Johnson, M.; Martinez-Garcia, G.; Garrido, M. Short-term impacts of Pulse: An app-based teen pregnancy prevention progrm for Black and Latinx women. J. Adolesc. Health 2020, 66, 224–232. [Google Scholar] [CrossRef] [PubMed]
- DiClemente, R.; Wingood, G.; Sales, J.; Brown, J.; Rose, E.; Davis, T.; Lang, D.; Caliendo, A.; Hardin, J. Efficacy of a telephone-delivered sexually transmitted infection/human immunodeficiency virus prevention maintenance interveiton for adolescents: A randomized clinical trial. JAMA Pediatrics 2014, 168, 938–946. [Google Scholar] [CrossRef]
- Brayboy, L.; McCoy, K.; Thamotharan, S.; Zhu, E.; Gil, G.; Houck, C. The use of technology in the sexual health education especially among minority adolescent girls in the United States. Curr. Opin. Obstet. Gynecol. 2018, 30, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Goesling, B. Making Sense of Replication Studies: Guidance for Teen Pregnancy Prevention Researchers; Office of the Assistant Secretary for Planning and Evaluation, Office of Human Services Policy, US Department of Health and Human Services: Washington, DC, USA, 2015.
- Kappeler, E. Building the evidence to prevent adolescent pregnancy. Am. J. Public Health 2016, 106, S5. [Google Scholar] [CrossRef]
- Valentine, J.; Biglan, A.; Boruch, R.; Gonzalez Castro, F.; Collins, L.; Flay, B.; Kellam, S.; Moscicki, E.; Schincke, S. Replication in prevention science. Prev. Sci. 2011, 12, 103–117. [Google Scholar] [CrossRef]
- Dehlendorf, C.; Rodriguez, M.; Levy, K.; Borrero, S.; Steinauer, J. Disparities in family planning. Am. J. Obstet. Gynecol. 2010, 202, 214–220. [Google Scholar] [CrossRef]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Bandura, A. Cognitive Social Learning Theory. In Six Theories of Child Development; Lawler, E., Ed.; JAI: Greenwich, CT, USA, 1989. [Google Scholar]
- Manlove, J.; Cook, E.; Whitfield, B.; Johnson, M.; Finocharo, J. Evaluating Pulse: Lessons from an Online Evaluation of an App-Based Approach to Teen Pregnancy Prevention; Child Trends: Bethesda, MD, USA, 2019. [Google Scholar]
- Healthy Teen Network. What We Do: Pulse. Available online: https://www.healthyteennetwork.org/projects/pulse/#:~:text=Healthy%20Teen%20Network%20is%20evaluating,informative%2C%20youth%2Dengaging%20platform. (accessed on 29 June 2020).
- Harris, K. The National Longitudinal Study of Adolescent Health (Add Health), Waves I & II, 1994–1996; Wave III, 2001–2002; Wave IV, 2007–2009; Carolina Population Center: Chapel Hill, NC, USA, 2009. [Google Scholar]
- National Survey of Family Growth. National Survey of Family Growth, User’s Guide; U.S. Department of Health and Human Services: Hyattsville, MD, USA, 2013.
- Frost, J.; Lindberg, L.; Finer, L. Young adults’ contraceptive knowledge, norms, and attitudes: Associations with risk of unintended pregnancy. Perspect. Sex. Reprod. Health 2012, 44, 107–116. [Google Scholar] [CrossRef]
- Healthy Teen Network. Crush: Research Brief; Healthy Teen Network: Baltimore, MD, USA, 2018. [Google Scholar]
- Smith, K.; Colman, S. Evaluation of Adolescent Pregnancy Prevention Approaches: Design of the Imapct Study; Mathematica Policy Research: Princeton, NJ, USA, 2012. [Google Scholar]
- Office of Adolescent Health. Resource: Survey Items; Office of Adolescent Health: Washington, DC, USA, 2016. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Matts, J.; Lachin, J. Properties of permuted-block randomization in clinical trials. Control. Clin. Trials 1988, 9, 327–344. [Google Scholar] [CrossRef]
- Deke, J. Using the Linear Probability Model to Estimate Impacts on Binary Outcomes in Randomized Controlled Trials; Mathematica Policy Research: Washington, DC, USA, 2014. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Jackson, A.; Karasek, D.; Dehlendorf, C.; Greene Foster, D. Racial and ethnic differences in women’s preferences for features of contraceptive methods. Contraception 2016, 93, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.; Bogart, L. Birth control conspiracy beliefs, perceived discrimination, and contraception among African Americans: An exploratory study. J. Health Psychol. 2003, 8, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Peskin, M.; Shegog, R.; Markham, C.; Thiel, M.; Baumler, E.; Addy, R.; Gabay, E.; Tortolero, E. Efficacy of It’s Your Game-Tech: A computer-based sexual health education program for middle school youth. J. Adolesc. Health 2015, 56, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Whitfield, B.; Welti, K.; Manlove, J. Evaluating Young Women’s Engagement with an Online Reproductive Health App; Child Trends: Bethesda, MD, USA, 2019. [Google Scholar]
- Confessore, N. Cambridge Analytica and Facebook: The Scandal and the Fallout So Far. The New York Times. 4 April 2018. Available online: https://www.nytimes.com/2018/04/04/us/politics/cambridge-analytica-scandal-fallout.html (accessed on 30 April 2020).
- Arigo, D.; Pagoto, S.; Carter-Harris, L.; Lillie, S.; Nebeker, C. Using social media for health research: Methodological and ethical considerations for recruitment and intervention delivery. Digit. Health 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Moreno, M.; Waite, A.; Pumper, M.; Colburn, T.; Holm, M.; Mendoza, J. Recruiting adolescent research participants: In-person compared to social media approaches. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Topolovec-Vranic, J.; Natarajan, K. The use of socialmedia in recruitment for medical research studies: A scoping review. J. Med. Internet Res. 2016, 18, e286. [Google Scholar] [CrossRef]
- Eichner, J.; Salaway, J.; Smith-Jones, J.; McCall, R. Evaluation of Seventeen Days in Ohio, Pennsylvania, and West Virginia: Findings from the Replication of an Evidence-Based Teen Pregnancy Prevention Program; University of Pittsburgh, Office of Child Development: Pittsburgh, PA, USA, 2015. [Google Scholar]
- Bridges, T.; Moore, M. 23% of Young Black Women Now Identify as Bisexual. Available online: https://theconversation.com/23-of-young-black-women-now-identify-as-bisexual-116116 (accessed on 30 April 2020).
- Office of Adolescent Health. Results from the OAH Teen Pregnancy Prevention Program; HHS Office of Adolescent Health: Washington, DC, USA, 2015.


{kind=link}
| Measure | Pulse Intervention %/Mean | Control %/Mean | Difference | p-Value * |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Age at baseline (mean years) | 18.7 | 18.8 | 0.0 | 0.656 |
| Race/Hispanic ethnicity | ||||
| Hispanic | 53.5% | 49.2% | −4.3% | 0.209 |
| Non-Hispanic Black | 46.5% | 50.8% | 4.3% | 0.209 |
| Highest level of education attained | ||||
| Less than high school degree or GED | 19.8% | 24.0% | 4.2% | 0.133 |
| High school degree or GED | 18.0% | 14.0% | −4.0% | 0.106 |
| Some college, technical school, or more | 62.2% | 61.8% | −0.4% | 0.897 |
| Has at least one child | 8.8% | 8.7% | −0.1% | 0.967 |
| Currently living with family | 76.0% | 79.2% | 3.1% | 0.267 |
| Sexual activity and pregnancy history | ||||
| Ever had vaginal sex | 66.9% | 66.1% | −0.8% | 0.793 |
| Vaginal sex in the past three months | 54.6% | 54.9% | 0.3% | 0.926 |
| Ever been pregnant | 12.1% | 12.1% | 0.0% | 0.983 |
| Unprotected sex (in past 3 months) | ||||
| Sex without any method | 26.2% | 29.0% | 2.8% | 0.361 |
| Sex without a hormonal/LARC method | 28.5% | 33.4% | 4.9% | 0.122 |
| Contraceptive use | ||||
| Current hormonal/LARC use a | 40.3% | 36.1% | −4.2% | 0.304 |
| Hormonal/LARC use at last sex b | 47.2% | 41.0% | −6.2% | 0.173 |
| Sample N | 434 | 437 | ||
| Measure | Original Study %/Mean | Replication Study %/Mean | Difference | p-Value * |
|---|---|---|---|---|
| Sociodemographic characteristics | ||||
| Age at baseline (mean years) | 18.8 | 18.7 | 0.0 | 0.679 |
| Race/Hispanic ethnicity | ||||
| Hispanic | 38.8% | 53.5% | 14.7% | 0.000 * |
| Non-Hispanic Black | 37.3% | 46.5% | 9.2% | 0.003 * |
| Non-Hispanic Other a | 23.9% | 0.0% | −23.9% | 0.000 * |
| Highest level of education attained | ||||
| Less than high school | 16.6% | 19.8% | 3.2% | 0.195 |
| High school degree or GED | 11.7% | 18.0% | 6.3% | 0.005 * |
| Some college, technical school, or more | 71.7% | 62.2% | −9.5% | 0.002 * |
| Has at least one child | 6.4% | 8.8% | 2.4% | 0.153 |
| Currently living with family | 80.2% | 76.0% | −4.1% | 0.115 |
| Sexual activity and pregnancy history | ||||
| Ever had vaginal sex | 68.8% | 66.9% | −2.0% | 0.513 |
| Vaginal sex in the past three months | 56.6% | 54.6% | −1.9% | 0.544 |
| Ever been pregnant | 8.9% | 12.1% | 3.2% | 0.100 |
| Ever had a pregnancy scare | 48.7% | 49.0% | 0.3% | 0.928 |
| Unprotected sex (in past 3 months) | ||||
| Sex without any method | 23.5% | 26.2% | 2.7% | 0.331 |
| Sex without a hormonal/LARC method | 28.3% | 28.5% | 0.2% | 0.946 |
| Contraceptive use | ||||
| Current hormonal/LARC use b | 49.4% | 40.3% | −9.1% | 0.019 * |
| Hormonal/LARC use at last sex c | 58.2% | 47.2% | −10.9% | 0.011 * |
| Birth control knowledge (% correct) | 43.4% | 39.7% | −3.7% | 0.092 |
| Attitudes | ||||
| Attitudes about birth control | ||||
| Disagree that birth control is too much of a hassle to use | 59.8% | 52.0% | −7.8% | 0.014 * |
| Disagree that birth control has too many negative side effects | 37.8% | 29.4% | −8.5% | 0.005 * |
| Attitudes about sexual and reproductive health care | ||||
| Disagree that going to a health care provider for sexual and reproductive health services is hard | 47.7% | 50.1% | 2.4% | 0.448 |
| Disagree that going to a health care provider for sexual and reproductive health services is expensive | 25.6% | 25.8% | 0.1% | 0.961 |
| Self-Efficacy and Intentions | ||||
| Self-efficacy to use birth control | ||||
| Confident can use birth control during every sexual intercourse | 63.9% | 56.1% | −7.9% | 0.012 * |
| Self-efficacy to access sexual and reproductive health services | ||||
| Confident can go to a health care provider for sexual and reproductive health services | 78.4% | 79.9% | 1.5% | 0.573 |
| Intentions | ||||
| Intend to visit a health care provider for sexual or reproductive health services | 37.8% | 36.7% | −1.0% | 0.735 |
| Intend to use a hormonal/LARC method | 58.3% | 55.7% | −2.6% | 0.411 |
| App Usage | ||||
| Ever logged into the app | 86.5% | 85.3% | −1.3% | 0.596 |
| Logged into the app more than once | 51.6% | 39.9% | −11.8% | 0.001 * |
| Average number of app logins | 2.8 | 2.2 | −0.6 | 0.002 * |
| Average number of app clicks | 34.3 | 23.3 | −11.1 | 0.000 * |
| Average number of sections visited (out of six) | 3.7 | 3.4 | −0.4 | 0.030 * |
| Visited all six sections | 45.2% | 40.5% | −4.8% | 0.169 |
| Average percentage of activities completed d | 27.8% | 21.9% | −5.9% | 0.002 * |
| Text Messages | ||||
| Opted out of receiving texts | 10.5% | 10.1% | −0.3% | 0.875 |
| Experienced a bounce back e | 25.6% | 16.6% | −9.0% | 0.001 * |
| Received a reminder text | 61.9% | 78.1% | 16.3% | 0.000 * |
| Received all content texts | 59.1% | 68.7% | 9.6% | 0.003 * |
| Sample N | 565 | 434 | ||
| Measure | Total Sample Size | Pulse Intervention | Control | Difference | p-Value |
|---|---|---|---|---|---|
| Unprotected sex (in past 6 weeks) | |||||
| Sex without any method | |||||
| Original study | 1087 | 22.7 | 25.1 | −2.40 | 0.265 |
| Replication study | 851 | 23.6 | 24.5 | −0.95 | 0.694 |
| Sex without a hormonal/LARC method | |||||
| Original study | 1086 | 22.1 | 29.7 | −7.56 | 0.001 * |
| Replication study | 858 | 28.7 | 23.8 | 4.82 | 0.058 |
| Contraceptive use | |||||
| Current hormonal/LARC use a | |||||
| Original study | 763 | 48.9 | 49.1 | −0.16 | 0.945 |
| Replication study | 571 | 39.1 | 36.5 | 2.60 | 0.277 |
| Hormonal/LARC use at last sex b | |||||
| Original study | 578 | 49.1 | 51.7 | −2.62 | 0.379 |
| Replication study | 409 | 45.1 | 40.7 | 4.40 | 0.156 |
| Birth control knowledge (% correct) | |||||
| Original study | 1124 | 51.5 | 44.5 | 7.04 | 0.000 * |
| Replication study | 851 | 49.8 | 41.8 | 8.00 | 0.000 * |
| Attitudes | |||||
| Attitudes about birth control | |||||
| Disagree that birth control is too much of a hassle to use | |||||
| Original study | 1122 | 55.5 | 53.9 | 1.61 | 0.539 |
| Replication study | 854 | 45.5 | 45.8 | −0.33 | 0.914 |
| Disagree that birth control has too many negative side effects | |||||
| Original study | 1119 | 37.5 | 33.8 | 3.72 | 0.144 |
| Replication study | 855 | 23.2 | 22.0 | 1.16 | 0.642 |
| Attitudes about sexual and reproductive health care | |||||
| Disagree that going to a health care provider for sexual and reproductive health services is hard | |||||
| Original study | 1120 | 53.0 | 51.4 | 1.70 | 0.524 |
| Replication study | 847 | 49.9 | 46.4 | 3.54 | 0.265 |
| Disagree that going to a health care provider for sexual and reproductive health services is expensive | |||||
| Original study | 1119 | 30.8 | 25.5 | 5.30 | 0.027 c |
| Replication study | 843 | 29.6 | 26.0 | 3.60 | 0.212 |
| Self-Efficacy and Intentions | |||||
| Birth control self-efficacy | |||||
| Confident can use birth control during every sexual intercourse | |||||
| Original study | 1123 | 67.3 | 61.5 | 5.75 | 0.025 * |
| Replication study | 850 | 52.9 | 51.5 | 1.43 | 0.645 |
| Sexual and reproductive health self-efficacy | |||||
| Confident can go to a health care provider for sexual and reproductive health services | |||||
| Original study | 1118 | 80.0 | 80.3 | −0.30 | 0.898 |
| Replication study | 849 | 75.7 | 72.6 | 3.04 | 0.306 |
| Intentions | |||||
| Intend to visit a health care provider for sexual or reproductive health services | |||||
| Original study | 1121 | 43.4 | 39.5 | 3.90 | 0.120 |
| Replication study | 866 | 42.2 | 39.6 | 2.58 | 0.396 |
| Intend to use a hormonal/LARC method | |||||
| Original study | 1121 | 57.2 | 54.4 | 2.83 | 0.273 |
| Replication study | 864 | 54.5 | 48.6 | 5.89 | 0.052 |
| Measure | Total Sample Size | Pulse Intervention | Control | Difference | p-Value |
|---|---|---|---|---|---|
| Unprotected sex (in past three months) | |||||
| Sex without any method | 766 | 31.2 | 31.9 | −0.95 | 0.694 |
| Sex without a hormonal/LARC method | 778 | 32.0 | 32.6 | −0.53 | 0.863 |
| Contraceptive use (among sexually experienced at baseline) | |||||
| Current hormonal/LARC use a | 503 | 37.2 | 36.7 | 0.58 | 0.858 |
| Hormonal/LARC use at last sex b | 391 | 43.4 | 40.8 | 2.65 | 0.508 |
| Pregnancy history | |||||
| Ever been pregnant | 752 | 16.6 | 18.3 | −1.70 | 0.278 |
| Pregnancy scare in past six months | 751 | 34.8 | 33.7 | 1.15 | 0.710 |
| Clinic utilization | |||||
| Visited a provider for sexual and reproductive health services in past six months | 784 | 41.7 | 38.5 | 3.18 | 0.326 |
| Birth control knowledge (% correct) | 772 | 50.6 | 47.1 | 3.49 | 0.096 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manlove, J.; Whitfield, B.; Finocharo, J.; Cook, E. Lessons Learned from Replicating a Randomized Control Trial Evaluation of an App-Based Sexual Health Program. Int. J. Environ. Res. Public Health 2021, 18, 3305. https://doi.org/10.3390/ijerph18063305
Manlove J, Whitfield B, Finocharo J, Cook E. Lessons Learned from Replicating a Randomized Control Trial Evaluation of an App-Based Sexual Health Program. International Journal of Environmental Research and Public Health. 2021; 18(6):3305. https://doi.org/10.3390/ijerph18063305
Chicago/Turabian StyleManlove, Jennifer, Brooke Whitfield, Jane Finocharo, and Elizabeth Cook. 2021. "Lessons Learned from Replicating a Randomized Control Trial Evaluation of an App-Based Sexual Health Program" International Journal of Environmental Research and Public Health 18, no. 6: 3305. https://doi.org/10.3390/ijerph18063305
APA StyleManlove, J., Whitfield, B., Finocharo, J., & Cook, E. (2021). Lessons Learned from Replicating a Randomized Control Trial Evaluation of an App-Based Sexual Health Program. International Journal of Environmental Research and Public Health, 18(6), 3305. https://doi.org/10.3390/ijerph18063305