
Too Much of a Good Thing? Exercise Dependence in Endurance Athletes: Relationships with Personal and Social Resources



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Preliminary Analysis
3.3. Descriptive Statistics and Correlation Analyses
3.4. Regression Analyses
3.5. Mediation Analyses—Self-Control, Self-Concordance and Exercise Dependence
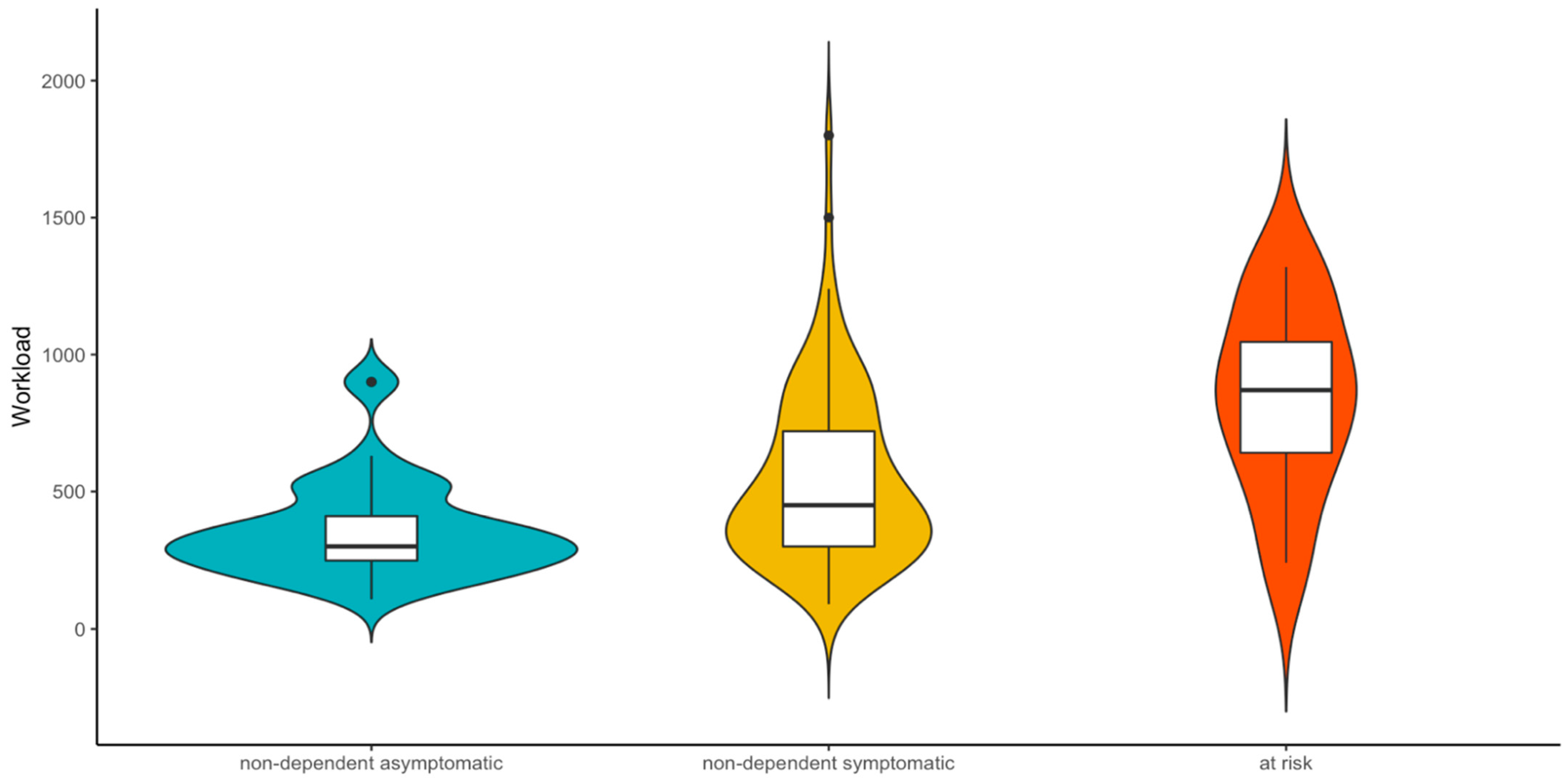
3.6. Supplemental Analysis—Risk Factor Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reiner, M.; Niermann, C.; Jekauc, D.; Woll, A. Long-term health benefits of physical activity—A systematic review of longitudinal studies. BMC Public Health 2013, 13, 813. [Google Scholar] [CrossRef]
- WHO. Guidelines on Physical Activity and Sedentary Behaviour. Available online: https://www.who.int/publications/i/item/9789240015111 (accessed on 1 December 2020).
- O’Donovan, G.; Blazevich, A.J.; Boreham, C.; Cooper, A.R.; Crank, H.; Ekelund, U.; Fox, K.R.; Gately, P.; Giles-Corti, B.; Gill, J.M.R.; et al. The ABC of Physical Activity for Health: A consensus statement from the British Association of Sport and Exercise Sciences. J. Sports Sci. 2010, 28, 573–591. [Google Scholar] [CrossRef] [PubMed]
- Berczik, K.; Szabó, A.; Griffiths, M.D.; Kurimay, T.; Kun, B.; Urbán, R.; Demetrovics, Z. Exercise addiction: Symptoms, diagnosis, epidemiology, and etiology. Subst. Use Misuse 2012, 47, 403–417. [Google Scholar] [CrossRef] [PubMed]
- Szabo, A.; Griffiths, M.D.; Marcos, R.D.L.V.; Mervó, B.; Demetrovics, Z. Methodological and conceptual limitations in exercise addiction research. Yale J. Biol. Med. 2015, 88, 303. [Google Scholar] [PubMed]
- Brown, R.I.F. Some contributions of the study of gambling to the study of other addictions. In Gambling Behavior and Problem Gambling; Eadington, W.R., Cornelius, J.A., Eds.; University of Nevada Press: Reno, NV, USA, 1993; pp. 241–272. [Google Scholar]
- Griffiths, M. A ‘components’ model of addiction within a biopsychosocial framework. J. Subst. Use 2005, 10, 191–197. [Google Scholar] [CrossRef]
- Szabo, A. Addiction to Exercise: A Symptom or a Disorder? Nova Science Publishers: New York, NY, USA, 2010. [Google Scholar]
- Adams, J.; Kirkby, R.J. Excessive exercise as an addiction: A review. Addict. Res. Theory 2002, 10, 415–437. [Google Scholar] [CrossRef]
- Landolfi, E. Exercise addiction. Sports Med. 2013, 43, 111–119. [Google Scholar] [CrossRef]
- Nogueira, A.; Molinero, O.; Salguero, A.; Márquez, S. Exercise addiction in practitioners of endurance sports: A literature review. Front. Psychol. 2018, 9, 1484. [Google Scholar] [CrossRef] [PubMed]
- Caudwell, K.M.; Mullan, B.A.; Hagger, M.S. Combining motivational and volitional approaches to reducing excessive alcohol consumption in pre-drinkers: A theory-based intervention protocol. BMC Public Health 2016, 16, 45. [Google Scholar] [CrossRef] [PubMed]
- Tangney, J.P.; Baumeister, R.F.; Boone, A.L. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J. Pers. 2004, 72, 271–324. [Google Scholar] [CrossRef]
- Brailovskaia, J.; Rohmann, E.; Bierhoff, H.W.; Schillack, H.; Margraf, J. The relationship between daily stress, social support and Facebook Addiction Disorder. Psychiatry Res. 2019, 276, 167–174. [Google Scholar] [CrossRef]
- Sheldon, K.M.; Elliot, A.J. Goal striving, need satisfaction, and longitudinal well-being: The self-concordance model. J. Pers. Soc. Psychol. 1999, 76, 482. [Google Scholar] [CrossRef] [PubMed]
- Koestner, R.; Lekes, N.; Powers, T.A.; Chicoine, E. Attaining personal goals: Self-concordance plus implementation intentions equals success. J. Pers. Soc. Psychol. 2002, 83, 231. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Overview of self-determination theory: An organismic dialectical perspective. In Handbook of Self-Determination Research; Deci, E.L., Ryan, R.M., Eds.; University of Rochester: Rochester, NY, USA, 2002; pp. 3–33. [Google Scholar]
- Cox, W.M.; Klinger, E. Motivational structure: Relationships with substance use and processes of change. Addict. Behav. 2002, 27, 925–940. [Google Scholar] [CrossRef]
- Heckhausen, J.; Heckhausen, H. Motivation and Action; Cambridge University Press: New York, NY, USA, 2008; Volume 2. [Google Scholar]
- Baumeister, R.F.; Bratslavsky, E.; Muraven, M.; Tice, D.M. Ego depletion: Is the active self a limited resource? J. Pers. Soc. Psychol. 1998, 74, 1252. [Google Scholar] [CrossRef]
- De Ridder, D.T.D.; Lensvelt-Mulders, G.; Finkenauer, C.; Stok, F.M.; Baumeister, R.F. Taking stock of self-control: A meta-analysis of how trait self-control relates to a wide range of behaviors. Pers. Soc. Psychol. Rev. 2012, 16, 76–99. [Google Scholar] [CrossRef]
- Hoyle, R.H.; Davisson, E.K. Varieties of self-control and their personality correlates. In Handbook of Self-Regulation: Research, Theory, and Applications; Vohs, K.D., Baumeister, R.F., Eds.; The Guilford Press: New York, NY, USA, 2016; pp. 396–413. [Google Scholar]
- Duckworth, A.L.; Seligman, M.E.P. Self-discipline outdoes IQ in predicting academic performance of adolescents. Psychol. Sci. 2005, 16, 939–944. [Google Scholar] [CrossRef] [PubMed]
- Gottfredson, M.R.; Hirschi, T. A General Theory of Crime; Stanford University Press: Redwood City, CA, USA, 1990. [Google Scholar]
- Hagger, M.S.; Wood, C.W.; Stiff, C.; Chatzisarantis, N.L. Self-regulation and self-control in exercise: The strength-energy model. Int. Rev. Sport Exerc. Psychol. 2010, 3, 62–86. [Google Scholar] [CrossRef]
- Hofmann, W.; Friese, M.; Roefs, A. Three ways to resist temptation: The independent contributions of executive attention, inhibitory control, and affect regulation to the impulse control of eating behavior. J. Exp. Soc. Psychol. 2009, 45, 431–435. [Google Scholar] [CrossRef]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.L.; Houts, R.; Poulton, R.; Roberts, B.W.; Ross, S.; et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. USA 2011, 108, 2693–2698. [Google Scholar] [CrossRef]
- Zhao, J.; Meng, G.; Sun, Y.; Xu, Y.; Geng, J.; Han, L. The relationship between self-control and procrastination based on the self-regulation theory perspective: The moderated mediation model. Curr. Psychol. 2019, 1–11. [Google Scholar] [CrossRef]
- Wills, T.A.; DuHamel, K.; Vaccaro, D. Activity and mood temperament as predictors of adolescent substance abuse; Test of a self-regulation mediational model. J. Pers. Soc. Psycol. 1995, 68, 901–916. [Google Scholar] [CrossRef]
- Vohs, K.D.; Faber, R.J. Spent resources: Self-regulatory resource availability affects impulse buying. J. Consum. Res. 2007, 3, 537–547. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Stokes, J.P. The process and mechanism of social support. In The Handbook of Research in Personal Relationships; Duck, S.W., Ed.; Wiley: London, UK, 1998; pp. 497–517. [Google Scholar]
- Holt, N.L.; Hoar, S.D. The multidimensional construct of social support. In Literature Reviews in Sport Psychology; Hanton, S., Mellalieu, S.D., Eds.; Nova: New York, NY, USA, 2006; pp. 199–225. [Google Scholar]
- Sarason, I.G.; Sarason, B.R.; Shearin, E.N. Social support as an individual difference variable: Its stability, origins, and relational aspects. J. Pers. Soc. Psychol. 1986, 50, 845. [Google Scholar] [CrossRef]
- Berkman, L.F.; Glass, T. Social integration, social networks, social support, and health. Soc. Epidemiol. 2000, 1, 137–173. [Google Scholar]
- Ditzen, B.; Heinrichs, M. Psychobiology of social support: The social dimension of stress buffering. Restor. Neurol. Neurosci. 2014, 32, 149–162. [Google Scholar] [CrossRef]
- Pressman, S.D.; Cohen, S. Does positive affect influence health? Psychol. Bull. 2005, 131, 925. [Google Scholar] [CrossRef]
- Uchino, B.N. Social Support and Physical Health: Understanding the Health Consequences of Relationships; Yale University Press: New Haven, CT, USA, 2004. [Google Scholar]
- Brummett, B.H.; Barefoot, J.C.; Siegler, I.C.; Clapp-Channing, N.E.; Lytle, B.L.; Bosworth, H.B.; Williams, R.B., Jr.; Mark, D.B. Characteristics of socially isolated patients with coronary artery disease who are at elevated risk for mortality. Psychosom. Med. 2001, 63, 267–272. [Google Scholar] [CrossRef]
- Rutledge, T.; Reis, S.E.; Olson, M.; Owens, J.; Kelsey, S.F.; Pepine, C.J.; Mankad, S.; Rogers, W.J.; Merz, C.N.B.; Sopko, G.; et al. Social networks are associated with lower mortality rates among women with suspected coronary disease: The National Heart, Lung, and Blood Institute-Sponsored Women’s Ischemia Syndrome Evaluation study. Psychosom. Med. 2004, 66, 882–888. [Google Scholar] [CrossRef]
- Kulik, J.A.; Mahler, H.I. Social support and recovery from surgery. Health Psychol. 1989, 8, 221. [Google Scholar] [CrossRef]
- Bianco, T.; Eklund, R.C. Conceptual considerations for social support research in sport and exercise settings: The case of sport injury. J. Sport Exerc. Psychol. 2001, 23, 85–107. [Google Scholar] [CrossRef]
- DiMatteo, M.R. Social support and patient adherence to medical treatment: A meta-analysis. Health Psychol. 2004, 23, 207. [Google Scholar] [CrossRef]
- Martire, L.M.; Schulz, R. Involving family in psychosocial interventions for chronic illness. Curr. Dir. Psychol. Sci. 2007, 16, 90–94. [Google Scholar] [CrossRef]
- DeFreese, J.D.; Smith, A.L. Athlete social support, negative social interactions and psychological health across a competitive sport season. J. Sport Exerc. Psychol. 2014, 36, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.H. A meta-analysis of the relationship between social support and well-being. Kaohsiung J. Med. Sci. 1998, 14, 717–726. [Google Scholar]
- Havassy, B.E.; Hall, S.M.; Wasserman, D.A. Social support and relapse: Commonalities among alcoholics, opiate users, and cigarette smokers. Addict. Behav. 1991, 16, 235–246. [Google Scholar] [CrossRef]
- Thomas, A.C.; Allen, F.L.; Phillips, J.; Karantzas, G. Gaming machine addiction: The role of avoidance, accessibility and social support. Psychol. Addict. Behav. 2011, 25, 738. [Google Scholar] [CrossRef] [PubMed]
- Lukacs, A.; Sasvári, P.; Varga, B.; Mayer, K. Exercise addiction and its related factors in amateur runners. J. Behav. Addict. 2019, 8, 343–349. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.; McCabe, M.P. Striving for success or addiction? Exercise dependence among elite Australian athletes. J. Sports Sci. 2012, 30, 755–766. [Google Scholar] [CrossRef]
- Di Lodovico, L.; Poulnais, S.; Gorwood, P. Which sports are more at risk of physical exercise addiction: A systematic review. Addict. Behav. 2019, 93, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Mayolas-Pi, C.; Simon-Grima, J.; Peñarrubia-Lozano, C.; Munguía-Izquierdo, D.; Moliner-Urdiales, D.; Legaz-Arrese, A. Exercise addiction risk and health in male and female amateur endurance cyclists. J. Behav. Addict. 2016, 6, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Schüler, J.; Knechtle, B.; Wegner, M. Antecedents of exercise dependence in ultra-endurance sports: Reduced basic need satisfaction and avoidance-motivated self-control. Front. Psychol. 2018, 9, 1275. [Google Scholar] [CrossRef] [PubMed]
- Schipfer, M.; Cook, B.; Stoll, O. OR-95: Examination of changes in exercise dependece symptoms in endurance athletes throughout a competition season. J. Behav. Addict. 2016, 5, 39. [Google Scholar]
- Hausenblas, H.A.; Downs, D.S. How much is too much? The development and validation of the exercise dependence scale. Psychol. Health 2002, 17, 387–404. [Google Scholar] [CrossRef]
- De Coverley Veale, D.M.E. Exercise dependence. Brit. J. Addict. 1987, 82, 735–740. [Google Scholar] [CrossRef]
- Schultz, U.; Schwarzer, R. Social support by coping with illness: The Berlin Social Support Scale (BSSS). Diagnostica 2003, 40, 73–82. [Google Scholar]
- Bertrams, A.; Unger, A.; Dickhäuser, O. Momentan verfügbare Selbstkontrollkraft—Vorstellung eines Messinstruments und erste Befunde aus pädagogisch-psychologischen Kontexten. [Momentarily available self-control strength—Introduction of a measure and first findings from educational-psychological contexts]. Z. Für Pädagogische Psychol. 2011, 25, 185–196. [Google Scholar]
- Seelig, H.; Fuchs, R. Messung der sport-und bewegungsbezogenen Selbstkonkordanz [Measurement of exercise-related self-concordance]. Z. Für Sportpsychol. 2006, 13, 121–139. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- JASP Team. JASP (Version 0.14.1) [Computer Software]; Department of Psychological Methods, University of Amsterdam: Amsterdam, The Netherlands, 2020. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Wickham, H. Ggplot2; Springer: New York, NY, USA, 2009. [Google Scholar]
- Dumitru, D.C.; Dumitru, T.; Maher, A.J. A systematic review of exercise addiction: Examining gender differences. J. Phys. Educ. Sport 2018, 18, 1738–1747. [Google Scholar]
- Wolff, W.; Martarelli, C.S. Bored into Depletion? Toward a Tentative Integration of Perceived Self-Control Exertion and Boredom as Guiding Signals for Goal-Directed Behavior. Perspect. Psychol. Sci. 2020, 15, 1272–1283. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.T.D.; Kroese, F.; Gillebaart, M. Whatever happened to self-control? A proposal for integrating notions from trait self-control studies into state self-control research. Motiv. Sci. 2018, 4, 39. [Google Scholar] [CrossRef]
- Hofmann, W.; Baumeister, R.F.; Förster, G.; Vohs, K.D. Everyday temptations: An experience sampling study of desire, conflict, and self-control. J. Pers. Soc. Psychol. 2012, 102, 1318. [Google Scholar] [CrossRef]
- Duckworth, A.L.; Gendler, T.S.; Gross, J.J. Situational Strategies for Self-Control. Perspect. Psychol. Sci. 2016, 11, 35–55. [Google Scholar] [CrossRef] [PubMed]
- Ent, M.R.; Baumeister, R.F.; Tice, D.M. Trait self-control and the avoidance of temptation. Pers. Individ. Differ. 2015, 74, 12–15. [Google Scholar] [CrossRef]
- Gillebaart, M.; de Ridder, D.T.D. Effortless self-control: A novel perspective on response conflict strategies in trait self-control. Soc. Personal. Psychol. Compass 2015, 9, 88–99. [Google Scholar] [CrossRef]
- Hale, B.D.; Diehl, D.; Weaver, K.; Briggs, M. Exercise dependence and muscle dysmorphia in novice and experienced female bodybuilders. J. Behav. Addict. 2013, 2, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.J.; Mesagno, C. Personality traits and exercise dependence: Exploring the role of narcissism and perfectionism. Int. J. Sport Exerc. Psychol. 2014, 12, 368–381. [Google Scholar] [CrossRef]
- Weik, M.; Hale, B.D. Contrasting gender differences on two measures of exercise dependence. Br. J. Sports Med. 2009, 43, 204–207. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Karr, T.M.; Zunker, C.; Thompson, R.A.; Sherman, R.T.; Erickson, A.; Cao, L.; Crosby, R.D.; Mitchell, J.E. Moderators of the association between exercise identity and obligatory exercise among participants of an athletic event. Body Image 2013, 10, 70–77. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zarauz-Sancho, A.; Ruiz-Juan, F.; Flores-Allende, G.; Arufe Giráldez, V. Predictor variables of the perception of success: Differential aspects in route runners. Rev. Int. Med. Cienc. Act. Física Del Deporte 2016, 16, 601–615. [Google Scholar]
- Sheldon, K.M. Becoming Oneself: The Central Role of Self-Concordant Goal Selection. Pers. Soc. Psychol. Rev. 2014, 18, 349–365. [Google Scholar] [CrossRef]
- Weinberg, R.S.; Gould, D. Foundations of Sport and Exercise Psychology; Human Kinetics: Champaign, IL, USA, 2014. [Google Scholar]
- Friese, M.; Frankenbach, J.; Job, V.; Loschelder, D.D. Does Self-Control Training Improve Self-Control? A Meta-Analysis. Perspect. Psychol. Sci. 2017, 12, 1077–1099. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Vohs, K.D.; Tice, D.M. The strength model of self-control. Curr. Dir. Psychol. Sci. 2007, 16, 351–355. [Google Scholar] [CrossRef]
- Miles, E.; Sheeran, P.; Baird, H.; Macdonald, I.; Webb, T.L.; Harris, P.R. Does self-control improve with practice? Evidence from a six-week training program. J. Exp. Psychol. Gen. 2016, 145, 1075–1091. [Google Scholar] [CrossRef] [PubMed]
- Muraven, M.; Baumeister, R.F. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol. Bull. 2000, 126, 247–259. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (N = 140) | Male (n = 82) | Female (n = 58) | t/U | p | |
|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | |||
| Exercise dependence | 2.98 (0.70) | 2.94 (0.73) | 3.04 (0.65) | −0.85 | 0.395 |
| Self-control (trait) | 3.52 (0.54) | 3.49 (0.58) | 3.56 (0.47) | −0.76 | 0.446 |
| Self-concordance * | 3.16 (0.98) | 3.15 (0.92) | 3.17 (1.08) | 2311.50 | 0.780 |
| Self-control (state) * | 5.13 (1.03) | 5.27 (1.00) | 4.92 (1.04) | 2842.00 | 0.050 |
| Perceived support * | 3.61 (0.51) | 3.56 (0.55) | 3.69 (0.45) | 1986.00 | 0.087 |
| Received support * | 3.33 (0.54) | 3.28 (0.57) | 3.39 (0.50) | 2117.50 | 0.271 |
| Workload * | 512.16 (305.88) | 549.54 (320.39) | 459.48 (278.30) | 2814.50 | 0.065 |
| Variables | EDS | SCT | SSC | SCS | PER | REC | WKL |
|---|---|---|---|---|---|---|---|
| Exercise dependence—EDS | 1 | ||||||
| Self-control (trait)—SCT | −0.26 ** | 1 | |||||
| Self-concordance—SSC | −0.23 ** | 0.36 *** | 1 | ||||
| Self-control (state)—SCS | −0.39 *** | 0.49 *** | 0.53 *** | 1 | |||
| Perceived support—PER | −0.10 | 0.21 * | 0.21 * | 0.29 *** | 1 | ||
| Received support—REC | 0.01 | 0.18 * | 0.18 * | 0.14 | 0.52 *** | 1 | |
| Workload—WKL | 0.31 *** | 0.10 | 0.05 | 0.06 | −0.01 | 0.12 | 1 |
| Mean | 3.01 | 3.50 | 3.08 | 5.09 | 3.59 | 3.32 | 526.28 |
| SD | 0.70 | 0.55 | 1.04 | 1.03 | 0.54 | 0.54 | 334.11 |
| Range | 1–7 | 1–5 | −6–6 | 1–7 | 1–4 | 1–4 | 90–1800 |
| Variable | Model 1 | Model 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| b | SE b | β | p | 95% CI | b | SE b | β | p | 95% CI | |
| Intercept | 4.14 | 0.38 | 0.001 | 4.52 | 0.38 | 0.001 | ||||
| Self-concordance | −0.12 | 0.06 | −0.16 | 0.066 | [−0.241, 0.008] | −0.02 | 0.07 | −0.03 | 0.751 | [−0.151, 0.109] |
| Trait self-control | −0.23 | 0.12 | −0.18 | 0.052 | [−0.453, 0.002] | −0.07 | 0.12 | −0.05 | 0.556 | [−0.305, 0.165] |
| State self-control | −0.24 | 0.07 | −0.35 | 0.001 | [−0.371, −0.108] | |||||
| R2 | 0.08 | 0.16 | ||||||||
| Adj. R2 | 0.07 | 0.14 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimanyi, Z.; Wolff, W.; Schüler, J. Too Much of a Good Thing? Exercise Dependence in Endurance Athletes: Relationships with Personal and Social Resources. Int. J. Environ. Res. Public Health 2021, 18, 2966. https://doi.org/10.3390/ijerph18062966
Zimanyi Z, Wolff W, Schüler J. Too Much of a Good Thing? Exercise Dependence in Endurance Athletes: Relationships with Personal and Social Resources. International Journal of Environmental Research and Public Health. 2021; 18(6):2966. https://doi.org/10.3390/ijerph18062966
Chicago/Turabian StyleZimanyi, Zsuzsanna, Wanja Wolff, and Julia Schüler. 2021. "Too Much of a Good Thing? Exercise Dependence in Endurance Athletes: Relationships with Personal and Social Resources" International Journal of Environmental Research and Public Health 18, no. 6: 2966. https://doi.org/10.3390/ijerph18062966
APA StyleZimanyi, Z., Wolff, W., & Schüler, J. (2021). Too Much of a Good Thing? Exercise Dependence in Endurance Athletes: Relationships with Personal and Social Resources. International Journal of Environmental Research and Public Health, 18(6), 2966. https://doi.org/10.3390/ijerph18062966