
Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19)



Abstract
1. Overview
2. Detection of Malnutrition in COVID-19 Patients Is a Challenge
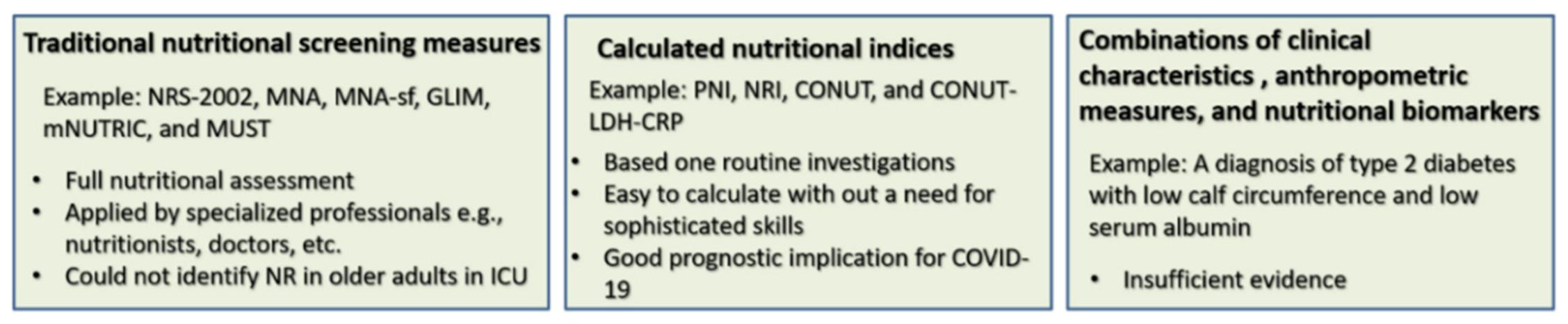
3. Measures Used for Nutritional Screening in COVID-19 Patients
4. Critical Risk Factors for Malnutrition in COVID-19
5. Identifying Malnutrition in the General Public during COVID-19 Outbreak Is a Necessity
6. Current Knowledge on the Management of Malnutrition in COVID-19
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APACHE II | Acute Physiology and Chronic Health Evaluation II |
| ARDS | Severe acute pneumonia-associated respiratory syndrome |
| AST | Aspartate aminotransferase |
| AUC | Area under the ROC curve |
| BMI | Body mass index |
| COVID-19 | Coronavirus disease 2019 |
| CK | Creatine kinase |
| CONUT | The controlling nutritional status score |
| CRP | C-reactive protein |
| GI | Gastrointestinal |
| GLIM | Global Leadership Initiative on Malnutrition |
| ICU | Intensive care unit |
| IL | Interleukin |
| LDH | Lactate dehydrogenase |
| LOS | Length of stay |
| MNA | Mini Nutritional Assessment |
| MNA-sf | MNA-short form |
| mNUTRIC | Modified Nutrition Risk in the Critically ill |
| MUST | Malnutrition Universal Screening Tool |
| NR | Nutrition risk |
| NRI | Nutritional Risk Index |
| NRS-2002 | Nutrition Risk Screening 2002 |
| SARS-CoV-2 | Severe acute respiratory syndrome-coronavirus-2 |
| SGA | Subjective Global Assessment |
| SOFA | Sequential Organ Failure Assessment |
References
- Goyal, B.; Goyal, D. Targeting the Dimerization of the Main Protease of Coronaviruses: A Potential Broad-Spectrum Therapeutic Strategy. ACS Comb. Sci. 2020, 22, 297–305. [Google Scholar] [CrossRef]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Propolis, bee honey, and their components protect against coronavirus disease 2019 (Covid-19): A review of in silico, in vitro, and clinical studies. Molecules 2021, 26, 1232. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Taneri, P.E.; Gómez-Ochoa, S.A.; Llanaj, E.; Raguindin, P.F.; Rojas, L.Z.; Roa-Díaz, Z.M.; Salvador, D., Jr.; Groothof, D.; Minder, B.; Kopp-Heim, D.; et al. Anemia and iron metabolism in COVID-19: A systematic review and meta-analysis. Eur. J. Epidemiol. 2020, 35, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef]
- Ikewaki, N.; Rao, K.-S.; Archibold, A.D.; Iwasaki, M.; Senthilkumar, R.; Preethy, S.; Katoh, S.; Abraham, S.J.K. Coagulopathy associated with COVID-19—Perspectives & Preventive strategies using a biological response modifier Glucan. Thromb. J. 2020, 18, 27. [Google Scholar] [CrossRef]
- De Biasi, S.; Meschiari, M.; Gibellini, L.; Bellinazzi, C.; Borella, R.; Fidanza, L.; Gozzi, L.; Iannone, A.; Lo Tartaro, D.; Mattioli, M.; et al. Marked T cell activation, senescence, exhaustion and skewing towards TH17 in patients with COVID-19 pneumonia. Nat. Commun. 2020, 11, 3434. [Google Scholar] [CrossRef] [PubMed]
- Codo, A.C.; Davanzo, G.G.; Monteiro, L.B.; de Souza, G.F.; Muraro, S.P.; Virgilio-da-Silva, J.V.; Prodonoff, J.S.; Carregari, V.C.; de Biagi Junior, C.A.O.; Crunfli, F.; et al. Elevated Glucose Levels Favor SARS-CoV-2 Infection and Monocyte Response through a HIF-1α/Glycolysis-Dependent Axis. Cell Metab. 2020, 32, 437–446.e435. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Apitherapy for age-related skeletal muscle dysfunction (sarcopenia): A review on the effects of royal jelly, propolis, and bee pollen. Foods 2020, 9, E1362. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Intermittent fasting, dietary modifications, and exercise for the control of gestational diabetes and maternal mood dysregulation: A review and a case report. Int. J. Environ. Res. Public Health 2020, 17, 9379. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Corona Virus Disease 2019 (COVID-19): A pandemic that threatens physical and mental health by promoting physical inactivity. Sports Med. Health Sci. 2020, 2, 221–223. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Fu, B.; Zheng, X.; Wang, D.; Zhao, C.; Qi, Y.; Sun, R.; Tian, Z.; Xu, X.; Wei, H. Pathogenic T-cells and inflammatory monocytes incite inflammatory storms in severe COVID-19 patients. Natl. Sci. Rev. 2020, 7, 998–1002. [Google Scholar] [CrossRef]
- Wen, W.; Su, W.; Tang, H.; Le, W.; Zhang, X.; Zheng, Y.; Liu, X.; Xie, L.; Li, J.; Ye, J.; et al. Immune cell profiling of COVID-19 patients in the recovery stage by single-cell sequencing. Cell Discov. 2020, 6, 31. [Google Scholar] [CrossRef]
- Diao, B.; Wang, C.; Tan, Y.; Chen, X.; Liu, Y.; Ning, L.; Chen, L.; Li, M.; Liu, Y.; Wang, G.; et al. Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Front. Immunol. 2020, 11, 827. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, S.; Das, J.K.; Ismail, T.; Wahid, M.; Saeed, W.; Bhutta, Z.A. Nutritional perspectives for the prevention and mitigation of COVID-19. Nutr. Rev. 2020. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Bee honey protects astrocytes against oxidative stress: A preliminary in vitro investigation. Neuropsychopharmacol. Rep. 2019, 39, 312–314. [Google Scholar] [CrossRef]
- Kunugi, H.; Ali, A.M. Royal Jelly and Its Components Promote Healthy Aging and Longevity: From Animal Models to Humans. Int. J. Mol. Sci. 2019, 20, 4662. [Google Scholar] [CrossRef]
- Manzanares, W.; Moreira, E.; Hardy, G. Pharmaconutrition revisited for critically ill patients with coronavirus disease 2019 (COVID-19): Does selenium have a place? Nutrition 2021, 81, 110989. [Google Scholar] [CrossRef]
- Majeed, M.; Nagabhushanam, K.; Gowda, S.; Mundkur, L. An exploratory study of selenium status in healthy individuals and in patients with COVID-19 in a south Indian population: The case for adequate selenium status. Nutrition 2020, 82, 111053. [Google Scholar] [CrossRef]
- Im, J.H.; Je, Y.S.; Baek, J.; Chung, M.-H.; Kwon, H.Y.; Lee, J.-S. Nutritional status of patients with COVID-19. Int. J. Infect. Dis. 2020, 100, 390–393. [Google Scholar] [CrossRef]
- Huang, W.; Li, C.; Wang, Z.; Wang, H.; Zhou, N.; Jiang, J.; Ni, L.; Zhang, X.A.; Wang, D.-W. Decreased serum albumin level indicates poor prognosis of COVID-19 patients: Hepatic injury analysis from 2623 hospitalized cases. Sci. China Life Sci. 2020, 63, 1678–1687. [Google Scholar] [CrossRef]
- Das, A.; Das, M.; Ghosh, S. Impact of nutritional status and anemia on COVID-19: Is it a public health concern? Evidence from National Family Health Survey-4 (2015–2016), India. Public Health 2020, 185, 93–94. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.; Xu, J.; Chen, W.; Yang, Z.; Xu, X.; Liu, L.; Chen, R.; Xie, J.; Liu, M.; Wu, J.; et al. Anemia is associated with severe illness in COVID-19: A retrospective cohort study. J. Med. Virol. 2021, 93, 1478–1488. [Google Scholar] [CrossRef] [PubMed]
- Benoit, J.L.; Benoit, S.W.; de Oliveira, M.H.S.; Lippi, G.; Henry, B.M. Anemia and COVID-19: A prospective perspective. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Li, Y.; Ge, Y.; Shi, Y.; Lv, P.; Zhang, J.; Fu, G.; Zhou, Y.; Jiang, K.; Lin, N.; et al. Evaluation of Nutrition Risk and Its Association With Mortality Risk in Severely and Critically Ill COVID-19 Patients. JPEN J. Parenter. Enter. Nutr. 2020, 45, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Ahmed, A.H.; Smail, L. Psychological Climacteric Symptoms and Attitudes toward Menopause among Emirati Women. Int. J. Environ. Res. Public Health 2020, 17, 5028. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Apitherapy for Parkinson’s disease: A focus on the effects of propolis and royal jelly. Oxid Med. Cell Longev. 2020, 1727142. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Royal jelly as an intelligent anti-aging—a focus on cognitive aging and Alzheimer’s disease: A review. Antioxidants 2020, 9, 937. [Google Scholar] [CrossRef] [PubMed]
- Fishbane, S.; Hirsch, J.S. Erythropoiesis-Stimulating Agent Treatment in Patients With COVID-19. AJKDD 2020, 76, 303–305. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.; Hu, L.; Wang, Y.; Huang, L.; Zhao, L.; Zhang, C.; Liu, X.; Xu, R.; Liu, F.; Li, J.; et al. Diagnostic performance of initial blood urea nitrogen combined with D-dimer levels for predicting in-hospital mortality in COVID-19 patients. Int. J. Antimicrob. Agents 2020, 56, 106110. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, S.; Mao, Z.; Wang, W.; Hu, H. Clinical significance of nutritional risk screening for older adult patients with COVID-19. Eur. J. Clin. Nutr. 2020, 74, 876–883. [Google Scholar] [CrossRef]
- Zhong, H.; Wang, Y.; Zhang, Z.L.; Liu, Y.X.; Le, K.J.; Cui, M.; Yu, Y.T.; Gu, Z.C.; Gao, Y.; Lin, H.W. Efficacy and safety of current therapeutic options for COVID-19—Lessons to be learnt from SARS and MERS epidemic: A systematic review and meta-analysis. Pharmacol. Res. 2020, 157, 104872. [Google Scholar] [CrossRef]
- Bellmann-Weiler, R.; Lanser, L.; Barket, R.; Rangger, L.; Schapfl, A.; Schaber, M.; Fritsche, G.; Wöll, E.; Weiss, G. Prevalence and Predictive Value of Anemia and Dysregulated Iron Homeostasis in Patients with COVID-19 Infection. J. Clin. Med. 2020, 9, 2429. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Hypoproteinemia predicts disease severity and mortality in COVID-19: A call for action. Diagn. Pathol. 2021. under review. [Google Scholar]
- Piano, S.; Dalbeni, A.; Vettore, E.; Benfaremo, D.; Mattioli, M.; Gambino, C.G.; Framba, V.; Cerruti, L.; Mantovani, A.; Martini, A.; et al. Abnormal liver function tests predict transfer to intensive care unit and death in COVID-19. Liver Int. 2020, 40, 2394–2406. [Google Scholar] [CrossRef]
- Gualtieri, P.; Falcone, C.; Romano, L.; Macheda, S.; Correale, P.; Arciello, P.; Polimeni, N.; Lorenzo, A. Body Composition Findings by Computed Tomography in SARS-CoV-2 Patients: Increased Risk of Muscle Wasting in Obesity. Int. J. Mol. Sci. 2020, 21, 4670. [Google Scholar] [CrossRef] [PubMed]
- Zeppa, S.D.; Agostini, D.; Piccoli, G.; Stocchi, V.; Sestili, P. Gut Microbiota Status in COVID-19: An Unrecognized Player? Front. Cell. Infect. Microbiol. 2020, 10, 576551. [Google Scholar] [CrossRef]
- Wei, C.; Liu, Y.; Li, Y.; Zhang, Y.; Zhong, M.; Meng, X. Evaluation of the nutritional status in patients with COVID-19. J. Clin. Biochem. Nutr. 2020, 67, 116–121. [Google Scholar] [CrossRef]
- Silva, D.F.O.; Lima, S.; Sena-Evangelista, K.C.M.; Marchioni, D.M.; Cobucci, R.N.; Andrade, F.B. Nutritional Risk Screening Tools for Older Adults with COVID-19: A Systematic Review. Nutrients 2020, 12, 2956. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; He, Z.; Yu, G.; Peng, D.; Feng, Y.; Ling, J.; Wang, Y.; Li, S.; Bian, Y. The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patients. Clin. Nutr. 2020, 40, 534–541. [Google Scholar] [CrossRef]
- Bellanti, F.; Lo Buglio, A.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. 2020, 9, 1898. [Google Scholar] [CrossRef]
- Wang, R.; He, M.; Yue, J.; Bai, L.; Liu, D.; Huang, Z.; Zhu, T.; Kang, Y. CONUT score is associated with mortality in patients with COVID-19: A retrospective study in Wuhan. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Baron, D.M.; Franchini, M.; Goobie, S.M.; Javidroozi, M.; Klein, A.A.; Lasocki, S.; Liumbruno, G.M.; Muñoz, M.; Shander, A.; Spahn, D.R.; et al. Patient blood management during the COVID–19 pandemic: A narrative review. Anaesthesia 2020, 75, 1105–1113. [Google Scholar] [CrossRef]
- Zhou, J.; Ma, Y.; Liu, Y.; Xiang, Y.; Tao, C.; Yu, H.; Huang, J. A Correlation Analysis Between the Nutritional Status and Prognosis of COVID-19 Patients. J. Nutr. Health Aging 2020, 25, 84–93. [Google Scholar] [CrossRef]
- Li, T.; Zhang, Y.; Gong, C.; Wang, J.; Liu, B.; Shi, L.; Duan, J. Prevalence of malnutrition and analysis of related factors in elderly patients with COVID-19 in Wuhan, China. Eur. J. Clin. Nutr. 2020, 74, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Reckman, G.A.R.; Gomes-Neto, A.W.; Vonk, R.J.; Ottery, F.D.; Schans, C.P.v.d.; Navis, G.J.; Jager-Wittenaar, H. Anabolic competence: Assessment and integration of the multimodality interventional approach in disease-related malnutrition. Nutrition 2019, 65, 179–184. [Google Scholar] [CrossRef]
- De Lorenzo, R.; Conte, C.; Lanzani, C.; Benedetti, F.; Roveri, L.; Mazza, M.G.; Brioni, E.; Giacalone, G.; Canti, V.; Sofia, V.; et al. Residual clinical damage after COVID-19: A retrospective and prospective observational cohort study. PLoS ONE 2020, 15, e0239570. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; De Lorenzo, R.; D’Amico, M.; Sofia, V.; Roveri, L.; Mele, R.; Saibene, A.; Rovere-Querini, P.; Conte, C. COVID-19 is associated with clinically significant weight loss and risk of malnutrition, independent of hospitalisation: A post-hoc analysis of a prospective cohort study. Clin. Nutr. 2020. [Google Scholar] [CrossRef]
- Haraj, N.E.; El Aziz, S.; Chadli, A.; Dafir, A.; Mjabber, A.; Aissaoui, O.; Barrou, L.; El Kettani El Hamidi, C.; Nsiri, A.; Al Harrar, R.; et al. Nutritional status assessment in patients with Covid-19 after discharge from the intensive care unit. Clin. Nutr. ESPEN 2021, 41, 423–428. [Google Scholar] [CrossRef]
- Bedock, D.; Bel Lassen, P.; Mathian, A.; Moreau, P.; Couffignal, J.; Ciangura, C.; Poitou-Bernert, C.; Jeannin, A.-C.; Mosbah, H.; Fadlallah, J.; et al. Prevalence and severity of malnutrition in hospitalized COVID-19 patients. Clin. Nutr. ESPEN 2020, 40, 214–219. [Google Scholar] [CrossRef]
- Du, X.; Liu, Y.; Chen, J.; Peng, L.; Jin, Y.; Cheng, Z.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Comparison of the Clinical Implications among Two Different Nutritional Indices in Hospitalized Patients with COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Song, F.; Ma, H.; Wang, S.; Qin, T.; Xu, Q.; Yuan, H.; Li, F.; Wang, Z.; Liao, Y.; Tan, X.; et al. Nutritional screening based on objective indices at admission predicts in-hospital mortality in patients with COVID-19. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Allard, L.; Ouedraogo, E.; Molleville, J.; Bihan, H.; Giroux-Leprieur, B.; Sutton, A.; Baudry, C.; Josse, C.; Didier, M.; Deutsch, D.; et al. Malnutrition: Percentage and Association with Prognosis in Patients Hospitalized for Coronavirus Disease 2019. Nutrients 2020, 12, 3679. [Google Scholar] [CrossRef]
- Gao, Y.-d.; Ding, M.; Dong, X.; Zhang, J.-j.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.-l.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Aloisio, E.; Chibireva, M.; Serafini, L.; Pasqualetti, S.; Falvella, F.S.; Dolci, A.; Panteghini, M. A Comprehensive Appraisal of Laboratory Biochemistry Tests as Major Predictors of COVID-19 Severity. Arch. Pathol. Lab. Med. 2020, 144, 1457–1464. [Google Scholar] [CrossRef]
- Lin, L.; Hu, K.; Cai, S.; Deng, X.; Shao, X.; Liang, Y.; Wang, J.; Zhong, T.; Hu, Z.; Lei, M. Hypoproteinemia is an independent risk factor for the prognosis of severe COVID-19 patients. J. Clin. Biochem. Nutr. 2020, 20–75. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Age-related skeletal muscle failure (sarcopenia)—a detrimental challenge during the Coronavirus Disease 2019 (COVID-19) era. Oxid. Med. Cell. Longev. 2021. under review. [Google Scholar]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Skeletal muscle damage in COVID-19: A call for action. Medicina 2021. under review. [Google Scholar]
- Chapple, L.A.; Fetterplace, K.; Asrani, V.; Burrell, A.; Cheng, A.C.; Collins, P.; Doola, R.E.; Ferrie, S.; Marshall, A.P.; Ridley, E.J. Nutrition management for critically and acutely unwell hospitalised patients with coronavirus disease 2019 (COVID-19) in Australia and New Zealand. Nutr. Diet. 2020, 77, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Barnett, J.; Brill, S.E.; Brown, J.S.; Denneny, E.K.; Hare, S.S.; Heightman, M.; Hillman, T.E.; Jacob, J.; Jarvis, H.C.; et al. ‘Long-COVID’: A cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 2020. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Girgis, C.M.; Cheung, N.W. COVID-19 and diabetes: Insulin requirements parallel illness severity in critically unwell patients. Clin. Endocrinol. 2020, 93, 390–393. [Google Scholar] [CrossRef]
- Lasbleiz, A.; Cariou, B.; Darmon, P.; Soghomonian, A.; Ancel, P.; Boullu, S.; Houssays, M.; Romain, F.; Lagier, J.C.; Boucekine, M.; et al. Phenotypic Characteristics and Development of a Hospitalization Prediction Risk Score for Outpatients with Diabetes and COVID-19: The DIABCOVID Study. J. Clin. Med. 2020, 9, 3726. [Google Scholar] [CrossRef] [PubMed]
- Cawood, A.L.; Walters, E.R.; Smith, T.R.; Sipaul, R.H.; Stratton, R.J. A Review of Nutrition Support Guidelines for Individuals with or Recovering from COVID-19 in the Community. Nutrients 2020, 12, 3230. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Keller, K. Sarcopenia. Wien. Med. Wochenschr. 2019, 169, 157–172. [Google Scholar] [CrossRef]
- Favaro-Moreira, N.C.; Krausch-Hofmann, S.; Matthys, C.; Vereecken, C.; Vanhauwaert, E.; Declercq, A.; Bekkering, G.E.; Duyck, J. Risk Factors for Malnutrition in Older Adults: A Systematic Review of the Literature Based on Longitudinal Data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef]
- Vandewoude, M.F.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef] [PubMed]
- Zhan, T.; Liu, M.; Tang, Y.; Han, Z.; Cheng, X.; Deng, J.; Chen, X.; Tian, X.; Huang, X. Retrospective analysis of clinical characteristics of 405 patients with COVID-19. J. Int. Med. Res. 2020, 48, 300060520949039. [Google Scholar] [CrossRef]
- Louca, P.; Murray, B.; Klaser, K.; Graham, M.S.; Mazidi, M.; Leeming, E.R.; Thompson, E.; Bowyer, R.; Drew, D.A.; Nguyen, L.H.; et al. Dietary supplements during the COVID-19 pandemic: Insights from 1.4 M users of the COVID Symptom Study app—A longitudinal app-based community survey. medRxiv 2020. [Google Scholar] [CrossRef]
- Azzolino, D.; Saporiti, E.; Proietti, M.; Cesari, M. Nutritional Considerations in Frail Older Patients with COVID-19. J. Nutr. Health Aging 2020, 24, 696–698. [Google Scholar] [CrossRef]
- Krznarić, Ž.; Bender, D.V.; Laviano, A.; Cuerda, C.; Landi, F.; Monteiro, R.; Pirlich, M.; Barazzoni, R. A simple remote nutritional screening tool and practical guidance for nutritional care in primary practice during the COVID-19 pandemic. Clin. Nutr. 2020, 39, 1983–1987. [Google Scholar] [CrossRef] [PubMed]
- Slullitel, P.A.; Lucero, C.M.; Soruco, M.L.; Barla, J.D.; Benchimol, J.A.; Boietti, B.R.; Zanotti, G.; Comba, F.; Taype-Zamboni, D.R.; Carabelli, G.S.; et al. Prolonged social lockdown during COVID-19 pandemic and hip fracture epidemiology. Int. Orthop. 2020, 1–9. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical Activity Changes and Its Risk Factors among Community-Dwelling Japanese Older Adults during the COVID-19 Epidemic: Associations with Subjective Well-Being and Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Yamada, M.; Kimura, Y.; Ishiyama, D.; Otobe, Y.; Suzuki, M.; Koyama, S.; Kikuchi, T.; Kusumi, H.; Arai, H. Effect of the COVID-19 Epidemic on Physical Activity in Community-Dwelling Older Adults in Japan: A Cross-Sectional Online Survey. J. Nutr. Health Aging 2020, 24, 948–950. [Google Scholar] [CrossRef]
- Ali, A.M.; Hendawy, A.O. Bee honey in combination with exercise—better physical performance and less fatigue for a more active lifestyle during the COVID-19 era. Sports Med. Health Sci. 2021. under review. [Google Scholar]
- Bellelli, G.; Rebora, P.; Valsecchi, M.G.; Bonfanti, P.; Citerio, G. Frailty index predicts poor outcome in COVID-19 patients. Intensive Care Med. 2020, 46, 1634–1636. [Google Scholar] [CrossRef]
- Hewitt, J.; Carter, B.; Vilches-Moraga, A.; Quinn, T.J.; Braude, P.; Verduri, A.; Pearce, L.; Stechman, M.; Short, R.; Price, A.; et al. The effect of frailty on survival in patients with COVID-19 (COPE): A multicentre, European, observational cohort study. Lancet Public Health 2020, 5, e444–e451. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Screening for sarcopenia (physical frailty) in the COVID-19 era. Int. J. Endocrinol. 2021. under review. [Google Scholar]
- Jeong, D.H.; Hong, S.B.; Lim, C.M.; Koh, Y.; Seo, J.; Kim, Y.; Min, J.Y.; Huh, J.W. Relationship between Nutrition Intake and 28-Day Mortality Using Modified NUTRIC Score in Patients with Sepsis. Nutrients 2019, 11, 1906. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Chittams, J.; Sammarco, T.; Higashibeppu, N.; Higashiguchi, T.; Heyland, D.K. Greater Nutrient Intake Is Associated With Lower Mortality in Western and Eastern Critically Ill Patients With Low BMI: A Multicenter, Multinational Observational Study. JPEN J. Parenter. Enter. Nutr. 2019, 43, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, B.; Calder, P.C.; Marino, L.V. Evaluation of implementation of fasting guidelines for enterally fed critical care patients. Clin. Nutr. 2019, 38, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hendawy, A.O. Vitamin K involvement in COVID-19 and possible benefits of vitamin K antagonists (VKA). Aging Clin. Exp. Res. 2021. under review. [Google Scholar]


{kind=link}
| Sample Size | Age (Years) | Male Gender | Nutritional Measure | COVID-19 Outcomes | Malnutrition Prevalence | Malnutrition Association with COVID-19 Outcomes | Ref. |
|---|---|---|---|---|---|---|---|
| 141 | 71.7 ± 5.9 | 48.2% | NRS-2002, MUST, MNA-sf, NRI | LOS, hospital expenses, appetite, disease severity, weight change | Malnutrition was identified by NRS-2002, MUST, MNA-sf, NRI in 85.8%, 41.1%, 77.3%, and 71.6% of patients, respectively. | Patients high on NRS 2002, MNA-sf, and NRI had significantly longer LOS, higher hospital expenses, poor appetite, disease severity, and more weight loss. | [34] |
| 136 | Median age = 69 (IQR: 57–77) | 63% | mNUTRIC | Mortality within 28 days of ICU admission | Malnutrition was identified in 61% of critically ill patients. | Compared with low NR patients, malnourished patients had higher mortality (87% vs. 49%, p < 0.001), the higher probability of death at ICU 28-day (adjusted HR = 2.01, 95% CI: 1.22–3.32, p = 0.006), higher incidence of ARDS, acute myocardial injury, secondary infection, shock, and use of vasopressors. | [43] |
| 114 | 59.9 ± 15.9 | 60.5% | GLIM | Clinical, radiological, and biological characteristics of COVID-19 patients | Moderate and severe malnutrition developed in 23.7%, and 18.4% in the whole sample, and in 66.7% of patients in the ICU. | GLIM correlated with lower albumin level and increased ICU admission regardless of age and CRP level. | [53] |
| 413 | 60.3 ± 12.7 | 51% | NRS-2002 | BMI, inflammatory and nutritional markers | Among all patients, severe, and critical patients, moderate malnutrition developed in 76%, 84%, and 38% of patients, respectively while severe malnutrition developed in 16%, 7%, and 62% of patients, respectively. | High NRS-2002 scores in critically ill patients correlated with inflammatory and nutrition-related markers, LOS, and a higher risk of mortality. | [28] |
| 182 | 68.5 ± 8.8 | 36% | MNA | Comorbidities, BMI, calf circumference, albumin, hemoglobin, and lymphocyte counts | Malnutrition and risk of malnutrition in developed in 52.7% and 27.5% of patients, respectively. | A score comprising a combination of diabetes mellitus, low calf circumference, and low albumin is an independent risk factor for malnutrition. | [48] |
| 348 | 66 (range = 56 to 73) | 52% | CONUT | Inflammation and malnutrition markers, mortality, muscle dystrophy | Mild and moderate-severe NR were identified in 46.3% and 39.9% of patients, respectively | Moderate-severe malnutrition correlated with age, inflammation and nutrition markers, the development of acute cardiac injury, and all-cause mortality. | [41] |
| 429 | 48.3% > 61 | 65.7% | CONUT | Clinical condition and COVID-19 adverse effects (ICU admission and all-cause death). | Malnutrition was identified in 65.7% of patients. | High CONUT score correlated with old age, diabetes, and hospital admission. Older adults with a high CONUT score had a 6.2 times higher risk of adverse outcomes. Gender, age, hypertension, and urinary erythrocytes were the key factors affecting adverse outcomes. High sensitivity and specificity of the CONUT on the ROC curve. | [47] |
| 295 | 58 (44–69) | 52.5% | GNRI, PNI, CONUT | Nutritional, inflammatory, and renal biomarkers, clinical data, and in-hospital death | Moderate and severe NR in critically ill patients were 10% and 30% on the PNI score and 34.6% and 30.8% on the CONUT score | Critically ill patients had significantly lower albumin levels and higher blood urea nitrogen and serum creatinine, CRP, IL6 than severe or mild/moderate patients (p < 0.0001). Baseline nutritional status correlated with in-hospital mortality. Good prognostic implication of GNRI and CONUT score on the ROC curve | [55] |
| 245 | Median age = 55 | 46.5% | PNI and CONUT | In-hospital mortality, clinical data, laboratory, and nutritional biomarkers. | Moderate and severe NR were identified in 12.7% and 12.2% on the PNI score and in 23.7% and 2.8% of patients on the CONUT score. | CONUT score (OR = 3.371,95% CI 1.124–10.106, p = 0.030) and PNI (OR = 0.721, 95% CI 0.581–0.896, p = 0.003) were independent predictors of all-cause death at an early stage. Higher PNI was an independent risk predictor of in-hospital death (OR = 24.225, 95% CI 2.147–273.327, p = 0.010). | [54] |
| 442 | 58 (41–70) | 46.6% | CONUT and NRS-2002 | In-hospital mortality, markers of inflammation, nutrition, renal, and liver function, COVID-19 complications | CONUT identified severe malnutrition in 7.6% of non-survivors. | In adjusted analysis, CONUT (p = 0.002), LDH (p < 0.001), CRP (p = 0.020) were risk factors of mortality in COVID-19 patients. Better prognostic potential of CONUT and combined CONUT-LDH-CRP than NRS-2002. | [45] |
| 108 | 62 ± 16 | 62.9% | NRI, BMI, 5% or 10% weight loss in the previous month or 6 months | Need for nasal oxygen, markers of inflammation, and nutrition. | NRI identified malnutrition and risk for malnutrition in 38.9% and 84.9% of patients. | NRI scores correlated with inflammation; lower plasma levels of proteins, albumin, prealbumin, and zinc, and the need for oxygen therapy. | [56] |
| 41 | 55 (19–85) | 51.2% | MNA | BMI, weight loss, anemia, and serum levels of Ca, Zn, Mg, albumin, and vitamin D. | MNA identified malnutrition and risk for malnutrition in 14.6% and 65.9% of ICU-discharged patients. | Weight loss in 61% (>10% of body weight in 26.2%) of patients. Hypoalbuminemia, hypoproteinemia, hypocalcemia, anemia, hypomagnesemia, and hypovitaminosis D were detected in 19.5%, 17.1%,19.5%, 34.1%, 12.2%, and 51.2% of patients, respectively. | [52] |
| 185 | 57 (48–67) | 65.5% | MNA | Need for follow-up due to dyspnea, tachypnea, new-onset cognitive impairment, and post-traumatic stress. | MNA identified malnutrition and risk for malnutrition in 5.4% and 57.3% of patients, 100 days following discharge from the hospital or ICU. | BMI and ≥33 Kg/m2, arterial oxygen partial pressure to fractional inspired oxygen ratio < 324, age > 63 years, diabetes, and non-invasive ventilation highly predicted the need for follow-up. | [50] |
| 213 | Median age = 59 (49.5–67.9) | 66% | MNA | Appetite, weight loss, and inflammation biomarkers. | MNA identified malnutrition and risk for malnutrition in 6.6% and 54.7% of remitting patients, following discharge from the hospital or treatment at home. | High risk of malnutrition among hospital and ICU admitted patients. Weight loss > 10% of initial body weight in hospitalized and home-treated patients (9.6% vs. 5.3%, p = 0.41) was associated with high CRP, renal injury, longer LOS, and disease duration independent of age, sex, pre-existing comorbidities, and most of the biochemical parameters upon admission. | [51] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, A.M.; Kunugi, H. Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19). Int. J. Environ. Res. Public Health 2021, 18, 2772. https://doi.org/10.3390/ijerph18052772
Ali AM, Kunugi H. Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19). International Journal of Environmental Research and Public Health. 2021; 18(5):2772. https://doi.org/10.3390/ijerph18052772
Chicago/Turabian StyleAli, Amira Mohammed, and Hiroshi Kunugi. 2021. "Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19)" International Journal of Environmental Research and Public Health 18, no. 5: 2772. https://doi.org/10.3390/ijerph18052772
APA StyleAli, A. M., & Kunugi, H. (2021). Approaches to Nutritional Screening in Patients with Coronavirus Disease 2019 (COVID-19). International Journal of Environmental Research and Public Health, 18(5), 2772. https://doi.org/10.3390/ijerph18052772