
Technical Accuracy of Dental Laboratories in the Quality and Shade Matching of Porcelain Fused to Metal Crowns: An In Vitro Study

 and
and
Abstract
1. Introduction
2. Materials and Methods
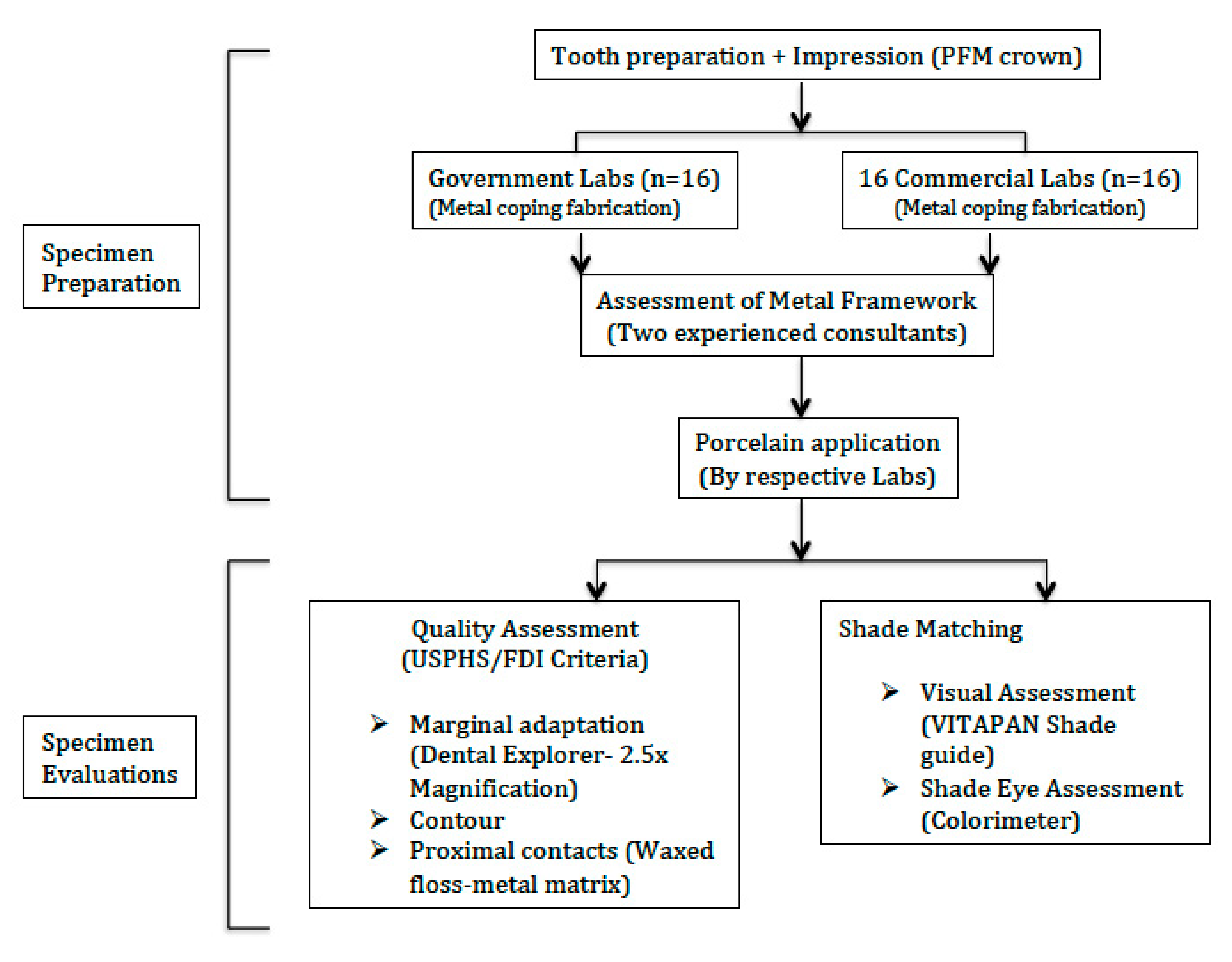
2.1. Specimen Preparation
2.2. Quality Evaluation
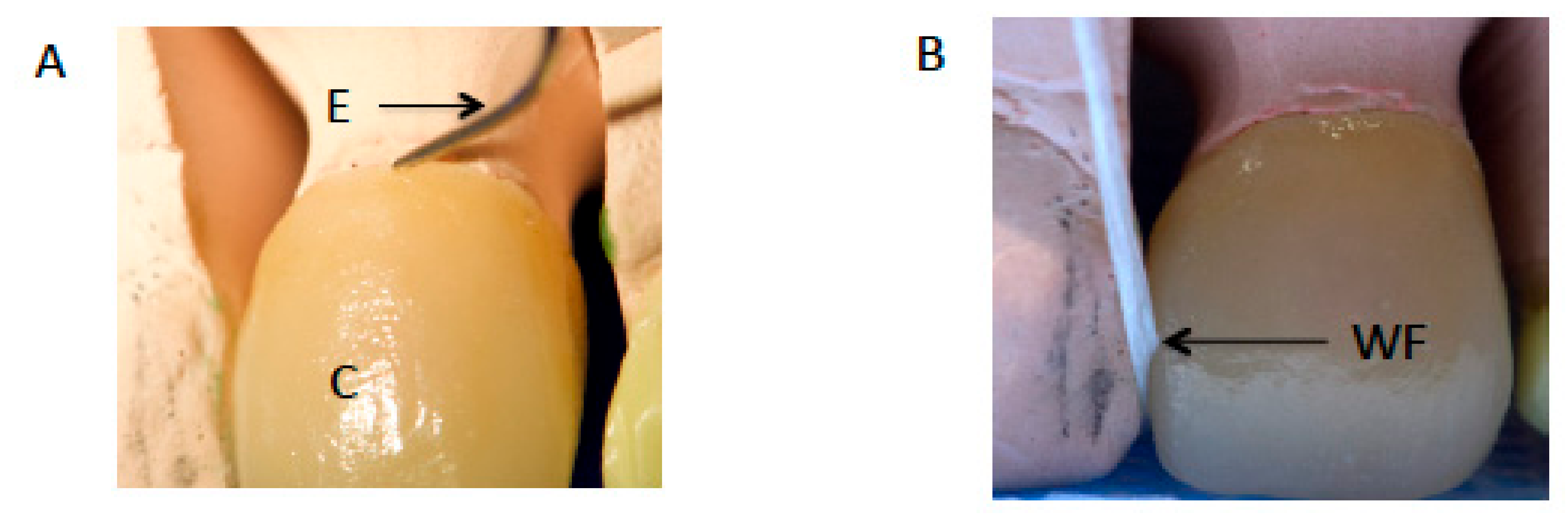
2.2.1. Marginal Adaptation
2.2.2. Contour
2.2.3. Proximal Contacts
2.3. Shade Evaluation
2.4. Statistical Analysis
3. Results
3.1. Quality
3.1.1. Marginal Adaptation
3.1.2. Crown Contours
3.1.3. Proximal Contacts
3.2. Shade Matching
3.2.1. Visual Assessment
3.2.2. ShadeEye Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCracken, M.S.; Litaker, M.S.; Gordan, V.V.; Karr, T.; Sowell, E.; Gilbert, G.H.; National Dental PBRN Collaborative Group. Remake Rates for Single-Unit Crowns in Clinical Practice: Findings from the National Dental Practice-Based Research Network. J. Prosthodont. 2019, 28, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Farah, J.W.; Dootz, E.; Mora, G.; Gregory, W. Insights of dental technicians: A survey of business and laboratory relations with dentists. Dentistry 1991, 11, 9. [Google Scholar] [PubMed]
- Bin-Shuwaish, M.S. Compliance of dental laboratory technicians with dentists’ instructions for fabrication of a PFM crown. Saudi J. Dent. Res. 2017, 8, 35–41. [Google Scholar] [CrossRef]
- Afsharzand, Z.; Rashedi, B.; Petropoulos, V.C. Communication between the dental laboratory technician and dentist. Work authorization for fixed partial dentures. J. Prosthodont. 2006, 15, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Leeper, S.H. Dentist and laboratory: A ‘‘love-hate’’ relationship. Dent. Clin. N. Am. 1979, 23, 87–99. [Google Scholar] [PubMed]
- Barsby, M.J.; Johnson, A.; Welfare, R.D.; Winstanley, R.B. Guides to Standards in Prosthetic Dentistry—Complete and Partial Dentures; British Society for the Study of Prosthetic Dentistry: London, UK, 2005. [Google Scholar]
- Almohareb, T.; Alkatheeri, M.S.; Vohra, F.; Alrahlah, A. Influence of experimental staining on the color stability of indirect computer-aided design/computer-aided manufacturing dental provisional materials. Eur. J. Dent. 2018, 12, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Vohra, F.; Labban, N.; Al-Hussaini, A.; Al-Jarboua, M.; Zawawi, R.; Alrahlah, A.; Naseem, M. Influence of Er; Cr: YSGG Laser on Shear Bond Strength and Color Stability of Lithium Disilicate Ceramics: An In Vitro Study. Photobiomodulation Photomed. Laser Surg. 2019, 37, 483–488. [Google Scholar] [CrossRef]
- Samer, M.S.; Faraz, Q.; Al-Dubai, S.A.; Vohra, F.; Abdullah, H.; Taiyeb-Ali, T.B.; Saub, R. Clinical outcomes and predictors of satisfaction in patients with improved lithium disilicate all-ceramic crowns. Med. Princ. Pract. 2017, 26, 470–479. [Google Scholar] [CrossRef]
- Vohra, F.; Altwaim, M.; Alshuwaier, A.S.; Alomayri, A.; Al-Deeb, M.; AlFawaz, Y.F.; Alrabiah, M.; Al-Ahdal, K.; Al-Deeb, L.; Abduljab-bar, T. Bond integrity and microleakage of dentin-bonded crowns cemented with bioactive cement in comparison to resin cements: In vitro study. J. Appl. Biomater. Funct. Mater. 2020, 18, 2280800020905768. [Google Scholar] [CrossRef]
- Al-Aali, K.A.; Alhamdan, R.S.; Maawadh, A.M.; Vohra, F.; Abduljabbar, T. Influence of contemporary CAD-CAM milling systems on the fit and adaptation of partially stabilized Zirconia fixed partial dentures. Pak. J. Med. Sci. 2020, 37, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Vohra, F.; Altwaim, M.; Alshuwaier, A.S.; Al-Deeb, M.; Alfawaz, Y.; Alrabiah, M.; Abduljabbar, T. Influence of Bioactive, Resin and Glass Ionomer luting cements on the fracture loads of dentin bonded ceramic crowns. Pak. J. Med. Sci. 2020, 36, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Van der Burgt, T.P.; Ten Bosch, J.J.; Borsboom, P.C.; Kortsmit, W.J. A comparison of new and conventional methods for quantifica-tion of tooth color. J. Prosthet. Dent. 1990, 63, 155–162. [Google Scholar] [CrossRef]
- Behr, M.; Zeman, F.; Baitinger, T.; Galler, J.; Koller, M.; Handel, G.; Rosentritt, M. The clinical performance of porcelain-fused-to-metal precious alloy single crowns: Chipping, recurrent caries, periodontitis, and loss of retention. Int. J. Prosthodont. 2014, 27, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Seghi, R.; Johnston, W.; O’Brien, W. Spectrophotometric analysis of color differences between porcelain systems. J. Prosthet. Dent. 1986, 56, 35–40. [Google Scholar] [CrossRef]
- Chiche, G.J.; Pinault, A. Esthetics of Anterior Fixed Prosthodontics; Quintessence: Chicago, IL, USA, 1994; pp. 61–64. [Google Scholar]
- White, J.; O’Brien, W. The Colors of Mixtures of Dental Opaque Porcelains. J. Dent. Res. 1989, 68, 1319–1322. [Google Scholar] [CrossRef]
- Reyes, J.; Acosta, P.; Ventura, D. Repeatability of the human eye compared to an intraoral scanner in dental shade matching. Heliyon 2019, 5, e02100. [Google Scholar] [CrossRef]
- Yilmaz, B.; Karaagaclioglu, L. In vitro evaluation of color replication of metal ceramic specimens using visual and instrumental color determinations. J. Prosthet. Dent. 2011, 105, 21–27. [Google Scholar] [CrossRef]
- Jathmi, A.A.A.; Alqahtani, M.A.A.; Hussain, M.W. Evaluation of accuracy of shade selection ability of students in the dental clinics and duplication of selected shade by the dental laboratory. A spectrophotometric in-vivo study. Saudi Dent. J. 2019, 31, S77. [Google Scholar] [CrossRef]
- Alshiddi, I.F.; Habib, S.R.; Al-Mazrou, F.Y.; Aly, A.M.; Al-Zaid, A.M. Comparing government (school) vs. private (non-school) dental laboratories in marginal adaptation of single porcelain-fused-to-metal crowns. Oral Health Dent. Manag. 2014, 13, 707–711. [Google Scholar]
- Cvar, J.F.; Ryge, G. Reprint of Criteria for the clinical evaluation of dental restorative materials. Clin. Oral Investig. 2006, 10, 92. [Google Scholar] [CrossRef]
- Bayne, S.C.; Schmalz, G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin. Oral Investig. 2005, 9, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Hickel, R.; Peschke, A.; Tyas, M.; Mjör, I.; Bayne, S.; Peters, M.; Hiller, K.A.; Randall, R.; Vanherle, G.; Heintze, S.D. FDI World Dental Federation: Clinical criteria for the evaluation of direct and indirect restorations—Update and clinical examples. Clin. Oral Investig. 2010, 14, 349–366. [Google Scholar] [CrossRef]
- Marquillier, T.; Doméjean, S.; le Clerc, J.; Chemla, F.; Gritsch, K.; Maurin, J.-C.; Millet, P.; Pérard, M.; Grosgogeat, B.; Dursun, E. The use of FDI criteria in clinical trials on direct dental restorations: A scoping review. J. Dent. 2018, 68, 1–9. [Google Scholar] [CrossRef]
- Selz, C.F.; Strub, J.R.; Vach, K.; Guess, P.C. Long-term performance of posterior InCeram Alumina crowns cemented with different luting agents: A prospective, randomized clinical split-mouth study over 5 years. Clin. Oral Investig. 2014, 18, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Batson, E.R.; Cooper, L.F.; Duqum, I.; Mendonça, G. Clinical outcomes of three different crown systems with CAD/CAM technology. J. Prosthet. Dent. 2014, 112, 770–777. [Google Scholar] [CrossRef]
- Baldissara, P.; Baldissara, S.; Scotti, R. Reliability of tactile perception using sharp and dull explorers in marginal opening identification. Int. J. Prosthodont. 1998, 11, 591–594. [Google Scholar]
- Hayashi, M.; Wilson, N.H.; Ebisu, S.; Watts, D.C. Influence of explorer tip diameter in identifying restoration margin discrepancies. J. Dent. 2005, 33, 669–674. [Google Scholar] [CrossRef]
- Teich, S.T.; Joseph, J.; Sartori, N.; Heima, M.; Duarte, S. Dental floss selection and its impact on evaluation of interproximal contacts in licensure exams. J. Dent. Educ. 2014, 78, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Prakki, A.; Cilli, R.; Saad, J.O.C.; Rodrigues, J.R. Clinical evaluation of proximal contacts of Class II esthetic direct restorations. Quintessence Int. 2004, 35, 785–789. [Google Scholar]
- Boice, P.A.; Niles, S.M.; Dubois, L.M. Evaluation of proximal contacts with shim stock. J. Oral Rehabil. 1987, 14, 91–94. [Google Scholar] [CrossRef]
- Dubois, L.M.; Niles, S.M.; Boice, P.A. The magnitude of interproximal spaces between adjacent teeth. Am. J. Dent. 1993, 6, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Jung, J.-H.; Kim, H.-J.; Chung, C.-H.; Oh, S.-H. Evaluation of tightness of proximal tooth contact in permanent dentition. J. Korean Acad. Prosthodont. 2008, 46, 553–560. [Google Scholar] [CrossRef]
- Chen, H.; Huang, J.; Dong, X.; Qian, J.; He, J.; Qu, X.; Lu, E. A systematic review of visual and instrumental measurements for tooth shade matching. Quintessence Int. 2012, 43, 649–659. [Google Scholar]
- Brewer, J.D.; Wee, A.; Seghi, R. Advances in color matching. Dent. Clin. N. Am. 2004, 48, 341–358. [Google Scholar] [CrossRef] [PubMed]
- Okubo, S.R.; Kanawati, A.; Richards, M.W.; Childressd, S. Evaluation of visual and instrument shade matching. J. Prosthet. Dent. 1998, 80, 642–648. [Google Scholar] [CrossRef]
- Yuan, K.; Sun, X.; Wang, F.; Wang, H.; Chen, J.-H. In Vitro and In Vivo Evaluations of Three Computer-Aided Shade Matching Instruments. Oper. Dent. 2012, 37, 219–227. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Marginal Adaptation | ||||
|---|---|---|---|---|
| Quality of Fit Criteria-Based Evaluation. | Government LABs (N and Row %) | Commercial LABs (N and Row %) | Total (N and Column %) | p Value |
| Excellent | 0 (0) | 4 (100) | 4 (12.5) | 0.007 |
| Acceptable | 10 (45.5) | 12 (54.5) | 22 (68.8) | |
| Acceptable with modifications | 4 (100) | 0 (0) | 4 (12.5) | |
| Unacceptable | 2 (100) | 0 (0) | 2 (6.20) | |
| Crown Contours | ||||
| Quality of Contours Criteria-Based Evaluation. | Government LABs (N and Row Percentage) | Commercial LABs (N and Row Percentage) | Total (N and Column %) | p Value |
| Excellent | 2 (16.6) | 10 (83.4) | 12 (37.5) | 0.002 |
| Acceptable | 2 (33.4) | 4 (66.6) | 6 (18.75) | |
| Acceptable with modifications | 8 (80) | 2 (20) | 10 (31.25) | |
| Unacceptable | 4 (100) | 0 (0) | 4 (12.5) | |
| Mesial Proximal Contact | ||||
|---|---|---|---|---|
| Quality of Contacts Criteria-Based Evaluation | Government LABs (N and Row %) | Commercial LABs (N and Row %) | Total (N and Column %) | p Value |
| Excellent | 2 (25) | 6 (75) | 8 (25) | 0.125 |
| Acceptable | 2 (100) | 0 (0) | 2 (6.25) | |
| Acceptable with modifications | 10 (50) | 10 (50) | 20 (62.5) | |
| Unacceptable | 2 (100) | 0 (0) | 2 (6.25) | |
| Distal Proximal Contact | ||||
| Quality of Contacts Criteria-Based Evaluation | Government LABs (N and Row Percentage) | Commercial LABs (N and Row Percentage) | Total (N and Column %) | p Value |
| Excellent | 2 (20) | 8 (80) | 10 (31.3) | 0.106 |
| Acceptable | 4 (66.6) | 2 (33.4) | 6 (18.7) | |
| Acceptable with modifications | 4 (50) | 4 (50) | 8 (25) | |
| Unacceptable | 6 (75) | 2 (25) | 8 (25) | |
| Visual Shade Matching, Cervical 3rd | ||||
|---|---|---|---|---|
| Accuracy of Shade, Criteria-Based Evaluation. | Government LABs (N and Row %) | Commercial LABs (N and Row %) | Total (N and Column %) | p Value |
| Matching | 8 (40) | 12 (60) | 20(62.5) | 0.273 |
| Non-Matching | 8 (66.6) | 4 (33.4) | 12 (37.5) | |
| Visual Shade Matching, Middle Third | ||||
| Matching | 12 (50) | 12 (50) | 24 (75) | 1.0 |
| Non-Matching | 4 (50) | 4 (50) | 8 (25) | |
| Visual Shade Matching, Incisal Thid | ||||
| Matching | 3 (21.5) | 11 (78.5) | 14 (43.7) | 0.004 |
| Non-Matching | 13 (72.3) | 5 (27.7) | 18 (56.3) | |
| Overall Visual Shade Matching (All Thirds) | ||||
| Complete Matching | 1 (12.5) | 7 (87.5) | 8 (25) | 0.005 |
| 2/3rd matching | 11 (61.2) | 7 (38.8) | 18 (56.25) | |
| 1/3rd matching | 0 (0) | 2 (100) | 2 (6.25) | |
| None matching | 4 (100) | 0 (0) | 4 (12.5) | |
| ShadeEye Shade Matching, Cervical Third | ||||
|---|---|---|---|---|
| Accuracy of Shade, Criteria-Based Evaluation. | Government LABs (N and Row %) | Commercial LABs (N and Row %) | Total (N and Column %) | p Value |
| Matching | 8 (40) | 12 (60) | 20(62.5) | 0.27 |
| Non-Matching | 8 (66.6) | 4 (33.3) | 12 (37.5) | |
| ShadeEye Shade Matching, Middle Third | ||||
| Matching | 14 (51.8) | 13 (48.1) | 27 (84.4) | 1.0 |
| Non-Matching | 2 (40) | 3 (60) | 5 (15.6) | |
| ShadeEye Shade Matching, Incisal Third | ||||
| Matching | 2 (16.6) | 10 (83.3) | 12 (37.5) | 0.004 |
| Non-Matching | 14 (70) | 6 (30) | 20 (62.5) | |
| Overall ShadeEye Shade Matching (All Thirds) | ||||
| Complete Matching | 0 (0) | 8 (100) | 8 (25) | 0.001 |
| 2/3rd matching | 10 (83.4) | 2 (16.6) | 12 (37.5) | |
| 1/3rd matching | 4 (40) | 6 (60) | 10 (31.3) | |
| None matching | 2 (100) | 0 (0) | 2 (6.2) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bin-Shuwaish, M.S.; AlFawaz, Y.F.; AlGamaiah, H.A.; AlSani, A.S.; Abobakr, I.B.; Alzahrani, K.M.; Almutairi, B.; Attar, E.A.; Vohra, F.; Abduljabbar, T. Technical Accuracy of Dental Laboratories in the Quality and Shade Matching of Porcelain Fused to Metal Crowns: An In Vitro Study. Int. J. Environ. Res. Public Health 2021, 18, 2722. https://doi.org/10.3390/ijerph18052722
Bin-Shuwaish MS, AlFawaz YF, AlGamaiah HA, AlSani AS, Abobakr IB, Alzahrani KM, Almutairi B, Attar EA, Vohra F, Abduljabbar T. Technical Accuracy of Dental Laboratories in the Quality and Shade Matching of Porcelain Fused to Metal Crowns: An In Vitro Study. International Journal of Environmental Research and Public Health. 2021; 18(5):2722. https://doi.org/10.3390/ijerph18052722
Chicago/Turabian StyleBin-Shuwaish, Mohammed. S., Yasser F. AlFawaz, Hamad A. AlGamaiah, Abdulaziz S. AlSani, Ibrahim B. Abobakr, Khaled M. Alzahrani, Basil Almutairi, Esraa A. Attar, Fahim Vohra, and Tariq Abduljabbar. 2021. "Technical Accuracy of Dental Laboratories in the Quality and Shade Matching of Porcelain Fused to Metal Crowns: An In Vitro Study" International Journal of Environmental Research and Public Health 18, no. 5: 2722. https://doi.org/10.3390/ijerph18052722
APA StyleBin-Shuwaish, M. S., AlFawaz, Y. F., AlGamaiah, H. A., AlSani, A. S., Abobakr, I. B., Alzahrani, K. M., Almutairi, B., Attar, E. A., Vohra, F., & Abduljabbar, T. (2021). Technical Accuracy of Dental Laboratories in the Quality and Shade Matching of Porcelain Fused to Metal Crowns: An In Vitro Study. International Journal of Environmental Research and Public Health, 18(5), 2722. https://doi.org/10.3390/ijerph18052722