
Effects of the Physician–Primary-Healthcare Nurse Telemedicine Model (P-NTM) on Medication Adherence and Health-Related Quality of Life (HRQoL) of Patients with Chronic Disease at Remote Rural Areas


Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection and Procedures
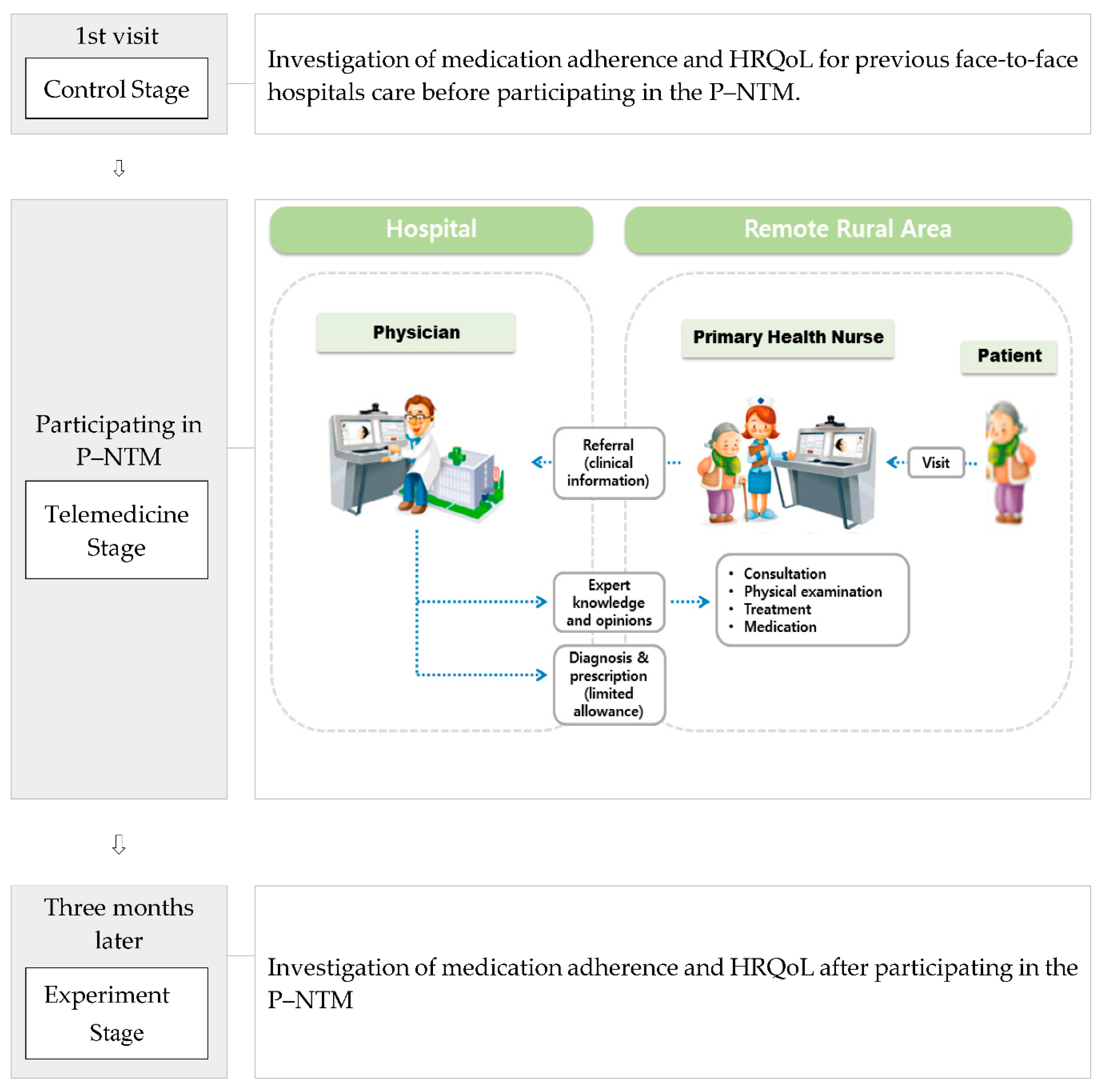
2.2.1. Chronic-Disease Management Program Utilizing P–NTM
2.2.2. Medication Adherence
2.2.3. Health-Related Quality of Life (HRQoL)
2.3. Ethical Considerations
2.4. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Comparison of Variables between Previous Hospital Care and P–NTM
3.3. Logistic-Regression Analyses
4. Discussion
4.1. Limitations
4.2. Implications for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Status Report on Non-Communicable Diseases. 2014. Available online: https://www.who.int/ncds/introduction/en/ (accessed on 11 January 2020).
- Megari, K. Quality of life in chronic disease patients. Health Psychol. Res. 2013, 1, 141–148. [Google Scholar] [CrossRef]
- Horvat, N.; Locatelli, I.; Kos, M.; Janežič, J. Medication adherence and health-related quality of life among patients with chronic obstructive pulmonary disease. Acta. Pharm. 2018, 68, 117–125. [Google Scholar] [CrossRef]
- Jachimowicz, J.M.; Gladstone, J.J.; Berry, D.; Kirkdale, C.L.; Thornley, T.; Galinsky, A.D. Making medications stick: Improving medication adherence by highlighting the personal health costs of non-compliance. Behav. Public Policy 2019, 1–21. [Google Scholar] [CrossRef]
- Lyons, I.; Barber, N.; Raynor, D.K.; Wei, L. Evaluation (MASE): A randomized controlled trial of a pharmacist-led telephone based intervention designed to improve medication adherence. BMJ Qual. Saf. 2016, 25, 759–769. [Google Scholar] [CrossRef]
- Vik, S.A.; Maxwell, C.J.; Hogan, D.B.; Patten, S.B.; Johnson, J.A.; Romonko-Slack, L. Assessing medication adherence among older persons in community settings. Can. J. Clin. Pharmacol. 2005, 12, e152–e164. [Google Scholar]
- Hsiao, C.Y.; Chang, C.; Chen, C.D. An investigation on illness perception and adherence among hypertensive patients. Kaohsiung J. Med. Sci. 2012, 28, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.M.; Ponieman, D.; Leventhal, H.; Halm, E.A. Predictors of adherence to diabetes medications: The role of disease and medication beliefs. J. Behav. Med. 2009, 32, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Vermeire, E.; Hearnshaw, H.; Royen, P.V.; Denekens, J. Patient adherence to treatment: Three decades of research. A comprehensive review. J. Clin. Pharm. Ther. 2001, 26, 331–342. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. 2003. Available online: http://www.who.int/chp/knowledge/publications/adherence_report/en/ (accessed on 15 May 2020).
- Gomes, D.; Placido, A.I.; Mó, R.; Simões, J.L.; Amaral, O.; Fernandes, I.; Lima, F.; Morgado, M.; Figueiras, A.; Herdeiro, M.T.; et al. Daily medication management and adherence in the polymedicated elderly: A cross-sectional study in Portugal. Int. J. Environ. Res. Public Health 2020, 17, 200. [Google Scholar] [CrossRef] [PubMed]
- Korea Institute for Health and Social Affairs. A Report on the Korea Health Panel Survey of 2017. Available online: https://www.kihasa.re.kr/english/publications/eng_research/list.do?keyField=title&key=2017&menuId=68&tid=34&bid=30 (accessed on 10 March 2020).
- Hiratsuka, V.; Delafield, R.; Starks, H.; Ambrose, A.J.; Mau, M.M. Patient and provider perspectives on using telemedicine for chronic disease management among native Hawaiian and Alaska native people. Int. J. Circumpolar Health 2013, 72, 21401. [Google Scholar] [CrossRef] [PubMed]
- Dal Bello-Haas, V.P.M.; O’Connell, M.E.; Morgan, D.G.; Crossley, M. Lessons learned: Feasibility and acceptability of a telehealth-delivered exercise intervention for rural-dwelling individuals with dementia and their caregivers. Rural Remote Health 2014, 14, 2715. [Google Scholar]
- Mehrotra, A.; Jena, A.B.; Busch, A.B.; Souza, J.; Uscher-Pines, L.; Landon, B.E. Utilization of telemedicine among rural medicare beneficiaries. JAMA 2016, 315, 2015–2016. [Google Scholar] [CrossRef]
- Wootton, R. Twenty years of telemedicine in chronic disease management—An evidence synthesis. J. Telemed. Telecare 2012, 18, 211–220. [Google Scholar] [CrossRef]
- Wootton, R.; Craig, J.; Patterson, V. Introduction to Telemedicine, 2nd ed.; The Royal Society of Medicine Press: London, UK, 2017. [Google Scholar]
- von Storch, K.; Graaf, E.; Wunderlich, M.; Rietz, C.; Polidori, M.C.; Woopen, C. Telemedicine-assisted self-management program for type 2 diabetes patients. Diabetes Technol. Ther. 2019, 21, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Gellis, Z.D.; Kenaley, B.L.; Have, T.T. Integrated telehealth care for chronic illness and depression in geriatric home care patients: The integrated telehealth education and activation of mood (I-TEAM) study. J Am. Geriatr. Soc. 2014, 62, 889–895. [Google Scholar] [CrossRef]
- Korean Ministry of Health and Welfare, National Medical Center. 2018 Pilot Telemedicine Project for Underserved Remote Rural Areas: Development of the Model and Its’ Evaluation; Korean Ministry of Health and Welfare, National Medical Center: Seoul, Korea, 2019; ISBN 11135200000140610. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Korean Ministry of Government Legislation. The Medical Law. Available online: http://www.moleg.go.kr (accessed on 15 January 2020).
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine practice: Review of the current ethical and legal challenges. Telemed. E-Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef]
- Kim, S.O. Medication adherence of elderly with hypertension and/or diabetes-mellitus and its’ influencing factors. Korean J. Clin. Pharm. 2011, 21, 81–89. [Google Scholar]
- Case Management Society of America. Case Management Adherence Guidelines; Version 1.0; Case Management Society of America: Nashville, TN, USA, 2004; pp. 29–31. [Google Scholar]
- Morisky, D.E.; Levin, D.M.; Green, L.W.; Shapiro, S.; Russell, R.P.; Smith, C.R. Five-year blood pressure control and mortality following health education for hypertensive patients. Am. J. Public Health 1983, 73, 153–162. [Google Scholar] [CrossRef]
- Kim, J.I.; Kim, E.J.; Kim, J.H.; Oh, C.O. Validity of morisky medication adherence scales in assessment of statin adherence in dyslipidemic patients. Korean J. Fam. Pract. 2015, 5, 332–337. [Google Scholar]
- Kim, M.H.; Cho, Y.S.; Uhm, W.S.; Kim, S.; Bae, S.C. Cross-cultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual. Life Res. 2005, 14, 1401–1406. [Google Scholar] [CrossRef]
- Kim, H.S.; Yang, S.J.; Jeong, Y.J.; Kim, Y.E.; Hong, S.W.; Cho, J.H. Satisfaction survey on information technology-based glucose monitoring system targeting diabetes mellitus in private local clinics in Korea. Diabetes Metab. J. 2017, 41, 213–222. [Google Scholar] [CrossRef]
- Farrell, B. Utilizing Telehealth Technology to Reduce Social Isolation and Depression in Seniors. 2020. Available online: https://digital.sandiego.edu/dnp/113 (accessed on 1 June 2020).
- Maresca, G.; De Cola, M.C.; Caliri, S.; De Luca, R.; Manuli, A.; Scarcella, I.; Silvestri, G.; Bramanti, P.; Torrisi, M.; Calabrò, R.S.; et al. Moving towards novel multidisciplinary approaches for improving elderly quality of life: The emerging role of telemedicine in Sicily. J. Telemed. Telecare 2019, 25, 318–324. [Google Scholar] [CrossRef]
- Sun, C.; Sun, L.; Xi, S.; Zhang, H.; Wang, H.; Feng, Y.; Deng, Y.; Wang, H.; Xiao, X.; Wang, G.; et al. Mobile phone-based telemedicine practice in older Chinese patients with type 2 diabetes mellitus: Randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e10664. [Google Scholar] [CrossRef] [PubMed]
- Benson, G.A.; Sidebottom, A.; Hayes, J.; Miedema, M.D.; Boucher, J.; Vacquier, M.; Sillah, A.; Gamam, S.; VanWormer, J.J. Impact of ENHANCED (diEtitiaNs helping pAtieNts CarE for diabetes) telemedicine randomized controlled trial on diabetes optimal care outcomes in patients with type 2 diabetes. J. Acad. Nutr. Diet. 2019, 119, 585–598. [Google Scholar] [CrossRef]
- Park, S.J.; Rim, S.J.; Kim, C.E.; Park, S. Effect of comorbid depression on health-related quality of life of patients with chronic diseases: A South Korean nationwide study (2007–2015). J. Psychosom. Res. 2019, 116, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Moon, J.Y.; Yoo, B.I.; Park, K.J.; Choi, J.Y.; Jhang, W.G.; Park, Y.H. Review on the physician–patient telemedicine in legal and social systemic aspect. Korean J. Med. Law 2013, 21, 201–219. [Google Scholar]
- Kim, J.S.; Oh, S.H. A comparative analysis on current status of telemedicine policy: Focused on United States, Japan, Korea. Korean J. Health Econ. Policy 2018, 24, 1–35. [Google Scholar]
- Vidal-Alaball, J.; Acosta-Roja, R.; Pastor Hernández, N.; Sanchez Luque, U.; Morrison, D.; Narejos Pérez, S.; Perez-Llano, J.; López Seguí, F.; Salvador Vèrges, A. Telemedicine in the face of the COVID-19 pandemic. Aten. Primaria 2020, 52, 418–422. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Categories | n | % |
|---|---|---|---|
| Gender | Male | 40 | 35.4 |
| Female | 73 | 64.6 | |
| Age (years) | ≤64 | 34 | 31.5 |
| 65–69 | 16 | 14.8 | |
| 70–74 | 16 | 14.8 | |
| 75–79 | 22 | 20.4 | |
| ≥80 | 20 | 18.5 | |
| M ± SD | 69.74 ± 9.36 | ||
| Range | 47–86 | ||
| Employment status | Employment | 55 | 50.9 |
| Unemployment | 53 | 49.1 | |
| Health security | National health insurance | 106 | 94.6 |
| Medical benefits | 6 | 5.4 | |
| No. of households | Living alone | 43 | 38.1 |
| Two households | 59 | 52.2 | |
| Over three households | 11 | 9.7 | |
| Disease | Hypertension | 75 | 66.4 |
| Hyperlipidemia | 6 | 5.3 | |
| Diabetes mellitus | 10 | 8.8 | |
| More than two diseases | 22 | 19.5 | |
| Characteristics | Items | Medication Adherence | HRQoL 2 | ||||
|---|---|---|---|---|---|---|---|
| Previous Hospital Care | P−NTM 3 | t (p) | Previous Hospital Care | P−NTM 3 | t (p) | ||
| Gender | Male | 10.70 ± 1.11 | 11.23 ± 0.89 | −3.20 (0.003) | 14.13 ± 1.18 | 14.35 ± 1.23 | −1.94 (0.060) |
| Female | 10.25 ± 1.79 | 11.20 ± 0.95 | −4.21 (<0.001) | 13.24 ± 1.62 | 13.49 ± 1.74 | −2.84 (0.006) | |
| Age, (years) | ≤64 | 10.27 ± 2.25 | 11.35 ± 0.73 | −2.76 (0.009) | 14.44 ± 0.96 | 14.47 ± 1.08 | −0.30 (0.768) |
| 65–69 | 9.88 ± 1.31 | 11.00 ± 0.97 | −3.74 (0.002) | 13.75 ± 1.13 | 14.38 ± 1.09 | −4.04 (0.001) | |
| 70–74 | 10.31 ± 1.20 | 11.19 ± 0.83 | −3.96 (0.001) | 13.19 ± 1.97 | 13.75 ± 2.08 | −2.76 (0.014) | |
| 75–79 | 10.90 ± 1.04 | 11.33 ± 0.80 | −1.63 (0.119) | 13.10 ± 1.41 | 13.43 ± 1.60 | −2.09 (0.049) | |
| ≥80 | 10.65 ± 0.99 | 10.90 ± 1.33 | −0.84 (0.412) | 12.65 ± 1.66 | 12.70 ± 1.69 | −0.25 (0.804) | |
| Employment status | Employment | 10.25 ± 1.93 | 11.09 ± 0.91 | −3.12 (0.003) | 14.33 ± 0.92 | 14.51 ± 0.90 | −2.63 (0.011) |
| Unemployment | 10.57 ± 1.12 | 11.37 ± 0.85 | −4.92 (<0.001) | 12.71 ± 1.65 | 13.12 ± 1.90 | −3.44 (0.001) | |
| Health security | National health insurance | 10.41 ± 1.61 | 13.57 ± 1.54 | −4.94 (<0.001) | 13.57 ± 1.54 | 13.84 ± 1.59 | −3.29 (0.001) |
| Medical benefits | 10.83 ± 1.17 | 12.67 ± 1.97 | −1.20 (0.286) | 12.67 ± 1.97 | 12.83 ± 2.14 | −0.54 (0.611) | |
| Number of households | Living alone | 10.79 ± 0.92 | 11.17 ± 1.08 | −1.95 (0.058) | 13.07 ± 1.55 | 13.33 ± 1.65 | −2.05 (0.047) |
| Two households | 10.07 ± 1.96 | 11.25 ± 0.84 | −4.80 (<0.001) | 13.81 ± 1.50 | 14.12 ± 1.55 | −3.34 (0.001) | |
| Over three households | 10.90 ± 0.74 | 11.10 ± 0.74 | −1.50 (0.168) | 14.00 ± 1.26 | 13.82 ± 1.60 | 1.49 (0.167) | |
| Disease | Hypertension | 10.42 ±1.22 | 11.21 ± 0.87 | −5.92 (<0.001) | 13.49 ± 1.55 | 13.73 ± 1.70 | −2.77 (0.007) |
| Hyperlipidemia | 10.83 ± 0.98 | 11.17 ± 0.98 | −1.00 (0.363) | 13.33 ± 2.73 | 13.50 ± 2.35 | −1.00 (0.363) | |
| Diabetes | 10.00 ± 3.59 | 11.70 ± 0.67 | −1.41 (0.191) | 14.10 ± 0.88 | 14.60 ± 0.70 | −3.00 (0.015) | |
| Over two diseases | 10.45 ± 1.47 | 11.00 ± 1.16 | −1.67 (0.110) | 13.59 ± 1.33 | 13.72 ± 1.42 | −0.77 (0.451) | |
| Variables | B | S.E. | p | Exp (B) | 95% CI |
|---|---|---|---|---|---|
| Medication adherence | 0.57 | 0.14 | <0.001 | 1.76 | 1.34–2.31 |
| HRQoL | 0.07 | 0.09 | 0.459 | 1.07 | 0.90–1.27 |
| Constant | −7.07 | 1.85 | 0.000 | 0.001 |
| B | S.E. | p | Exp (B) | 95% CI | |
|---|---|---|---|---|---|
| Knowledge of medication adherence | 0.22 | 0.26 | 0.408 | 1.24 | 0.74–2.07 |
| Motivation of medication adherence | 0.73 | 0.18 | 0.000 | 2.08 | 1.47–2.97 |
| Mobility | 0.34 | 0.52 | 0.513 | 1.41 | 0.54–3.93 |
| Self–care | −0.53 | 0.59 | 0.371 | 0.59 | 0.19–1.88 |
| Usual activity | −0.84 | 0.53 | 0.113 | 0.43 | 0.15–1.22 |
| Pain and discomfort | 0.40 | 0.33 | 0.224 | 1.49 | 0.78–2.84 |
| Anxiety and depression | 0.81 | 0.35 | 0.019 | 2.25 | 1.14–4.45 |
| Constant | −5.40 | 2.19 | 0.014 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwak, M.Y.; Hwang, E.J.; Lee, T.H. Effects of the Physician–Primary-Healthcare Nurse Telemedicine Model (P-NTM) on Medication Adherence and Health-Related Quality of Life (HRQoL) of Patients with Chronic Disease at Remote Rural Areas. Int. J. Environ. Res. Public Health 2021, 18, 2502. https://doi.org/10.3390/ijerph18052502
Kwak MY, Hwang EJ, Lee TH. Effects of the Physician–Primary-Healthcare Nurse Telemedicine Model (P-NTM) on Medication Adherence and Health-Related Quality of Life (HRQoL) of Patients with Chronic Disease at Remote Rural Areas. International Journal of Environmental Research and Public Health. 2021; 18(5):2502. https://doi.org/10.3390/ijerph18052502
Chicago/Turabian StyleKwak, Mi Young, Eun Jeong Hwang, and Tae Ho Lee. 2021. "Effects of the Physician–Primary-Healthcare Nurse Telemedicine Model (P-NTM) on Medication Adherence and Health-Related Quality of Life (HRQoL) of Patients with Chronic Disease at Remote Rural Areas" International Journal of Environmental Research and Public Health 18, no. 5: 2502. https://doi.org/10.3390/ijerph18052502
APA StyleKwak, M. Y., Hwang, E. J., & Lee, T. H. (2021). Effects of the Physician–Primary-Healthcare Nurse Telemedicine Model (P-NTM) on Medication Adherence and Health-Related Quality of Life (HRQoL) of Patients with Chronic Disease at Remote Rural Areas. International Journal of Environmental Research and Public Health, 18(5), 2502. https://doi.org/10.3390/ijerph18052502