
Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran


 ,
, 
 and
and 
Abstract
1. Introduction
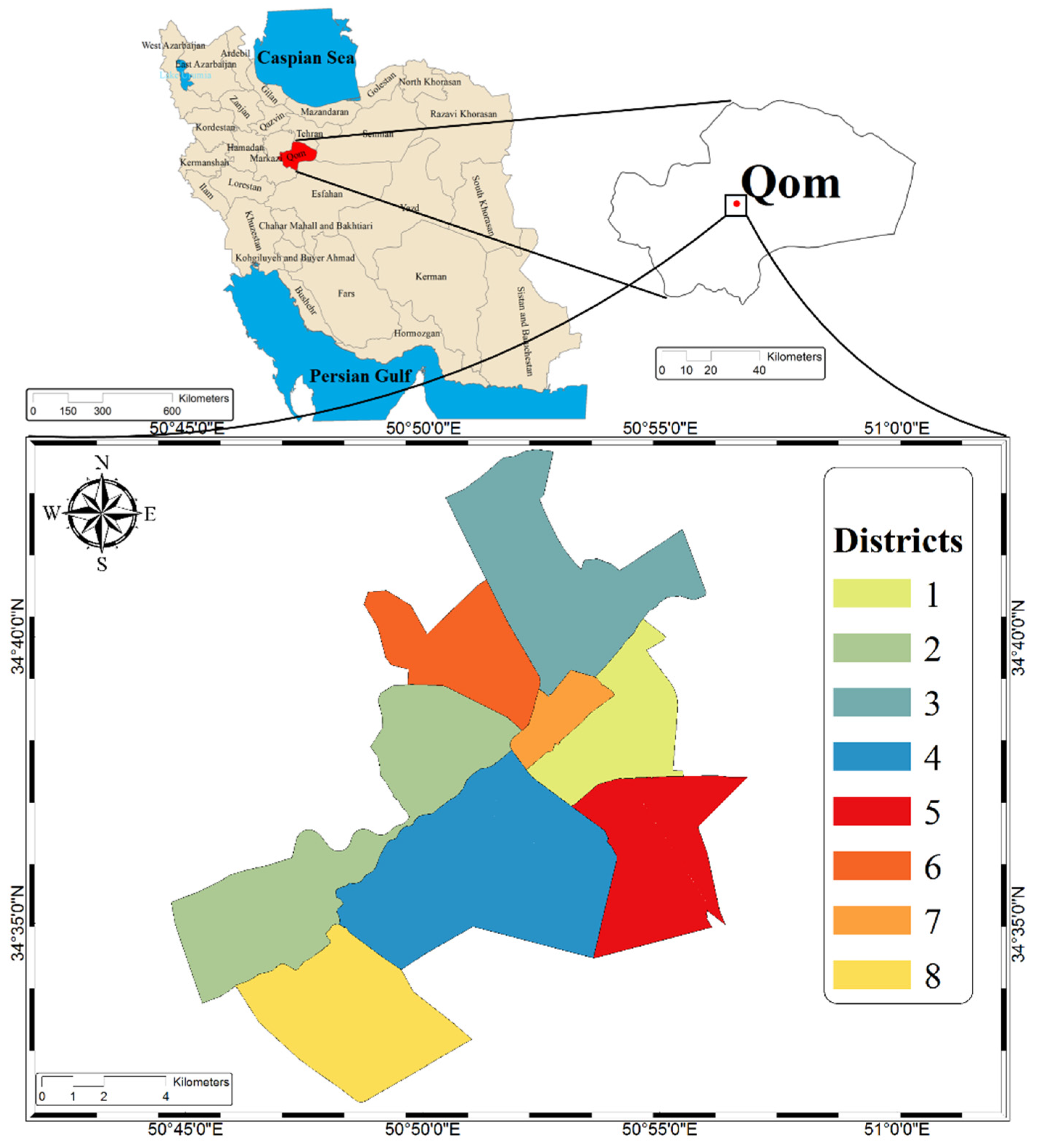
2. Materials and Methods
3. Results
3.1. Socio-Demographic Information
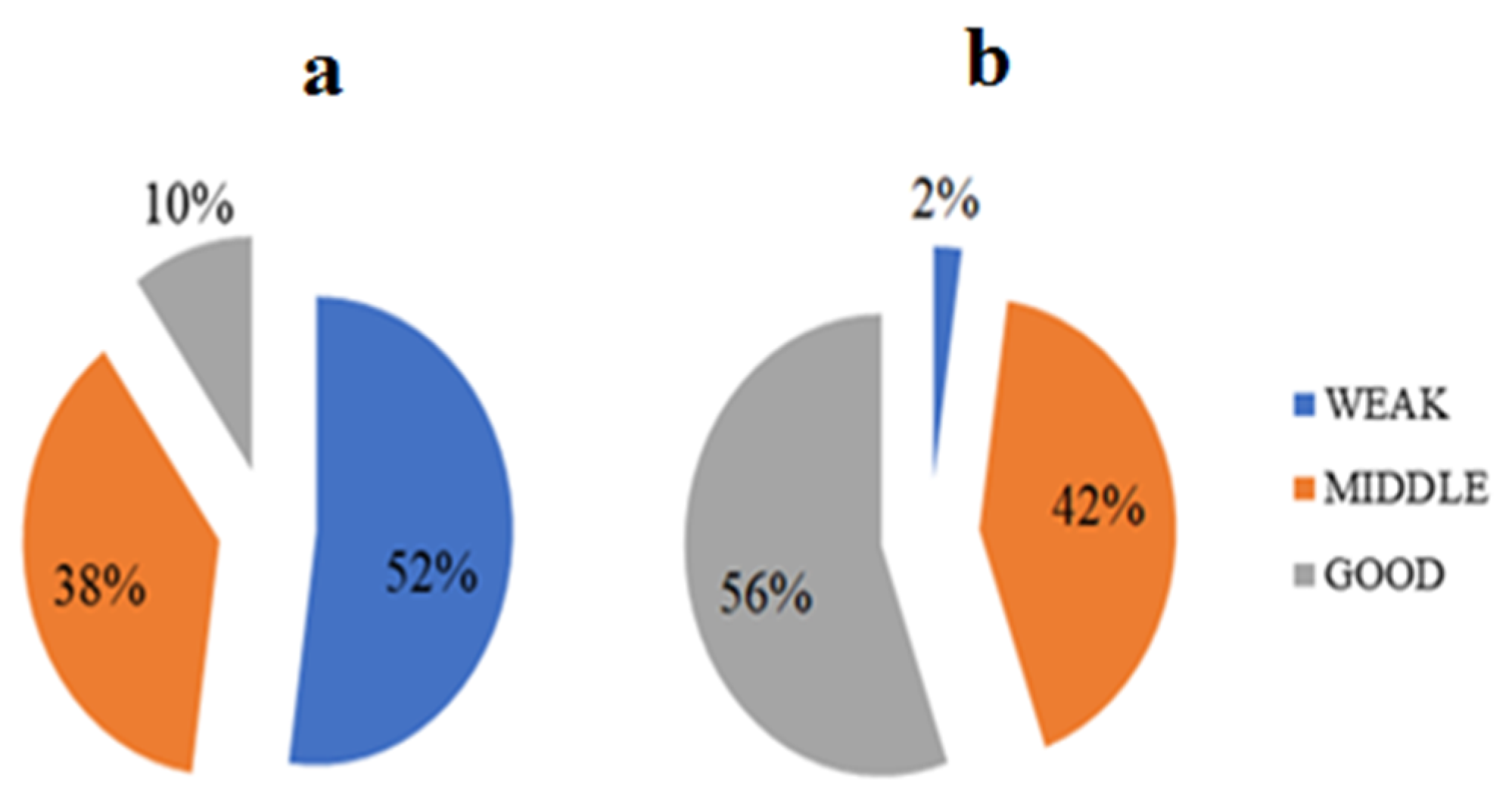
3.2. Awareness
3.3. Performance
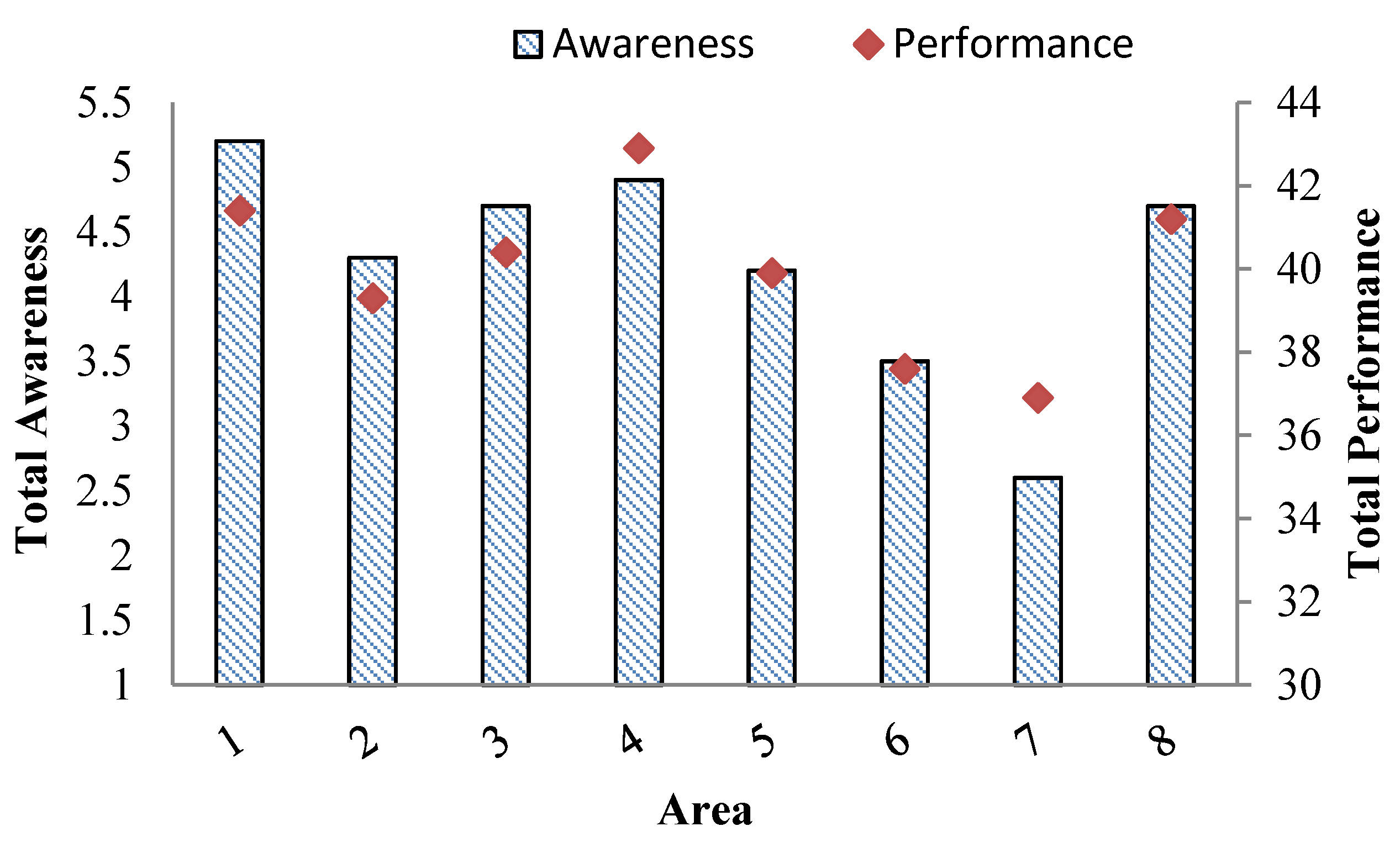
3.4. Total Awareness and Performance Scores
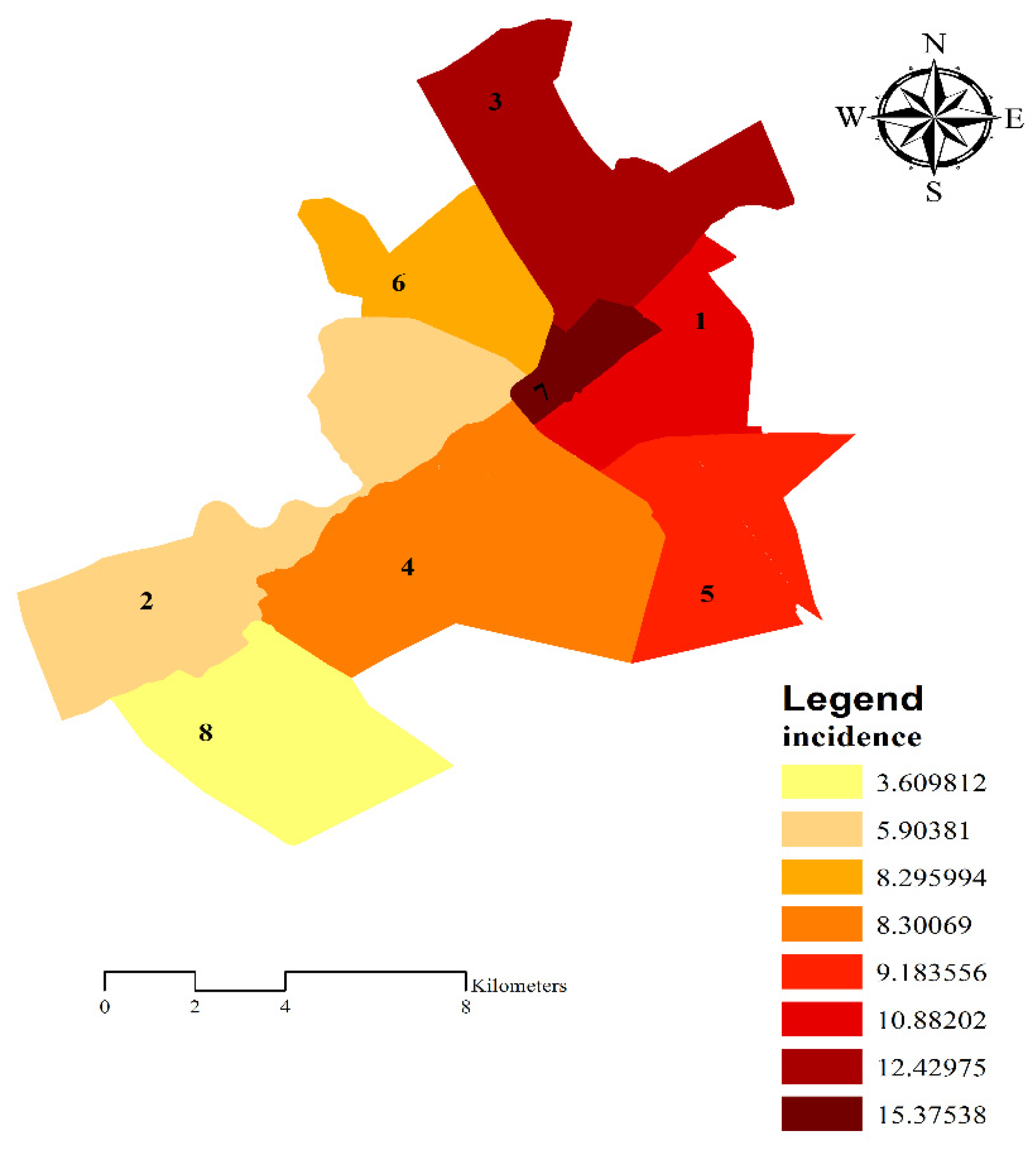
3.5. Relationship between Mean Scores of Awareness and Performance and COVID-19 Incidence
4. Discussion
Limitations, Strengths and Suggestions for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV); WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Katayoon, K.; Shahla, A. Coronavirus (Middle Eastern Respiratory Syndrome). J. Army Sch. Nurs. 2016. Available online: https://civilica.com/doc/898710/ (accessed on 7 April 2020).
- Fathizadeh, H.; Maroufi, P.; Momen-Heravi, M.; Dao, S.; Köse, Ş.; Ganbarov, K.; Pagliano, P.; Esposito, S.; Kafil, H.S. Protection and disinfection policies against SARS-CoV-2 (COVID-19). Infez. Med. 2020, 28, 185–191. [Google Scholar]
- Bagheri, S.H.; Asghari, A.; Farhadi, M.; Shamshiri, A.R.; Kabir, A.; Kamrava, S.K.; Jalessi, M.; Mohebbi, A.; Alizadeh, R.; Honarmand, A.A. Coincidence of COVID-19 epidemic and olfactory dysfunction outbreak in Iran. Med. J. Islamic Repub. Iran 2020, 34, 62. [Google Scholar]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report 46; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Abdi, M. Coronavirus disease 2019 (COVID-19) outbreak in Iran: Actions and problems. Infect. Control Hosp. Epidemiol. 2020, 41, 754–755. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. 2020. Available online: https://covid19.who.int/region/emro/country/ir (accessed on 6 September 2020).
- Rahimi, N.R.; Fouladi-Fard, R.; Aali, R.; Shahryari, A.; Rezaali, M.; Ghafouri, Y.; Ghalhari, M.R.; Ghalhari, M.A.; Farzinnia, B.; Fiore, M. Bidirectional Association Between COVID-19 and the Environment: A Systematic Review. Environ. Res. 2020, 194, 110692. [Google Scholar] [CrossRef]
- Farcas, A.C.; Galanakis, C.M.; Socaciu, C.; Pop, O.L.; Tibulca, D.; Paucean, A.; Jimborean, M.A.; Fogarasi, M.; Salanta, L.C.; Tofana, M. Food Security during the Pandemic and the Importance of the Bioeconomy in the New Era. Sustainability 2020, 13, 150. [Google Scholar] [CrossRef]
- Wax, R.S.; Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can. J. Anesth. J. Can. Danesthésie 2020, 67, 568–576. [Google Scholar] [CrossRef]
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, taaa021. [Google Scholar] [CrossRef]
- Yang, Y.; Lu, Q.; Liu, M.; Wang, Y.; Zhang, A.; Jalali, N.; Dean, N.; Longini, I.; Halloran, M.E.; Xu, B. Epidemiological and clinical features of the 2019 novel coronavirus outbreak in China. medRxiv 2020. [Google Scholar] [CrossRef]
- Hosseini, M.R.; Fouladi-Fard, R.; Aali, R. COVID-19 pandemic and sick building syndrome. Indoor Built Environ. 2020, 29, 1181–1183. [Google Scholar] [CrossRef]
- World Health Organization. Considerations for Quarantine of Individuals in the Context of Containment for Coronavirus Disease (COVID-19): Interim Guidance, 29 February 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Sadati, A.K.; B Lankarani, M.H.; Bagheri Lankarani, K. Risk Society, Global Vulnerability and Fragile Resilience; Sociological View on the Coronavirus Outbreak: Kowsar, Iran, 2020. [Google Scholar]
- Li, J.-P.O.; Lam, D.S.C.; Chen, Y.; Ting, D.S.W. Novel Coronavirus Disease 2019 (COVID-19): The Importance of Recognising Possible Early Ocular Manifestation and Using Protective Eyewear; BMJ Publishing Group Ltd.: London, UK, 2020. [Google Scholar]
- Jinia, A.J.; Sunbul, N.B.; Meert, C.A.; Miller, C.A.; Clarke, S.D.; Kearfott, K.J.; Matuszak, M.M.; Pozzi, S.A. Review of Sterilization Techniques for Medical and Personal Protective Equipment Contaminated With SARS-CoV-2. IEEE Access 2020, 8, 111347–111354. [Google Scholar] [CrossRef]
- Luo, W.; Majumder, M.; Liu, D.; Poirier, C.; Mandl, K.; Lipsitch, M.; Santillana, M. The role of absolute humidity on transmission rates of the COVID-19 outbreak. DASH 2020. [Google Scholar] [CrossRef]
- Arab-Mazar, Z.; Sah, R.; Rabaan, A.A.; Dhama, K.; Rodriguez-Morales, A.J. Mapping the incidence of the COVID-19 hotspot in Iran–Implications for Travellers. Travel Med. Infect. Dis. 2020, 101630. [Google Scholar] [CrossRef]
- Alamdari, N.M.; Afaghi, S.; Rahimi, F.S.; Tarki, F.E.; Tavana, S.; Zali, A.; Fathi, M.; Besharat, S.; Bagheri, L.; Pourmotahari, F. Mortality Risk Factors among Hospitalized COVID-19 Patients in a Major Referral Center in Iran. Tohoku J. Exp. Med. 2020, 252, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Khazaei, M.; Mahvi, A.H.; Fard, R.F.; Izanloo, H.; Yavari, Z.; Tashayoei, H.R. Dental caries prevalence among Schoolchildren in Urban and Rural areas of Qom Province, Central part of Iran. Middle East J. Sci. Res. 2013, 18, 584–591. [Google Scholar]
- Fard, R.F.; Naddafi, K.; Yunesian, M.; Nodehi, R.N.; Dehghani, M.H.; Hassanvand, M.S. The assessment of health impacts and external costs of natural gas-fired power plant of Qom. Environ. Sci. Pollut. Res. 2016, 23, 20922–20936. [Google Scholar] [CrossRef] [PubMed]
- Fard, R.F.; Naddafi, K.; Hassanvand, M.S.; Khazaei, M.; Rahmani, F. Trends of metals enrichment in deposited particulate matter at semi-arid area of Iran. Environ. Sci. Pollut. Res. 2018, 25, 18737–18751. [Google Scholar] [CrossRef]
- Fahiminia, M.; Fard, R.F.; Ardani, R.; Naddafi, K.; Hassanvand, M.; Mohammadbeigi, A. Indoor radon measurements in residential dwellings in Qom, Iran. Int. J. Radiat. Res. 2016, 14, 331. [Google Scholar] [CrossRef]
- Mojarrad, H.; Fouladi Fard, R.; Rezaali, M.; Heidari, H.; Izanloo, H.; Mohammadbeigi, A.; Mohammadi, A.; Sorooshian, A. Spatial trends, health risk assessment and ozone formation potential linked to BTEX. Hum. Ecol. Risk Assess. Int. J. 2019, 26, 2836–2857. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 7 April 2020).
- World Health Organization. Cleaning and Disinfection of Environmental Surfaces in the Context of COVID-19. 2020. Available online: https://www.who.int/publications/i/item/cleaning-and-disinfection-of-environmental-surfaces-inthe-context-of-covid-19 (accessed on 7 April 2020).
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef]
- Minhas, S.; Chaudhry, R.M.; Sajjad, A.; Manzoor, I.; Masood, A.; Kashif, M. Corona pandemic: Awareness of health care providers in Pakistan. Aims Public Health 2020, 7, 548. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, M.R.; Fouladi-Fard, R.; Omidi Oskouei, A.; Balali, M.; Ebrahimi, A.A.; Aali, R. Behavior and Knowledge of the Citizens about Ultra Violet Radiation in a Semi-arid Region in Iran. Arch. Hyg. Sci. 2020, 9, 193–204. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.A.; Da Molin, G.; De Giglio, O.; Caggiano, G.; Di Onofrio, V.; Ferracuti, S.; Montagna, M.T.; Liguori, G.; Orsi, G.B. Understanding Knowledge and Behaviors Related to CoViD–19 Epidemic in Italian Undergraduate Students: The EPICO Study. Int. J. Environ. Res. Public Health 2020, 17, 3481. [Google Scholar]
- Akalu, Y.; Ayelign, B.; Molla, M.D. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect. Drug Resist. 2020, 13, 1949. [Google Scholar] [CrossRef] [PubMed]
- Huynh, G.; Nguyen, T.N.H.; Vo, K.N.; Pham, L.A. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac. J. Trop. Med. 2020, 13, 260. [Google Scholar] [CrossRef]
- Lau, L.L.; Hung, N.; Go, D.J.; Ferma, J.; Choi, M.; Dodd, W.; Wei, X. Knowledge, attitudes and practices of COVID-19 among income-poor households in the Philippines: A cross-sectional study. J. Glob. Health 2020, 10, 011007. [Google Scholar] [CrossRef] [PubMed]
- Nemati, M.; Ebrahimi, B.; Nemati, F. Assessment of Iranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Arch. Clin. Infect. Dis. 2020, 15, e102848. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number | Percent |
|---|---|---|
| Sex | ||
| Male | 128 | 32 |
| Female | 246 | 61.5 |
| Missing values | 26 | 6.5 |
| Marital Status | ||
| Single | 51 | 12.75 |
| Married | 333 | 83.25 |
| Missing values | 16 | 4 |
| Age (Years) | ||
| 20–30 | 107 | 26.75 |
| 31–40 | 171 | 42.75 |
| 41–50 | 95 | 23.75 |
| 51–60 | 21 | 5.25 |
| 60+ | 3 | 0.75 |
| Missing values | 3 | 0.75 |
| Municipality Districts | ||
| 1 | 65 | 16.25 |
| 2 | 58 | 14.5 |
| 3 | 48 | 12 |
| 4 | 75 | 18.75 |
| 5 | 25 | 6.25 |
| 6 | 80 | 20 |
| 7 | 14 | 3.5 |
| 8 | 35 | 8.75 |
| Missing values | - | - |
| Education Level | ||
| No education | 8 | 2 |
| Junior High school | 74 | 18.5 |
| High school diploma | 143 | 35.75 |
| Bachelor | 127 | 31.75 |
| Master and Ph.D. | 44 | 11 |
| Missing values | 4 | 1 |
| Job Status | ||
| Self-employed | 80 | 20 |
| Governmental employee | 79 | 19.75 |
| Housewife | 192 | 48 |
| Student | 9 | 2.25 |
| Jobless | 10 | 2.5 |
| Missing values | 30 | 7.5 |
| Income Status | ||
| Less than 1 m * | 115 | 28.75 |
| 1–2 m | 120 | 30 |
| 2–5 m | 103 | 25.75 |
| 5–10 m | 12 | 3 |
| 10+ | 2 | 0.5 |
| Missing values | 48 | 12 |
| The Questions | Number | Percent |
|---|---|---|
| 1. Which alcohol is used as a disinfectant? | ||
| Ethanol | 197 | 49.25 |
| Methanol | 37 | 9.25 |
| Both | 44 | 11 |
| None | 39 | 9.75 |
| Do not know | 73 | 18.25 |
| Missing values | 10 | 2.5 |
| 2. Which one is used for surface disinfection? | ||
| Sodium hypochlorite | 155 | 38.75 |
| Perchlorine | 12 | 3 |
| Alcohol | 73 | 18.25 |
| All | 135 | 33.75 |
| Do not know | 21 | 5.25 |
| Missing values | 4 | 1 |
| 3. Which alcohol is an industrial alcohol which is toxic and deadly? | ||
| Methanol | 223 | 55.75 |
| Ethanol | 39 | 9.75 |
| Both | 29 | 7.25 |
| None | 7 | 1.75 |
| Do not know | 96 | 24 |
| Missing values | 6 | 1.5 |
| 4. How much chlorine is normally present in bleach? | ||
| 100% | 23 | 5.75 |
| 20% | 36 | 9 |
| 70% | 54 | 13.5 |
| 5% | 61 | 15.25 |
| Do not know | 220 | 55 |
| Missing values | 6 | 1.5 |
| 5. What is the ratio of bleach to water for making surface disinfection? | ||
| 1 to 5 | 165 | 41.25 |
| 1 to 2 | 9 | 2.25 |
| 3 to 1 | 18 | 4.5 |
| 1 to 50 | 165 | 41.25 |
| Do not know | 39 | 9.75 |
| Missing values | 4 | 1 |
| 6. For pre-disinfection of fruits and vegetables, how many minutes do they need to be in water and dishwashing liquid? | ||
| 5 to 10 | 199 | 49.75 |
| 2 to 5 | 118 | 29.5 |
| 60 | 8 | 2 |
| 30 | 39 | 9.75 |
| Do not know | 32 | 8 |
| Missing values | 4 | 1 |
| 7. How many dishwashing liquid drops are needed for pre-disinfection of fruits? | ||
| 1 to 3 | 285 | 71.25 |
| 7 to 10 | 54 | 13.5 |
| 20 to 30 | 10 | 2.5 |
| 15 to 20 | 5 | 1.25 |
| Do not know | 42 | 10.5 |
| Missing values | 4 | 1 |
| 8. Which one is the most effective concentration of alcohol for disinfection? | ||
| 96% | 43 | 10.75 |
| 70% | 246 | 61.5 |
| 0.50% | 8 | 2 |
| 1% | 11 | 2.75 |
| Do not know | 86 | 21.5 |
| Missing values | 6 | 1.5 |
| 9. How long can it take for the disinfectant solution prepared by chlorine to be used for disinfection? | ||
| 1 h | 32 | 8 |
| 24 h | 143 | 35.75 |
| 1 w | 33 | 8.25 |
| 1 m | 24 | 6 |
| Do not know | 161 | 40.25 |
| Missing values | 7 | 1.75 |
| 10. At which temperature do you use water to dilute disinfectant solution? | ||
| Warm | 36 | 9 |
| Cold | 182 | 45.5 |
| Tepid | 127 | 31.75 |
| None | 8 | 2 |
| Do not know | 43 | 10.75 |
| Missing values | 4 | 1 |
| Variables | Total Awareness * | Total Performance *** | ||||
|---|---|---|---|---|---|---|
| Mean | SD | p-Value ** | Mean | SD | p-Value ** | |
| Sex | 0.31 | 0.8 | ||||
| Men | 3.8 | 2.2 | 39.5 | 7.6 | ||
| Women | 4.7 | 2.1 | 40.6 | 7.6 | ||
| Marital Status | 0.06 | 0.77 | ||||
| Single | 4.3 | 1.9 | 38 | 7.5 | ||
| Married | 4.4 | 2.2 | 40.6 | 7.6 | ||
| Age | 0.04 | 0.1 | ||||
| 20–30 | 4 | 2.1 | 38.7 | 7.5 | ||
| 31–40 | 4.7 | 2 | 40.4 | 8.1 | ||
| 41–50 | 4.4 | 2.3 | 41.1 | 7.5 | ||
| 51–60 | 3.3 | 2.3 | 42.6 | 6.5 | ||
| 60+ | 4.3 | 1.2 | 43.3 | 5.6 | ||
| Municipality Districts | 0.00 | 0.01 | ||||
| 1st | 5.1 | 2.4 | 41.4 | 6.6 | ||
| 2nd | 4.3 | 1.8 | 39.3 | 8.3 | ||
| 3rd | 4.7 | 2.3 | 40.4 | 8.6 | ||
| 4th | 4.8 | 2.2 | 43 | 7.1 | ||
| 5th | 4.1 | 2.1 | 39.9 | 7.2 | ||
| 6th | 3.4 | 1.7 | 37.6 | 8.4 | ||
| 7th | 2.6 | 1.8 | 36.6 | 6.9 | ||
| 8th | 4.6 | 1.7 | 41.2 | 6.2 | ||
| Education Level | 0.00 | 0.01 | ||||
| No education | 3.2 | 2.2 | 30.4 | 8.7 | ||
| Junior high school | 3.7 | 2 | 38.6 | 8.2 | ||
| High school diploma | 4.1 | 2 | 40.4 | 7.6 | ||
| Bachelor | 4.7 | 2.3 | 41.1 | 7.7 | ||
| Master and Ph.D. | 5.34 | 2.1 | 41.5 | 6.1 | ||
| Job Status | 0.01 | 0.01 | ||||
| Self-Employed | 3.8 | 2.1 | 38.1 | 8.5 | ||
| Governmental-employee | 4.8 | 2.1 | 41.4 | 6.9 | ||
| Housewife | 4.6 | 2 | 40.7 | 7.7 | ||
| Student | 5 | 2.6 | 41.5 | 4.9 | ||
| Jobless | 3.9 | 2.3 | 35.3 | 8.2 | ||
| Income Status | ||||||
| Less Than 1 m | 4.4 | 2.2 | 0.53 | 39.9 | 8.1 | 0.33 |
| 1–2 m | 4.1 | 2.1 | 39 | 8.5 | ||
| 2–5 m | 4.5 | 2.3 | 41.1 | 6.2 | ||
| 5–10 m | 4.5 | 1.7 | 42 | 8.9 | ||
| Above10 | 3 | 2.8 | 41 | 4.2 | ||
| Total | 4.4 | 2.2 | 40.2 | 7.8 | ||
| Municipality District | Population | Patient | Incidence |
|---|---|---|---|
| 1 | 192,060 | 209 | 10.9 |
| 2 | 189,708 | 112 | 5.9 |
| 3 | 171,363 | 213 | 12.4 |
| 4 | 192,755 | 160 | 8.3 |
| 5 | 78,401 | 72 | 9.2 |
| 6 | 213,356 | 177 | 8.3 |
| 7 | 41,625 | 64 | 15.3 |
| 8 | 121,890 | 44 | 3.6 |
| Municipality | Standard Error | p-Value | 95% Confidence Interval | ||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| 7 | 1 | 0.64 | 0.00 | −3.86 | −1.34 |
| 2 | 0.65 | 0.01 | −2.98 | −0.43 | |
| 3 | 0.66 | 0.001 | −3.44 | −0.84 | |
| 4 | 0.63 | 0.00 | −3.54 | −1.05 | |
| 5 | 0.73 | 0.03 | −3.02 | −0.16 | |
| 6 | 0.63 | 0.05 | −2.13 | 0.35 | |
| 8 | 0.69 | 0.00 | −3.44 | −0.74 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Safari, Z.; Fouladi-Fard, R.; Vahidmoghadam, R.; Hosseini, M.R.; Mohammadbeigi, A.; Omidi Oskouei, A.; Rezaali, M.; Ferrante, M.; Fiore, M. Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran. Int. J. Environ. Res. Public Health 2021, 18, 2099. https://doi.org/10.3390/ijerph18042099
Safari Z, Fouladi-Fard R, Vahidmoghadam R, Hosseini MR, Mohammadbeigi A, Omidi Oskouei A, Rezaali M, Ferrante M, Fiore M. Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran. International Journal of Environmental Research and Public Health. 2021; 18(4):2099. https://doi.org/10.3390/ijerph18042099
Chicago/Turabian StyleSafari, Zahra, Reza Fouladi-Fard, Razieh Vahidmoghadam, Mohammad Raza Hosseini, Abolfazl Mohammadbeigi, Alireza Omidi Oskouei, Mostafa Rezaali, Margherita Ferrante, and Maria Fiore. 2021. "Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran" International Journal of Environmental Research and Public Health 18, no. 4: 2099. https://doi.org/10.3390/ijerph18042099
APA StyleSafari, Z., Fouladi-Fard, R., Vahidmoghadam, R., Hosseini, M. R., Mohammadbeigi, A., Omidi Oskouei, A., Rezaali, M., Ferrante, M., & Fiore, M. (2021). Awareness and Performance towards Proper Use of Disinfectants to Prevent COVID-19: The Case of Iran. International Journal of Environmental Research and Public Health, 18(4), 2099. https://doi.org/10.3390/ijerph18042099