
Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Internet Survey
2.2. Symptoms from Exposure to Secondhand Combustible Cigarette Smoke and HTP Aerosol
‘Have you inhaled the smoke of combustible cigarettes that other people were smoking within this one year?’ Response options were ‘never, 1–4 times, or 5 or more times.’
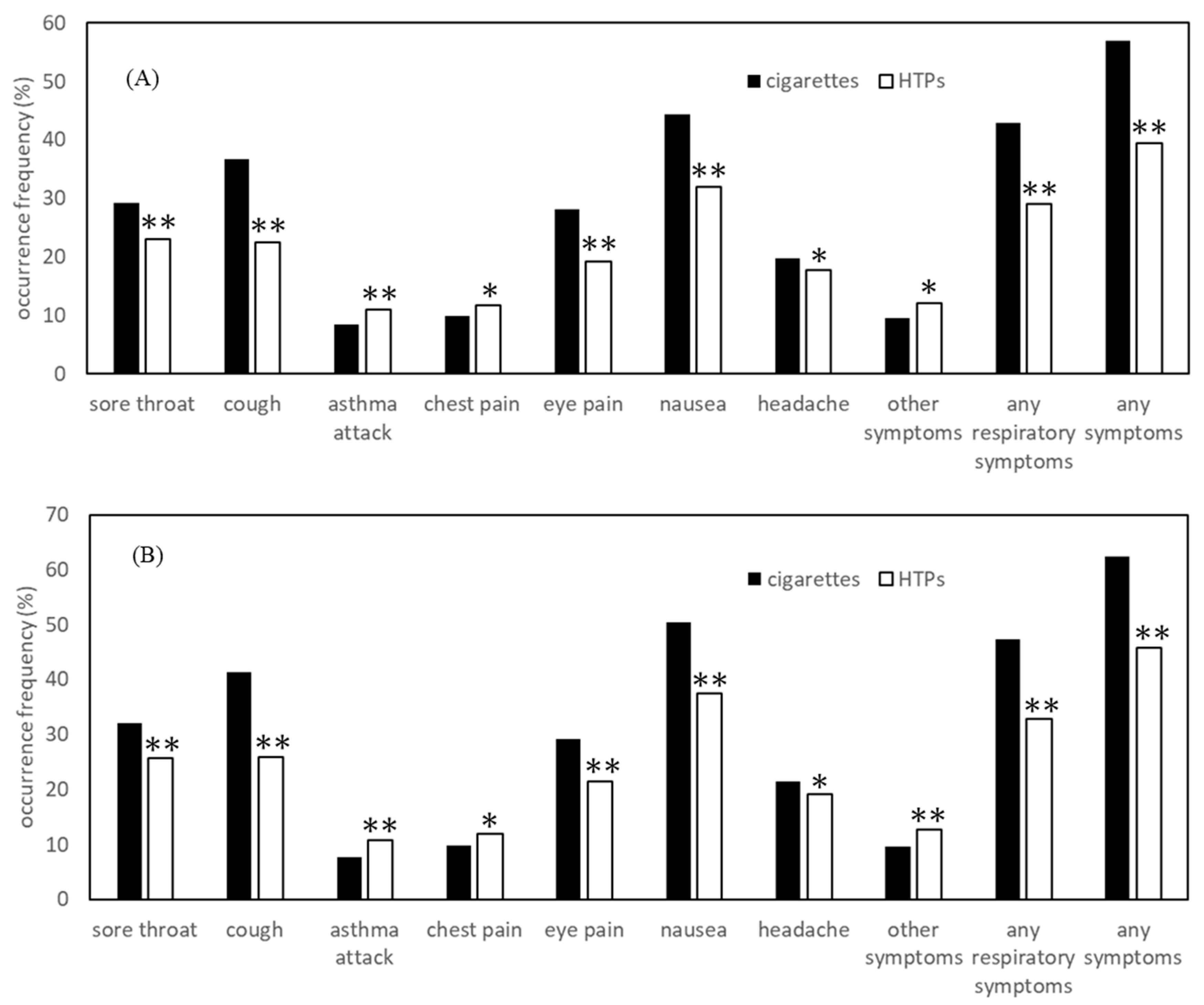
‘Within this one year, have you experienced sore throat/cough/asthma attack/chest pain/eye pain/nausea/headache/other symptoms, after inhaling the smoke of combustible cigarette that other people were producing?’ Response options were ‘no, 1–4 times, or 5 or more times’.
2.3. Characteristic Variables
2.4. Statistical Analysis
3. Results
3.1. Percentages of Secondhand Exposure
3.2. Symptoms Associated with Secondhand Exposure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- US Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General 2006; US Department of Health and Human Services: Washington, DC, USA, 2006.
- US Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General 2014; US Department of Health and Human Services: Washington, DC, USA, 2014.
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Simonavicius, E.; McNeill, A.; Shahab, L.; Brouse, L.S. Heat-not-burn tobacco products: A systematic literature review. Tob. Control 2019, 28, 582–594. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare National Health and Nutrition Examination Survey. Available online: https://www.mhlw.go.jp/stf/newpage_14156.html (accessed on 23 November 2020).
- Hori, A.; Tabuchi, T.; Kunugita, N. Rapid increase in heated tobacco product (HTP) use from 2015 to 2019: From the Japan ’Society and New Tobacco’ Internet Survey (JASTIS). Tob. Control 2020. [Google Scholar] [CrossRef] [PubMed]
- Tabuchi, T.; Gallus, S.; Shinozaki, T.; Nakaya, T.; Kunugita, N.; Colwell, B. Heat-not-burn tobacco product use in Japan: Its prevalence, predictors and perceived symptoms from exposure to secondhand heat-not-burn tobacco aerosol. Tob. Control 2018, 27, e25–e33. [Google Scholar] [CrossRef] [PubMed]
- Kato, T.; Endo, A. Involving citizens in sharing disaster experiences across areas: An investigation into disaster-stricken communities and observing communities. Int. J. Disaster Risk Reduct. 2020, 42, 101378. [Google Scholar] [CrossRef]
- Tabuchi, T.; Shinozaki, T.; Kunugita, N.; Nakamura, M.; Tsuji, I. Study Profile: The Japan “Society and New Tobacco” Internet Survey (JASTIS): A Longitudinal Internet Cohort Study of Heat-Not-Burn Tobacco Products, Electronic Cigarettes, and Conventional Tobacco Products in Japan. J. Epidemiol. 2019, 29, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Kiyohara, K.; Tabuchi, T. Use of heated tobacco products in smoke-free locations in Japan: The JASTIS 2019 study. Tob. Control 2020. [Google Scholar] [CrossRef] [PubMed]
- Perkins, K.A.; Epstein, L.H.; Jennings, J.R.; Stiller, R. The cardiovascular effects of nicotine during stress. Psychopharmacology 1986, 90, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama, S.; Noguchi, M.; Takagi, N.; Hayashida, H.; Inaba, Y.; Ogura, H.; Kunugita, N. Simple determination of gaseous and particulate compounds generated from heated tobacco products. Chem. Res. Toxicol. 2018, 31, 585–593. [Google Scholar] [CrossRef] [PubMed]
- St Helen, G.; Jacob, P.; Nardone, N.; Benowitz, N.L. IQOS: Examination of Philip Morris International’s claim of reduced exposure. Tob. Control 2018, 27, s30–s36. [Google Scholar] [CrossRef] [PubMed]
- Davis, B.; To, V.; Talbot, P. Comparison of cytotoxicity of IQOS aerosols to smoke from Marlboro Red and 3R4F reference cigarettes. Toxicol. In Vitro 2019, 61, 104652. [Google Scholar] [CrossRef] [PubMed]
- Stephens, W.E. Comparing the cancer potencies of emissions from vapourised nicotine products including e-cigarettes with those of tobacco smoke. Tob. Control 2017, 27, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Pisinger, C.; Døssing, M. A systematic review of health effects of electronic cigarettes. Prev. Med. 2014, 69, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Shields, P.G.; Berman, M.; Brasky, T.M.; Freudenheim, J.L.; Mathe, E.; McElroy, J.P.; Song, M.A.; Wewers, M.D. A review of pulmonary toxicity of electronic cigarettes in the context of smoking: A focus on inflammation. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1175–1191. [Google Scholar] [CrossRef] [PubMed]
- McConnell, R.; Barrington-Trimis, J.L.; Wang, K.; Urman, R.; Hong, H.; Unger, J.; Samet, J.; Leventhal, A.; Berhane, K. Electronic cigarette use and respiratory symptoms in adolescents. Am. J. Respir. Crit. Care Med. 2017, 195, 1043–1049. [Google Scholar] [CrossRef] [PubMed]
- Osei, A.D.; Mirbolouk, M.; Orimoloye, O.A.; Dzaye, O.; Uddin, S.M.I.; Dardari, Z.A.; DeFilippis, A.P.; Bhatnagar, A.; Blaha, M.J. The association between e-cigarette use and asthma among never combustible cigarette smokers: Behavioral risk factor surveillance system (BRFSS) 2016 & 2017. BMC Pulm. Med. 2019, 19, 180. [Google Scholar] [CrossRef]
- Layden, J.E.; Ghinai, I.; Pray, I.; Kimball, A.; Layer, M.; Tenforde, M.W.; Navon, L.; Hoots, B.; Salvatore, P.P.; Elderbrook, M.; et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin—Preliminary Report. N. Engl. J. Med. 2020, 382, 903–916. [Google Scholar] [CrossRef] [PubMed]
- Tabuchi, T.; Nakamura, M. Disparity of secondhand smoke exposure at home and/or workplace according to age, education and medical insurance in Japan. JACR Monogr. 2014, 20, 39–48. [Google Scholar]
- Tabuchi, T.; Hoshino, T.; Nakayama, T. Are Partial Workplace Smoking Bans as Effective as Complete Smoking Bans? A National Population-Based Study of Smoke-Free Policy among Japanese Employees. Nicotine Tob. Res. 2016, 18, 1265–1273. [Google Scholar] [CrossRef] [PubMed]
- Gorukanti, A.; Delucchi, K.; Ling, P.; Fisher-Travis, R.; Halpern-Felsher, B. Adolescents’ attitudes towards e-cigarette ingredients, safety, addictive properties, social norms, and regulation. Prev. Med. 2017, 94, 65–71. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total | Secondhand Cigarette Smoke Exposure | Secondhand HTP Aerosol Exposure | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Total | 8784 | 100.0 | 5142 | 58.5 | 2923 | 33.3 |
| Sex | ||||||
| Man | 4286 | 48.8 | 2583 | 60.3* | 1606 | 37.5 ** |
| Woman | 4498 | 51.2 | 2559 | 56.9 | 1317 | 29.3 |
| Age group, years | ||||||
| 15–19 | 853 | 9.7 | 483 | 56.6 ** | 278 | 32.6 ** |
| 20–29 | 1539 | 17.5 | 883 | 57.4 | 606 | 39.4 |
| 30–39 | 1373 | 15.6 | 807 | 58.8 | 527 | 38.4 |
| 40–49 | 1650 | 18.8 | 1002 | 60.7 | 603 | 36.5 |
| 50–59 | 1507 | 17.2 | 952 | 63.2 | 501 | 33.2 |
| 60– | 1862 | 21.2 | 1015 | 54.5 | 408 | 21.9 |
| Current cigarette smoker | ||||||
| No | 7482 | 85.2 | 4129 | 55.2 ** | 2267 | 30.3 ** |
| Yes | 1302 | 14.8 | 1013 | 77.8 | 656 | 50.4 |
| Current HTP user | ||||||
| No | 7993 | 91.0 | 4554 | 57.0 ** | 2412 | 30.2 ** |
| Yes | 791 | 9.0 | 588 | 74.3 | 511 | 64.6 |
| Education | ||||||
| High school/less | 2874 | 32.7 | 1616 | 56.2 ** | 868 | 30.2 ** |
| 2-year-college | 1752 | 19.9 | 974 | 55.6 | 520 | 29.7 |
| University/more | 4158 | 47.3 | 2552 | 61.4 | 1535 | 36.9 |
| Marital status | ||||||
| Married | 4492 | 51.1 | 2674 | 59.5 | 1461 | 32.5 * |
| Unmarried | 3740 | 42.6 | 2158 | 57.7 | 1302 | 34.8 |
| Divorced/widowed | 552 | 6.3 | 310 | 56.2 | 160 | 29.0 |
| Self-related health | ||||||
| Good | 7778 | 88.5 | 4568 | 58.7 | 2617 | 33.6 * |
| Poor | 1006 | 11.5 | 574 | 57.1 | 306 | 30.4 |
| Sore Throat | Cough | Asthma Attack | Chest Pain | Respiratory Symptoms | Any Symptom | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cig | HTP | Cig | HTP | Cig | HTP | Cig | HTP | Cig | HTP | Cig | HTP | |
| Total | 29.2 | 23.0 | 36.8 | 22.5 | 8.4 | 10.9 | 9.9 | 11.8 | 42.8 | 29.0 | 56.8 | 39.5 |
| Sex | ||||||||||||
| Man | 26.9 ** | 22.4 | 30.8 ** | 20.5 * | 9.9 ** | 12.6 * | 11.0 * | 13.1 * | 36.9 ** | 26.8* | 49.6 ** | 35.6 ** |
| Woman | 31.5 | 23.6 | 42.8 | 25.0 | 6.8 | 8.9 | 8.7 | 10.3 | 48.8 | 31.6 | 64.2 | 44.2 |
| Age group, years | ||||||||||||
| 15–19 | 32.5 ** | 30.2 ** | 58.0 ** | 36.7 ** | 10.6 ** | 16.5 ** | 15.5 ** | 16.9 ** | 63.1 ** | 44.6 ** | 78.9 ** | 61.5 ** |
| 20–29 | 34.1 | 27.6 | 45.3 | 28.7 | 12.1 | 15.0 | 14.0 | 15.7 | 51.9 | 37.1 | 66.9 | 50.0 |
| 30–39 | 30.0 | 24.1 | 36.4 | 24.1 | 9.0 | 10.6 | 10.5 | 13.3 | 43.7 | 29.6 | 57.5 | 40.8 |
| 40–49 | 31.2 | 21.6 | 33.5 | 17.7 | 8.8 | 10.0 | 10.8 | 10.9 | 40.4 | 25.0 | 55.3 | 33.3 |
| 50–59 | 25.8 | 19.6 | 29.9 | 17.0 | 7.0 | 8.4 | 7.0 | 8.2 | 35.4 | 21.8 | 48.0 | 30.5 |
| 60– | 23.7 | 15.9 | 29.2 | 15.7 | 4.3 | 6.1 | 4.7 | 6.4 | 34.0 | 20.1 | 46.9 | 27.2 |
| Current cigarette smoker | ||||||||||||
| No | 32.2 ** | 24.9 ** | 41.4 ** | 24.9 ** | 8.1 | 10.9 | 10.1 | 11.8 | 47.5 ** | 31.6 ** | 62.6 ** | 43.8 ** |
| Yes | 16.8 | 16.2 | 18.1 | 14.5 | 9.6 | 11.3 | 9.0 | 11.7 | 23.9 | 19.8 | 33.4 | 24.5 |
| Current HTP user | ||||||||||||
| No | 29.5 | 23.6 | 38.0 ** | 23.7 * | 7.3 ** | 10.2 * | 9.1 ** | 11.3 | 43.9 ** | 30.0 * | 58.4 ** | 42.3 ** |
| Yes | 26.4 | 20.0 | 27.0 | 17.0 | 16.8 | 14.5 | 15.6 | 14.1 | 35.0 | 24.1 | 45.1 | 26.2 |
| Education | ||||||||||||
| High school/less | 29.8 | 24.4 | 39.7 * | 25.1 | 9.4 * | 12.9 * | 10.7 | 12.9 | 44.9 | 31.6 | 58.2 | 42.5 |
| 2-year-college | 27.6 | 22.9 | 35.2 | 21.5 | 6.4 | 8.5 | 8.4 | 11.9 | 40.2 | 27.3 | 54.1 | 36.3 |
| University/more | 29.3 | 22.1 | 35.5 | 21.4 | 8.5 | 10.7 | 9.9 | 11.1 | 42.5 | 28.1 | 57.0 | 38.8 |
| Marital status | ||||||||||||
| Married | 28.9 | 21.4 * | 32.9 ** | 19.9 ** | 7.8 ** | 10.1 * | 8.7 ** | 10.7 * | 39.4 ** | 26.1 ** | 53.3 ** | 34.8 ** |
| Unmarried | 30.3 | 25.4 | 42.3 | 26.5 | 9.7 | 12.4 | 12.0 | 13.6 | 48.0 | 33.2 | 62.5 | 46.0 |
| Divorced/widowed | 23.9 | 17.5 | 31.3 | 14.4 | 4.2 | 6.9 | 5.2 | 7.5 | 36.5 | 20.6 | 48.7 | 28.8 |
| Self-related health | ||||||||||||
| Good | 27.9 ** | 22.0 * | 35.6 ** | 21.7 ** | 7.8 ** | 10.5 * | 9.4 * | 11.3 * | 41.7 ** | 28.2 ** | 56.3 * | 38.7 ** |
| Poor | 39.0 | 31.0 | 45.8 | 29.7 | 13.1 | 15.0 | 13.6 | 16.0 | 51.6 | 35.6 | 61.3 | 46.1 |
| Eye Pain | Nausea | Headache | Other Symptoms | |||||
|---|---|---|---|---|---|---|---|---|
| Cig | HTP | Cig | HTP | Cig | HTP | Cig | HTP | |
| Total | 28.2 | 19.3 | 44.4 | 31.9 | 19.8 | 17.7 | 9.5 | 12.0 |
| Sex | ||||||||
| Man | 28.0 | 20.1 | 37.8 ** | 29.1 ** | 18.0 * | 17.7 | 11.0 ** | 13.4 * |
| Woman | 28.4 | 18.2 | 51.1 | 35.4 | 21.6 | 17.7 | 8.1 | 10.3 |
| Age group, years | ||||||||
| 15–19 | 32.9 ** | 23.4 ** | 65.8 ** | 50.4 ** | 32.1 ** | 26.6 ** | 12.2 ** | 15.8 ** |
| 20–29 | 30.6 | 23.8 | 52.1 | 39.4 | 25.0 | 23.6 | 12.5 | 16.0 |
| 30–39 | 30.7 | 21.6 | 45.0 | 34.3 | 22.3 | 19.2 | 10.0 | 12.0 |
| 40–49 | 32.9 | 18.6 | 42.7 | 27.9 | 20.9 | 16.6 | 10.8 | 11.3 |
| 50–59 | 24.6 | 15.0 | 38.3 | 24.8 | 16.6 | 12.8 | 8.1 | 10.2 |
| 60– | 20.5 | 13.0 | 34.5 | 19.9 | 9.4 | 8.6 | 5.5 | 6.9 |
| Current cigarette smoker | ||||||||
| No | 29.7 ** | 20.7 ** | 50.4 ** | 35.8 ** | 21.8 ** | 18.7 * | 10.0 * | 12.5 |
| Yes | 22.1 | 14.3 | 20.0 | 18.6 | 11.7 | 14.3 | 7.8 | 10.2 |
| Current HTP user | ||||||||
| No | 27.9 | 19.7 | 46.1 ** | 34.5 ** | 19.7 | 17.7 | 8.9 ** | 11.7 |
| Yes | 30.6 | 17.2 | 31.6 | 20.0 | 20.6 | 17.8 | 14.3 | 13.5 |
| Education | ||||||||
| High school/less | 29.3 | 19.7 | 44.7 | 34.6 | 21.2 | 19.4 | 9.5 | 12.8 |
| 2-year-college | 25.6 | 17.9 | 41.7 | 30.6 | 17.8 | 16.3 | 8.4 | 11.0 |
| University/more | 28.4 | 19.5 | 45.3 | 30.9 | 19.7 | 17.2 | 10.0 | 11.9 |
| Marital status | ||||||||
| Married | 27.0* | 17.7 * | 41.3 ** | 27.6 ** | 17.5 ** | 15.4 ** | 8.8 * | 11.0 |
| Unmarried | 30.2 | 21.9 | 49.2 | 37.8 | 23.2 | 21.1 | 10.9 | 13.4 |
| Divorced/widowed | 24.8 | 12.5 | 38.1 | 23.8 | 15.8 | 10.6 | 6.8 | 10.0 |
| Self-related health | ||||||||
| Good | 27.4 ** | 18.5 * | 43.7 * | 31.1 * | 19.1 * | 16.7 ** | 9.2 * | 11.6 * |
| Poor | 34.5 | 25.5 | 50.3 | 38.6 | 25.3 | 26.5 | 12.4 | 15.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imura, Y.; Tabuchi, T. Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study. Int. J. Environ. Res. Public Health 2021, 18, 1766. https://doi.org/10.3390/ijerph18041766
Imura Y, Tabuchi T. Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study. International Journal of Environmental Research and Public Health. 2021; 18(4):1766. https://doi.org/10.3390/ijerph18041766
Chicago/Turabian StyleImura, Yuki, and Takahiro Tabuchi. 2021. "Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study" International Journal of Environmental Research and Public Health 18, no. 4: 1766. https://doi.org/10.3390/ijerph18041766
APA StyleImura, Y., & Tabuchi, T. (2021). Exposure to Secondhand Heated-Tobacco-Product Aerosol May Cause Similar Incidence of Asthma Attack and Chest Pain to Secondhand Cigarette Exposure: The JASTIS 2019 Study. International Journal of Environmental Research and Public Health, 18(4), 1766. https://doi.org/10.3390/ijerph18041766