
Comparing the Efficacy of Multidisciplinary Assessment and Treatment, or Acceptance and Commitment Therapy, with Treatment as Usual on Health Outcomes in Women on Long-Term Sick Leave—A Randomised Controlled Trial

 ,
,
Abstract
1. Introduction
2. Materials and Methods
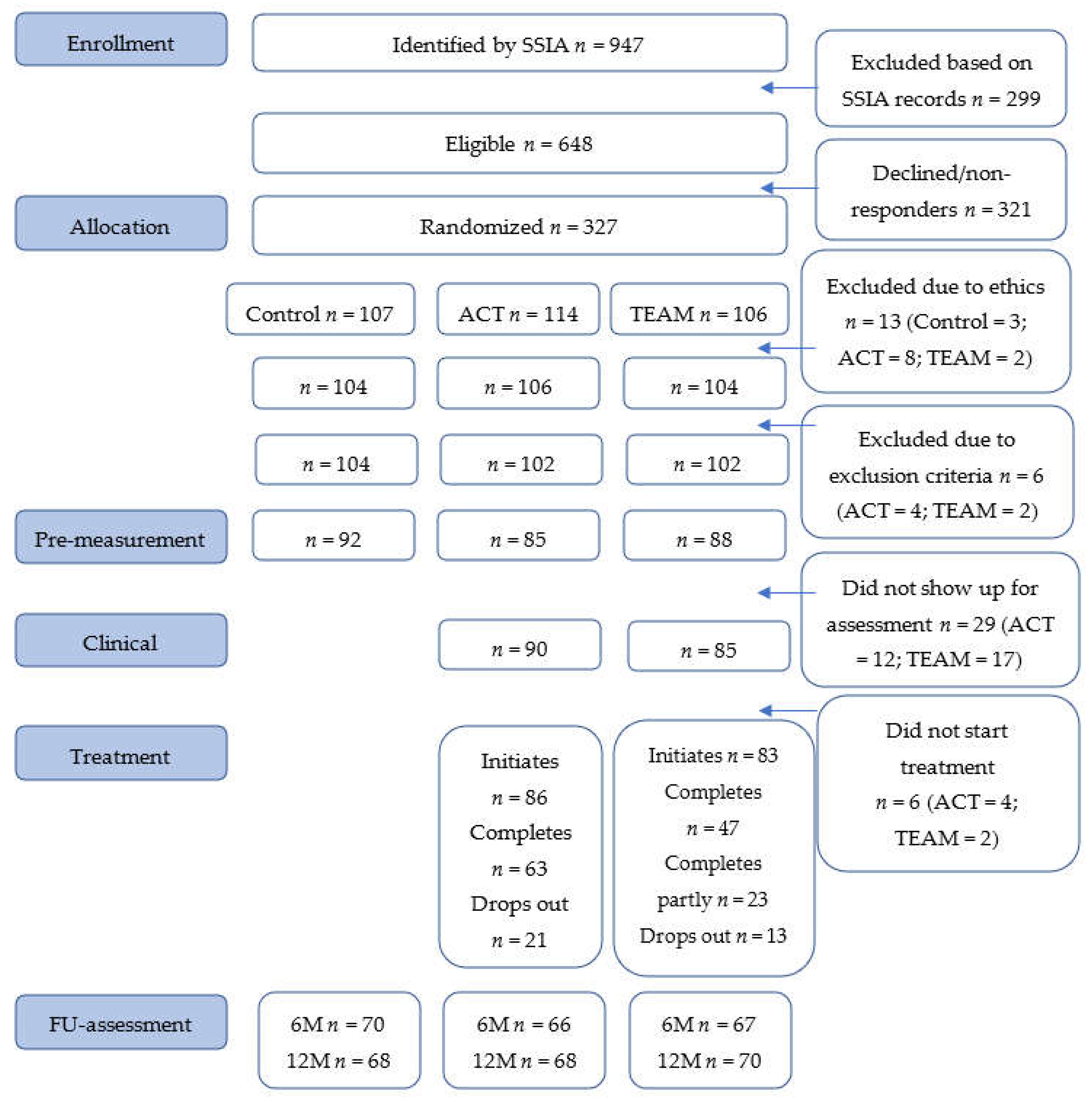
2.1. Design and Study Population
2.2. Inclusion and Exclusion Ciriteria
2.3. Randomization Procedure
2.4. Interventions
2.4.1. Collaboration with Other Authorities
2.4.2. Acceptance and Commitment Therapy
2.4.3. Multidisciplinary Assessment and Treatment
2.4.4. Control Group
2.5. Measures
2.6. Statistical and Data Analysis
2.7. Ethical Considerations and Trial Registration
3. Results
3.1. Sociodemographic and Pre-Treatment Data
3.2. Treatment Duration and Satisfaction with Treatment
3.3. Clinical Efficacy
3.4. Missing Data
3.5. Clinically Significant Change
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Henderson, M.; Harvey, S.B.; Overland, S.; Mykletun, A.; Hotopf, M. Work and common psychiatric disorders. J. R. Soc. Med. 2011, 104, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Linder, J.; Ekholm, K.S.; Jansen, G.B.; Lundh, G.; Ekholm, J. Long-term sick leavers with difficulty in resuming work: Comparisons between psychiatric-somatic comorbidity and monodiagnosis. Int. J. Rehabil. Res. 2009, 32, 20–35. [Google Scholar] [PubMed]
- Fishbain, D.A.; Cutler, R.; Rosomoff, H.L.; Rosomoff, R.S. Chronic pain-associated depression: Antecedent or consequence of chronic pain? A review. Clin. J. Pain 1997, 13, 116–137. [Google Scholar] [CrossRef]
- Jensen, I.B.; Bergstrom, G.; Ljungquist, T.; Bodin, L. A 3-year follow-up of a multidisciplinary rehabilitation programme for back and neck pain. Pain 2005, 115, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Swedish Council on Health Technology Assessment [SBU]. Rehabilitation of Patients with Chronic Pain Conditions A Systematic Review; Report No.: 198; SBU Stockholm: Stockholm, Sweden, 2010.
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.H.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of Workplace Interventions in Return-to-Work for Musculoskeletal, Pain-Related and Mental Health Conditions: An Update of the Evidence and Messages for Practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef]
- Momsen, A.H.; Stapelfeldt, C.M.; Nielsen, C.V.; Nielsen, M.B.; Aust, B.; Rugulies, R.; Jensen, C. Effects of a randomized controlled intervention trial on return to work and health care utilization after long-term sickness absence. BMC Public Health 2016, 16, 1149. [Google Scholar] [CrossRef] [PubMed]
- Finnes, A.; Enebrink, P.; Ghaderi, A.; Dahl, J.; Nager, A.; Öst, L.G. Psychological treatments for return to work in individuals on sickness absence due to common mental disorders or musculoskeletal disorders: A systematic review and meta-analysis of randomized-controlled trials. Int. Arch. Occup. Environ. Health 2019, 92, 273–293. [Google Scholar] [CrossRef]
- Newby, J.M.; McKinnon, A.; Kuyken, W.; Gilbody, S.; Dalgleish, T. Systematic review and meta-analysis of transdiagnostic psychological treatments for anxiety and depressive disorders in adulthood. Clin. Psychol. Rev. 2015, 40, 91–110. [Google Scholar] [CrossRef] [PubMed]
- Veehof, M.M.; Oskam, M.J.; Schreurs, K.M.; Bohlmeijer, E.T. Acceptance-based interventions for the treatment of chronic pain: A systematic review and meta-analysis. Pain 2011, 152, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Swain, J.; Hancock, K.; Hainsworth, C.; Bowman, J. Acceptance and commitment therapy in the treatment of anxiety: A systematic review. Clin. Psychol. Rev. 2013, 33, 965–978. [Google Scholar] [CrossRef]
- Hacker, T.; Stone, P.; MacBeth, A. Acceptance and commitment therapy—Do we know enough? Cumulative and sequential meta-analyses of randomized controlled trials. J. Affect. Disord. 2016, 190, 551–565. [Google Scholar] [CrossRef] [PubMed]
- A-Tjak, J.G.; Davis, M.L.; Morina, N.; Powers, M.B.; Smits, J.A.; Emmelkamp, P.M. A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychother. Psychosom. 2015, 84, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Twohig, M.P.; Levin, M.E. Acceptance and Commitment Therapy as a Treatment for Anxiety and Depression: A Review. Psychiatr. Clin. N. Am. 2017, 40, 751–770. [Google Scholar] [CrossRef] [PubMed]
- Dahl, J.; Wilson, K.G.; Nilsson, A. Acceptance and commitment therapy and the treatment of persons at risk for long-term disability resulting from stress and pain symptoms: A preliminary randomized trial. Behav. Ther. 2004, 35, 785–801. [Google Scholar] [CrossRef]
- Finnes, A.; Ghaderi, A.; Dahl, J.; Nager, A.; Enebrink, P. Randomized Controlled Trial of Acceptance and Commitment Therapy and a Workplace Intervention for Sickness Absence Due to Mental Disorders. J. Occup. Health Psychol. 2017, 24, 198–212. [Google Scholar] [PubMed]
- Lytsy, P.; Carlsson, L.; Anderzen, I. Effectiveness of two vocational rehabilitation programmes in women with long-term sick leave due to pain syndrome or mental illness: 1-year follow-up of a randomized controlled trial. J. Rehabil. Med. 2017, 49, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Riksrevisionen [The Swedish National Audit Office]. En Förändrad Sjukskrivningsprocess [An Altered Sickness Absence Process]; Riksdagstryckeriet: Stockholm, Sweden, 2010. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Harnett-Sheehan, K.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic interview. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar] [PubMed]
- Linton, S.J.; Hallden, K. Can we screen for problematic back pain? A screening questionnaire for predicting outcome in acute and subacute back pain. Clin. J. Pain 1998, 14, 209–215. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction With Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E.; Colvin, C.R.; Sandvik, E. Further validation of the Satisfaction with Life Scale: Evidence for the cross-method convergence of well-being measures. J. Pers. Assess. 1991, 57, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Blackwell, B. Psychiatric illness in general practice. A detailed study using a new method of case identification. Br. Med. J. 1970, 1, 439–443. [Google Scholar] [PubMed]
- McCabe, C.J.; Thomas, K.J.; Brazier, J.E.; Coleman, P. Measuring the mental health status of a population: A comparison of the GHQ-12 and the SF-36 (MHI-5). Br. J. Psychiatry 1996, 169, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, N.; Kruse, J.; Tress, W. Psychometric properties of the General Health Questionnaire (GHQ-12) in a German primary care sample. Acta Psychiatr. Scand. 1999, 100, 462–468. [Google Scholar] [CrossRef]
- Bates, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using Ime4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate imputation by Chained Equations. R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef]
- Reme, S.E.; Grasdal, A.L.; Lovvik, C.; Lie, S.A.; Overland, S. Work-focused cognitive-behavioural therapy and individual job support to increase work participation in common mental disorders: A randomised controlled multicentre trial. Occup. Environ. Med. 2015, 72, 745–752. [Google Scholar]



{kind=link}
{kind=link}
| Control | ACT | TEAM | |
|---|---|---|---|
| n = 104 | n = 102 | n = 102 | |
| Age mean (sd) | 47.5 (8.34) | 47.8 (7.76) | 49.9 (8.74) |
| Education n (%) | |||
| Primary school | 21 (22.8) | 17 (19.5) | 24 (27.3) |
| Secondary school | 39 (42.4) | 37 (42.5) | 38 (43.2) |
| University education | 32 (34.8) | 33 (37.9) | 26 (29.5) |
| Born outside Sweden n (%) | 22 (24.2) | 17 (19.5) | 15 (16.9) |
| Unemployed n (%) | 37 (35.6) | 43 (42.2) | 33 (32.4) |
| Diagnosis n (%) | |||
| Psychiatric diagnosis | 31 (29.8) | 41 (40.2) | 27 (26.5) |
| Pain diagnosis | 39 (37.5) | 34 (33.3) | 34 (33.3) |
| Psychiatric and pain diagnosis | 34 (32.7) | 25 (24.5) | 40 (39.2) |
| Other diagnosis | 0 (0.0) | 2 (2.0) | 1 (1.0) |
| Years of sick leave (mean (sd)) | 7.52 (3.36) | 7.57 (3.15) | 7.50 (3.08) |
| Reimbursement n (%) | |||
| 25% | 13 (12.6) | 15 (14.7) | 12 (11.9) |
| 50% | 31 (30.1) | 23 (22.5) | 33 (32.7) |
| 75% | 5 (4.9) | 9 (8.8) | 8 (7.9) |
| 100% | 54 (52.4) | 55 (53.9) | 48 (47.5) |
| Baseline | 6 Months | 12 Months | ||||
|---|---|---|---|---|---|---|
| Pain | n | M (SD) | n | M (SD) | n | M (SD) |
| ACT | 71 | 6.08 (1.98) | 43 | 5.67 (2.15) | 33 | 4.63 (2.90) |
| TEAM | 83 | 6.13 (2.05) | 38 | 5.59 (2.11) | 32 | 5.07 (2.77) |
| Control | 88 | 6.53 (2.11) | 38 | 6.83(1.67) | 35 | 5.91 (2.65) |
| HADS anxiety | ||||||
| ACT | 19 | 10.05 (4.91) | 35 | 9.00 (5.16) | 34 | 8.70 (5.15) |
| TEAM | 17 | 10.31 (4.79) | 35 | 8.83 (4.78) | 31 | 7.37 (4.51) |
| Control | 12 | 11.09 (5.08) | 33 | 11.37 (5.14) | 35 | 10.71 (5.48) |
| HADS depression | ||||||
| ACT | 85 | 8.45 (4.19) | 65 | 7.37 (5.04) | 67 | 7.06 (4.67) |
| TEAM | 86 | 9.22 (4.46) | 66 | 7.70 (4.87) | 70 | 6.56 (4.81) |
| Control | 91 | 9.22 (5.13) | 70 | 9.54 (5.22) | 67 | 9.48 (5.11) |
| SWLS | ||||||
| ACT | 83 | 16.72 (7.05) | 64 | 17.12 (7.53) | 67 | 17.40 (7.91) |
| TEAM | 88 | 15.26 (7.05) | 67 | 17.70 (7.81) | 69 | 18.94 (7.70) |
| Control | 91 | 14.51 (7.48) | 70 | 14.06 (6.61) | 66 | 14.33 (6.92) |
| GHQ | ||||||
| ACT | 84 | 18.80 (7.50) | 63 | 20.86 (7.52) | 66 | 20.85 (7.80) |
| TEAM | 87 | 17.25 (7.86) | 67 | 20.40 (7.54) | 66 | 22.20 (7.24) |
| Control | 92 | 16.43 (7.14) | 70 | 16.10 (7.22) | 69 | 16.88 (8.27) |
| Crude Linear Model on Original Data | Crude Linear Mixed Model on Imputed Data | Adjusted Linear Mixed Model on Imputed Data | |
|---|---|---|---|
| MD (CI) | MD (CI) | MD (CI) | |
| Pain | |||
| ACT | −1.28 ** (−2.22, −0.34) | −1.2 ** (−1.93, −0.48) | −1.16 ** (−1.85, −0.47) |
| TEAM | −0.84 (−1.77, 0.1) | −0.76 * (−1.5, −0.02) | −0.73 * (−1.45, −0.02) |
| HADS anxiety | |||
| ACT | −2 * (−3.72, −0.29) | −2.54 ** (−4.17, −0.91) | −2.78 *** (−4.34, −1.23) |
| TEAM | −3.33 ** (−5.03, −1.64) | −3.5 *** (−5.1, −1.9) | −3.43 *** (−4.97, −1.89) |
| HADS depression | |||
| ACT | −2.42 ** (−4.08, −0.76) | −2.74 *** (−4.28, −1.2) | −2.95 *** (−4.4, −1.5) |
| TEAM | −2.92 ** (−4.56, −1.28) | −2.86 ** (−4.38, −1.33) | −2.75 ** (−4.18, −1.32) |
| SWLS | |||
| ACT | 3.07 ** (0.5, 5.64) | 3.68 ** (1.41,5.95) | 3.97 *** (1.82, 6.12) |
| TEAM | 4.61 *** (2.05, 7.16) | 4.64 *** (2.38, 6.9) | 4.52 *** (2.36, 6.67) |
| GHQ | |||
| ACT | 3.97 ** (1.3, 6.64) | 4.45 *** (1.97, 6.94) | 4.89 *** (2.55, 7.23) |
| TEAM | 5.32 *** (2.68, 7.96) | 5.56 *** (3.15, 7.96) | 5.38 *** (3.1, 7.65) |
| Pain | HADS Anxiety | HADS Depression | SWLS | GHQ | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Crude | Adjusted | Crude | Adjusted | Crude | Adjusted | Crude | Adjusted | Crude | Adjusted | |
| Intercept | 6.45 *** | 5.51 *** | 11.24 *** | 13.0 *** | 9.24 *** | 11.49 *** | 14.44 *** | 12.47 *** | 16.34 *** | 13.86 *** |
| Time | −0.21 | −0.23 | −0.02 | 0.05 | 0.68 | 0.71 | −0.67 | −0.75 | −0.31 | −0.36 |
| ACT | −0.56 | −0.51 | −1.08 | −1.63 * | −0.73 | −1.22 | 2.34 * | 2.96 ** | 2.62 * | 3.46 *** |
| TEAM | −0.50 | −0.49 | −0.81 | −0.80 | 0.15 | 0.15 | 0.93 | 0.87 | 0.89 | 0.79 |
| Time*ACT | −0.87 ** | −0.84 * | −1.49 * | −1.59 * | −2.29 *** | −2.34 *** | 1.45 | 1.62 | 2.15 * | 2.29 * |
| Time*TEAM | −0.49 | −0.43 | −2.71 *** | −2.82 *** | −3.29 *** | −3.29 *** | 3.96 *** | 3.96 *** | 4.94 *** | 4.92 *** |
| Age | −0.00 | −0.02 | −0.03 | 0.03 | 0.03 | |||||
| Employed | 0.63 * | 0.44 | 0.26 | −1.03 | −0.17 | |||||
| Diagnosis pain | 1.25 *** | −3.40 *** | −2.95 *** | 3.20 *** | 5.11 *** | |||||
| Diagnosis pain and psych | 1.08 *** | −0.88 | −0.87 | 0.15 | 2.44 * | |||||
| Years sick leave | −0.03 | 0.02 | −0.01 | 0.03 | −0.08 | |||||
| Sick leave 50% | 0.52 | 0.51 | 1.58 * | −0.57 | −1.37 | |||||
| Sick leave 75% | 1.29 * | 0.72 | 2.27 * | −1.79 | −2.01 | |||||
| Sick leave 100% | 1.61 *** | 2.61 ** | 4.11 *** | −4.68 *** | −5.54 *** | |||||
| ACT | TEAM | Control | ||||
|---|---|---|---|---|---|---|
| Months | 6 | 12 | 6 | 12 | 6 | 12 |
| HADS anxiety | n = 57 | n = 62 | n = 72 | |||
| Recovered | 13 | 12 | 9 | 34 | 4 | 10 |
| Improved | 10 | 7 | 4 | 4 | 4 | 2 |
| Unchanged | 77 | 79 | 84 | 62 | 85 | 80 |
| Deteriorated | 0 | 2 | 2 | 0 | 8 | 8 |
| HADS depression | n = 57 | n = 60 | n = 64 | |||
| Recovered | 13 | 14 | 24 | 36 | 4 | 2 |
| Improved | 5 | 12 | 2 | 11 | 4 | 0 |
| Unchanged | 77 | 71 | 67 | 47 | 85 | 90 |
| Deteriorated | 5 | 2 | 7 | 7 | 6 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finnes, A.; Anderzén, I.; Pingel, R.; Dahl, J.; Molin, L.; Lytsy, P. Comparing the Efficacy of Multidisciplinary Assessment and Treatment, or Acceptance and Commitment Therapy, with Treatment as Usual on Health Outcomes in Women on Long-Term Sick Leave—A Randomised Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 1754. https://doi.org/10.3390/ijerph18041754
Finnes A, Anderzén I, Pingel R, Dahl J, Molin L, Lytsy P. Comparing the Efficacy of Multidisciplinary Assessment and Treatment, or Acceptance and Commitment Therapy, with Treatment as Usual on Health Outcomes in Women on Long-Term Sick Leave—A Randomised Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(4):1754. https://doi.org/10.3390/ijerph18041754
Chicago/Turabian StyleFinnes, Anna, Ingrid Anderzén, Ronnie Pingel, JoAnne Dahl, Linnea Molin, and Per Lytsy. 2021. "Comparing the Efficacy of Multidisciplinary Assessment and Treatment, or Acceptance and Commitment Therapy, with Treatment as Usual on Health Outcomes in Women on Long-Term Sick Leave—A Randomised Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 4: 1754. https://doi.org/10.3390/ijerph18041754
APA StyleFinnes, A., Anderzén, I., Pingel, R., Dahl, J., Molin, L., & Lytsy, P. (2021). Comparing the Efficacy of Multidisciplinary Assessment and Treatment, or Acceptance and Commitment Therapy, with Treatment as Usual on Health Outcomes in Women on Long-Term Sick Leave—A Randomised Controlled Trial. International Journal of Environmental Research and Public Health, 18(4), 1754. https://doi.org/10.3390/ijerph18041754