Health Studies in the Context of Artisanal and Small-Scale Mining: A Scoping Review

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Terms and Strategy
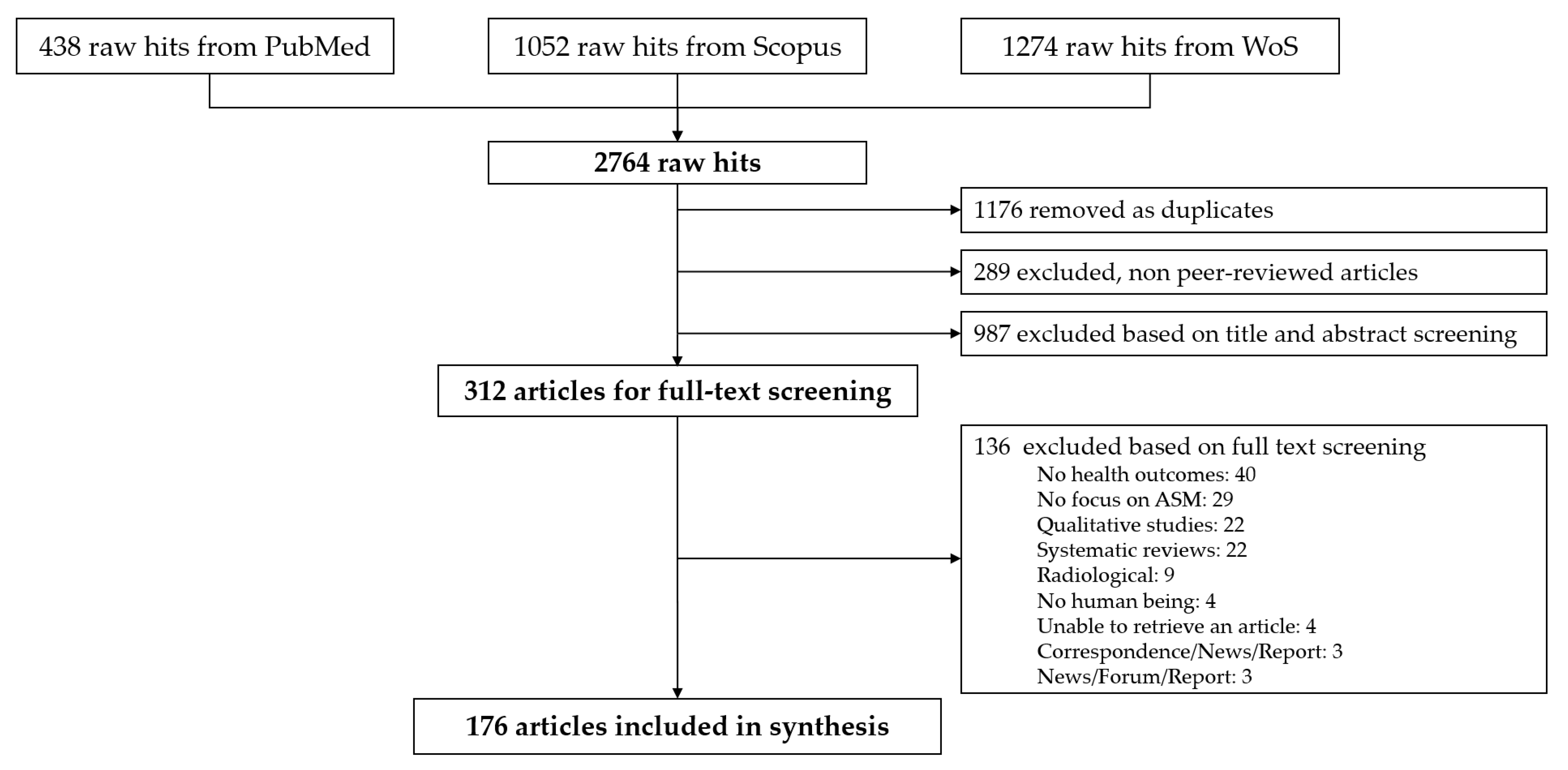
2.2. Peer-Reviewed Literature Searches and Screening
2.3. Data Extraction and Analysis
3. Results
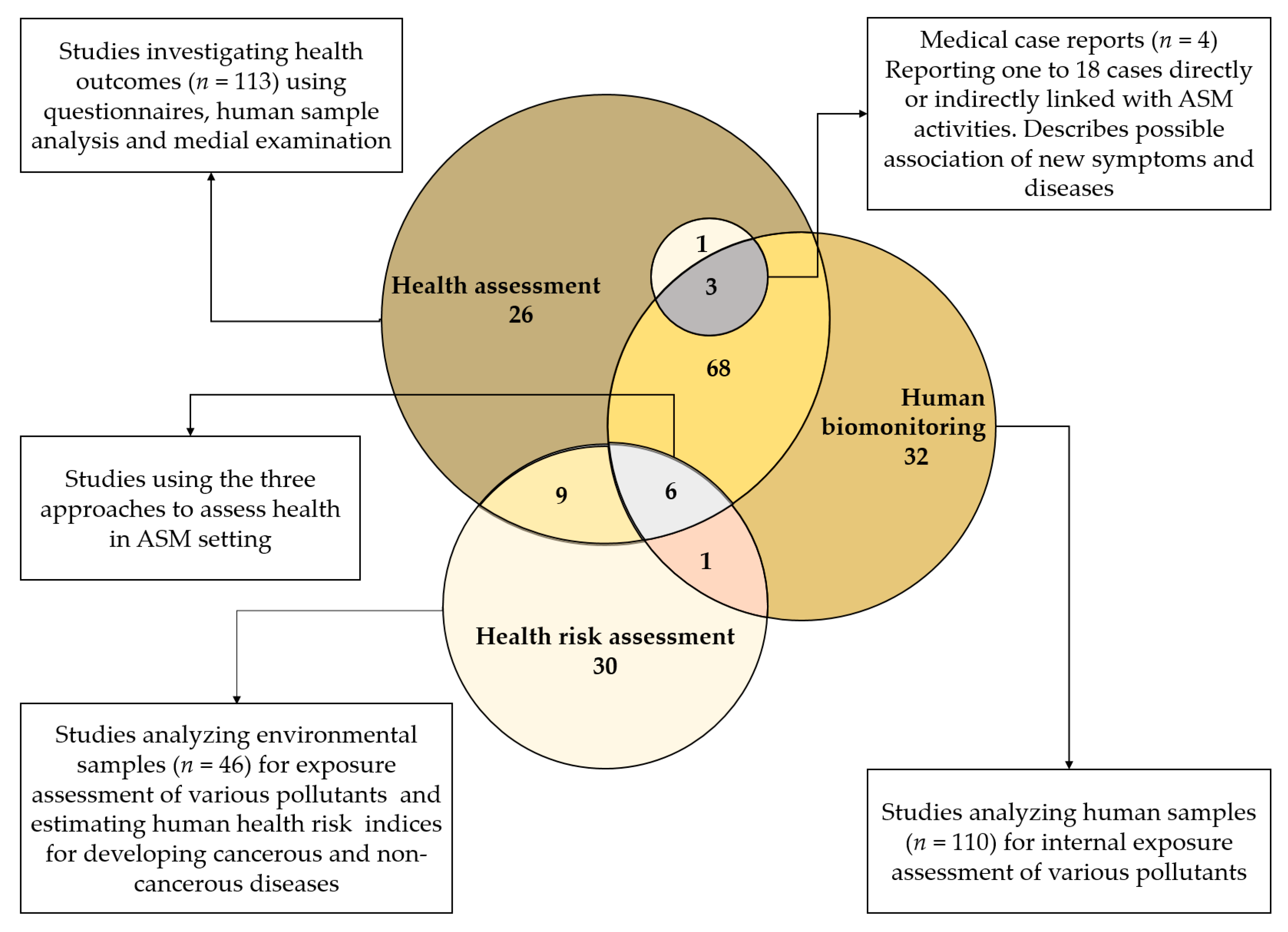
3.1. Overview of Studies
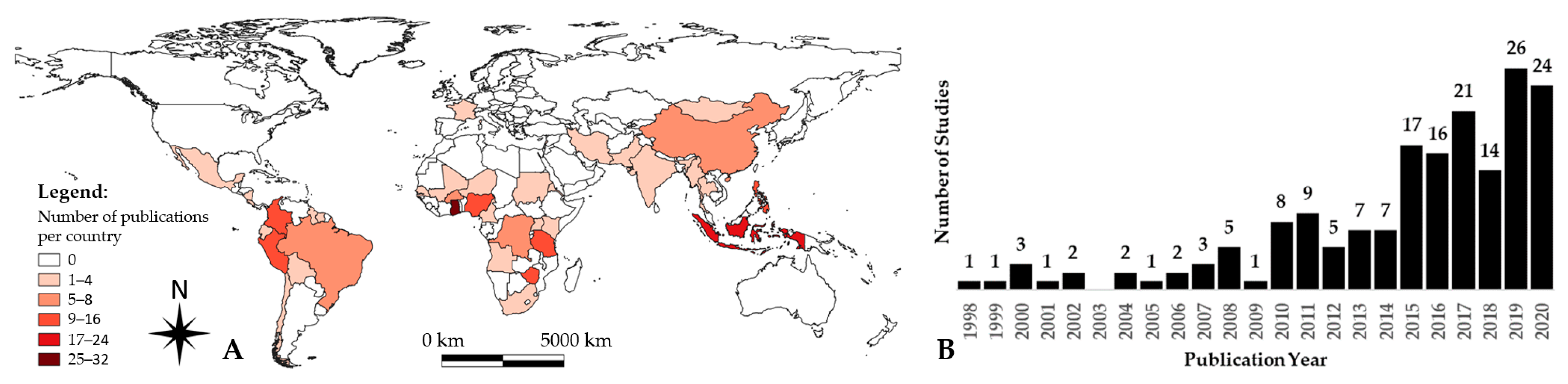
3.2. Study Characterization Regarding Country and Year of Publication
3.3. Study Characteristics Regarding Key Topics Covered
3.3.1. Type of ASM as Function of Extracted Commodities
3.3.2. Characteristics of Study Populations
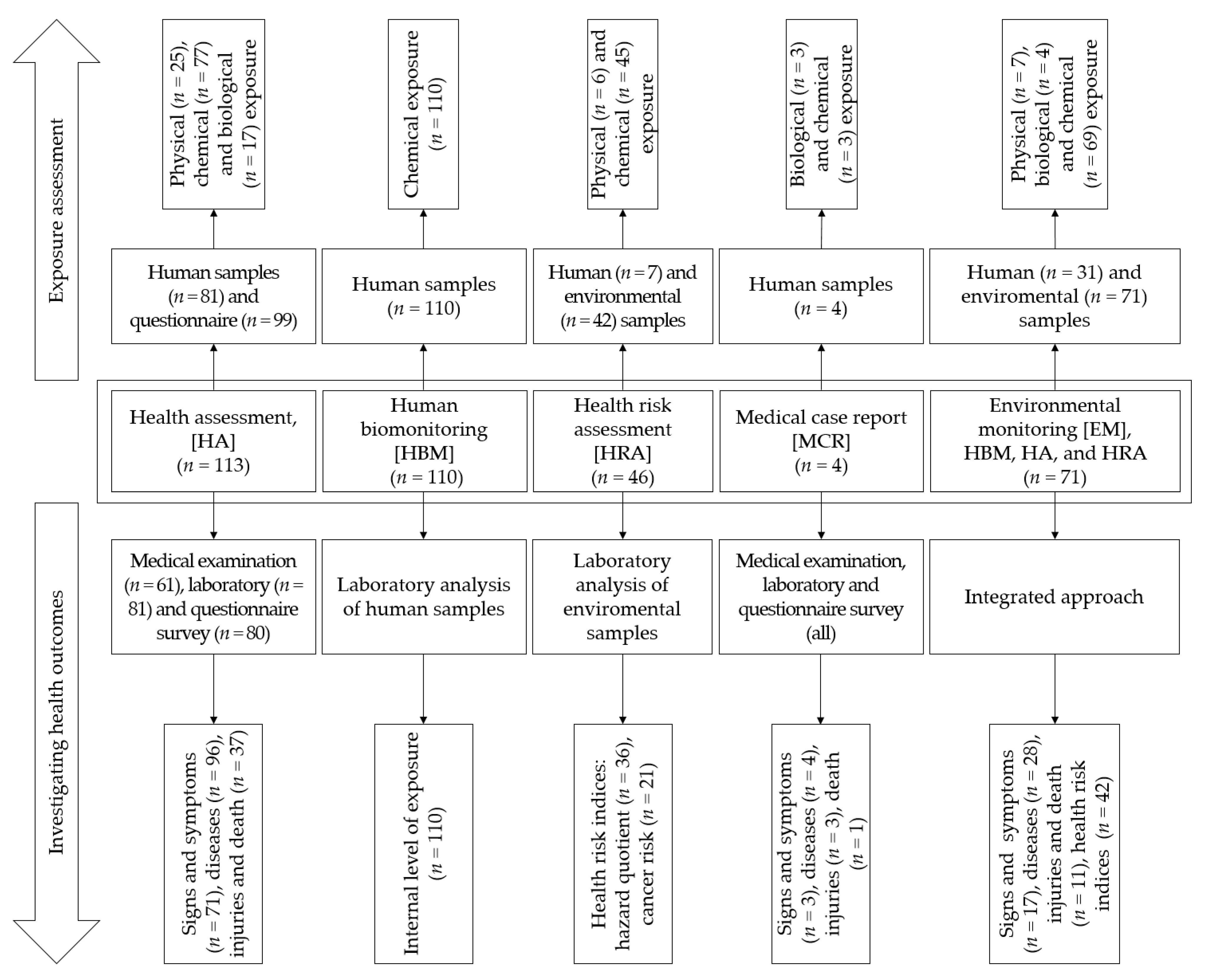
3.4. Type of Investigated Samples and Health Effects
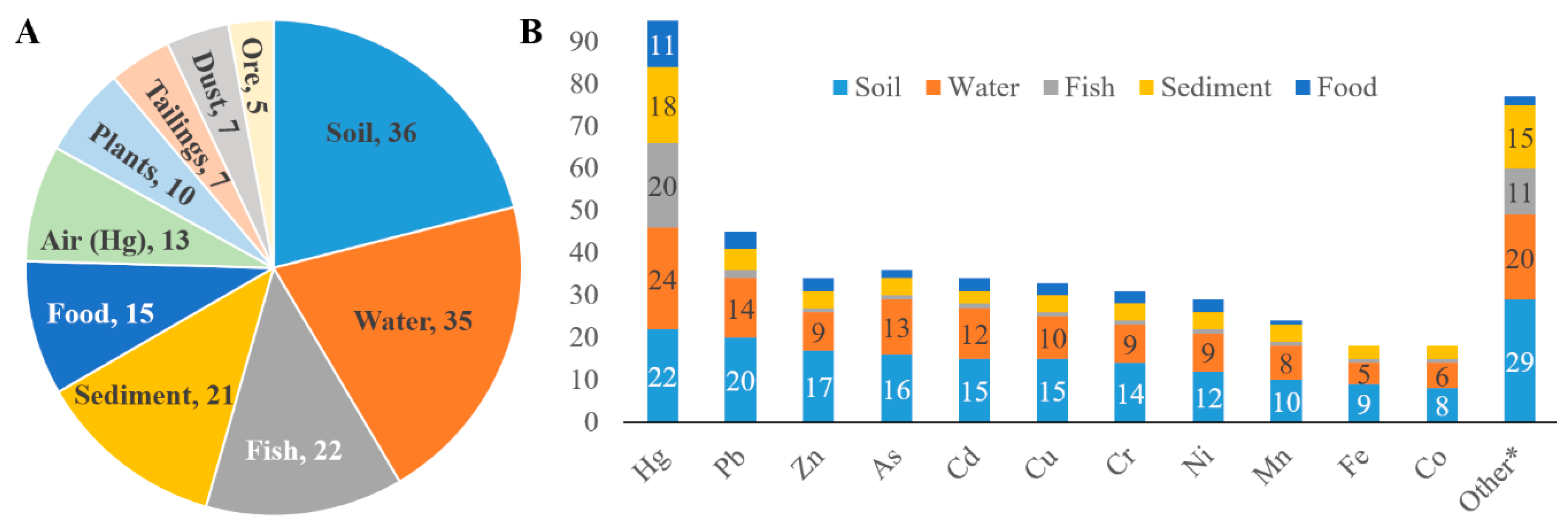
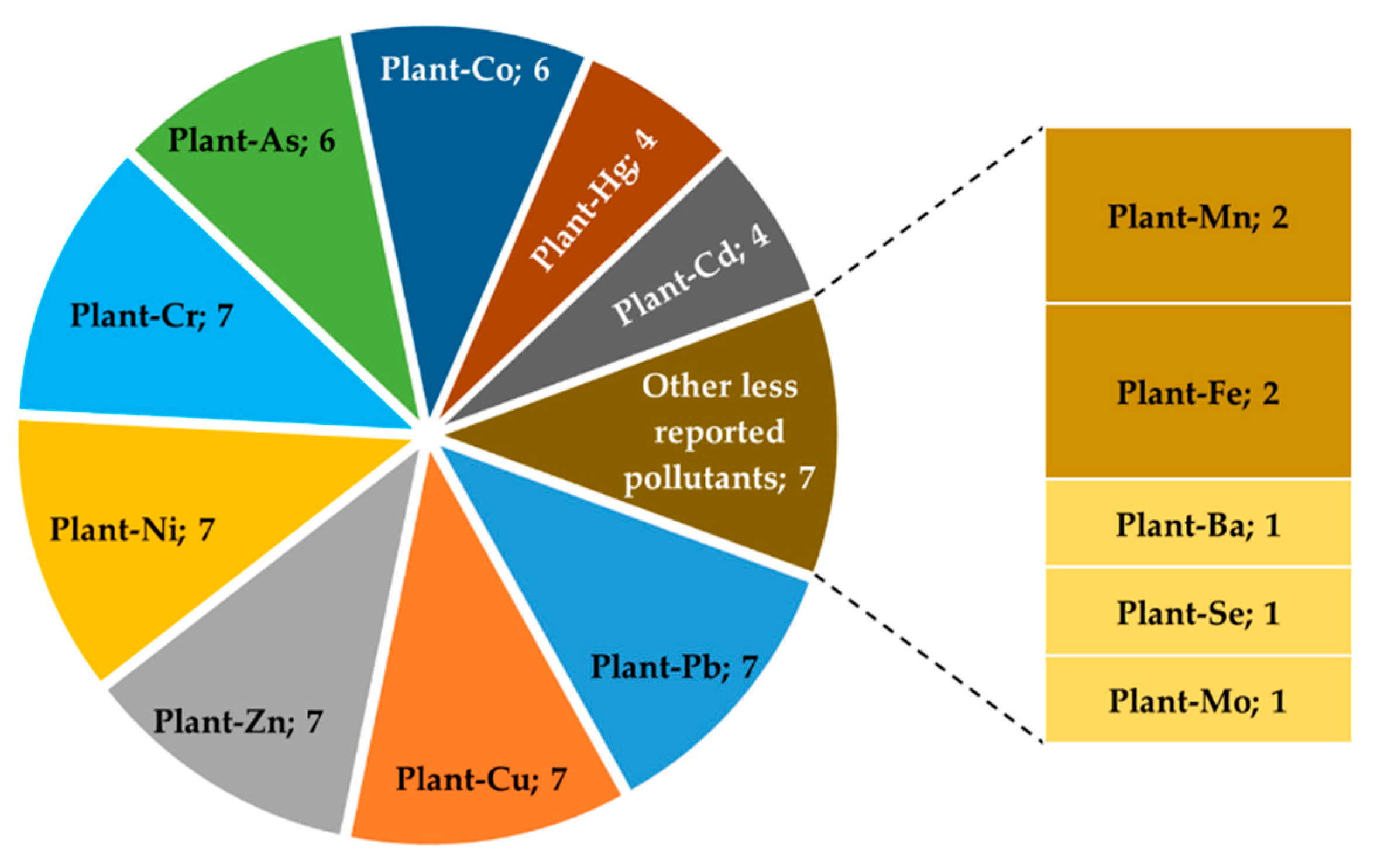
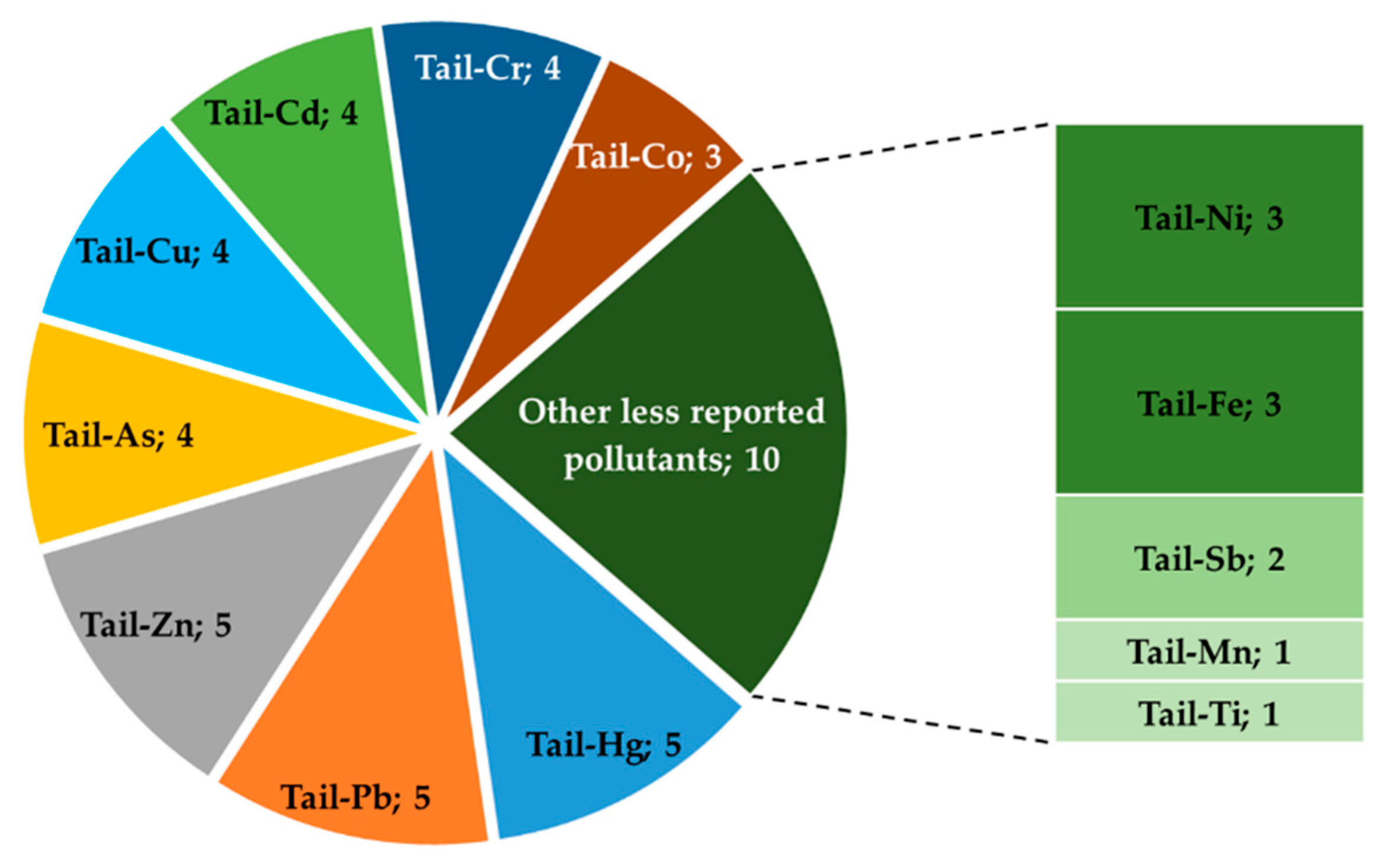
3.4.1. Environmental Samples and Related Pollutants
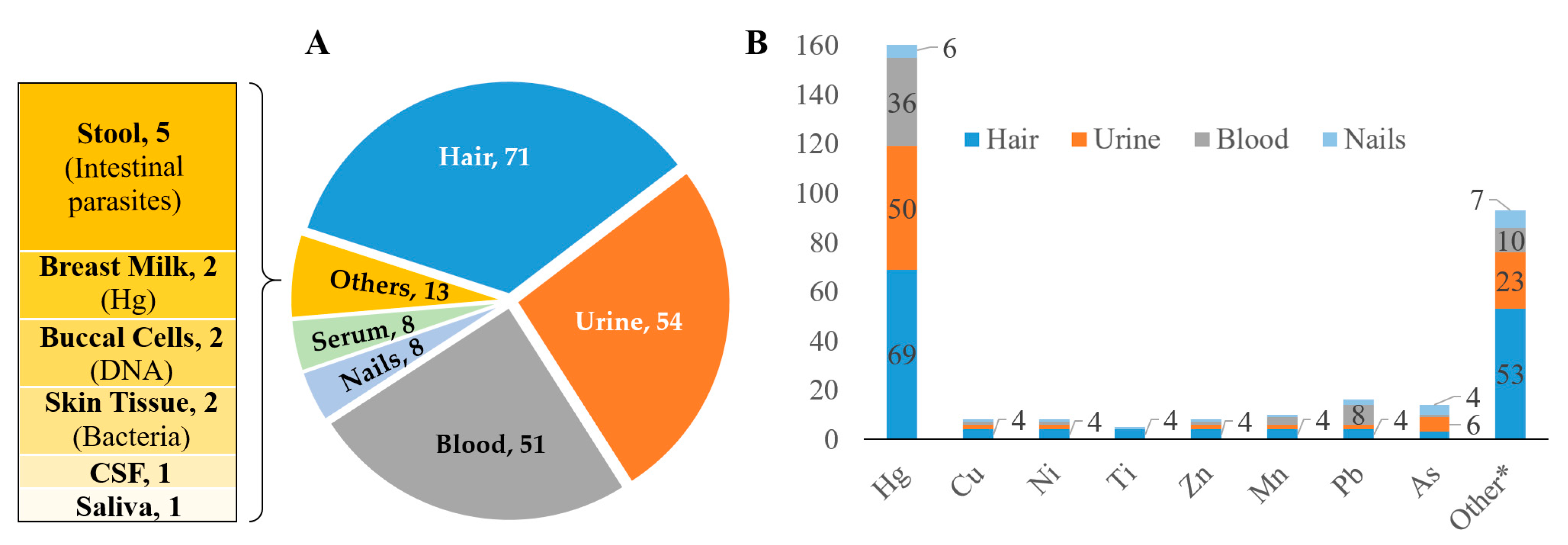
3.4.2. Human Samples and Related Biomarkers
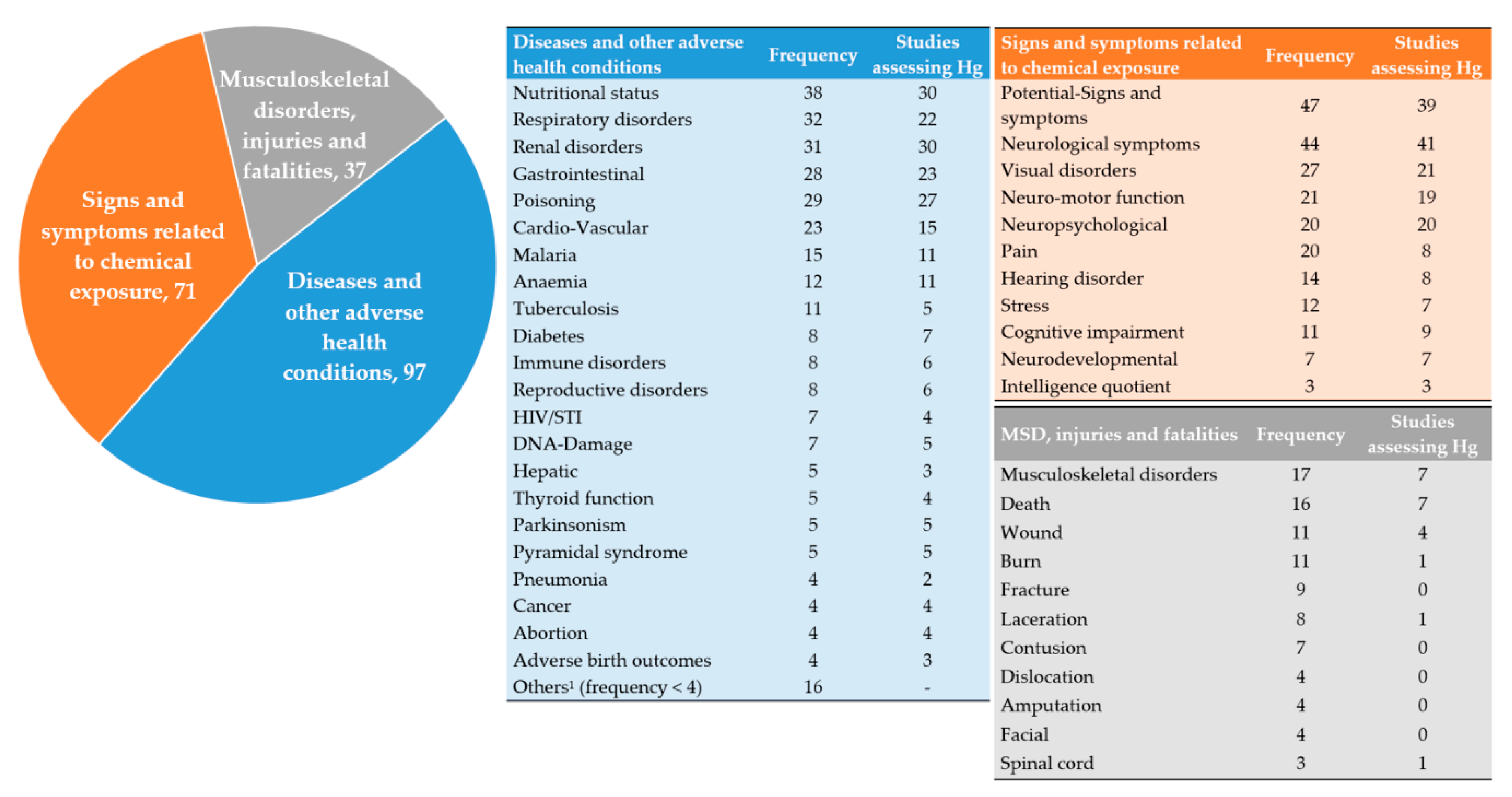
3.5. Adverse Health Conditions and Fatalities
3.5.1. Signs and Symptoms Related to Chemical Exposure
3.5.2. Adverse Health Conditions
3.5.3. Musculoskeletal Disorders, Injuries, and Fatalities
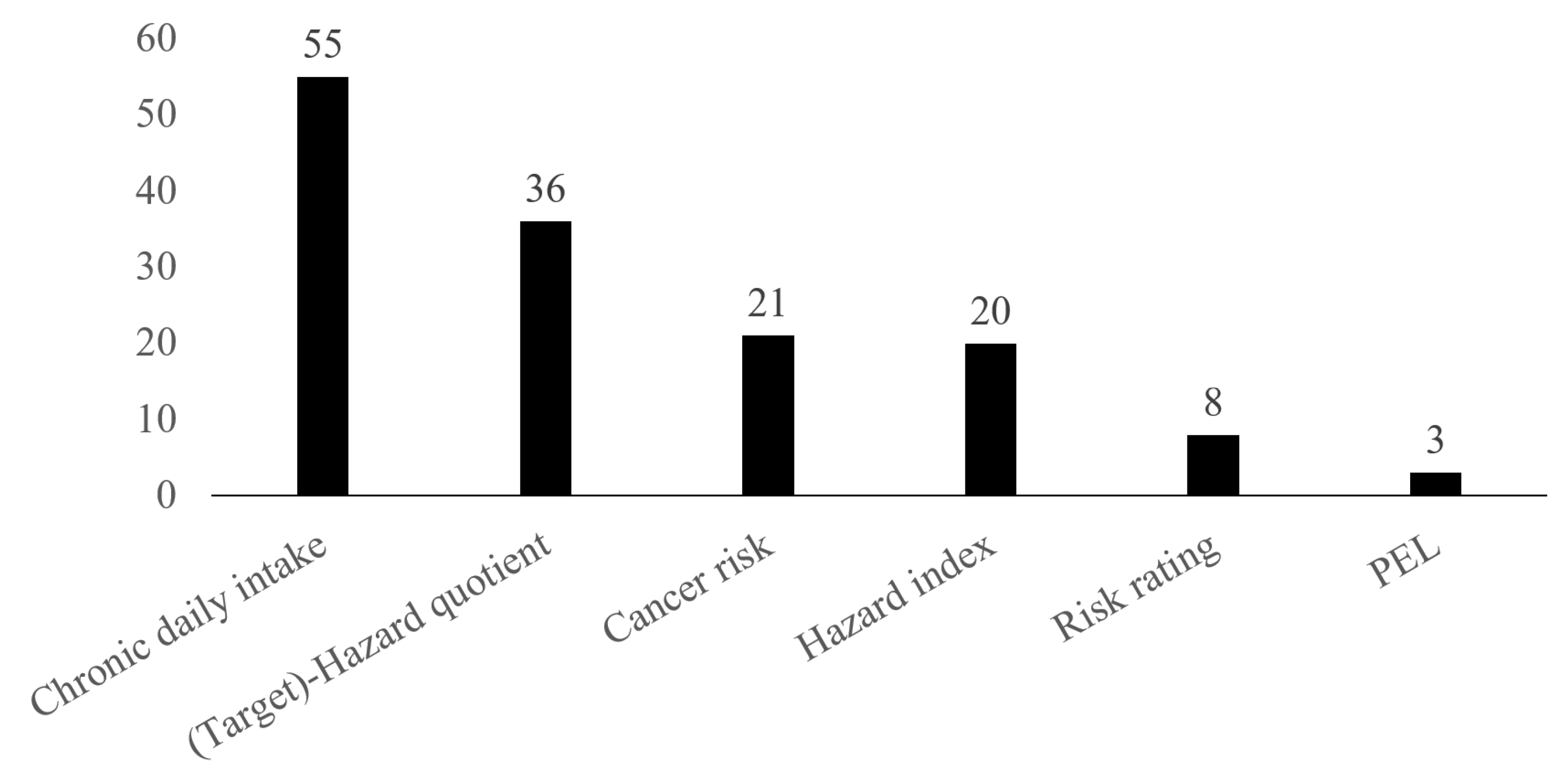
3.6. Health Risk Indices
4. Discussion
4.1. Representativeness of Health Research in ASM
4.2. Inclusion of Vulnerable Groups
4.3. Gaps Identified in Exposure Assessments
4.4. Widening the Focus of Health Conditions Studied
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Database | Search Terminology and Strategy | Number of Records (14 July 2020) |
|---|---|---|
| PubMed | ((artisanal[TIAB 1] OR small-scale[TIAB]) AND (mining[TIAB] OR mine[TIAB] OR miner[TIAB] OR mining[Mesh])) AND (health *[TIAB] OR health *[Mesh 2] OR disease *[TIAB] OR disease *[Mesh] OR injur *[TIAB] OR wound *[TIAB] OR “Wounds and Injuries”[Mesh] OR infect *[TIAB] OR infect *[Mesh] OR inciden *[TIAB] OR incidence[Mesh] OR prevalen *[TIAB] OR prevalence[Mesh] OR death *[TIAB] OR death[Mesh] OR dead *[TIAB] OR die[TIAB] OR died[TIAB] OR dying[TIAB] OR mortal *[Mesh] OR fatal *[TIAB] OR surviv *[TIAB] OR survival[Mesh] OR safety[TIAB] OR “safety management”[Mesh] OR risk[TIAB] OR risk[Mesh] OR hazard[TIAB] OR poisoning[TIAB] OR poisoning[Mesh]) | 438 |
| Web of Science (all databases) | TS 3 = (((artisanal OR small-scale) AND (mine OR miner OR mining)) AND (health OR disease * OR wound * OR injur * OR infect * OR inciden * OR prevalen * OR death * OR dead * OR die OR died OR dying OR mortal * OR fatal * OR surviv * OR safety OR risk OR hazard OR poison *)) | 1274 |
| Scopus | title-abs-key 4 (artisanal OR “small-scale” OR “small-scale” OR “small scale”) AND title-abs-key (mine OR miner OR mining) AND title-abs-key (health OR disease OR diseases OR wound * OR injur * OR infection * OR inciden * OR prevalen * OR death * OR dead * OR die OR died OR dying OR mortal * OR fatal * OR surviv * OR safety OR risk OR hazard OR poison *) | 1052 |
Appendix B
| Chemical Names and Symbols of Pollutants | Frequency of Reporting Studies per Type of Environmental Samples | ||||
|---|---|---|---|---|---|
| Soil | Water | Sediment | Fish | Food | |
| Antimony (Sb) | 4 | 2 | 2 | 0 | 0 |
| Selenium (Se) | 4 | 3 | 1 | 1 | 2 |
| Aluminium (Al) | 3 | 2 | 2 | 0 | 0 |
| Barium (Ba) | 2 | 1 | 0 | 0 | 0 |
| Phosphorus (P) | 2 | 0 | 0 | 0 | 0 |
| Tin (Sn) | 2 | 1 | 0 | 0 | 0 |
| Titanium (Ti) | 2 | 2 | 0 | 0 | 0 |
| Calcium (Ca) | 1 | 0 | 0 | 0 | 0 |
| Cerium (Ce) | 1 | 1 | 0 | 0 | 0 |
| Lithium (Li) | 1 | 1 | 0 | 0 | 0 |
| Molybdenum (Mo) | 1 | 2 | 1 | 1 | 0 |
| Neodymium (Nd) | 1 | 1 | 0 | 0 | 0 |
| Silicon (Si) | 1 | 0 | 0 | 0 | 0 |
| Uranium (U) | 1 | 1 | 0 | 0 | 0 |
| Vanadium (V) | 1 | 1 | 0 | 0 | 0 |
| Yttrium (Y) | 1 | 1 | 0 | 0 | 0 |
| Zirconium (Zr) | 1 | 1 | 0 | 0 | 0 |
| Chemical Names and Symbols of Pollutants | Frequency of Reporting Studies per Type of Environmental Samples | |
|---|---|---|
| Dust | Ore | |
| Mercury (Hg) | 3 | 1 |
| Lead (Pb) | 2 | 4 |
| Aluminium (Al) | 1 | 1 |
| Antimony (Sb) | 1 | 1 |
| Arsenic (As) | 1 | 2 |
| Cadmium (Cd) | 1 | 2 |
| Cerium (Ce) | 1 | 1 |
| Chromium (Cr) | 1 | 1 |
| Cobalt (Co) | 1 | 1 |
| Copper (Cu) | 1 | 1 |
| Iron (Fe) | 1 | 1 |
| Lanthanum (La) | 1 | 1 |
| Manganese (Mn) | 1 | 2 |
| Molybdenum (Mo) | 1 | 1 |
| Neodymium (Nd) | 1 | 1 |
| Nickel (Ni) | 1 | 1 |
| Selenium (Se) | 1 | 1 |
| Silicon (Si) | 1 | 0 |
| Tin (Sn) | 1 | 1 |
| Titanium (Ti) | 1 | 1 |
| Uranium (U) | 0 | 1 |
| Vanadium (V) | 1 | 1 |
| Yttrium (Y) | 1 | 1 |
| Zinc (Zn) | 1 | 1 |
| Zirconium (Zr) | 1 | 1 |


Appendix C
| Symbols of Chemicals | Frequencies | Symbols of Chemicals | Frequencies | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hair | Urine | Blood | Nails | Hair | Urine | Blood | Nails | ||
| Cd | 3 | 2 | 3 | 1 | I | 1 | 0 | 0 | 0 |
| Co | 3 | 2 | 2 | 1 | In | 1 | 1 | 0 | 0 |
| Cr | 3 | 2 | 1 | 1 | Mg | 1 | 0 | 0 | 0 |
| Al | 2 | 2 | 0 | 1 | Mo | 1 | 1 | 0 | 0 |
| Ca | 2 | 0 | 0 | 0 | Nb | 1 | 0 | 0 | 0 |
| Cl | 2 | 0 | 0 | 0 | Pd | 1 | 0 | 1 | 0 |
| Fe | 2 | 0 | 0 | 0 | Pt | 1 | 1 | 0 | 0 |
| K | 2 | 0 | 0 | 0 | Rb | 1 | 0 | 0 | 0 |
| Na | 2 | 0 | 0 | 0 | Sb | 1 | 1 | 0 | 1 |
| P | 2 | 0 | 0 | 0 | Se | 1 | 2 | 0 | 1 |
| S | 2 | 0 | 0 | 0 | Sn | 1 | 1 | 0 | 0 |
| Si | 2 | 0 | 0 | 0 | Sr | 1 | 0 | 0 | 0 |
| Ag | 1 | 0 | 0 | 0 | Te | 1 | 1 | 0 | 0 |
| Au | 1 | 0 | 0 | 1 | V | 1 | 1 | 0 | 0 |
| Ba | 1 | 1 | 0 | 0 | W | 1 | 0 | 0 | 0 |
| Bi | 1 | 1 | 0 | 0 | Y | 1 | 0 | 0 | 0 |
| Br | 1 | 0 | 0 | 0 | Zr | 1 | 0 | 0 | 0 |
| Ce | 1 | 0 | 0 | 0 | Be | 0 | 1 | 0 | 0 |
| Cs | 1 | 0 | 0 | 0 | Li | 0 | 1 | 0 | 0 |
| Ga | 1 | 0 | 0 | 0 | Tl | 0 | 1 | 2 | 0 |
| Ge | 1 | 0 | 0 | 0 | U | 0 | 1 | 1 | 0 |
| Physiological Parameter | Frequency |
|---|---|
| Micronutrients | 7 |
| Autoantibody/IRP | 5 |
| Creatinine | 4 |
| ALT | 3 |
| AST | 3 |
| Urea | 3 |
| Glucose | 2 |
| HIV antibodies | 2 |
| T4 | 2 |
| TSH | 2 |
| T3 | 1 |
Appendix D
| Diseases | Frequency |
|---|---|
| Hepatitis | 3 |
| Typhoid | 3 |
| Agnathia–otocephaly | 1 |
| Bodily vibration syndrome | 1 |
| Buruli ulcer | 1 |
| Dengue | 1 |
| Dermatophyte infections | 1 |
| Hansen | 1 |
| Heatstroke | 1 |
| Hernia | 1 |
| Infertility | 1 |
| Sexual violence | 1 |
References
- Zvarivadza, T. Artisanal and Small-Scale Mining as a challenge and possible contributor to Sustainable Development. Resour. Policy 2018, 56, 49–58. [Google Scholar] [CrossRef]
- Hentschel, T.; Hruschka, F.; Priester, M. Artisanal and Small-Scale Mining: Challenges and Opportunities; International Institute for Environment and Development (IIED) and WBCSD: London, UK, 2003; p. 80. ISBN 1-84369-470-0. [Google Scholar]
- Hinton, J.J. Communities and Small Scale Mining: An Integrated Review For Development Planning, 1st ed.; Walser, G., Ed.; Mining Department, World Bank Group: Washington, DC, USA, 2005; Volume 1, pp. 4–24. [Google Scholar]
- Artisanalmining.org. The Artisanal and Small-Scale Mining Knowledge Sharing Archive. Available online: http://artisanalmining.org/ (accessed on 4 September 2020).
- WHO. Environmental and Occupational Health Hazards Associated with Artisanal and Small-Scale Gold Mining; World Health Organization: Geneva, Switzerland, 2016; Volume 1, p. 26. ISBN 9789241510271. [Google Scholar]
- Mutemeri, N.; Walker, J.Z.; Coulson, N.; Watson, I. Capacity building for self-regulation of the Artisanal and Small-Scale Mining (ASM) sector: A policy paradigm shift aligned with development outcomes and a pro-poor approach. Extr. Ind. Soc. Int. J. 2016, 3, 653–658. [Google Scholar] [CrossRef]
- Buxton, A. Responding to the Challenge of Artisanal and Small-Scale Mining: How Can Knowledge Networks Help? International Institute for Environment and Development: London, UK, 2013; p. 30. [Google Scholar]
- Fritz, M.; McQuilken, J.; Collins, N.; Weldegiorgis, F. Global Trends in Artisanal and Small-Scale Mining (ASM): A Review of Key Numbers and Issues; Intergovernmental Forum on Mining, Minerals, Metals and Sustainable Development (IGF): Winnipeg, MA, Canada, 2018; p. 81. [Google Scholar]
- Hilson, G. Small-scale mining, poverty and economic development in sub-Saharan Africa: An overview. Resour. Policy 2009, 34, 1–5. [Google Scholar] [CrossRef]
- Eftimie, A.; Heller, K.; Strongman, J.; Hinton, J.; Lahiri-Dutt, K.; Mutemeri, N. Gender Dimensions of Artisanal and Small-Scale Mining: A Rapid Assessment Toolkit; Report Number: 67520; World Bank: Washington, DC, USA, 2012; p. 128. [Google Scholar]
- Levin-Nally, E. Global Trends in Artisanal and Small-Scale Mining: What do these mean for Mongolia? Available online: https://www.levinsources.com/knowledge-centre/insights/global-trends-in-artisanal-and-small-scale-mining-what-do-these-mean-for-mongolia (accessed on 4 September 2020).
- Jennings, N.S. Social and Labour Issues in Small-Scale Mines. Report for Discussion at the Tripartite Meeting on Social and Labour Issues in Small-scale Mines; International Labour Organization (ILO): Geneve, Switzerland, 1999; Volume 1, p. 99. ISBN 92-2-111480-5. [Google Scholar]
- Langston, J.D.; Lubis, M.I.; Sayer, J.A.; Margules, C.; Boedhihartono, A.K.; Dirks, P.H.G.M. Comparative development benefits from small and large scale mines in North Sulawesi, Indonesia. Extr. Ind. Soc. 2015, 2, 434–444. [Google Scholar] [CrossRef]
- Smith, N.M.; Ali, S.; Bofinger, C.; Collins, N. Human health and safety in artisanal and small-scale mining: An integrated approach to risk mitigation. J. Clean. Prod. 2016, 129, 43–52. [Google Scholar] [CrossRef]
- World Bank. 2019 State of the Artisanal and Small-Scale Mining Sector; World Bank: Washington, DC, USA, 2019; p. 85. [Google Scholar]
- Bradley, J.; Rehman, A.M.; Schwabe, C.; Vargas, D.; Monti, F.; Ela, C.; Riloha, M.; Kleinschmidt, I. Reduced Prevalence of Malaria Infection in Children Living in Houses with Window Screening or Closed Eaves on Bioko Island, Equatorial Guinea. PLoS ONE 2013, 8, e80626. [Google Scholar] [CrossRef]
- Gan, W.Q.; Sanderson, W.T.; Browning, S.R.; Mannino, D.M. Different types of housing and respiratory health outcomes. Prev. Med. Rep. 2017, 7, 124–129. [Google Scholar] [CrossRef]
- Dondeyne, S.; Ndunguru, E.; Rafael, P.; Bannerman, J. Artisanal mining in central Mozambique: Policy and environmental issues of concern. Resour. Policy 2009, 34, 45–50. [Google Scholar] [CrossRef]
- Secretary-General, U. Small-Scale Mining Activities in Developing Countries and Economies in Transition: Report of the Secretary-General; E/C.7/1994/9; United Nations: New York, NY, USA, 1993; p. 30. [Google Scholar]
- Ramazzini, B. De morbis artificum diatriba [diseases of workers]. 1713. Am. J. Public Health 2001, 91, 1380–1382. [Google Scholar] [CrossRef]
- Rose, G. The History of Miners′ Diseases: A Medical and Social Interpretation. J. Am. Med. Assoc. 1944, 125, 758. [Google Scholar] [CrossRef]
- Cole, F.J. The History of Miners′ Diseases. Nature 1944, 154, 161–162. [Google Scholar] [CrossRef]
- Basu, N.; Clarke, E.; Green, A.; Calys-Tagoe, B.; Chan, L.; Dzodzomenyo, M.; Fobil, J.; Long, R.N.; Neitzel, R.L.; Obiri, S.; et al. Integrated Assessment of Artisanal and Small-Scale Gold Mining in Ghana-Part 1: Human Health Review. Int. J. Environ. Res. Public Health 2015, 12, 5143–5176. [Google Scholar] [CrossRef]
- Afrifa, J.; Opoku, Y.K.; Sorkpor, R.D. The Clinical Importance of the Mercury Problem in Artisanal Small-Scale Gold Mining. Front Public Health 2019, 7, 131. [Google Scholar] [CrossRef] [PubMed]
- Ostfeld, R.S. Biodiversity loss and the ecology of infectious disease. Lancet Planet Health 2017, 1, e2–e3. [Google Scholar] [CrossRef]
- Baeuml, J.; Bose-O’Reilly, S.; Gothe, R.M.; Lettmeier, B.; Roider, G.; Drasch, G.; Siebert, U. Human Biomonitoring Data from Mercury Exposed Miners in Six Artisanal Small-Scale Gold Mining Areas in Asia and Africa. Minerals 2011, 1, 122–143. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Nowak, D.; Bernaudat, L.; Drasch, G. Signs and Symptoms of Mercury-Exposed Gold Miners. Int. J. Occup. Med. Environ. Health 2017, 30, 249–269. [Google Scholar] [CrossRef]
- Pringle, J.D. The Unprecedented Lead-Poisoning Outbreak: Ethical Issues in a Troubling Broader Context. Public Health Ethics 2014, 7, 301–305. [Google Scholar] [CrossRef]
- Gibb, H.; O'Leary, K.G. Mercury Exposure and Health Impacts among Individuals in the Artisanal and Small-Scale Gold Mining Community: A Comprehensive Review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef]
- Tirima, S.; Bartrem, C.; von Lindern, I.; von Braun, M.; Lind, D.; Anka, S.M.; Abdullahi, A. Food contamination as a pathway for lead exposure in children during the 2010-2013 lead poisoning epidemic in Zamfara, Nigeria. J. Environ. Sci. 2018, 67, 260–272. [Google Scholar] [CrossRef]
- Nkulu, C.B.L.; Casas, L.; Saenen, N.D.; Kayembe-Kitenge, T.; Ilunga, J.-M.L.; Nawrot, T.S.; Nemery, B. Sustainability of artisanal mining of cobalt in DR Congo. Nat. Sustain. 2018, 1, 495–504. [Google Scholar] [CrossRef]
- Nyanza, E.C.; Dewey, D.; Manyama, M.; Martin, J.W.; Hatfield, J.; Bernier, F.P. Maternal exposure to arsenic and mercury and associated risk of adverse birth outcomes in small-scale gold mining communities in Northern Tanzania. Environ. Int. 2020, 137, 105450. [Google Scholar] [CrossRef] [PubMed]
- Stuckler, D.; Basu, S.; McKee, M.; Lurie, M. Mining and Risk of Tuberculosis in Sub-Saharan Africa. Am. J. Public Health 2011, 101, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Ostfeld, R.S. Tropical forests and child health. Lancet Planet Health 2017, 1, e164–e165. [Google Scholar] [CrossRef]
- Steckling, N.; Bose-O'Reilly, S.; Pinheiro, P.; Plass, D.; Shoko, D.; Drasch, G.; Bernaudat, L.; Siebert, U.; Hornberg, C. The burden of chronic mercury intoxication in artisanal small-scale gold mining in Zimbabwe: Data availability and preliminary estimates. Environ. Health 2014, 13, 111. [Google Scholar] [CrossRef]
- Steckling, N.; Tobollik, M.; Plass, D.; Hornberg, C.; Ericson, B.; Fuller, R.; Bose-O'Reilly, S. Global Burden of Disease of Mercury Used in Artisanal Small-Scale Gold Mining. Ann. Glob. Health 2017, 83, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Betancur-Corredor, B.; Loaiza-Usuga, J.C.; Denich, M.; Borgemeister, C. Gold mining as a potential driver of development in Colombia: Challenges and opportunities. J. Clean. Prod. 2018, 199, 538–553. [Google Scholar] [CrossRef]
- Wilson, M.L.; Renne, E.; Roncoli, C.; Agyei-Baffour, P.; Tenkorang, E.Y. Integrated Assessment of Artisanal and Small-Scale Gold Mining in Ghana—Part 3: Social Sciences and Economics. Int. J. Environ. Res. Public Health 2015, 12, 8133–8156. [Google Scholar] [CrossRef]
- Esdaile, L.J.; Chalker, J.M. The Mercury Problem in Artisanal and Small-Scale Gold Mining. Chemistry 2018, 24, 6905–6916. [Google Scholar] [CrossRef] [PubMed]
- Basu, N.; Ayelo, P.A.; Djogbénou, L.S.; Kedoté, M.; Lawin, H.; Tohon, H.; Oloruntoba, E.O.; Adebisi, N.A.; Cazabon, D.; Fobil, J.; et al. Occupational and Environmental Health Risks Associated with Informal Sector Activities-Selected Case Studies from West Africa. New Solut. A J. Environ. Occup. Health Policy 2016, 26, 253–270. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O'Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Dorne, J.-L.C.M.; Kass, G.E.N.; Bordajandi, L.R.; Amzal, B.; Bertelsen, U.; Castoldi, A.F.; Heppner, C.; Eskola, M.; Fabiansson, S.; Ferrari, P.; et al. Human risk assessment of heavy metals: Principles and applications. In Metal Ions in Toxicology: Effects, Interactions, Interdependencies; Sigel, A., Sigel, H., Sigel, R.K.O., Eds.; The Royal Society of Chemistry: Cambridge, UK, 2011; Volume 8, pp. 27–60. [Google Scholar]
- Orisakwe, O.E.; Dagur, E.A.; Mbagwu, H.O.; Udowelle, N.A. Lead Levels in Vegetables from Artisanal Mining Sites of Dilimi River, Bukuru and Barkin Ladi North Central Nigeria: Cancer and Non-Cancer Risk Assessment. Asian Pac. J. Cancer Prev. 2017, 18, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Laffont, L.; Sonke, J.E.; Maurice, L.; Monrroy, S.L.; Chincheros, J.; Amouroux, D.; Behra, P. Hg speciation and stable isotope signatures in human hair as a tracer for dietary and occupational exposure to mercury. Environ. Sci. Technol. 2011, 45, 9910–9916. [Google Scholar] [CrossRef] [PubMed]
- Rembold, F.; Kerdiles, H.; Meroni, M.; Pérez-Hoyos, A.; Urbano, F.; Agudo, L.M.; Dimou, M.; Bande, A.; Vojnović, P.; Team, A. ASPA—Anomaly Hotspots of Agricultural Production. Available online: https://mars.jrc.ec.europa.eu/asap/files/gaul0_asap_v04.zip (accessed on 2 June 2020).
- Malek, A.A.K.; El Khoury, R.; Halabi-Tawil, M.; Choucair, J. Chronic Mercury Intoxication Masquerading as Systemic Disease: A Case Report and Review of the Literature. Eur. J. Case Rep. Intern. Med. 2017, 4, 000632. [Google Scholar] [CrossRef]
- Tony, K.K.; Vicky, M.K.; de Luca, C.; Paul, M.O.; Eric, K.I.; Sébastien, M.M.; Tim, N.; Lubaba Nkulu, C.B.; Nemery, B.; Devriendt, K. Agnathia otocephaly: A case from the Katanga Copperbelt. Birth Defects Res. 2020, 112, 1287–1291. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Schierl, R.; Nowak, D.; Siebert, U.; William, J.F.; Owi, F.T.; Ir, Y.I. A preliminary study on health effects in villagers exposed to mercury in a small-scale artisanal gold mining area in Indonesia. Environ. Res. 2016, 149, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.M.; Nyland, J.F.; Silva, I.A.; Ventura, A.M.; Souza, J.M.d.; Silbergeld, E.K. Mercury exposure, serum antinuclear/antinucleolar antibodies, and serum cytokine levels in mining populations in Amazonian Brazil: A cross-sectional study. Environ. Res. 2010, 110, 345–354. [Google Scholar] [CrossRef]
- Motts, J.A.; Shirley, D.L.; Silbergeld, E.K.; Nyland, J.F. Novel biomarkers of mercury-induced autoimmune dysfunction: A cross-sectional study in Amazonian Brazil. Environ. Res. 2014, 132, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Orisakwe, O.E.; Dagur, E.A.; Mbagwu, H.O.C.; Udowelle, N.A.; Offor, S.J. Levels of some heavy metals in vegetables from artisanal mining sites of Dilimi River, Bukuru and Barkin Ladi North Central Nigeria: Any public health concern? Rocz. Panstw. Zakl. Hig. 2018, 69, 335–345. [Google Scholar] [CrossRef]
- Liu, S.; Tian, S.; Li, K.; Wang, L.; Liang, T. Heavy metal bioaccessibility and health risks in the contaminated soil of an abandoned, small-scale lead and zinc mine. Environ. Sci. Pollut. Res. Int. 2018, 25, 15044–15056. [Google Scholar] [CrossRef]
- Sun, Z.; Hu, Y.; Cheng, H. Public health risk of toxic metal(loid) pollution to the population living near an abandoned small-scale polymetallic mine. Sci. Total Environ. 2020, 718, 137434. [Google Scholar] [CrossRef]
- Getriana, A.; Achmadi, U.F.; Leometa, C.H. Behavioral mercury exposure of people in artisanal and small-scale gold mining site area at lebaksitu village, 2017. Indian J. Public Health Res. Dev. 2018, 9, 433–438. [Google Scholar] [CrossRef]
- Ohlander, J.; Huber, S.M.; Schomaker, M.; Heumann, C.; Schierl, R.; Michalke, B.; Jenni, O.G.; Caflisch, J.; Munoz, D.M.; von Ehrenstein, O.S.; et al. Risk factors for mercury exposure of children in a rural mining town in northern Chile. PLoS ONE 2013, 8, e79756. [Google Scholar] [CrossRef]
- Rustad, S.A.; Ostby, G.; Nordas, R. Artisanal mining, conflict, and sexual violence in Eastern DRC. Extr. Ind. Soc. Int. J. 2016, 3, 475–484. [Google Scholar] [CrossRef]
- Darko, G.; Adjei, S.; Nkansah, M.A.; Borquaye, L.S.; Boakye, K.O.; Dodd, M. Accumulation and bioaccessibility of toxic metals in root tubers and soils from gold mining and farming communities in the Ashanti region of Ghana. Int. J. Environ. Health Res. 2020. [Google Scholar] [CrossRef]
- Ashe, K. Elevated Mercury Concentrations in Humans of Madre de Dios, Peru. PLoS ONE 2012, 7, e33305. [Google Scholar] [CrossRef]
- Nyanza, E.C.; Joseph, M.; Premji, S.S.; Thomas, D.S.K.; Mannion, C. Geophagy practices and the content of chemical elements in the soil eaten by pregnant women in artisanal and small scale gold mining communities in Tanzania. BMC Pregnancy Childbirth 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed]
- Nyanza, E.C.; Bernier, F.P.; Manyama, M.; Hatfield, J.; Martin, J.W.; Dewey, D. Maternal exposure to arsenic and mercury in small-scale gold mining areas of Northern Tanzania. Environ. Res. 2019, 173, 432–442. [Google Scholar] [CrossRef]
- Nyanza, E.C.; Dewey, D.; Bernier, F.; Manyama, M.; Hatfield, J.; Martin, J.W. Validation of Dried Blood Spots for Maternal Biomonitoring of Nonessential Elements in an Artisanal and Small-Scale Gold Mining Area of Tanzania. Environ. Toxicol. Chem. 2019, 38, 1285–1293. [Google Scholar] [CrossRef]
- Wickliffe, J.K.; Lichtveld, M.Y.; Zijlmans, C.W.; MacDonald-Ottevanger, S.; Shafer, M.; Dahman, C.; Harville, E.W.; Drury, S.; Landburg, G.; Ouboter, P. Exposure to total and methylmercury among pregnant women in Suriname: Sources and public health implications. J. Expo. Sci. Environ. Epidemiol. 2021, 31, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, D.J.X.; Arain, A.; Fernandez, L.E. Mercury exposure, risk factors, and perceptions among women of childbearing age in an artisanal gold mining region of the Peruvian Amazon. Environ. Res. 2019, 179, 108786. [Google Scholar] [CrossRef]
- Santos, E.C.d.O.; Jesus, I.M.d.; Brabo, E.d.S.; Loureiro, E.C.B.; Mascarenhas, A.F.d.S.; Weirich, J.; Câmara, V.d.M.; Cleary, D. Mercury exposures in riverside Amazon communities in Para, Brazil. Environ. Res. 2000, 84, 100–107. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gyamfi, O.; Sorenson, P.B.; Darko, G.; Ansah, E.; Bak, J.L. Human health risk assessment of exposure to indoor mercury vapour in a Ghanaian artisanal small-scale gold mining community. Chemosphere 2020, 241, 125014. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Maramba, N.; Reyes, J.P.; Francisco-Rivera, A.T.; Akagi, H.; Sunio, R.; Panganiban, L.C. Health and environmental assessment of mercury exposure in a gold mining community in Western Mindanao, Philippines. J. Environ. Manag. 2006, 81, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Mayala, L.P.; Veiga, M.M.; Khorzoughi, M.B. Assessment of mine ventilation systems and air pollution impacts on artisanal tanzanite miners at M-erelani, Tanzania. J. Clean. Prod. 2016, 116, 118–124. [Google Scholar] [CrossRef]
- Clemente, E.; Sera, K.; Futatsugawa, S.; Murao, S. PIXE analysis of hair samples from artisanal mining communities in the Acupan region, Benguet, Philippines. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 2004, 219, 161–165. [Google Scholar] [CrossRef]
- Murao, S.; Daisa, E.; Sera, K.; Maglambayan, V.B.; Futatsugawa, S. PIXE measurement of human hairs from a small-scale mining site of the Philippines. Nucl. Instrum. Methods Phys. Res. Sect. B Beam Interact. Mater. At. 2002, 189, 168–173. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Lettmeier, B.; Shoko, D.; Roider, G.; Drasch, G.; Siebert, U. Infants and mothers levels of mercury in breast milk, urine and hair, data from an artisanal and small-scale gold mining area in Kadoma/Zimbabwe. Environ. Res. 2020, 184, 109266. [Google Scholar] [CrossRef]
- Bose-O’Reilly, S.; Lettmeier, B.; Roider, G.; Siebert, U.; Drasch, G. Mercury in breast milk—A health hazard for infants in gold mining areas? Int. J. Hyg. Environ. Health 2008, 211, 615–623. [Google Scholar] [CrossRef]
- Knoblauch, A.M.; Farnham, A.; Ouoba, J.; Zanetti, J.; Müller, S.; Jean-Richard, V.; Utzinger, J.; Wehrli, B.; Brugger, F.; Diagbouga, S.; et al. Potential health effects of cyanide use in artisanal and small-scale gold mining in Burkina Faso. J. Clean. Prod. 2020, 252, 119689. [Google Scholar] [CrossRef]
- Leung, A.M.; Lu, J.L. Environmental Health and Safety Hazards of Indigenous Small-Scale Gold Mining Using Cyanidation in the Philippines. Environ. Health Insights 2016, 10, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Osim, E.E.; Tandayi, M.; Chinyanga, H.M.; Matarira, H.T.; Mudambo, K.K.; Musabayane, C.T. Lung function, blood gases, pH and serum electrolytes of small-scale miners exposed to chrome ore dust on the Great Dyke in Zimbabwe. Trop. Med. Int. Health 1999, 4, 621–628. [Google Scholar] [CrossRef]
- Berky, A.J.; Meyer, J.; Ortiz, E.; Weinhouse, C.; Pan, W.K. Epidemiological Survey on Mitochondrial DNA Copy Number and Mitochondrial DNA Damage in the Peruvian Amazon. In Proceedings of the Environmental Mutagenesis and Genomics Society 47th Annual Meeting, Westin Kansas City, Kansas City, MO, USA, 24–28 September 2016; p. S78. [Google Scholar]
- Rosales-Rimache, J.A.; Elizabeth Malca, N.; Alarcon, J.J.; Chavez, M.; Gonzales, M.A. Genotoxic damage among artisanal and small-scale mining workers exposed to mercury. Rev. Peru Med. Exp. Salud Publica 2013, 30, 595–600. [Google Scholar] [PubMed]
- Berky, A.J.; Ryde, I.T.; Feingold, B.; Ortiz, E.J.; Wyatt, L.H.; Weinhouse, C.; Hsu-Kim, H.; Meyer, J.N.; Pan, W.K. Predictors of mitochondrial DNA copy number and damage in a mercury-exposed rural Peruvian population near artisanal and small-scale gold mining: An exploratory study. Environ. Mol. Mutagen. 2018, 60, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, L.; Permar, S.R.; Ortiz, E.; Berky, A.; Woods, C.W.; Amouou, G.F.; Itell, H.; Hsu-Kim, H.; Pan, W. Mercury Exposure and Poor Nutritional Status Reduce Response to Six Expanded Program on Immunization Vaccines in Children: An Observational Cohort Study of Communities Affected by Gold Mining in the Peruvian Amazon. Int. J. Environ. Res. Public Health 2019, 16, 638. [Google Scholar] [CrossRef]
- Rodríguez, L.H.S.; Flórez-Vargas, O.; Rodríguez-Villamizar, L.A.; Fiallo, Y.V.; Stashenko, E.E.; Ramírez, G. Lack of autoantibody induction by mercury exposure in artisanal gold mining settings in Colombia: Findings and a review of the epidemiology literature. J. Immunotoxicol. 2015, 12, 368–375. [Google Scholar] [CrossRef]
- Essien-Baidoo, J.A.S.; Ephraim, R.K.D.; Nkrumah, D.; Dankyira, D.O. Reduced egfr, elevated urine protein and low level of personal protective equipment compliance among artisanal small scale gold miners at Bibiani-Ghana: A cross-sectional study. BMC Public Health 2017, 17, 601. [Google Scholar] [CrossRef]
- Crompton, P.; Ventura, A.M.; De Souza, J.M.; Santos, E.; Strickland, G.T.; Silbergeld, E. Assessment of mercury exposure and malaria in a Brazilian Amazon riverine community. Environ. Res. 2002, 90, 69–75. [Google Scholar] [CrossRef]
- Sagaon-Teyssier, L.; Balique, H.; Diallo, F.; Kalampalikis, N.; Mora, M.; Bourrelly, M.; Suzan-Monti, M.; Spire, B.; Dembele Keita, B. Prevalence of HIV at the Kokoyo informal gold mining site: What lies behind the glitter of gold with regard to HIV epidemics in Mali? A community-based approach (the ANRS-12339 Sanu Gundo cross-sectional survey). BMJ Open 2017, 7, e016558. [Google Scholar] [CrossRef]
- Green, A.; Jones, A.D.; Sun, K.; Neitzel, R.L. The Association between Noise, Cortisol and Heart Rate in a Small-Scale Gold Mining Community-A Pilot Study. Int. J. Environ. Res. Public Health 2015, 12, 9952–9966. [Google Scholar] [CrossRef]
- Opare, J.; Ohuabunwo, C.; Afari, E.; Wurapa, F.; Sackey, S.; Der, J.; Afakye, K.; Odei, E. Outbreak of cholera in the East Akim Municipality of Ghana following unhygienic practices by small-scale gold miners, November 2010. Ghana. Med. J. 2012, 46, 116–123. [Google Scholar] [PubMed]
- Castilhos, Z.; Villas-Bôas, R.; Miranda, A.; Rodrigues-Filho, S.; Jesus, I.d.; Brabo, E.; Cesar, R.; Lima, M.; Beinhoff, C.; Faial, K.; et al. Human exposure and risk assessment associated with mercury contamination in artisanal gold mining areas in the Brazilian Amazon. Environ. Sci. Pollut. Res. 2015, 22, 11255–11264. [Google Scholar] [CrossRef]
- Elenge, M.M.; De Brouwer, C. Identification of hazards in the workplaces of Artisanal mining in Katanga. Int. J. Occup. Med. Environ. Health 2011, 24, 57–66. [Google Scholar] [CrossRef]
- Bartrem, C.; Tirima, S.; Lindern, I.v.; Braun, M.v.; Worrell, M.C.; Anka, S.M.; Abdullahi, A.; Moller, G. Unknown risk: Co-exposure to lead and other heavy metals among children living in small-scale mining communities in Zamfara State, Nigeria. Int. J. Environ. Health Res. 2014, 24, 304–319. [Google Scholar] [CrossRef]
- Riaz, A.; Khan, S.; Muhammad, S.; Liu, C.; Shah, M.T.; Tariq, M. Mercury contamination in selected foodstuffs and potential health risk assessment along the artisanal gold mining, Gilgit-Baltistan, Pakistan. Environ. Geochem Health 2018, 40, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Villalobos, N.F. Exposición a mercurio de las personas que trabajan en la minería artesanal de oro, Costa Rica, 2015-2016. Poblac. Y Salud Mesoam. 2019, 17. [Google Scholar] [CrossRef]
- Diallo, M.; Soulama, M.; Compaore, N.A.; Kabore, D.S.R.; Ouedraogo, G.A.; Dakoure, P.W.H. Gold panner blast hand. Hand Surg. Rehabil. 2020, 39, 393–401. [Google Scholar] [CrossRef]
- Coulibaly, G.; Sanou, G.; Sanon, M.; Lengani, A.H.Y.; Bonzi, J.Y.; Semde, A. Clinical, Paraclinical, and Evolutionary Profiles of Kidney Failure in Gold Miners Hospitalized in a Nephrological Service in a Sub-Saharan African Country. Int. J. Nephrol. 2020, 2020, 6. [Google Scholar] [CrossRef] [PubMed]
- Umbangtalad, S.; Parkpian, P.; Visvanathan, C.; Delaune, R.D.; Jugsujinda, A. Assessment of Hg contamination and exposure to miners and schoolchildren at a small-scale gold mining and recovery operation in Thailand. J. Environ. Sci. Health A Tox Hazard. Subst. Environ. Eng. 2007, 42, 2071–2079. [Google Scholar] [CrossRef]
- Bello, S.; Nasiru, R.; Garba, N.N.; Adeyemo, D.J. Carcinogenic and non-carcinogenic health risk assessment of heavy metals exposure from Shanono and Bagwai artisanal gold mines, Kano state, Nigeria. Sci. Afr. 2019, 6, e00197. [Google Scholar] [CrossRef]
- Johnbull, O.; Abbassi, B.; Zytner, R.G. Risk assessment of heavy metals in soil based on the geographic information system-Kriging technique in Anka, Nigeria. Environ. Eng. Res. 2019, 24, 150–158. [Google Scholar] [CrossRef]
- Abbas, H.H.; Sakakibara, M.; Sera, K.; Arma, L.H. Mercury Exposure and Health Problems in Urban Artisanal Gold Mining (UAGM) in Makassar, South Sulawesi, Indonesia. Geosciences 2017, 7, 44. [Google Scholar] [CrossRef]
- Lyster, O.; Singo, J. Impacts of COVID-19 on women in ASM. Available online: https://www.levinsources.com/knowledge-centre/insights/impacts-covid-19-women-asm (accessed on 1 November 2020).
- Adewumi, A.J.; Laniyan, T.A.; Xiao, T.; Liu, Y.; Ning, Z. Exposure of children to heavy metals from artisanal gold mining in Nigeria: Evidences from bio-monitoring of hairs and nails. Acta Geochim. 2019, 39, 451–470. [Google Scholar] [CrossRef]
- Hilson, G. Poverty traps in small-scale mining communities: The case of sub-Saharan Africa. Can. J. Dev. Stud. 2012, 33, 180–197. [Google Scholar] [CrossRef]
- Richter, M.S.; Groft, J.Ν.; Prinsloo, L. Ethical issues surrounding studies with vulnerable populations: A case study of South African street children. Int. J. Adolesc Med. Health 2007, 19, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Calys-Tagoe, B.N.L.; Clarke, E.; Robins, T.; Basu, N. A comparison of licensed and un-licensed artisanal and small-scale gold miners (ASGM) in terms of socio-demographics, work profiles, and injury rates. BMC Public Health 2017, 17, 862. [Google Scholar] [CrossRef]
- United Nations. Minamata Convention on Mercury, 1st ed.; United Nations: New York, NY, USA, 2013; Volume 2, p. 50. [Google Scholar]
- Farnham, A.; Cossa, H.; Dietler, D.; Engebretsen, R.; Leuenberger, A.; Lyatuu, I.; Nimako, B.; Zabre, H.R.; Brugger, F.; Winkler, M.S. Investigating Health Impacts of Natural Resource Extraction Projects in Burkina Faso, Ghana, Mozambique, and Tanzania: Protocol for a Mixed Methods Study. Jmir. Res. Protoc. 2020, 9, e17138. [Google Scholar] [CrossRef] [PubMed]
- Rose, S. International Ethical Guidelines for Epidemiological Studies. Am. J. Epidemiol. 2009, 170, 1451–1452. [Google Scholar] [CrossRef]
- Wurr, C.; Cooney, L. Ethical Dilemmas in Population-Level Treatment of Lead Poisoning in Zamfara State, Nigeria. Public Health Ethics 2014, 7, 298–300. [Google Scholar] [CrossRef]
- Calys-Tagoe, B.N.L.; Ovadje, L.; Clarke, E.; Basu, N.; Robins, T. Injury Profiles Associated with Artisanal and Small-Scale Gold Mining in Tarkwa, Ghana. Int. J. Environ. Res. Public Health 2015, 12, 7922–7937. [Google Scholar] [CrossRef]
- Harris, K.M. An integrative approach to health. Demography 2010, 47, 1–22. [Google Scholar] [CrossRef]
- Tsangaris, C.; Kormas, K.; Strogyloudi, E.; Hatzianestis, I.; Neofitou, C.; Andral, B.; Galgani, F. Multiple biomarkers of pollution effects in caged mussels on the Greek coastline. Comp. Biochem. Physiol. C Toxicol. Pharm. 2010, 151, 369–378. [Google Scholar] [CrossRef]
- Hilson, G.; Zolnikov, T.R.; Ortiz, D.R.; Kumah, C. Formalizing artisanal artisanal gold mining under the Minamata convention: Previewing the challenge in Sub-Saharan Africa. Environ. Sci. Policy 2018, 85, 123–131. [Google Scholar] [CrossRef]
- Niane, B.; Guedron, S.; Moritz, R.; Cosio, C.; Ngom, P.M.; Deverajan, N.; Pfeifer, H.R.; Pote, J. Human exposure to mercury in artisanal small-scale gold mining areas of Kedougou region, Senegal, as a function of occupational activity and fish consumption. Environ. Sci. Pollut. Res. Int. 2015, 22, 7101–7111. [Google Scholar] [CrossRef]
- Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- IHME. Global Health Data Exchange (GHDx): GBD Compare and Viz Hub. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 10 November 2020).
- Knoblauch, A.M.; Winkler, M.S.; Archer, C.; Divall, M.J.; Owuor, M.; Yapo, R.M.; Yao, P.A.; Utzinger, J. The epidemiology of malaria and anaemia in the Bonikro mining area, central Cote d'Ivoire. Malar. J. 2014, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Nongrem, W.I.E.; Chhawna, V. An Exploratory Study of Health and Livelihood Conditions of Coal Workers in Jaintia Hills District, Meghalaya. Indian J. Labour Econ. 2020, 63, 499–509. [Google Scholar] [CrossRef]
- Tse, L.A.; Li, Z.M.; Wong, T.W.; Fu, Z.M.; Yu, I.T. High prevalence of accelerated silicosis among gold miners in Jiangxi, China. Am. J. Ind. Med. 2007, 50, 876–880. [Google Scholar] [CrossRef]
- Alcala-Orozco, M.; Caballero-Gallardo, K.; Olivero-Verbel, J. Mercury exposure assessment in indigenous communities from Tarapaca village, Cotuhe and Putumayo Rivers, Colombian Amazon. Environ. Sci. Pollut. Res. Int. 2019, 26, 36458–36467. [Google Scholar] [CrossRef]









| Population Characteristics | Children (<15 Years) | Adolescents and Adults (≥15 Years) | Adults (≥18 Years) | All Ages (≥6 Months) | Age Group Not Defined | Total |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Males and females | 8 | 14 | 50 | 77 | 5 | 154 |
| Female | 1 | 5 | 2 | 1 | 1 | 10 |
| Male | 0 | 0 | 9 | 1 | 1 | 11 |
| Gender not defined | 1 | 0 | 0 | 0 | 0 | 1 |
| Population groups | ||||||
| Miners and residents | 1 | 5 | 21 | 57 | 1 | 85 |
| Miners | 0 | 8 | 32 | 7 | 5 | 52 |
| Residents | 9 | 6 | 8 | 15 | 1 | 39 |
| Total | 10 | 19 | 61 | 79 | 7 | 176 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cossa, H.; Scheidegger, R.; Leuenberger, A.; Ammann, P.; Munguambe, K.; Utzinger, J.; Macete, E.; Winkler, M.S. Health Studies in the Context of Artisanal and Small-Scale Mining: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 1555. https://doi.org/10.3390/ijerph18041555
Cossa H, Scheidegger R, Leuenberger A, Ammann P, Munguambe K, Utzinger J, Macete E, Winkler MS. Health Studies in the Context of Artisanal and Small-Scale Mining: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(4):1555. https://doi.org/10.3390/ijerph18041555
Chicago/Turabian StyleCossa, Hermínio, Rahel Scheidegger, Andrea Leuenberger, Priska Ammann, Khátia Munguambe, Jürg Utzinger, Eusébio Macete, and Mirko S. Winkler. 2021. "Health Studies in the Context of Artisanal and Small-Scale Mining: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 4: 1555. https://doi.org/10.3390/ijerph18041555
APA StyleCossa, H., Scheidegger, R., Leuenberger, A., Ammann, P., Munguambe, K., Utzinger, J., Macete, E., & Winkler, M. S. (2021). Health Studies in the Context of Artisanal and Small-Scale Mining: A Scoping Review. International Journal of Environmental Research and Public Health, 18(4), 1555. https://doi.org/10.3390/ijerph18041555