
Effects of Physical Exercise on Women with Disabilities in South Korea: A Meta-Analysis


Abstract
1. Introduction
- What is the overall effectiveness of physical exercises performed by female PWDs as a dependent variable?
- What are the effect sizes by type of physical exercise (weight-bearing exercise, resistance exercise and aerobic exercise) performed by female PWDs?
- What are the effect sizes for physical exercise among female PWDs by individual characteristics (disability type and age)?
- What are the effect sizes for physical exercise among female PWDs by program characteristics (duration, period and frequency)?
2. Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
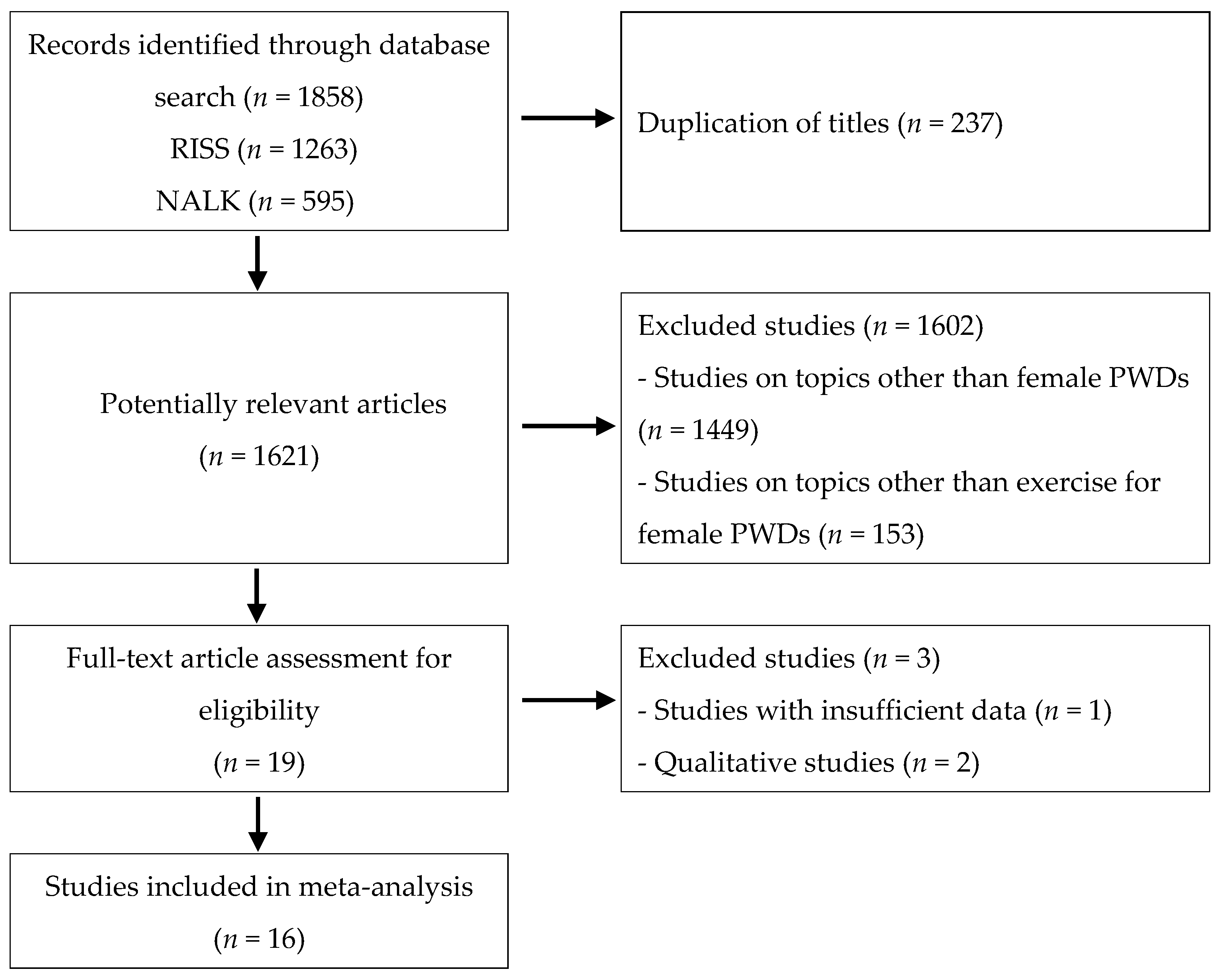
2.3. Search Strategy
2.4. Study Screening and Selection
2.5. Data Extraction
2.6. Effect Size
2.7. Publication Bias and Qualitative Evaluation
3. Results
3.1. Publication Bias and Qualitative Evaluation
3.2. Heterogeneity Test
3.3. Study Characteristics
3.4. Overall Effect Size
3.5. Effect Size of Exercise for Female PWDs by Exercise Outcome and Type
3.6. Control Group
3.7. Effect Size by Individual Characteristics of Female PWDs
3.8. Effect Size by Program Characteristics of Exercise among Female PWDs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casebolt, M.T. Barriers to reproductive health services for women with disability in low-and middle-income countries: A review of the literature. Sex. Reprod. Healthc. 2020, 24, 100485. [Google Scholar] [CrossRef]
- Ruiz-Pérez, I.; Pastor-Moreno, G.; Escribà-Agüir, V.; Maroto-Navarro, G. Intimate partner violence in women with disabilities: Perception of healthcare and attitudes of health professionals. Disabil. Rehabil. 2017, 40, 1059–1065. [Google Scholar] [CrossRef]
- Del Río Ferres, E.; Megías, J.L.; Expósito, F. Gender-based violence against women with visual and physical disabilities. Psicothema 2013, 25, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Narayan, U. Dislocating Cultures: Identities, Traditions, and Third-World Feminism; Routledge: New York, NY, USA, 1997. [Google Scholar]
- World Bank Country and Lending Groups—World Bank Data Help Desk. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 15 March 2021).
- Korea Disabled People’s Development Institute. Yearbook of Disability Statistics. 2020. Available online: http://www.koddi.or.kr (accessed on 24 October 2021).
- Kim, J.Y. Social support effects on life satisfaction of women with disabilities: Focusing on mediating effects of depression. Soc. Welf. Pol. 2020, 47, 33–58. [Google Scholar]
- Ministry of Health and Welfare. Available online: http://www.mohw.go.kr/react/index.jsp (accessed on 15 March 2021).
- Emmett, T.; Alant, E. Women and disability: Exploring the interface of multiple disadvantage. Dev. South. Afr. 2006, 23, 445–460. [Google Scholar] [CrossRef]
- Nosek, M.A.; Foley, C.C.; Hughes, R.B.; Howland, C.A. Vulnerabilities for abuse among women with disabilities. Sex. Disabil. 2001, 19, 177–189. [Google Scholar] [CrossRef]
- Lee, M.H. The convention on the rights of persons with disabilities and the rights of women with disabilities. Ewha J. Gend. Law. 2021, 13, 111–143. [Google Scholar]
- Oh, H.K. Current status of disabled women in Korea and welfare measures. Soc. Welf. Policy. 2002, 14, 141–169. [Google Scholar]
- Lee, J.; Kim, J.; Hong, S. Development of the questionnaire for impeding leisure sports activities of women with disabilities. J. Adapt. Phys. Act. Exerc. 2016, 24, 97–111. [Google Scholar]
- Im, C.K.; Park, B. Understanding of the adjustment process of a female with SCI to disabled sports. J. Adapt. Phys. Act. Exerc. 2010, 18, 113–129. [Google Scholar]
- Kim, W.Y.; Mun, Y. The expansion of disability: Is the pluralistic application of disability study possible? Reinterpretation Disabil. 2010, 1, 65–113. [Google Scholar]
- Reindal, S.M. Disability, gene therapy, and eugenics: A challenge to John Harris. J. Med. Ethics 2000, 26, 89–94. [Google Scholar] [CrossRef]
- Oliver, M. Understanding Disability: From Theory to Practice; Palgrave Macmillan: London, UK, 1996. [Google Scholar]
- Hingorjo, M.R.; Syed, S.; Qureshi, M.A. Role of exercise in osteoporosis prevention current concepts. J. Pak. Med Assoc. 2008, 58, 78–81. [Google Scholar] [PubMed]
- Van der Ploeg, H.P.; van der Beek, A.J.; van der Woude, L.H.; van Mechelen, W. Physical activity for people with a disability: A conceptual model. Sports Med. 2004, 34, 639–649. [Google Scholar] [CrossRef]
- Pyfer, J.; Auxter, D. Principles and Methods of Adapted Physical Education and Recreation; McGraw-Hill Humanities: New York, NY, USA, 2001. [Google Scholar]
- Kim, Y.K. Effects of physical activity participation on physical self-efficacy and happiness index of the disabled. Korean J. Sport 2019, 17, 225–232. [Google Scholar]
- Jeoung, B.J. The effects of sports activities on life satisfaction and obesity for individuals with disabilities. JKPESAGW 2005, 19, 121–130. [Google Scholar]
- Richardson, E.V.; Smith, B.; Papathomas, A. Collective stories of exercise: Making sense of gym experiences with disabled peers. APAQ 2017, 34, 276–294. [Google Scholar] [CrossRef] [PubMed]
- Park, E.K. Effects of dance therapy on the mental health of physically handicapped people. JKPESAGW 2000, 14, 95–103. [Google Scholar]
- Park, Y.S.; Park, W.H. A study on yoga activity programs among obese women with intellectual disabilities. Study Lifelong Educ. Welf. People Disabil. 2015, 19, 97–122. [Google Scholar]
- Dickson, A.; Ward, R.; O’Brien, G.; Allan, D.; O’Carroll, R. Difficulties adjusting to post-discharge life following a spinal cord injury: An interpretative phenomenological analy23sis. Psychol. Health Med. 2011, 16, 463–474. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.J. Benefits and barriers to physical activity for individuals with disabilities: A social-relational model of disability perspective. Disabil. Rehabil. 2013, 35, 2030–2037. [Google Scholar] [CrossRef]
- Kim, M.; Kim, K. Physical activity participation levels, patterns, and settings for women with disabilities. Korean J. Converg. Sci. 2019, 8, 142–156. [Google Scholar]
- Jang, D.H.; Shin, I.S. Historical development of meta-analysis as an educational research methodology. J. Curric. Eval. 2011, 14, 309–332. [Google Scholar] [CrossRef][Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Cooper, H. Research Synthesis and Meta-Analysis: A Step-by-Step Approach; Sage Publications: New York, NY, USA, 2016; Volume 2. [Google Scholar]
- Becker, B.J. Synthesizing standardized mean-change measures. Br. J. Math. Stat. Psychol 1988, 41, 257–278. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Santabarbara, J.; Idoiaga, N.; Ozamiz-Etxebarria, N.; Bueno-Notivol, J. Prevalence of Anxiety in Dental Students during the COVID-19 Outbreak: A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10978. [Google Scholar] [CrossRef] [PubMed]
- Shim, S.; Bae, J.M.; Shin, I.S. Intervention meta-analysis using STATA software. J. Health Info. Stat. 2016, 41, 123–134. [Google Scholar] [CrossRef]
- Hwang, S.D. Meta-Analysis Using, R.; Hakjisa: Seoul, Korea, 2015. [Google Scholar]
- Hedges, L.V.; Olkin, L. Statistical Methods for Meta-Analysis; Academic: New York, NY, USA, 1985. [Google Scholar]
- Song, C.H. The effects of swimming exercise on body composition and bone mineral density in the disabled women. J. Sport Leis. Stud. 2009, 37, 1081–1090. [Google Scholar] [CrossRef]
- Ahn, S.H.; Lee, J.P.; Yoon, J.H.; Kim, S.H.; Oh, J.K. The effect of elastic-band exercise on strength of lower extremities, balance and gait ability in hemiplegia. J. Adapt. Phys. Act. 2009, 17, 51–70. [Google Scholar]
- Kim, S.D.; Lim, E.M. Effects of gymball exercise with aerobic exercise training on physical fitness and metabolic syndrome risk of factors in elderly women with educable mental patients. J. Adapt. Phys. Act. 2009, 17, 183–199. [Google Scholar]
- Park, K.Y.; Lee, Y.S.; Seo, B.W.; Kim, S.J. Impact of sitting volleyball program on the isokinetic muscular strength and mental health of women with disabilities. Korean J. Phys. Mult. Disabil. 2010, 53, 71–87. [Google Scholar]
- Kim, D.W.; Park, K.Y. The effects of participation in 12-week sitting volleyball on body composition, blood lipid, and psychological well-being of physically disabled females. Korean J. Adapt. Phys. Act. 2012, 20, 129–143. [Google Scholar]
- Kim, Y.K. Sitting-volleyball sedentary existence participation and involvement around the female difference physically disabled ego—Resilience and physical self-efficacy, after the due. Korean J. Sport 2018, 16, 61–67. [Google Scholar]
- Lee, S.A. The effect of wheelchair-tennis for isokinetic muscular strength and physical self efficiency in women with physical disabilities. J. Rehab. Res. 2011, 15, 107–128. [Google Scholar]
- Lee, S.A. Wheel chair dance program participation in the blood geological features and the psychological well of the feminine delay disabled person it affects round. Korean Res. J. Danc. Documetation 2012, 27, 85–104. [Google Scholar]
- Kim, H.C.; Kim, D.W.; Kim, H.S.; Lee, Y.A. The effects of horse riding program on foot pressure in middle-aged women with visual impairment. Korean J. Adapt. Phys. Act. 2013, 21, 55–67. [Google Scholar]
- Lee, Y.A.; Lee, S.A. Effects of horse riding program participation on resilience in middle-aged women with visual impairment. J. Rehabil. Res. 2015, 19, 321–344. [Google Scholar]
- Kang, M.C.; Kim, D.W. The influence of participation in badminton class of female people with physical disabilities on physical respect and sports value perception. Korean J. Sport Sci. 2020, 18, 121–127. [Google Scholar]
- Park, H.R. The effects of yogic exercise training on physical fitness and body composition of factors in elderly women with educable mental patients. J. Korean Soc. Danc. Sci. 2011, 24, 105–118. [Google Scholar]
- Choi, M.Y.; Chang, I.H. Effect of Korean dance on body composition and blood lipids in female with mental retardation. J. Coach. Dev. 2010, 12, 269–278. [Google Scholar]
- Kwon, Y.W. The effect of aerobic and resistance training on body composition and inflammatory factors in mentally retarded female. Korean J. Growth Dev. 2011, 19, 297–303. [Google Scholar]
- Lee, Y.A.; Kim, D.W. Effects of swimming program participation on objectified body consciousness and exercise adherence in middle-aged women physically disabled. Korean J. Phys. Educ. 2015, 54, 633–642. [Google Scholar]
- Kim, D.W. The effect of participation in swimming class in middle-aged women with physical disabilities on sport value recognition and exercise commitment. Korean J. Sport 2018, 16, 521–527. [Google Scholar]
- Saxton, M. Hard bodies: Exploring historical and cultural factors in disabled people’s participation in exercise; applying critical disability theory. Sport Soc. 2018, 21, 22–39. [Google Scholar] [CrossRef]
- Durstine, J.L.; Painter, P.; Franklin, B.A.; Morgan, D.; Pitetti, K.H.; Roberts, S.O. Physical activity for the chronically ill and disabled. Sports Med. 2000, 30, 207–219. [Google Scholar] [CrossRef]
- Junker, L.; Carlberg, E.B. Factors that affect exercise participation among people with physical disabilities. Adv. Physiother. 2011, 13, 18–25. [Google Scholar] [CrossRef]
- Top, E.; Akkoyunlu, Y.; Akil, M. Analysis of the influence of a twelve month swimming exercise on mentally disabled individuals’ changes in physical strength level. Int. J. Phys. Educ. Sports Health 2015, 2, 315–322. [Google Scholar]
- Son, B.K.; Choi, E.M.; Kwon, L.S. Physical recovery through health management education for the disabled or the elderly. J. Wellbeing Manag. Appl. Psychol. 2021, 4, 27–34. [Google Scholar]
- Kim, S.E.; Jeong, Y. A qualitative study on marathon cub activity experiences of woman with intellectual disabilities. J. Rehab. Res. 2017, 21, 149–176. [Google Scholar]
- Chun, H.J.; Lee, S.H.; Hong, Y.J. A survey on the current status of participation of lifetime sports for women with disabilities. JKPESAGW 2008, 22, 191–204. [Google Scholar]
- Chun, H.J.; Shim, Y.S. The influence of perceived motivational climate on sports commitment and satisfaction among elite athletes with physical disabilities. JKPESAGW 2015, 29, 301–312. [Google Scholar]



{kind=link}
{kind=link}
| Model | Q-Value | df (Q) | p-Value | I-Squared |
|---|---|---|---|---|
| Fixed | 343.423 | 126 | 0.000 | 63.311 |
| No. | Researcher | Effect Size | Participant’s Disability Type | Participant’s Age | Number of Participants | Exercise Type | Effect of Exercise | Duration of Exercise (min) | Frequency of Exercise/per Week | Period of Exercise (Weeks) | Total Number of Sessions |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Song (2009) | 0.866 | Physical disability | Not indicated | 6 | Water exercise | Changes in body composition | 60 | 5 | 8 | 40 |
| 2 | Ahn et al. (2009) | 0.975 | Hemiplegia after stroke | 50s and 60s | 6 | Elastic band exercise | Changes in physical strength | 50 | 6 | 6 | 36 |
| 3 | Kim & Lim (2009) | 1.037 | Mental disorder | 40s and 50s | 10 | Aerobic and gym ball exercise | Changes in body composition | 50 | 3 | 16 | 48 |
| 4 | Park et al. (2010) | 1.011 | Physical disability | 40s and 50s | 11 | Sitting volleyball | Changes in muscle strength | 120 | 3 | 12 | 36 |
| 5 | Choi & Jang (2010) | 0.838 | Intellectual disability | 30s and 40s | 10 | Korean dance | Changes in body composition | 60 | 1 | 8 | 8 |
| 6 | Gwon (2011) | 0.598 | Intellectual disability | 20s | 11 | Aerobics | Changes in body composition | 40 | 4 | 12 | 48 |
| 7 | Park (2011) | 0.558 | Mental disorder | 40s and 50s | 10 | Yoga | Changes in physical strength | 50–60 | 3 | 12 | 36 |
| 8 | Lee (2011) | 0.669 | Physical dysfunction and joint disorder | 40s | 10 | Wheelchair tennis | Changes in muscle strength | 60 | 3 | 12 | 36 |
| 9 | Kim & Park (2012) | 0.627 | Physical disability | 40s | 10 | Sitting volleyball | Changes in body composition | 60 | 3 | 12 | 36 |
| 10 | Lee (2012) | 0.821 | Physical disability | 40s | 10 | Wheelchair dance | Changes in blood lipids | 60 | 3 | 24 | 72 |
| 11 | Kim et al. (2013) | 0.537 | Visual impairment | 40s | 10 | Horseback riding | Changes in muscle strength | 45–50 | 3 | 12 | 36 |
| 12 | Lee & Kim (2015) | 0.903 | Physical disability | 40s | 11 | Swimming | Psychological change | 50 | 3 | 15 | 45 |
| 13 | Lee & Lee (2015) | 0.589 | Visual impairment | 40s | 10 | Horseback riding | Psychological change | 45–50 | 3 | 12 | 36 |
| 14 | Kim (2018) | 1.319 | Physical disability | 30s and 40s | 10 | Sitting volleyball | Psychological change | 60 | 3 | 16 | 48 |
| 15 | Kim (2018) | 1.748 | Physical disability | 40s | 10 | Swimming | Psychological change | 60 | 3 | 12 | 36 |
| 16 | Kang & Kim (2020) | 0.088 | Physical disability | 30s and 40s | 9 | Badminton | Psychological change | 60 | 3 | 8 | 24 |
| k | ES | 95% CI | Q-Value | df | p-Value | I2 | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Total | 127 | 0.808 | 0.665 | 0.950 | 343.423 | 126 | 0.000 | 63.311 |
| Category | k | d | SE | 95% CI | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Exercise outcome | |||||
| Changes in muscle strength | 12 | 2.407 | 0.473 | 1.481 | 3.334 |
| Changes in body composition | 28 | 0.336 | 0.088 | 0.164 | 0.508 |
| Changes in physical strength | 25 | 0.545 | 0.108 | 0.332 | 0.758 |
| Psychological change | 37 | 1.325 | 0.183 | 1.013 | 1.637 |
| Mental health change | 7 | 0.491 | 0.164 | 0.170 | 0.812 |
| Inflammatory factor changes | 6 | 0.422 | 0.183 | 0.064 | 0.780 |
| Changes in blood lipids | 12 | 0.370 | 0.131 | 0.113 | 0.626 |
| Exercise type | |||||
| Strength exercise | 6 | 0.423 | 0.185 | 0.060 | 0.785 |
| Badminton | 6 | 1.194 | 0.228 | 0.747 | 1.641 |
| Swimming | 10 | 1.648 | 0.304 | 1.051 | 2.245 |
| Water exercise | 4 | 0.292 | 0.292 | 0.279 | 0.864 |
| Horseback riding | 13 | 3.080 | 0.408 | 2.280 | 3.881 |
| Yoga | 9 | 0.358 | 0.151 | 0.063 | 0.653 |
| Aerobic exercise | 20 | 0.304 | 0.121 | 0.068 | 0.541 |
| Sitting volleyball | 24 | 0.625 | 0.108 | 0.413 | 0.836 |
| Elastic band exercise | 16 | 0.742 | 0.170 | 0.409 | 1.074 |
| Korean dance | 6 | 0.090 | 0.183 | 0.268 | 0.448 |
| Wheelchair dance | 8 | 0.276 | 0.160 | 0.037 | 0.588 |
| Wheelchair tennis | 5 | 1.238 | 0.220 | 0.806 | 1.670 |
| Category | k | d | SE | 95% CI | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Disability type | |||||
| Hemiplegia after stroke | 16 | 0.742 | 0.170 | 0.409 | 1.074 |
| Visual impairment | 13 | 3.080 | 0.408 | 2.280 | 3.881 |
| Mental disorder | 23 | 0.325 | 0.094 | 0.141 | 0.510 |
| Intellectual disability | 18 | 0.307 | 0.105 | 0.100 | 0.513 |
| Physical dysfunction | 5 | 1.238 | 0.220 | 0.806 | 1.670 |
| Physical disability | 52 | 0.798 | 0.099 | 0.605 | 0.991 |
| Age | |||||
| 20s | 12 | 0.415 | 0.129 | 0.162 | 0.668 |
| 30s–40s | 15 | 0.886 | 0.216 | 0.464 | 1.308 |
| 40s | 46 | 1.390 | 0.169 | 1.058 | 1.722 |
| 40s–50s | 34 | 0.404 | 0.077 | 0.254 | 0.554 |
| 50s–60s | 16 | 0.742 | 0.170 | 0.409 | 1.074 |
| Not indicated | 4 | 0.292 | 0.292 | −0.279 | 0.864 |
| Category | k | d | SE | 95% CI | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Duration of session | |||||
| 40 min | 12 | 0.415 | 0.129 | 0.162 | 0.668 |
| 45–50 min | 13 | 3.080 | 0.408 | 2.280 | 3.881 |
| 50 min | 35 | 0.713 | 0.134 | 0.450 | 0.976 |
| 50–60 min | 9 | 0.358 | 0.151 | 0.063 | 0.653 |
| 60 min | 47 | 0.702 | 0.095 | 0.515 | 0.888 |
| 120 min | 11 | 0.558 | 0.131 | 0.300 | 0.815 |
| Frequency per week | |||||
| 1 session | 6 | 0.090 | 0.183 | −0.268 | 0.448 |
| 3 sessions | 89 | 0.963 | 0.095 | 0.776 | 1.150 |
| 4 sessions | 12 | 0.415 | 0.129 | 0.162 | 0.668 |
| 5 sessions | 4 | 0.292 | 0.292 | −0.279 | 0.864 |
| 6 sessions | 16 | 0.742 | 0.170 | 0.409 | 1.074 |
| Period (weeks) | |||||
| 6 | 16 | 0.742 | 0.170 | 0.409 | 1.074 |
| 8 | 16 | 0.533 | 0.155 | 0.230 | 0.837 |
| 12 | 65 | 0.950 | 0.109 | 0.737 | 1.164 |
| 15 | 5 | 1.974 | 0.640 | 0.719 | 3.228 |
| 16 | 17 | 0.555 | 0.154 | 0.252 | 0.857 |
| 24 | 8 | 0.276 | 0.160 | −0.037 | 0.588 |
| Total number of sessions | |||||
| 8 | 6 | 0.090 | 0.183 | −0.268 | 0.448 |
| 24 | 6 | 1.194 | 0.228 | 0.747 | 1.641 |
| 36 | 69 | 1.024 | 0.111 | 0.806 | 1.242 |
| 40 | 4 | 0.292 | 0.292 | −0.275 | 0.864 |
| 45 | 5 | 1.974 | 0.640 | 0.719 | 3.228 |
| 48 | 29 | 0.478 | 0.091 | 0.300 | 0.657 |
| 72 | 8 | 0.276 | 0.160 | −0.037 | 0.588 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Lee, S. Effects of Physical Exercise on Women with Disabilities in South Korea: A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12791. https://doi.org/10.3390/ijerph182312791
Kim Y, Lee S. Effects of Physical Exercise on Women with Disabilities in South Korea: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12791. https://doi.org/10.3390/ijerph182312791
Chicago/Turabian StyleKim, Yucheon, and Songyi Lee. 2021. "Effects of Physical Exercise on Women with Disabilities in South Korea: A Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12791. https://doi.org/10.3390/ijerph182312791
APA StyleKim, Y., & Lee, S. (2021). Effects of Physical Exercise on Women with Disabilities in South Korea: A Meta-Analysis. International Journal of Environmental Research and Public Health, 18(23), 12791. https://doi.org/10.3390/ijerph182312791