
Use of Antibiotic Treatment in Pregnancy and the Risk of Several Neonatal Outcomes: A Population-Based Study

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Background
2. Methods
2.1. Setting
2.2. Study Cohort
2.3. Exposure to Antibiotics
2.4. Outcomes
2.5. Maternal Covariates
2.6. Statistical Analyses
2.7. Sensitivity and Subgroup Analyses
3. Results
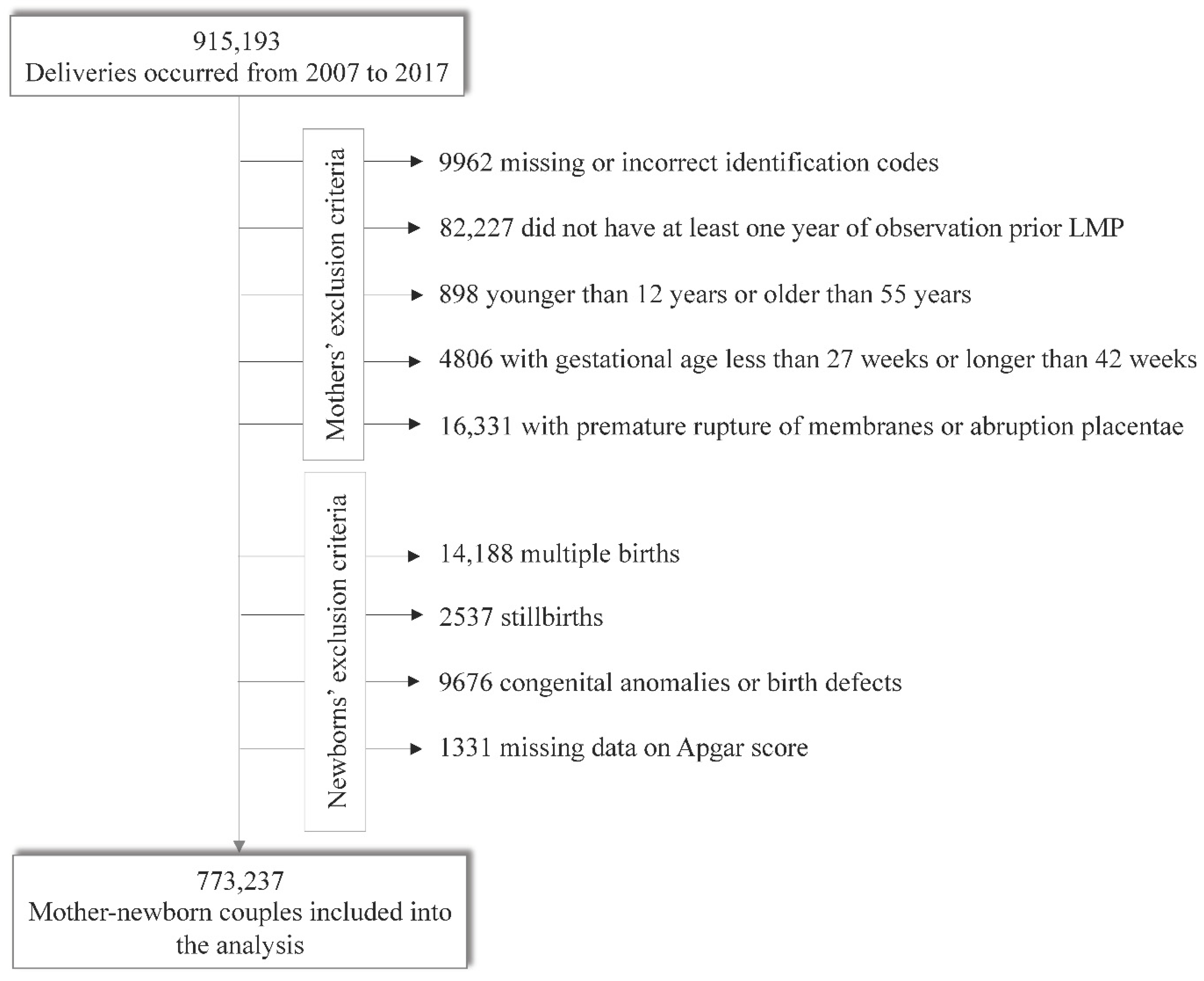
3.1. Study Cohort and Outcomes
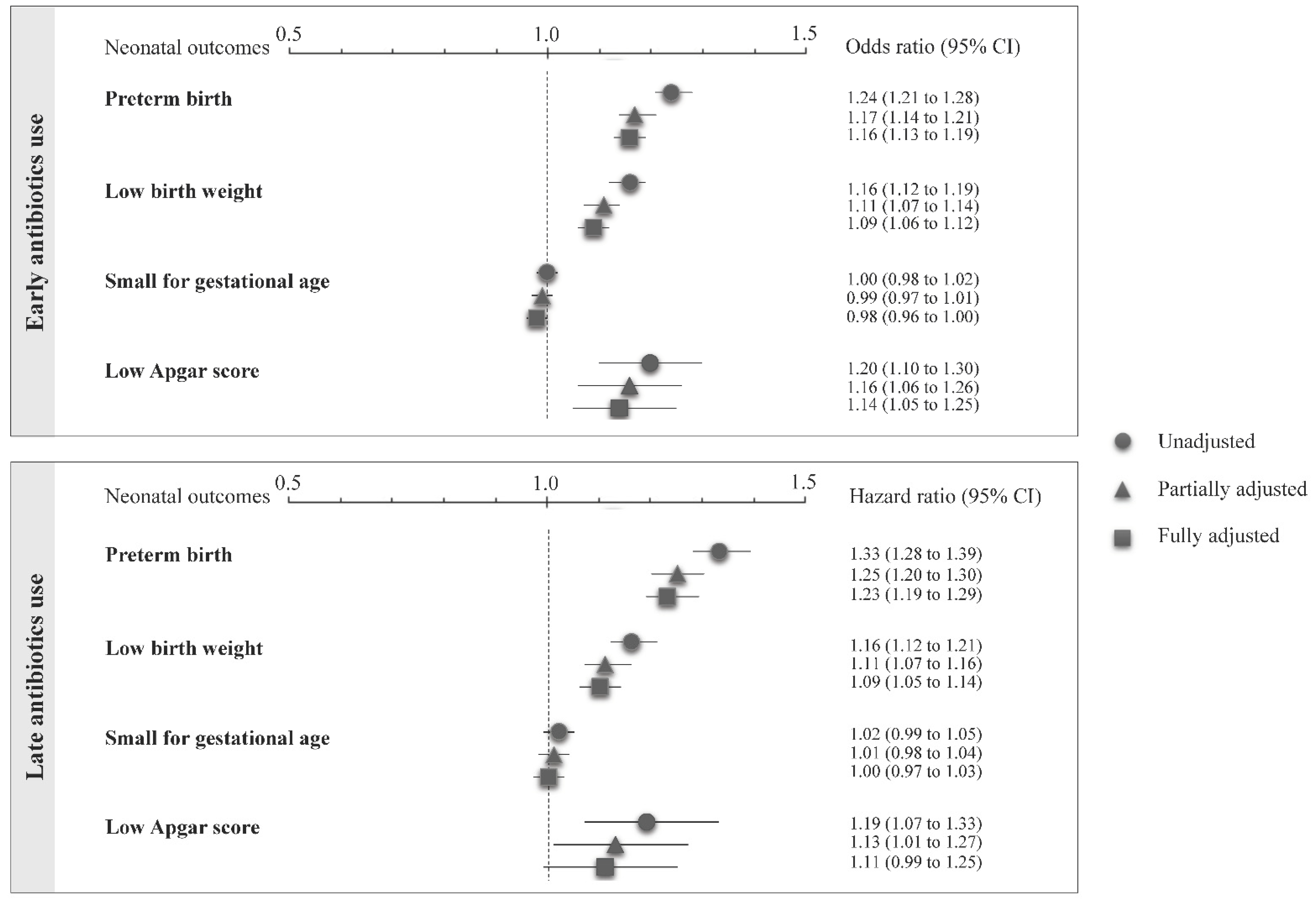
3.2. Use of Antibiotics and Neonatal Outcomes
4. Discussion
- Limited evidence is available on the safety and efficacy of antimicrobials during pregnancy.
- The concerns about the implications of antibiotics use during pregnancy on adverse neonatal outcomes involve the need for observational studies to assess the potential association between the use of antibiotics during pregnancy and several neonatal outcomes.
- Our results suggested an increased risk of several neonatal outcomes in women who were exposed to antibiotics during pregnancy.
- How the observed effects are due to the infections or the direct action of the considered antimicrobial drugs remains an important open question.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Heikkila, A.M. Antibiotics in pregnancy—A prospective cohort study on the policy of antibiotic prescription. Ann. Med. 1993, 5, 467–471. [Google Scholar] [CrossRef]
- Harbison, A.F.; Polly, D.M.; Musselman, M.E. Antiinfective therapy for pregnant or lactating patients in the emergency department. Am. J. Health Syst. Pharm. 2015, 3, 189–197. [Google Scholar] [CrossRef]
- Lamont, H.F.; Blogg, H.J.; Lamont, R.F. Safety of antimicrobial treatment during pregnancy: A current review of resistance, immunomodulation and teratogenicity. Expert. Opin. Drug Saf. 2014, 12, 1569–1581. [Google Scholar] [CrossRef]
- Miller, J.E.; Wu, C.; Pedersen, L.H.; de Klerk, N.; Olsen, J.; Burgner, D.P. Maternal antibiotic exposure during pregnancy and hospitalization with infection in offspring: A population–based cohort study. Int. J. Epidemiol. 2018, 47, 561–571. [Google Scholar] [CrossRef]
- Broe, A.; Pottegård, A.; Lamont, R.; Jørgensen, J.; Damkier, P. Increasing use of antibiotics in pregnancy during the period 2000–2010: Prevalence, timing, category, and demographics. BJOG 2014, 121, 988–996. [Google Scholar] [CrossRef] [Green Version]
- Nahum, G.G.; Uhl, K.; Kennedy, D.L. Antibiotic use in pregnancy and lactation: What is and is not known about teratogenic and toxic risks. Obstet. Gynecol. 2006, 107, 1120–1138. [Google Scholar] [CrossRef]
- Costantine, M.M. Physiologic and pharmacokinetic changes in pregnancy. Front Pharmacol. 2014, 65, 1–5. [Google Scholar] [CrossRef]
- Dunn, A.B.; Jordan, S.; Baker, B.J.; Carlson, N.S. The maternal infant microbiome Considerations for Labor and Birth. Wolters Kluwer Health 2017, 42, 318–325. [Google Scholar]
- Chernikova, D.A.; Koestler, D.C.; Hoen, A.G.; Housman, M.L.; Hibberd, P.L.; Moore, J.H.; Madan, J.C. Fetal exposures and perinatal influences on the stool microbiota of premature infants. J. Matern. Fetal. Neonatal. Med. 2016, 29, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuperman, A.A.; Koren, O. Antibiotic use during pregnancy: How bad is it? BMC Med. 2016, 14, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trifirò, G.; Gini, R.; Barone-Adesi, F.; Beghi, E.; Cantarutti, A.; Capuano, A.; Carnovale, C.; Clavenna, A.; Dellagiovanna, M.; Ferrajolo, C.; et al. The Role of European Healthcare Databases for Post-Marketing Drug Effectiveness, Safety and Value Evaluation: Where Does Italy Stand? Drug Saf. 2018, 42, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Cantarutti, A.; Franchi, M.; Rea, F.; Merlino, L.; Corrao, G. Use of Nimesulide during Early Pregnancy and the Risk of Congenital Malformations: A Population-Based Study from Italy. Adv. Ther. 2018, 35, 981–992. [Google Scholar] [CrossRef]
- Cantarutti, A.; Merlino, L.G.; Giaquinto, C.; Corrao, G. Use of antidepressant medication in pregnancy and adverse neonatal outcomes: A population-based investigation. Pharmacoepidemiol. Drug Saf. 2017, 26, 1100–1108. [Google Scholar] [CrossRef]
- Cantarutti, A.; Merlino, L.; Monzani, E.; Giaquinto, C.; Corrao, G. Is the Risk of Preterm Birth and Low Birth Weight Affected by the Use of Antidepressant Agents during Pregnancy? A Population-Based Investigation. PLoS ONE 2016, 11, e0168115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawn, J.; Gravett, M.G.; Nunes, T.M.; Rubens, C.; Stanton, C. Global report on preterm birth and stillbirth (1 of 7): Definitions, description of the burden and opportunities to improve data. BMC Pregnancy Childbirth 2010, 10, S1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Bernabé, J.V.; Soriano, T.; Albaladejo, R.; Juarranz, M.; Calle, M.E.; Martínez, D.; Domínguez-Rojas, V. Risk factor for low birth weight: A review. Eur. J. Obstet. Gynecol. 2004, 116, 3–15. [Google Scholar] [CrossRef]
- Parazzini, F.; Cortinovis, I.; Bortolus, R.; Zanardo, V. Weight at birth between 23a and 42a weeks of gestation in Italy. Med. Surg. Ped. 1998, 20, 93–97. [Google Scholar]
- Casey, B.M.; McIntire, D.D.; Leveno, K.J. The continuing value of the Apgar score for the assessment of newborn infants. N. Engl. J. Med. 2001, 344, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef] [Green Version]
- Matok, I.; Azoulay, L.; Yin, H.; Suissa, S. Immortal Time Bias in Observational Studies of Drug Effects in Pregnancy. Birth Defects Res. A Clin. Mol. Teratol. 2014, 100, 658–662. [Google Scholar] [CrossRef]
- Corrao, G.; Rea, F.; Franchi, M.; Beccalli, B.; Locatelli, A.; Cantarutti, A. Warning of Immortal Time Bias When Studying Drug Safety in Pregnancy: Application to Late Use of Antibiotics and Preterm Delivery. Int. J. Environ. Res. Public Health 2020, 17, 6465. [Google Scholar] [CrossRef]
- Burt, R.D.; Vaughan, T.L.; Daling, J.R. Evaluating the risks of cesarean section: Low Apgar score in repeat C-section and vaginal deliveries. Am. J. Public Health 1988, 78, 1312–1314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annibale, D.J.; Hulsey, T.C.; Wagner, C.L.; Southgate, W.M. Comparative neonatal morbidity of abdominal and vaginal deliveries after uncomplicated pregnancies. Arch. Pediatr. Adolesc. Med. 1995, 149, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.A.; Lamy-Filho, F.; Alves, M.T.; Coimbra, L.C.; Bettiol, H.; Barbieri, M.A. Risk factors for low birthweight in north-east Brazil: The role of caesarean section. Paediatr. Perinat. Epidemiol. 2001, 15, 257–264. [Google Scholar] [CrossRef]
- Bookstaver, P.B.; Bland, C.; Griffin, B.L.; Stover, K.R.; Eiland, L.S.; McLaughlin, M.M. A Review of Antibiotic Use in Pregnancy. Pharmacotherapy 2015, 35, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- Newman, S.C. Biostatistical Methods in Epidemiology; Wiley Series in Probability and Statistics; John Wiley & Sons: Hoboken, NJ, USA, 2002. [Google Scholar]
- Vidal, A.C.; Murphy, S.K.; Murtha, A.P.; Schildkraut, J.M.; Soubry, A.; Huang, Z.; Hoyo, C. Associations between antibiotic exposure during pregnancy, birthweight and aberrant methylation at imprinted genes among offspring. Int. J. Obes. 2013, 37, 907–913. [Google Scholar] [CrossRef] [Green Version]
- Mensah, K.B.; Opoku–Agyeman, K.; Ansah, C. Antibiotic use during pregnancy: A retrospective study of prescription patterns and birth outcomes at an antenatal clinic in rural Ghana. J. Pharm. Policy Pract. 2017, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Jepsen, P.; Skriver, M.V.; Floyd, A.; Lipworth, L.; Schønheyder, H.C.; Sørensen, H.T. A population-based study of maternal use of amoxicillin and pregnancy outcome in Denmark. Br. J. Clin. Pharmacol. 2003, 55, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Briggs, G.G.F.R. Drugs in Pregnancy and Lactation; Williams and Wilkins: Baltimore, MD, USA, 2014. [Google Scholar]
- United States National Library of Medicine. DailyMed. Available online: http://dailymed.nlm.nih.gov/dailymed/index.cfm (accessed on 27 August 2020).
- Dinur, A.B.; Koren, G.; Matok, I.; Wiznitzer, A.; Uziel, E.; Gorodischer, R.; Levy, A. Fetal safety of macrolides. Antimicrob. Agents Chemother. 2013, 57, 3307–3311. [Google Scholar] [CrossRef] [Green Version]
- Costeloe, K.; Hennessy, E.; Gibson, A.T.; Marlow, N.; Wilkinson, A.R. The EPICure study: Outcomes to discharge from hospital for infants born at the threshold of viability. Pediatrics 2000, 106, 659–671. [Google Scholar] [CrossRef] [Green Version]
- Petrou, S.; Abangma, G.; Johnson, S.; Wolke, D.; Marlow, N. Costs and health utilities associated with extremely preterm birth: Evidence from the EPICure study. Value Health 2009, 12, 1124–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morency, A.-M.; Bujold, E. The Effect of Second-Trimester Antibiotic Therapy on the Rate of Preterm Birth. J. Obstet. Gynaecol. Can. 2007, 29, 35–44. [Google Scholar] [CrossRef]
- Yoon, B.H.; Romero, R.; Bin Moon, J.; Shim, S.-S.; Kim, M.; Kim, G.; Jun, J.K. Clinical significance of intra-amniotic inflammation in patients with preterm labor and intact membranes. Am. J. Obstet. Gynecol. 2001, 185, 1130–1136. [Google Scholar] [CrossRef]
- Jacobsson, B.; Mattsby-Baltzer, I.; Andersch, B.; Bokström, H.; Holst, R.M.; Wennerholm, U.B.; Hagberg, H. Microbial invasion and cytokine response in amniotic fluid in a Swedish population of women in preterm labor. Acta Obstet. Gynecol. Scand. 2003, 82, 120–128. [Google Scholar] [CrossRef]
- Wahbeh, C.J.; Hill, G.B.; Eden, R.D.; Gall, S.A. Intra-amniotic bacterial colonization in premature labor. Am. J. Obstet. Gynecol. 1984, 148, 739–743. [Google Scholar] [CrossRef]
- Greig, P.C. The diagnosis of intrauterine infection in women with preterm premature rupture of membranes. Clin. Obstet. Gynecol. 1998, 41, 849–863. [Google Scholar] [CrossRef]
- Watts, D.H.; Krohn, M.A.; Hillier, S.L.; Eschenbach, D.A. The association of occult amniotic fluid infection with gestational age and neonatal outcome among women in preterm labor. Obstet. Gynecol. 1992, 79, 351–357. [Google Scholar] [CrossRef] [PubMed]
- De Tejada, B.M. Antibiotic Use and Misuse during Pregnancy and Delivery: Benefits and Risks. Int. J. Environ. Res. Public Health 2014, 11, 7993–8009. [Google Scholar] [CrossRef] [Green Version]
- Gavrielov-Yusim, N.; Friger, M. Use of administrative medical databases in population-based research. J. Epidemiol. Community Health 2014, 68, 283–287. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics | Early Users (a) | No Users (a) | SD | Late Users (b) | No Users (b) | SD |
|---|---|---|---|---|---|---|
| (N = 132,024) | (N = 564,292) | (N = 76,921) | (N = 696,316) | |||
| Socio-demographics | ||||||
| Age, mean (SD) (c) | 32.7 (5.3) | 32.3 (5.1) | 0.08 | 32.2 (5.4) | 32.4 (5.1) | −0.04 |
| No Italian nationality (c,d) | 29,180 (23.03%) | 121,975 (22.48%) | 0.01 | 18,725 (25.39%) | 151,155 (22.58%) | 0.07 |
| Unmarried status (c,d) | 40,353 (31.85%) | 167,681 (30.9%) | 0.02 | 22,615 (30.66%) | 208,034 (31.08%) | −0.01 |
| Education lower than high school (c,d) | 35,523 (28.03%) | 133,125 (24.53%) | 0.08 | 22,842 (30.97%) | 168,648 (25.2%) | 0.13 |
| Unemployed (c,d) | 35,892 (28.32%) | 142,578 (26.27%) | 0.05 | 23,772 (32.23%) | 178,470 (26.66%) | 0.12 |
| Previous miscarriages (c) | 34,601 (26.21%) | 134,620 (28.86%) | −0.06 | 20,505 (26.66%) | 169,221 (24.3%) | 0.05 |
| Primigravida (c,d) | 37,068 (29.25%) | 17,4241 (32.11%) | −0.06 | 20,601 (27.93%) | 211,309 (31.57%) | −0.08 |
| Comorbidities (e) | ||||||
| Substance dependence | 52 (0.04%) | 155 (0.03%) | 0.01 | 37 (0.05%) | 207 (0.03%) | 0.01 |
| Infection | 4383 (3.32%) | 11,955 (2.12%) | 0.07 | 4674 (6.08%) | 27,942 (4.01%) | 0.09 |
| Hypertension | 232 (0.18%) | 842 (0.15%) | 0.01 | 118 (0.15%) | 1074 (0.15%) | 0 |
| Preeclampsia | 105 (0.08%) | 393 (0.07%) | 0 | 61 (0.08%) | 498 (0.07%) | 0 |
| Diabetes | 328 (0.25%) | 1325 (0.22%) | 0.01 | 211 (0.27%) | 1563 (0.22%) | 0.01 |
| Obesity and overweight | 149 (0.11%) | 372 (0.07%) | 0.01 | 123 (0.16%) | 521 (0.07%) | 0.03 |
| Dyslipidaemia | 12 (0.01%) | 37 (0.01%) | 0 | 10 (0.01%) | 49 (0.01%) | 0 |
| Pain | 609 (0.46%) | 2135 (0.38%) | 0.01 | 399 (0.52%) | 2744 (0.39%) | 0.02 |
| C-section (f) | 39,092 (29.61%) | 150,491 (26.67%) | 0.07 | 21,449 (27.88%) | 189,583 (27.23%) | 0.01 |
| Concomitant medications (e) | ||||||
| NSAIDs | 8680 (6.57%) | 23,117 (4.1%) | 0.11 | 5171 (6.72%) | 31,797 (4.57%) | 0.09 |
| Drugs for acid-related disorders | 14,264 (10.8%) | 38,733 (6.86%) | 0.14 | 8274 (10.73%) | 52,997 (7.61%) | 0.11 |
| Healthcare utilization (e) | ||||||
| Hospital admissions | 26,706 (20.23%) | 106,000 (18.78%) | 0.04 | 1586 (20.62%) | 132,706 (19.06%) | 0.04 |
| No. of distinct prescription drugs, excluding antibiotics | ||||||
| =1 | 40,903 (30.98%) | 16,8528 (29.87%) | 0.02 | 23,531 (30.59%) | 209,431 (30.08%) | 0.01 |
| ≥2 | 43,965 (33.3%) | 12,6129 (22.35%) | 0.25 | 24,831 (32.28%) | 170,094 (24.43%) | 0.17 |
| Early Users | Late Users | |||||
|---|---|---|---|---|---|---|
| Entire Cohort | Women Who Experienced Neonatal Outcome | OR (95% CI) | Entire Cohort | Women Who Experienced Neonatal Outcome | HR (95% CI) | |
| Preterm birth | ||||||
| Cephalosporins | 7816 (1.1%) | 429 (5.5%) | 1.23 (1.12–1.36) | 4113 (0.5%) | 204 (4.9%) | 1.40 (1.22 to 1.61) |
| Penicillins | 84,211 (12.1%) | 3970 (4.7%) | 1.12 (1.08–1.16) | 45,285 (5.9%) | 1679 (3.7%) | 1.12 (1.07 to 1.18) |
| Macrolides | 24,763 (3.6%) | 1303 (5.3%) | 1.22 (1.15–1.30) | 8402 (1.1%) | 472 (5.6%) | 1.58 (1.44 to 1.73) |
| Fluoroquinolones | 6352 (0.9%) | 310 (4.9%) | 1.08 (0.96–1.21) | 1340 (0.2%) | 57 (4.2%) | 1.21 (0.93 to 1.57) |
| Other | 24,715 (3.6%) | 1243 (5.0%) | 1.18 (1.11–1.25) | 12,158 (1.6%) | 510 (4.2%) | 1.23 (1.13 to 1.53) |
| Homogeneity test (p-value) | 0.0448 | <0.0001 | ||||
| Low birth weight | ||||||
| Cephalosporins | 7816 (1.1%) | 411 (5.3%) | 1.10 (1.00–1.22) | 4675 (0.6%) | 217 (4.6%) | 1.26 (1.11 to 1.44) |
| Penicillins | 84,211 (12.1%) | 4050 (4.8%) | 1.05 (1.01–1.08) | 52,923 (6.8%) | 1967 (3.7%) | 1.05 (0.99 to 1.09) |
| Macrolides | 24,763 (3.6%) | 1347 (5.4%) | 1.17 (1.11–1.24) | 9316 (1.2%) | 462 (5.0%) | 1.33 (1.21 to 1.46) |
| Fluoroquinolones | 6352 (0.9%) | 331 (5.2%) | 1.09 (0.97–1.21) | 1550 (2.2%) | 71 (4.6%) | 1.25 (0.99 to 1.58) |
| Other | 24,715 (3.6%) | 1317 (5.3%) | 1.16 (1.09–1.23) | 13,885 (1.8%) | 534 (3.8%) | 1.05 (0.96 to 1.14) |
| Homogeneity test (p-value) | 0.0026 | <0.0001 | ||||
| Small for gestational age | ||||||
| Cephalosporins | 7816 (1.1%) | 575 (7.4%) | 0.99 (0.92 to 1.09) | 4675 (0.6%) | 345 (7.4%) | 1.10 (0.99 to 1.22) |
| Penicillins | 84,211 (12.1%) | 6045 (7.2%) | 0.97 (0.94 to 1.00) | 52,923 (6.8%) | 3696 (7.0%) | 1.00 (0.96 to 1.03) |
| Macrolides | 24,763 (3.6%) | 1858 (7.5%) | 1.02 (0.97 to 1.07) | 9316 (1.2%) | 673 (7.2%) | 1.07 (0.99 to 1.15) |
| Fluoroquinolones | 6352 (0.9%) | 466 (7.3%) | 0.99 (0.90 to 1.09) | 1550 (2.2%) | 126 (8.1%) | 1.15 (0.97 to 1.37) |
| Other | 24,715 (3.6%) | 1864 (7.5%) | 1.03 (0.98 to 1.09) | 13,885 (1.8%) | 960 (6.9%) | 0.98 (0.92 to 1.05) |
| Homogeneity test (p-value) | 0.2032 | 0.0971 | ||||
| Low 5 min Apgar score | ||||||
| Cephalosporins | 7816 (1.1%) | 50 (0.6%) | 1.33 (1.00 to 1.76) | 4675 (0.6%) | 16 (3.7%) | 0.84 (0.51 to 1.38) |
| Penicillins | 84,211 (12.1%) | 417 (0.5%) | 1.07 (0.96 to 1.18) | 52,923 (6.8%) | 234 (0.4%) | 1.10 (0.96 to 1.26) |
| Macrolides | 24,763 (3.6%) | 123 (0.5%) | 1.05 (0.88 to 1.26) | 9316 (1.2%) | 50 (0.5% | 1.35 (1.02 to 1.79) |
| Fluoroquinolones | 6352 (0.9%) | 36 (0.6%) | 1.16 (0.83 to 1.61) | 1550 (2.2%) | 3 (0.2%) | 0.45 (0.14 to 1.40) |
| Other | 24,715 (3.6%) | 151 (0.6%) | 1.32 (1.12 to 1.56) | 13,885 (1.8%) | 70 (0.5%) | 1.24 (0.97 to 1.57) |
| Homogeneity test (p-value) | 0.1782 | 0.1961 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantarutti, A.; Rea, F.; Franchi, M.; Beccalli, B.; Locatelli, A.; Corrao, G. Use of Antibiotic Treatment in Pregnancy and the Risk of Several Neonatal Outcomes: A Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 12621. https://doi.org/10.3390/ijerph182312621
Cantarutti A, Rea F, Franchi M, Beccalli B, Locatelli A, Corrao G. Use of Antibiotic Treatment in Pregnancy and the Risk of Several Neonatal Outcomes: A Population-Based Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12621. https://doi.org/10.3390/ijerph182312621
Chicago/Turabian StyleCantarutti, Anna, Federico Rea, Matteo Franchi, Benedetta Beccalli, Anna Locatelli, and Giovanni Corrao. 2021. "Use of Antibiotic Treatment in Pregnancy and the Risk of Several Neonatal Outcomes: A Population-Based Study" International Journal of Environmental Research and Public Health 18, no. 23: 12621. https://doi.org/10.3390/ijerph182312621
APA StyleCantarutti, A., Rea, F., Franchi, M., Beccalli, B., Locatelli, A., & Corrao, G. (2021). Use of Antibiotic Treatment in Pregnancy and the Risk of Several Neonatal Outcomes: A Population-Based Study. International Journal of Environmental Research and Public Health, 18(23), 12621. https://doi.org/10.3390/ijerph182312621