
Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Screening Process
2.4. Eligibility Criteria
- Clinical studies or case series;
- Minimum sample size of ≥3 patients;
- Articles written in English or German language.
- Case reports <3 patients, systematic reviews, in vitro studies;
- Missing details on the performed treatment (e.g., extrusion force, amount of movement);
- Duplicate article describing the same sample;
- Forced eruption for extraction/implant site development.
2.5. Resources Selection
2.6. Data Extraction
2.7. Quality Assessment
2.8. Statistical Analysis
- Does increased force during orthodontic extrusion lead to faster eruption without causing changes in soft and hard tissue as compared to light force?
- Does OFE influence root resorption on the tooth to be extruded?
- Do younger patients (under 50 years) benefit from OFE more than elderly patients (≥50 years) concerning pulp vitality and root resorption?
- Does the use of fixed orthodontic appliances accelerate the extrusion rate of OFE compared to OFE with posts and elastics?
- Does fiberotomy reduce the need for subsequent periodontal surgery after OFE?
3. Results
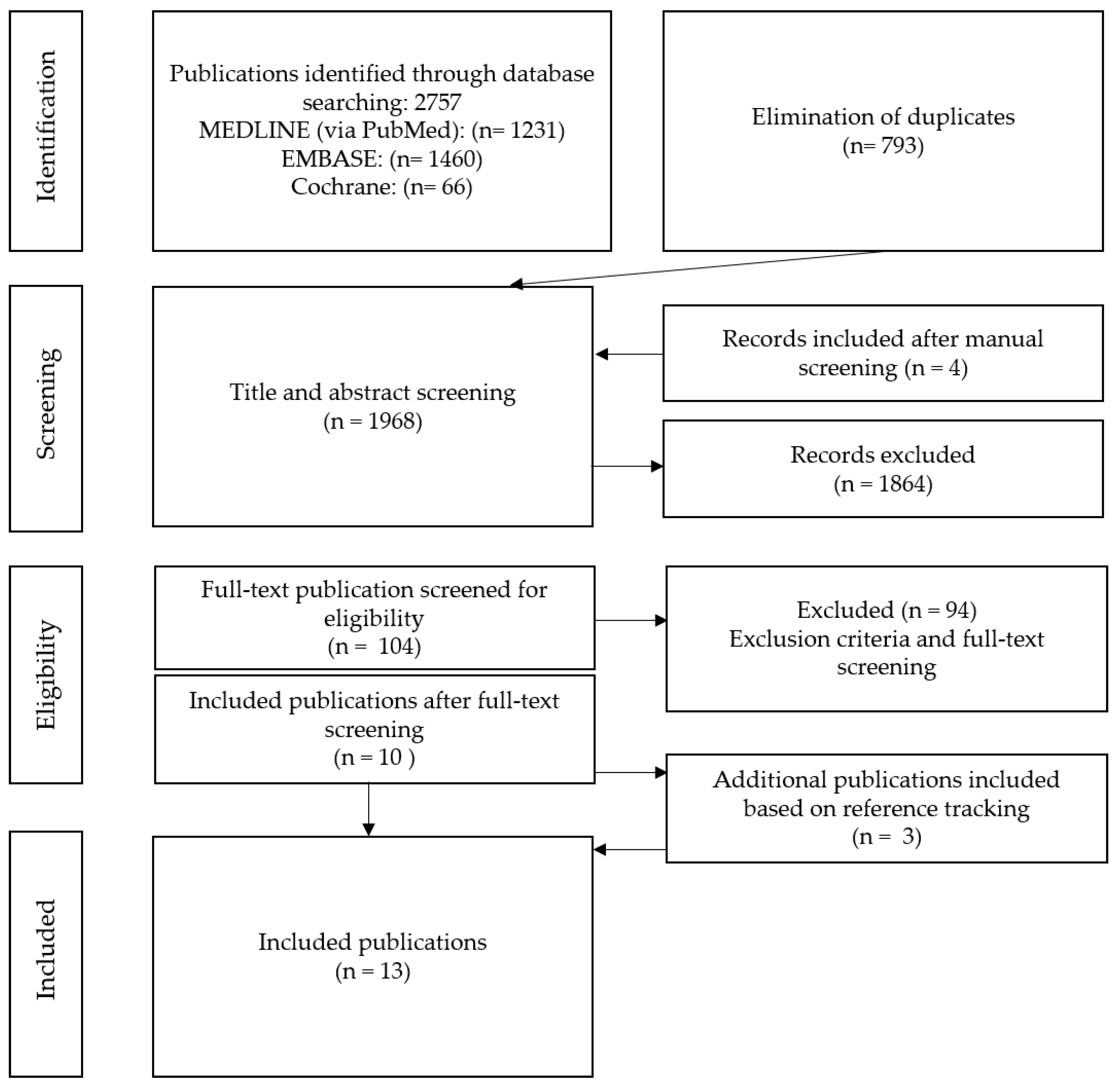
3.1. Screening Process
3.2. Studies Election
3.2.1. Included Studies
- OFE without migration of the gingiva and alveolar bone: OFE without tissue movement requires the use of strong extrusive force (>0.6 N), which was presented in the case series (32 patients) by Malmgren [29]. Another option to prevent gingival and alveolar bone migration is the use of fiberotomy. Both the prospective clinical trial and the RCT showed that coronal movement of the gingival margin can be prevented by sectioning of supracrestal gingival fibers at the beginning and during orthodontic extrusion treatment and simultaneous root planing from the top of the alveolar bone crest [15,16].
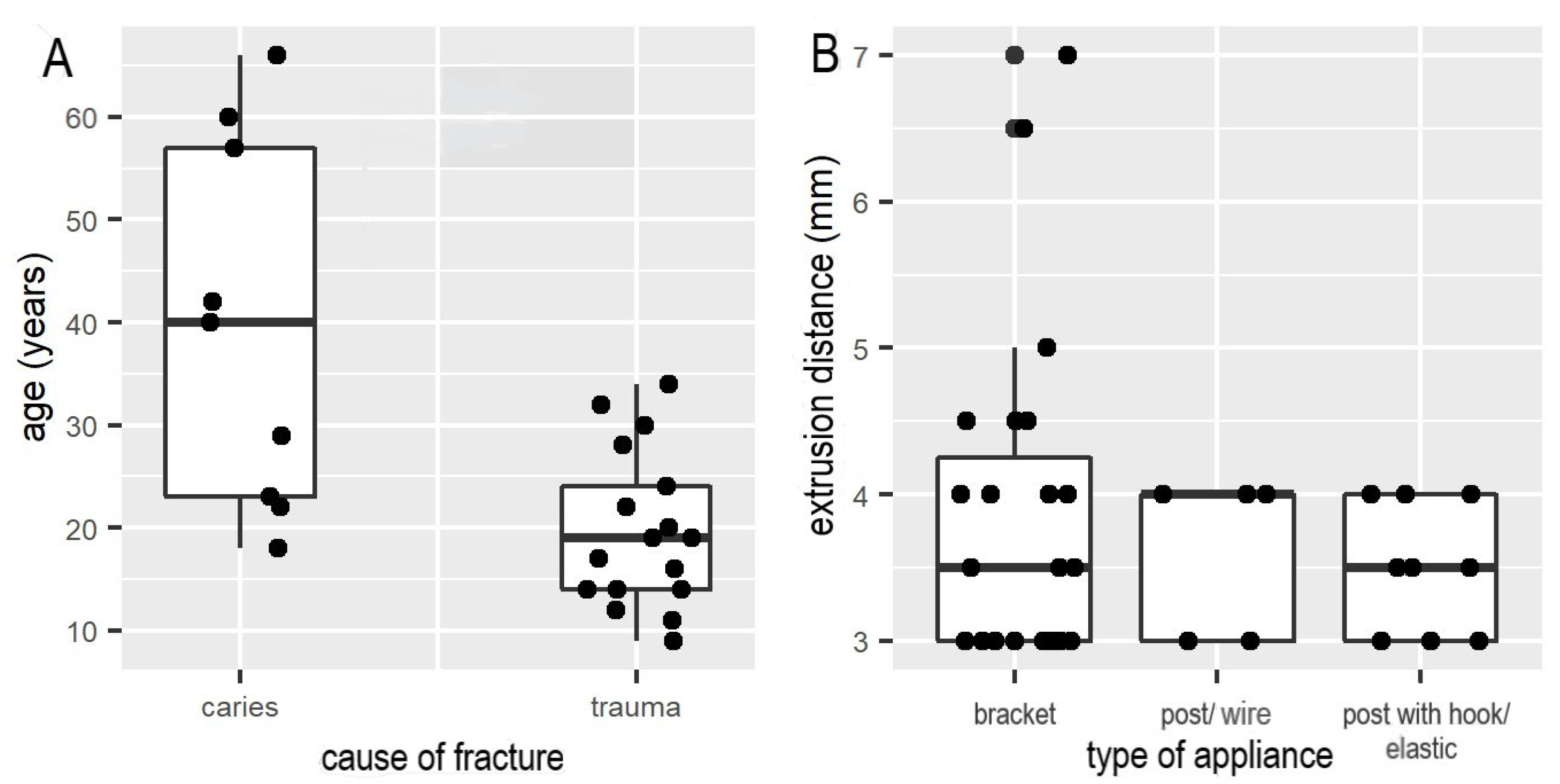
- OFE with gingival migration and slight alveolar bone migration: In the nine case series, this clinical purpose was accomplished by applying weak (0.2–0.3 N) to moderate (>0.3 N and <0.6 N) orthodontic force using round nickel–titanium wires; the mean extrusion distance was 1.5 mm per week. Furthermore, there was no substantial difference in extrusion distance (mm) per week achieved with straight wire appliances, or post with elastics or wires within case series (Figure 2B). However, a trend towards less extrusion distance with the use of elastics was observed (Figure 2B). Analysis of the nine case series showed significant correlations due to shorter extrusion times (up to six weeks) in younger patients (11 to 24 years) versus longer extrusion times per week in adults (up to ten weeks) (p < 0.05). Furthermore, there was a significant correlation between caries as a fracture reason and the range of patient’s age from 23 up to 57 years (Figure 2A, p < 0.03).
- OFE with migration of the gingiva and alveolar bone: The third technique, also known as orthodontic implant site development (OISD), is characterized by slow extrusion of the fractured tooth with weak (0.2–0.3 N) to moderate (>0.3 N and <0.6 N) force to induce coronal migration of gingival margin and alveolar bone [13,30]. Simon et al. reported two cases treated with this technique [31].
3.2.2. Methodological Quality
4. Discussion
4.1. OFE without Migration of the Gingival Margin and Alveolar Bone
4.2. OFE with Gingival Migration and Slight Alveolar Bone Migration
4.3. OFE with Migration of the Gingival Margin and Alveolar Bone
4.4. Extrusion and Anchorage Techniques
4.5. Pulp Vitality and Root Resorption
4.6. Stabilization after OFE
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Soliman, S.; Lang, L.M.; Hahn, B.; Reich, S.; Schlagenhauf, U.; Krastl, G.; Krug, R. Long-term outcome of adhesive fragment reattachment in crown-root fractured teeth. Dent. Traumatol. 2020, 36, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Krastl, G.; Filippi, A.; Zitzmann, N.U.; Walter, C.; Weiger, R. Current aspects of restoring traumatically fractured teeth. Eur. J. Esthet. Dent. 2011, 6, 124–141. [Google Scholar]
- Casaponsa, J.; Abella, F. Magnetic extrusion for restoring teeth with a negative ferrule effect: A 2-year follow-up case report. Int. J. Esthet. Dent. 2021, 16, 186–201. [Google Scholar] [PubMed]
- Nobre, C.M.; de Barros Pascoal, A.L.; Albuquerque Souza, E.; Machion Shaddox, L.; Dos Santos Calderon, P.; de Aquino Martins, A.R.; de Vasconcelos Gurgel, B.C. A systematic review and meta-analysis on the effects of crown lengthening on adjacent and non-adjacent sites. Clin. Oral. Investig. 2017, 21, 7–16. [Google Scholar] [CrossRef]
- Camargo, P.M.; Melnick, P.R.; Camargo, L.M. Clinical crown lengthening in the esthetic zone. J. Calif. Dent. Assoc. 2007, 35, 487–498. [Google Scholar]
- Pilalas, I.; Tsalikis, L.; Tatakis, D.N. Pre-restorative crown lengthening surgery outcomes: A systematic review. J. Clin. Periodontol. 2016, 43, 1094–1108. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.A. Forced eruption in the esthetic zone. Compend. Contin. Educ. Dent. 1997, 18, 795–803. [Google Scholar]
- Plotino, G.; Abella Sans, F.; Duggal, M.S.; Grande, N.M.; Krastl, G.; Nagendrababu, V.; Gambarini, G. Clinical procedures and outcome of surgical extrusion, intentional replantation and tooth autotransplantation—A narrative review. Int. Endod. J. 2020, 53, 1636–1652. [Google Scholar] [CrossRef]
- Elkhadem, A.; Mickan, S.; Richards, D. Adverse events of surgical extrusion in treatment for crown-root and cervical root fractures: A systematic review of case series/reports. Dent. Traumatol. 2014, 30, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Krug, R.; Connert, T.; Soliman, S.; Syfrig, B.; Dietrich, T.; Krastl, G. Surgical extrusion with an atraumatic extraction system: A clinical study. J. Prosthet. Dent. 2018, 120, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Heithersay, G.S. Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral. Surg. Oral. Med. Oral. Pathol. 1973, 36, 404–415. [Google Scholar] [CrossRef]
- Ingber, J.S. Forced eruption: Part II. A method of treating nonrestorable teeth-Periodontal and restorative considerations. J. Periodontol. 1976, 47, 203–216. [Google Scholar] [CrossRef] [PubMed]
- Salama, H.; Salama, M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: A systematic approach to the management of extraction site defects. Int. J. Periodontics Restor. Dent. 1993, 13, 312–333. [Google Scholar]
- Ingber, J.S. Forced eruption. I. A method of treating isolated one and two wall infrabony osseous defects-rationale and case report. J. Periodontol. 1974, 45, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Faramarzi, M.; Rikhtegaran, S.; Biroon, S.H. Effectiveness of Nd:YAG Laser Fiberotomy in Clinical Crown Lengthening by Forced Eruption. Int. J. Periodontics Restor. Dent. 2017, 37, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, C.V.; Bauer, F.P.; Romito, G.A.; Pannuti, C.M.; De Micheli, G. Orthodontic extrusion with or without circumferential supracrestal fiberotomy and root planing. Int. J. Periodontics Restor. Dent. 2006, 26, 87–93. [Google Scholar]
- Mehl, C.; Wolfart, S.; Kern, M. Orthodontic extrusion with magnets: A case report. Quintessence Int. 2008, 39, 371–379. [Google Scholar]
- Canjau, S.; Stefan, C.; Szuhanek, C.A. Alternative treatment approach for anterior subgingival dental lesions: Forced eruption using attractive magnets. Am. J. Orthod. Dentofac. Orthop. 2020, 158, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Faria, L.P.; Almeida, M.M.; Amaral, M.F.; Pellizzer, E.P.; Okamoto, R.; Mendonca, M.R. Orthodontic Extrusion as Treatment Option for Crown-Root Fracture: Literature Review with Systematic Criteria. J. Contemp. Dent. Prac. 2015, 16, 758–762. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 18, 343:d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P. Assessing Risk of Bias in a Non-Randomized Study. Cochrane Handbook for Systematic Reviews of Interventions. Chapter 25. Available online: www.training.cochrane.org/handbook (accessed on 1 November 2021).
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 November 2021).
- Pierson, D.J. How to Read a Case Report (or Teaching Case of the Month). Respir. Care 2009, 54, 1372–1378. [Google Scholar]
- Hill, A.B. The environment and disease: Association or causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oesterle, L.J.; Wood, L.W. Raising the root. A look at orthodontic extrusion. J. Am. Dent. Assoc. 1991, 122, 193–198. [Google Scholar] [CrossRef]
- Bauss, O.; Schafer, W.; Sadat-Khonsari, R.; Knosel, M. Influence of orthodontic extrusion on pulpal vitality of traumatized maxillary incisors. J. Endod. 2010, 36, 203–207. [Google Scholar] [CrossRef]
- Malmgren, O.; Malmgren, B.; Frykholm, A. Rapid orthodontic extrusion of crown root and cervical root fractured teeth. Endod. Dent. Traumatol. 1991, 7, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulou, A.K.; Papageorgiou, S.N.; Hatzopoulos, S.A.; Tsirlis, A.; Athanasiou, A.E. Alveolar ridge alterations in the maxillary anterior region after tooth extraction through orthodontic forced eruption for implant site development: A clinical CBCT study. Eur. J. Orthod. 2020, 42, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.H. Root extrusion. Rationale and techniques. Dent. Clin. 1984, 28, 909–921. [Google Scholar]
- Pontoriero, R.; Celenza, F., Jr.; Ricci, G.; Carnevale, G. Rapid extrusion with fiber resection: A combined orthodontic-periodontic treatment modality. Int. J. Periodontics Restor. Dent. 1987, 7, 30–43. [Google Scholar]
- González-Martín, O.; Solano-Hernandez, B.; González-Martín, A.; Avila-Ortiz, G. Orthodontic Extrusion: Guidelines for Contemporary Clinical Practice. Int. J. Periodontics Restor. Dent. 2020, 40, 667–676. [Google Scholar] [CrossRef]
- Zenobio, E.G.; Moreira, R.C.; Soares, R.V.; Feres, M.; Chambrone, L.; Shibli, J.A. A mixed-model study assessing orthodontic tooth extrusion for the reestablishment of biologic width. A systematic review and exploratory randomized trial. Int. J. Periodontics Restor. Dent. 2015, 35, 19–27. [Google Scholar] [CrossRef] [Green Version]
- Ivey, D.W.; Calhoun, R.L.; Kemp, W.B.; Dorfman, H.S.; Wheless, J.E. Orthodontic extrusion: Its use in restorative dentistry. J. Prosthet. Dent. 1980, 43, 401–407. [Google Scholar] [CrossRef]
- Bielak, S.; Bimstein, E.; Eidelman, E. Forced eruption: The treatment of choice of subgingivally fractured permanent incisors. ASDC J. Dent. Child. 1982, 49, 186–190. [Google Scholar]
- Razali, M.F.; Mahmud, A.S.; Mokhtar, N. Force delivery of NiTi orthodontic arch wire at different magnitude of deflections and temperatures: A finite element study. J. Mech. Behav. Biomed. Mater. 2018, 77, 234–241. [Google Scholar] [CrossRef]
- Oesterle, L.J.; Owens, J.M.; Newman, S.M.; Shellhart, W.C. Perceived vs. measured forces of interarch elastics. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 298–306. [Google Scholar] [CrossRef]
- Wang, T.; Zhou, G.; Tan, X.; Dong, Y. Evaluation of force degradation characteristics of orthodontic latex elastics in vitro and in vivo. Angle Orthod. 2007, 77, 688–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gioka, C.; Zinelis, S.; Eliades, T.; Eliades, G. Orthodontic latex elastics: A force relaxation study. Angle Orthod. 2006, 76, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Li, M.; Lu, J.; Hu, Y.; Cui, L.; Zhang, D.; Yang, Y. Age-related effects on osteoclastic activities after orthodontic tooth movement. Bone Jt. Res. 2016, 5, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danesh-Meyer, M.J.; Brice, D.M. Implant site development using orthodontic extrusion: A case report. N. Z. Dent. J. 2000, 96, 18–22. [Google Scholar] [PubMed]
- Mantzikos, T.; Shamus, I. Forced eruption and implant site development: Soft tissue response. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 596–606. [Google Scholar] [CrossRef]
- Amato, F.; Mirabella, A.D.; Macca, U.; Tarnow, D.P. Implant site development by orthodontic forced extraction: A preliminary study. Int. J. Oral. Maxillofac. Implant. 2012, 27, 411–420. [Google Scholar]
- Al-Gheshiyan, N.A. Forced eruption: Restoring nonrestorable teeth and preventing extraction site defects. Gen. Dent. 2004, 327–333. [Google Scholar]
- Bondemark, L.; Kurol, J.; Hallonsten, A.L.; Andreasen, J.O. Attractive magnets for orthodontic extrusion of crown-root fractured teeth. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 187–193. [Google Scholar] [CrossRef]
- Mostafa, Y.; Iskander, K.G.; el-Mangoury, N.H. Iatrogenic pulpal reactions to orthodontic extrusion. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 30–34. [Google Scholar] [CrossRef]
- Krastl, G.; Weiger, R.; Filippi, A.; Van Waes, H.; Ebeleseder, K.; Ree, M.; Connert, T.; Widbiller, M.; Tjaderhane, L.; Dummer, P.; et al. European society of endodontology position statement: Endodontic management of traumatized permanent teeth. Int. Endod. J. 2021, 54, 1473–1481. [Google Scholar] [CrossRef]
- Bourguignon, C.; Cohenca, N.; Lauridsen, E.; Flores, M.T.; O’Connell, A.C.; Day, P.F.; Tsilingaridis, G.; Abbott, P.V.; Fouad, A.F.; Hicks, L.; et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent. Traumatol. 2020, 36, 314–330. [Google Scholar] [CrossRef] [PubMed]
- Dammaschke, T.; Galler, K.M.; Krastl, G. Current recommendations for vital pulp treatment. Dtsch Zahnaärztl Z. Int. 2019, 1, 43–52. [Google Scholar] [CrossRef]
- Biggerstaff, R.H.; Sinks, J.H.; Carazola, J.L. Orthodontic extrusion and biologic width realignment procedures: Methods for reclaiming nonrestorable teeth. J. Am. Dent. Assoc. 1986, 112, 345–348. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Criteria | Specification |
|---|---|
| Research question (focus) | “Is orthodontic forced eruption a successful and effective pre-restorative therapy of non-restorable permanent teeth with subgingival dental hard tissue defects after trauma?” |
| Population | Patients with non-restorable permanent teeth with subgingival defects due to trauma or caries |
| Intervention | Orthodontic forced eruption techniques (including anchorage and stabilization) of the affected tooth |
| Comparator | Other treatment options |
| Outcomes | Pulp vitality, root resorption, soft and hard tissue changes, amount of tooth movement of the affected tooth |
| Database | Search Terms |
|---|---|
| PubMed | ((((((crown tooth[MeSH Terms]) OR tooth root[MeSH Terms]) OR fracture*) OR crown*) OR root*)) AND ((tooth extrusion[MeSH Terms]) OR tooth eruption[MeSH Terms] OR orthodontic forced eruption[MeSH Terms] OR orthodontic extrusion[MeSH Terms]) |
| Cochrane Library | crown tooth OR root tooth OR fracture/fractures OR crown/crowns OR root/roots AND tooth extrusion OR tooth eruption OR orthodontic forced eruption OR orthodontic extrusion |
| Embase | crown tooth OR root tooth OR fracture/fractures OR crown/crowns OR root/roots AND orthodontic extrusion OR tooth eruption OR orthodontic forced eruption |
| Assessing Risk of Reporting Biases for Case Series by Murad et al. (2018) | Bielak et al. (1982) | Biggerstaff et al. (1986) | Heithersay et al. (1973) | Ingber et al. (1976) | Ivey et al. (1980) | Levine et al. (1997) | Malmgren et al. (1991) | Pontoriero et al. (1987) | Simon et al. (1984) |
|---|---|---|---|---|---|---|---|---|---|
| Selection bias—selection method | − | − | − | − | − | − | − | − | − |
| Ascertainment—exposure | + | + | + | + | + | + | + | − | − |
| Ascertainment—outcome | + | + | + | + | + | + | + | + | + |
| Causality—alternatives | − | − | − | − | − | − | − | − | − |
| Causality—challenge | + | + | + | + | + | + | + | + | + |
| Causality—effect | + | + | + | + | + | + | + | + | + |
| Causality—follow-up | − | − | − | − | − | + | + | − | − |
| Reporting bias—details | + | + | + | + | + | + | + | + | + |
| Level of evidence | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| Overall risk of bias | 5 | 5 | 5 | 5 | 5 | 6 | 6 | 4 | 4 |
| Study | Study Design | Number of Treated Teeth and Defect Type | Orthodontic Appliance | Extrusion Force | Amount of Tooth Movement (mm/Week) | Fiberotomy | Periodontal Surgery | Soft and Hard Tissue Changes after OFE |
|---|---|---|---|---|---|---|---|---|
| Bauss et al. (2010) | Retrospective cohort study | Group 1: 32 (trauma) Orthodontic therapy + OFE after trauma Group 2: Orthodontic therapy without trauma Group 3: 68 (trauma) Trauma without orthodontic therapy/OFE | Sectional: Utility arch | Weak (0.2–0.3 N) | Not reported | No | No | Not reported |
| Bielak et al. (1982) | Case series | 3 (trauma) | Sectional: bracket position more apical | Moderate (<0.6 N) | 1.9 | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Biggerstaff et al. (1986) | Case series | 3 (trauma, caries) | Sectional: bracket position more apical | Moderate (<0.6 N) | 1.6 | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Carvalho et al. (2006) | RCT | 20 (trauma) fractured maxillary incisors Group A: OFE + fiberotomy and root planing Group B: OFE | Sectional: bracket position more apical | Moderate (<0.5 N) | Not reported | Group A: yes (weekly until retention time) Group B: no | FTF after OFE in group B | Marginal gingiva: unaltered in group A Marginal gingiva and alveolar bone more coronal in group B |
| Faramarzi et al. (2017) | Prospective clinical trial, 1 case report | 20 (caries, trauma) | Sectional: post included a hook and elastics; fixed sectional horizontal wire | Moderate (<0.6 N) | Not reported | Nd:YAG laser fiberotomy: 48 h after start of OFE; performed every 2 weeks | No | No migration of gingiva or alveolar bone |
| Heithersay et al. (1973) | Case series | 3 (trauma) | Sectional: temporary post and flexible spring; twistflex wire | Moderate (<0.6 N) | 1.5 | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Ingber et al. (1976) | Case series | 4 (trauma) | Sectional: bracket position more apical | Moderate (<0.6 N) | 1.7 | No | FTF and slight osteotomy after OFE | Marginal gingiva and alveolar bone more coronal |
| Ivey et al. (1980) | Case series | 4 (trauma, caries) | Sectional: bracket position more apical | Moderate (<0.6 N) | 1.3 | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Levine et al. (1997) | Case series | 4 (trauma, caries) | Sectional: bracket position more apical (3 cases); post and elastic (1 case) | Moderate (<0.6 N) | 1.8 | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Malmgren et al. (1991) | Case series | 32 (trauma) | Sectional: 0.16 × 0.16 inch Elgiloy | Strong (>0.6 N) | 1.3 | No | Gingivectomy after OFE | No migration of gingiva or alveolar bone |
| Oesterle et al. (1991) | Retrospective clinical trial | >100 (trauma, caries) | (a) temporary crown with a self-threading pin (b) hook bent from 0.020-inch stainless steel wire (c) elastic chain or tie | Weak (0.2–0.3 N) | Not reported | No | FTF after OFE | Marginal gingiva and alveolar bone more coronal |
| Pontoriero et al. (1987) | Case series | 3 (caries) | Sectional: post with hook and elastic; fixed wire | Moderate (<0.6 N) | 1.3 | Case 1: no Case 2: mesially, distally without fiberotomy (control) Case 3: circular; weekly during extrusion | Case 1: FTF and osteotomy Case 2: FTF and osteotomy distally of 14 Case 3: Gingivectomy | 1. Case: Marginal gingiva and alveolar bone more coronal 2. Case: More coronal (raised and beveled) distally instead of mesially Case 3: No migration of gingiva or alveolar bone |
| Simon et al. (1984) | Case series | 3 (trauma, caries) | Sectional: post with hook and elastic, fixed sectional horizontal wire | Moderate (<0.6 N) | Not reported | No | No | Migration of marginal gingiva, alveolar bone more coronal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reichardt, E.; Krug, R.; Bornstein, M.M.; Tomasch, J.; Verna, C.; Krastl, G. Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12580. https://doi.org/10.3390/ijerph182312580
Reichardt E, Krug R, Bornstein MM, Tomasch J, Verna C, Krastl G. Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12580. https://doi.org/10.3390/ijerph182312580
Chicago/Turabian StyleReichardt, Elisabeth, Ralf Krug, Michael M. Bornstein, Jürgen Tomasch, Carlalberta Verna, and Gabriel Krastl. 2021. "Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 23: 12580. https://doi.org/10.3390/ijerph182312580
APA StyleReichardt, E., Krug, R., Bornstein, M. M., Tomasch, J., Verna, C., & Krastl, G. (2021). Orthodontic Forced Eruption of Permanent Anterior Teeth with Subgingival Fractures: A Systematic Review. International Journal of Environmental Research and Public Health, 18(23), 12580. https://doi.org/10.3390/ijerph182312580