
Attitudinal Barriers Hindering Adoption of Telepsychiatry among Mental Healthcare Professionals: Israel as a Case-Study



Abstract
:1. Introduction
Background
2. Materials and Methods
2.1. The Israeli Context
2.2. Study Design
2.3. Recruitment of Participants
2.4. Data Collection and Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Interview Findings
3.2.1. Quality of Treatment Using Telepsychiatry
In a preliminary meeting with a patient, there is paramount importance to direct interpersonal interaction and body language. There are lots of senses, sensors, and skills that need to be employed in order to formulate a preliminary assessment of the patient—and the online medium is very restrictive in that sense. [Interviewee 13]
With some of my patients, the most significant improvement in their situation stems from the fact that they need to get up in the morning, leave their home, take the bus, and interact with other people on their way to the clinic. From my perspective, there is a significant therapeutic value in leaving one’s home… I fear we will lose that significant something when interacting through a screen [telepsychiatry]. [Interviewee 26]
There are no limitations on conducting a proper psychiatric examination in telepsychiatry. I do not conduct a slopier or less thorough examination online. My personal feeling is that there is no impairment on my ability to diagnose a patient via telepsychiatry. [Interviewee 04]
3.2.2. Efficiency and Economic Benefits
The most significant advantage in telepsychiatry is in reducing the costs for patients—in travel costs, commute time, and loss of wages. [Interviewee 08]
In reality, telepsychiatry is more expensive for HMOs because you need to occupy two rooms at the same time—one for the doctor and another for the patient. This means double rental and maintenance costs. [Interviewee 02]
The HMO is paying less for an online therapist, compared to what they pay a regular therapist, or even in comparison to an independent/freelance one. [Interviewee 17]
From our experience, the percentage of no-shows in telepsychiatry is very similar to traditional treatment. People treat it as no different from a regular appointment. The usage of virtual waiting rooms might reduce this rate somewhat. But, it’s something we have yet to try. [Interviewee 23]
In my opinion, even if it works wonderfully and without malfunctions, telepsychiatry will only serve to extend wait times because of a well-known rule in health economy: the more efficient and accessible a service is, the higher its demand and usage. [Interviewee 22]
In my opinion, a session of less than 30 min is not a “real” and meaningful session… it’s not even long enough in order to maintain rapport and build a working alliance. [Interviewee 16]
3.2.3. Effects on Therapists
My wife will not be happy if I’ll be closed-off in the study from 19:00 to 22:00, videoconferencing with patients, instead of spending time with my children. It will be very damaging to the work–life balance, which we strive so hard to preserve. [Interviewee 16]
It’s very difficult to overcome the technical issues involved [with telepsychiatry]. The conversation is interrupted regularly, and it takes a few minutes to resume connection. A significant portion of session-time is wasted on connectivity issues. Even afterwards, the sound quality is poor, and it is hard to hear the patient. [Interviewee 22]
Convenience [of telepsychiatry] is all well and good, as long as it’s available to the patients... However, the moment there is a problem, and this level of convenience and service they’ve gotten used to is no longer available, from a verity of reasons, this raises the level of frustration and anger, which may lead to aggressiveness and even violence. [Interviewee 13]
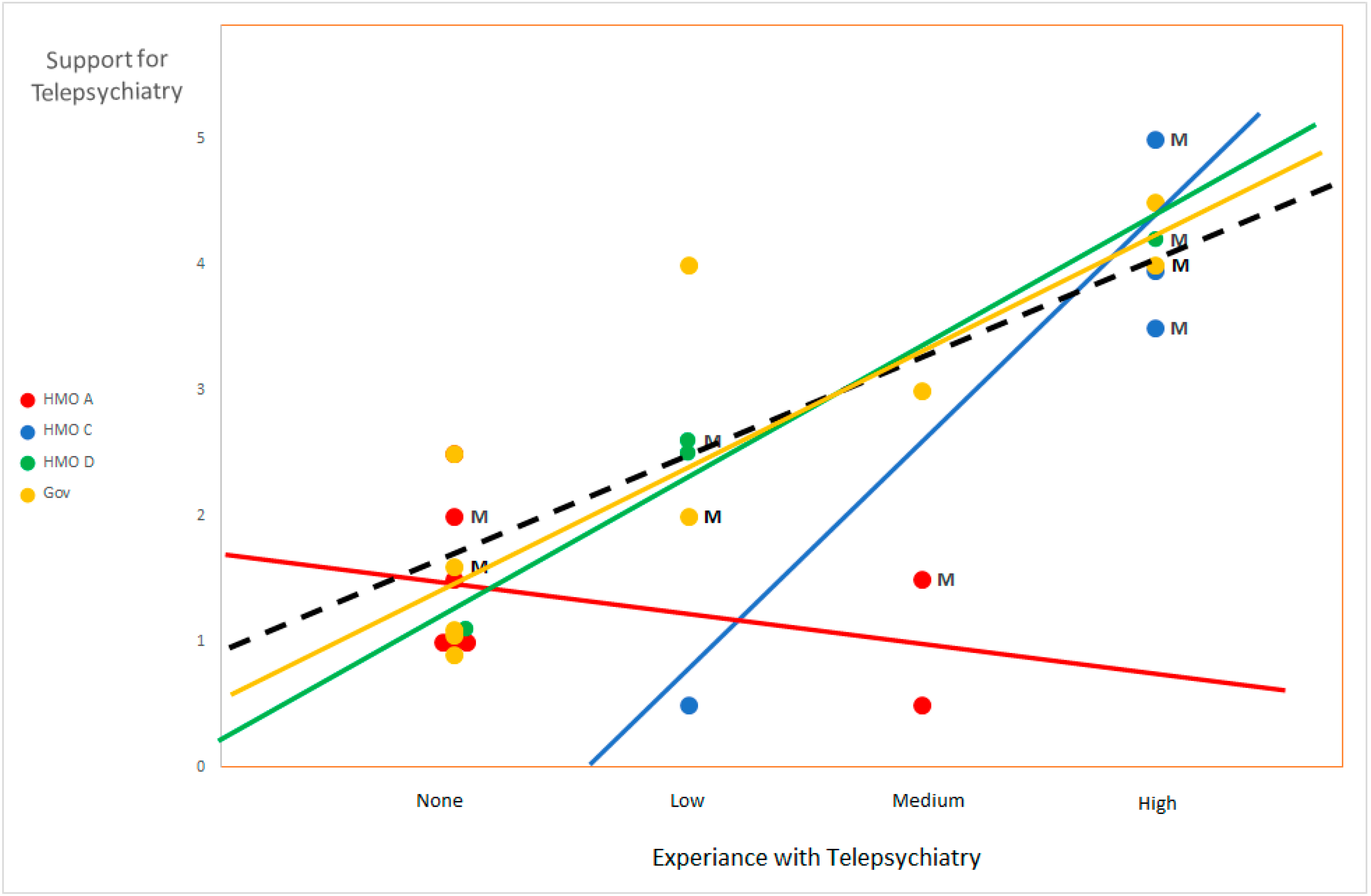
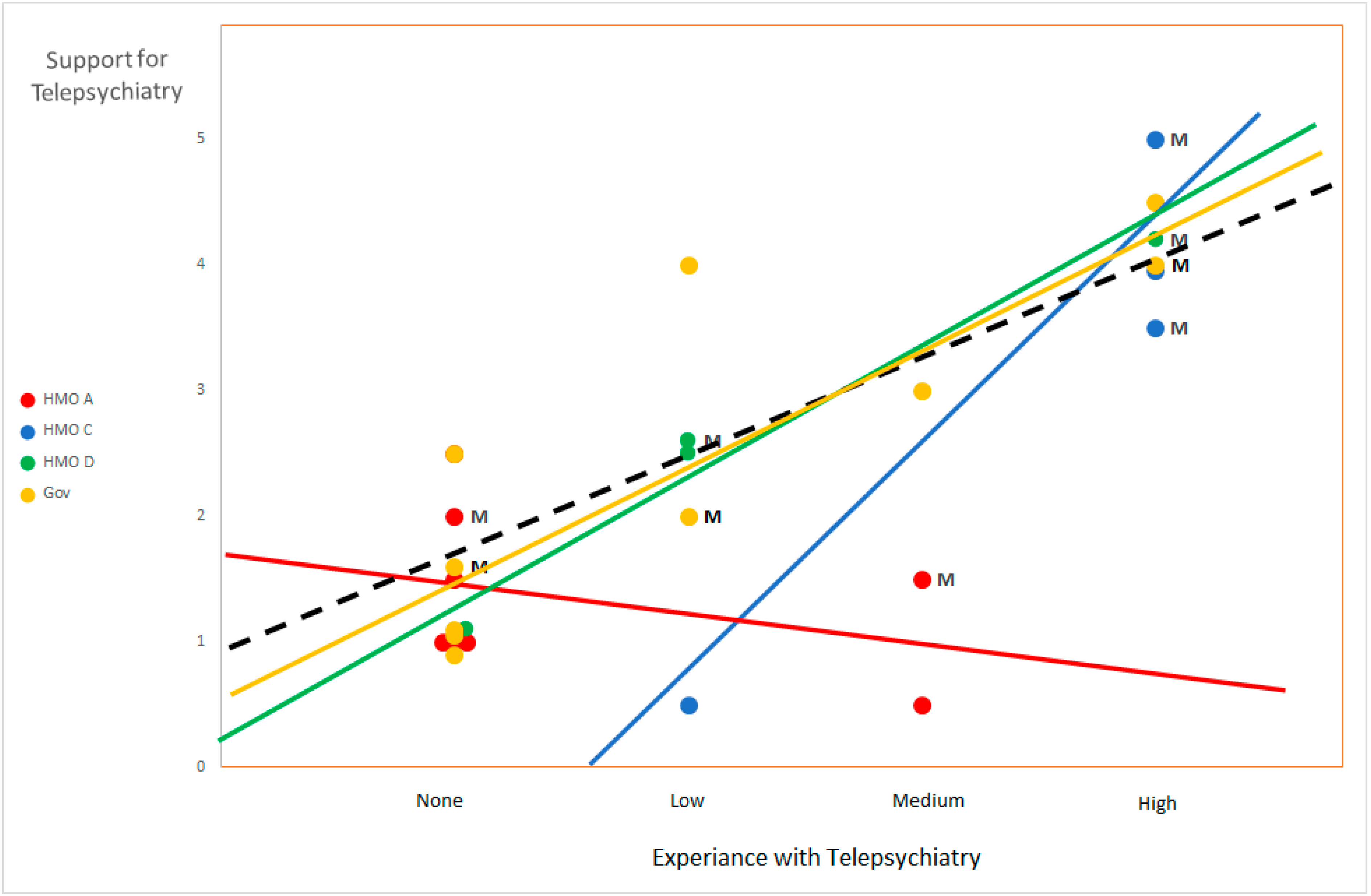
3.3. Relationship between Organizational Affiliation, Experiential Knowledge and Support for Telepsychiatry Services
4. Discussion
4.1. Principle Findings
4.2. Comparison with Prior Works
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- What are the main challenges/bottlenecks facing the Israeli public healthcare system today?
- What are the main obstacles/barriers to the provision of optimal care?
- What are your opinions about the current situation of psychiatric services? In regard to...
- Waiting-times;
- Workload in local clinics;
- Cultural and language barriers;
- Access to services in remote areas;
- “Special needs” populations;
- Availability of capable and trained staff.
- In your opinion, will new mediums of telecommunication—such as social media, the internet, or smartphones—be able to bridge some of these challenges/obstacles?
- Have you heard/read/or had any prior knowledge regarding telepsychiatry?
- Have you read any professional articles on this method?
- Have you undergone any professional training regarding videoconference-assisted treatment?
- Personal prior experience:
- Do you have any experience in treatment via videoconference?
- Do you have any experience in treatment over the telephone, chat, text, etc.?
- How many patients have you treated through telepsychiatry?
- For how long?
- Was it through public healthcare or private practice?
- How many patients over the past year/2019?
- How many sessions, on average?
- In your opinion. What are the possible advantages or disadvantages of telepsychiatry compared to face-to-face treatment?
- Will it lead to reduced expenses? Reduced costs?
- Shorten waiting times? Lessen workload?
- What will the clinical results be like? Is it clinically inferior?
- Will it reduce cultural barriers and misunderstandings?
- In your opinion, is telepsychiatry suitable for all stages of treatment:
- Interview/intake/diagnosis;
- Regular treatment sessions;
- Follow-up meetings;
- Emotional-psychological treatment;
- Medicine management.
- Would you feal comfortable—clinically and ethically—recommending involuntary commitment after conducting only an online examination of a patient?
- Which types of patients and diagnoses are suitable/unsuitable for tele-psychiatric treatment?
- Are there diagnoses/populations/situations where you would oppose any form of telepsychiatry? Advise against tele-psychiatric treatment?
- In your opinion, is telepsychiatry clinically equivalent/effective/inferior to traditional face-to-face psychiatry? How so?
- Is there a need for specific training/expertise in order to practice telepsychiatry?
- Do you perceive any ethical/moral/or legal problems associated with practicing telepsychiatry in the Israeli context?
- Will this new method of treatment have any effects on work practices, routines, and lifestyle of mental healthcare professionals, or patients?
- Are you yourself interested in practicing telepsychiatry in the public healthcare system?
- Are you encouraging others to partake in and practice telepsychiatry?
References
- Backhaus, A.; Agha, Z.; Maglione, M.L.; Repp, A.; Ross, B.; Zuest, D.; Rice-Thorp, N.M.; Lohr, J.; Thorp, S.R. Videoconferencing psychotherapy: A systematic review. Psychol. Serv. 2012, 9, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Berryhill, M.B.; Culmer, N.; Williams, N.; Halli-Tierney, A.; Betancourt, A.; Roberts, H.; King, M. Videoconferencing psychotherapy and depression: A systematic review. Telemed. e-Health 2019, 25, 435–446. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Parish, M.B.; Yellowlees, P.M. Telepsychiatry today. Curr. Psychiatry Rep. 2015, 17, 1–9. [Google Scholar] [CrossRef]
- Hilty, D.H.; Yellowlees, P.M.; Parish, M.B.; Chan, S. Telepsychiatry: Effective, evidence-based, and at a tipping point in health care delivery? Psychiatr. Clin. N. Am. 2015, 38, 559–592. [Google Scholar] [CrossRef]
- O’Brien, M.; McNicholas, F. The use of telepsychiatry during COVID-19 and beyond. Ir. J. Psychol. Med. 2020, 37, 250–255. [Google Scholar] [CrossRef]
- Shore, J.H.; Schneck, C.D.; Mishkind, M.C. Telepsychiatry and the Coronavirus Disease 2019 Pandemic—Current and Future Outcomes of the Rapid Virtualization of Psychiatric Care. JAMA Psychiatry 2020, 77, 1211–1212. [Google Scholar] [CrossRef]
- Kannarkat, J.T.; Smith, N.N.; McLeod-Bryant, S.A. Mobilization of Telepsychiatry in Response to COVID-19—Moving Toward 21st Century Access to Care. Adm. Policy Ment. Health Ment. Health Serv. Res. 2020, 47, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Hubley, S.; Lynch, S.B.; Schneck, C.; Thomas, M.; Shore, J.H. Review of key telepsychiatry outcomes. World J. Psychiatry 2016, 6, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Mayworm, A.M.; Lever, N.; Gloff, N.; Cox, J.; Willis, K.; Hoover, S.A. School-based telepsychiatry in an urban setting: Efficiency and satisfaction with care. Telemed. e-Health 2020, 26, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.A.; Maclaren, A.T.; Morton, M.; Carachi, R. Professional opinions of the use of telemedicine in child and adolescent psychiatry. Scott. Med J. 2009, 54, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G.; Leenknecht, C.; Zauher, J. Psychiatrists’ satisfaction with telepsychiatry. Telemed. e-Health 2006, 12, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Cowan, K.E.; McKean, A.J.; Gentry, M.T.; Hilty, D.M. Barriers to use of telepsychiatry: Clinicians as gatekeepers. Mayo Clin. Proc. 2019, 94, 2510–2523. [Google Scholar] [CrossRef] [Green Version]
- Mahmoud, H.; Vogt, E.L.; Sers, M.; Fattal, O.; Ballout, S. Overcoming barriers to larger-scale adoption of telepsychiatry. Psychiatr. Ann. 2019, 49, 82–88. [Google Scholar] [CrossRef]
- Werner, P. Willingness to use telemedicine for psychiatric care. Telemed. J. e-Health 2004, 10, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Hailey, D.; Roine, R.; Ohinmaa, A. The effectiveness of telemental health applications: A review. Can. J. Psychiatry 2008, 53, 769–778. [Google Scholar] [CrossRef]
- García-Lizana, F.; Muñoz-Mayorga, I. What about telepsychiatry? A systematic review. Prim. Care Companion J. Clin. Psychiatry 2010, 12, e1–e5. [Google Scholar]
- O’Reilly, R.; Bishop, J.; Maddox, K.; Hutchinson, L.; Fisman, M.; Takhar, J. Is telepsychiatry equivalent to face-to-face psychiatry? Results from a randomized controlled equivalence trial. Psychiatr. Serv. 2007, 58, 836–843. [Google Scholar] [CrossRef]
- Cook, J.E.; Doyle, C. Working alliance in online therapy as compared to face-to-face therapy: Preliminary results. Cyber Psychol. Behav. 2002, 5, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Rees, C.S.; Stone, S. Therapeutic alliance in face-to-face versus videoconferenced psychotherapy. Prof. Psychol. Res. Pract. 2005, 36, 649. [Google Scholar] [CrossRef] [Green Version]
- Wagner, B.; Brand, J.; Schulz, W.; Knaevelsrud, C. Online working alliance predicts treatment outcome for posttraumatic stress symptoms in Arab war-traumatized patients. Depress. Anxiety 2012, 29, 646–651. [Google Scholar] [CrossRef] [PubMed]
- Shore, J.H.; Savin, D.; Orton, H.; Jan, B.; Manson, S.M. Diagnostic reliability of telepsychiatry in American Indian veterans. Am. J. Psychiatry 2007, 164, 115–118. [Google Scholar] [CrossRef]
- Mazhari, S.; Ghaffari-Nejad, A.; Mofakhami, O.; Raaii, F.; Bahaadinbeigy, K. Evaluating the diagnostic agreement between telepsychiatry assessment and face-to-face visit: A preliminary study. Iran. J. Psychiatry 2019, 14, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Norwood, C.; Moghaddam, N.G.; Malins, S.; Sabin-Farrell, R. Working alliance and outcome effectiveness in videoconferencing psychotherapy: A systematic review and noninferiority meta-analysis. Clin. Psychol. Psychother. 2018, 25, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Werner, P.; Karnieli, E. A model of the willingness to use telemedicine for routine and specialized care. J. Telemed. Telecare 2003, 9, 264–272. [Google Scholar] [CrossRef]
- Schwartz-Ilan, D. Between Privatization and Walfare: The Development of Healthcare Insurance in Israel; Ben-Gurion University Press: Beer Sheva, Israel, 2011. (In Hebrew) [Google Scholar]
- Svirski, B. The Privatization of the Public Healthcare System in Israel: Expressions and Implications; Adva Research Center: Tel Aviv, Israel, 2007. (In Hebrew) [Google Scholar]
- Aviram, U. Policy and Sevices in Mental Healthcare in Israel: Beteen Progress and Stagnation; Resling Publications: Tel Aviv, Israel, 2019. (In Hebrew) [Google Scholar]
- Golovetzik, P. Telepsychiatry—The Remote Treatment Unit (in Hebrew). Available online: https://hospitals.clalit.co.il/geha/he/med/clinics/Pages/telepsychiatry.aspx (accessed on 24 May 2021). (In Hebrew).
- Mashiah, M. Meuhedet HMO: First in remote medical treatment. Haaretz, 6 April 2020; 6. (In Hebrew) [Google Scholar]
- Leumit Remote Mental Healthcare Services. Available online: https://www.leumit.co.il/heb/remotemedicalservices/remotemed/remotementalhealthservices/ (accessed on 24 May 2021). (In Hebrew).
- Raviv, G. You Do Not Need to Leave Your Home. Available online: https://www.meuhedet.co.il/%D7%9E%D7%90%D7%95%D7%97%D7%93%D7%AA-%D7%9C%D7%A0%D7%A4%D7%A9/%D7%A4%D7%A1%D7%99%D7%9B%D7%95%D7%AA%D7%A8%D7%A4%D7%99%D7%94-%D7%90%D7%95%D7%A0%D7%9C%D7%99%D7%99%D7%9F/. (accessed on 26 November 2021). (In Hebrew).
- Morse, J.M. Sampling in grounded theory. In The SAGE Handbook of Grounded Theory; Bryant, A., Charmaz, K., Eds.; SAGE Publications: London, UK, 2007; pp. 229–244. [Google Scholar]
- Robinson, O.C. Sampling in interview-based qualitative research: A theoretical and practical guide. Qual. Res. Psychol. 2014, 11, 25–41. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. Discovery of Grounded Theory: Strategies for Qualitative Research; Adline Press: Chicago, IL, USA, 1967. [Google Scholar]
- Strauss, A.L. Qualitative Analysis for Social Scientists; Cambridge University Press: Cambridge, UK, 1987. [Google Scholar]
- Carlfjord, S.; Festin, K. Association between organizational climate and perceptions and use of an innovation in Swedish primary health care: A prospective study of an implementation. BMC Health Serv. Res. 2015, 15, 364–380. [Google Scholar] [CrossRef] [PubMed]
- Heinze, K.L.; Heinze, J.E. Individual innovation adoption and the role of organizational culture. Rev. Manag. Sci. 2020, 14, 561–586. [Google Scholar] [CrossRef]
- Nystrom, P.C.; Ramamurthy, K.; Wilson, A.L. Organizational context, climate and innovativeness: Adoption of imaging technology. J. Eng. Technol. Manag. 2002, 19, 221–247. [Google Scholar] [CrossRef]
- Rye, C.B.; Kimberly, J.R. The Adoption of Innovations by Provider Organizations in Health Care. Med Care Res. Rev. 2007, 64, 235–278. [Google Scholar] [CrossRef]
- Connolly, S.L.; Miller, C.J.; Lindsay, J.A.; Bauer, M.S. A systematic review of providers’ attitudes toward telemental health via videoconferencing. Clin. Psychol. Sci. Pract. 2020, 27, e12311. [Google Scholar] [CrossRef]
- Wynn, R.; Bergvik, S.; Pettersen, G.; Fossum, S. Clinicians’ experiences with videoconferencing in psychiatry. Stud. Health Technol. Inform. 2012, 180, 1218–1220. [Google Scholar] [PubMed]
- Newman, L.; Bidargaddi, N.; Schrader, G. Service providers’ experiences of using a telehealth network 12 months after digitisation of a large Australian rural mental health service. Int. J. Med Inform. 2016, 94, 8–20. [Google Scholar] [CrossRef]
- Lindsay, J.A.; Hudson, S.; Martin, L.; Hogan, J.B.; Nessim, M.; Graves, L.; Gabriele, J.; White, D. Implementing Video to Home to increase access to evidence-based psychotherapy for rural veterans. J. Technol. Behav. Sci. 2017, 2, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Simms, D.C.; Gibson, K.; O’Donnell, S. To use or not to use: Clinicians’ perceptions of telemental health. Can. Psychol. Psychol. Can. 2011, 52, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Adler-Milstein, J.; Kvedar, J.; Bates, D.W. Telehealth among US hospitals: Several factors, including state reimbursement and licensure policies, influence adoption. Health Aff. 2014, 33, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Cooper, S.B. Opinion leaders’ perspective of the benefits and barriers in telemedicine: A grounded theory study of telehealth in the Midwest. Q. Rev. Distance Educ. 2015, 16, 25–53. [Google Scholar]
- Gagnon, M.P.; Lamothe, L.; Fortin, J.P.; Cloutier, A.; Gagné, C.; Godin, G.; Reinharz, D. Telehealth adoption in hospitals: An organisational perspective. J. Health Organ. Manag. 2005, 19, 32–56. [Google Scholar] [CrossRef]
- Madar, G.; Lev-on, A.; Ash, N. Family physicians’ perceptions of the impact of e-visit systems on patient perceptions of and interactions with their family physicians. In The Futures of eHealth and Legal Challenges; Bauhle, T., Wernick, A., Eds.; Humboldt Institute for Internet and Society: Berlin, Germany, 2019; pp. 71–77. [Google Scholar]

{kind=link}
| Hierarchical Position | |||||
|---|---|---|---|---|---|
| National Managers | Regional Managers | Hospital Managers | Local Clinics | ||
| Healthcare organizations | HMO A | 1 | 2 | 3 | 2 |
| HMO B | 1 | ||||
| HMO C | 1 | 2 | 1 | ||
| HMO D | 1 | 2 | 1 | ||
| Gov | 1 | 4 | 5 | ||
| Total | 27 | ||||
| Geographical regions | National | 5 | |||
| North | 2 | 2 | 3 | ||
| Center | 2 | 3 | 4 | ||
| South | 2 | 2 | 2 | ||
| Total | 27 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magal, T.; Negev, M.; Kaphzan, H. Attitudinal Barriers Hindering Adoption of Telepsychiatry among Mental Healthcare Professionals: Israel as a Case-Study. Int. J. Environ. Res. Public Health 2021, 18, 12540. https://doi.org/10.3390/ijerph182312540
Magal T, Negev M, Kaphzan H. Attitudinal Barriers Hindering Adoption of Telepsychiatry among Mental Healthcare Professionals: Israel as a Case-Study. International Journal of Environmental Research and Public Health. 2021; 18(23):12540. https://doi.org/10.3390/ijerph182312540
Chicago/Turabian StyleMagal, Tamir, Maya Negev, and Hanoch Kaphzan. 2021. "Attitudinal Barriers Hindering Adoption of Telepsychiatry among Mental Healthcare Professionals: Israel as a Case-Study" International Journal of Environmental Research and Public Health 18, no. 23: 12540. https://doi.org/10.3390/ijerph182312540
APA StyleMagal, T., Negev, M., & Kaphzan, H. (2021). Attitudinal Barriers Hindering Adoption of Telepsychiatry among Mental Healthcare Professionals: Israel as a Case-Study. International Journal of Environmental Research and Public Health, 18(23), 12540. https://doi.org/10.3390/ijerph182312540