
Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
- Phase I: Concept design, solution architecture and technical specifications;
- Phase II: Development of prototype systems;
- Phase III: Development and testing of pilot systems.
2. Materials and Methods
- The development, administration and analysis of questionnaires capturing patients’ and professionals’ views on possible system functionalities (functional requirements);
- The development of a template collecting information about existing systems at the procurers’ premises (non-functional requirements);
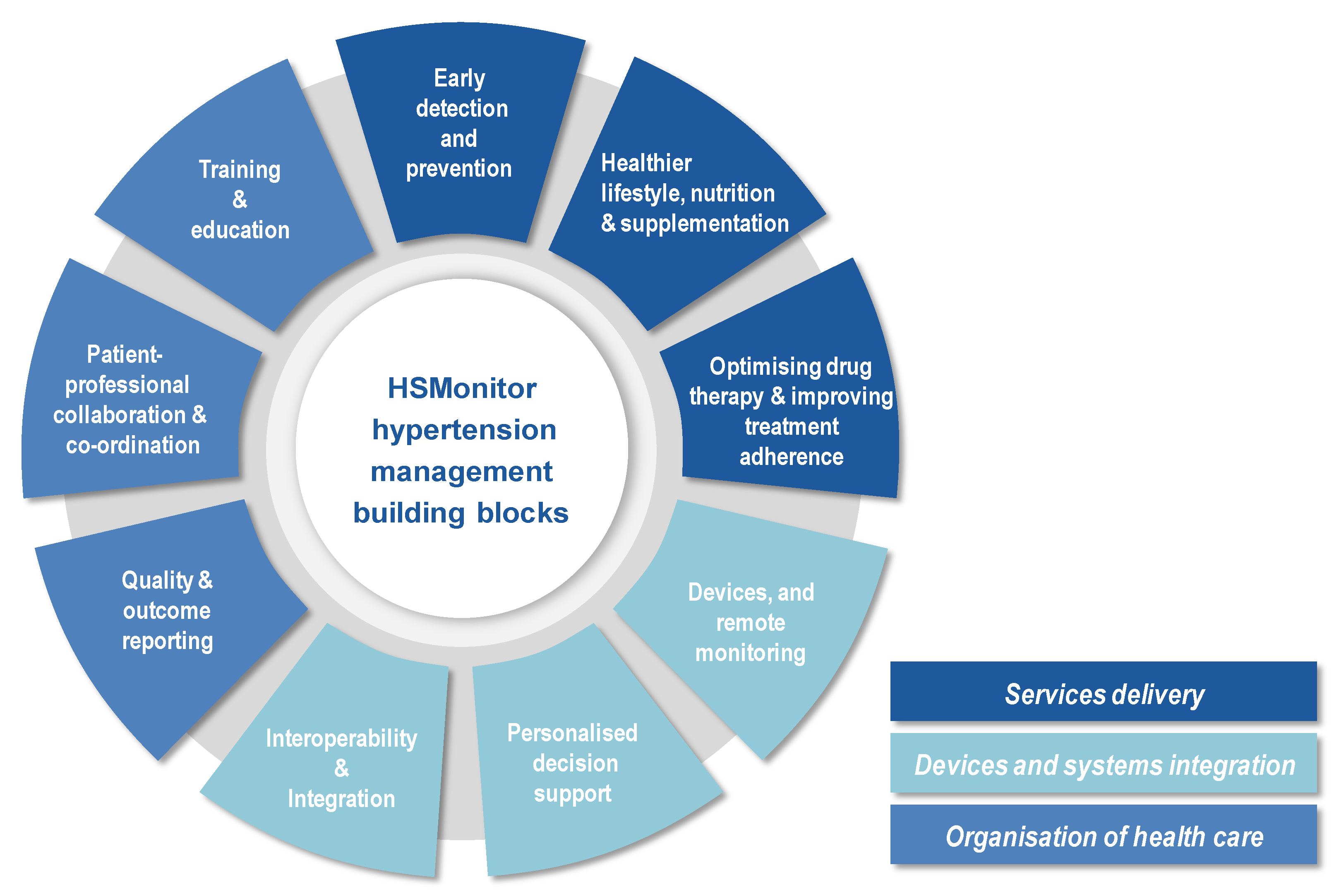
- The development of a set of use cases and corresponding process models, according to previously identified building blocks.
Data Collection to Inform the Development of Functional and Non-Functional Requirements
3. Results
3.1. Patients’ Questionnaire Results
3.2. Healthcare Professionals’ Questionnaire Results
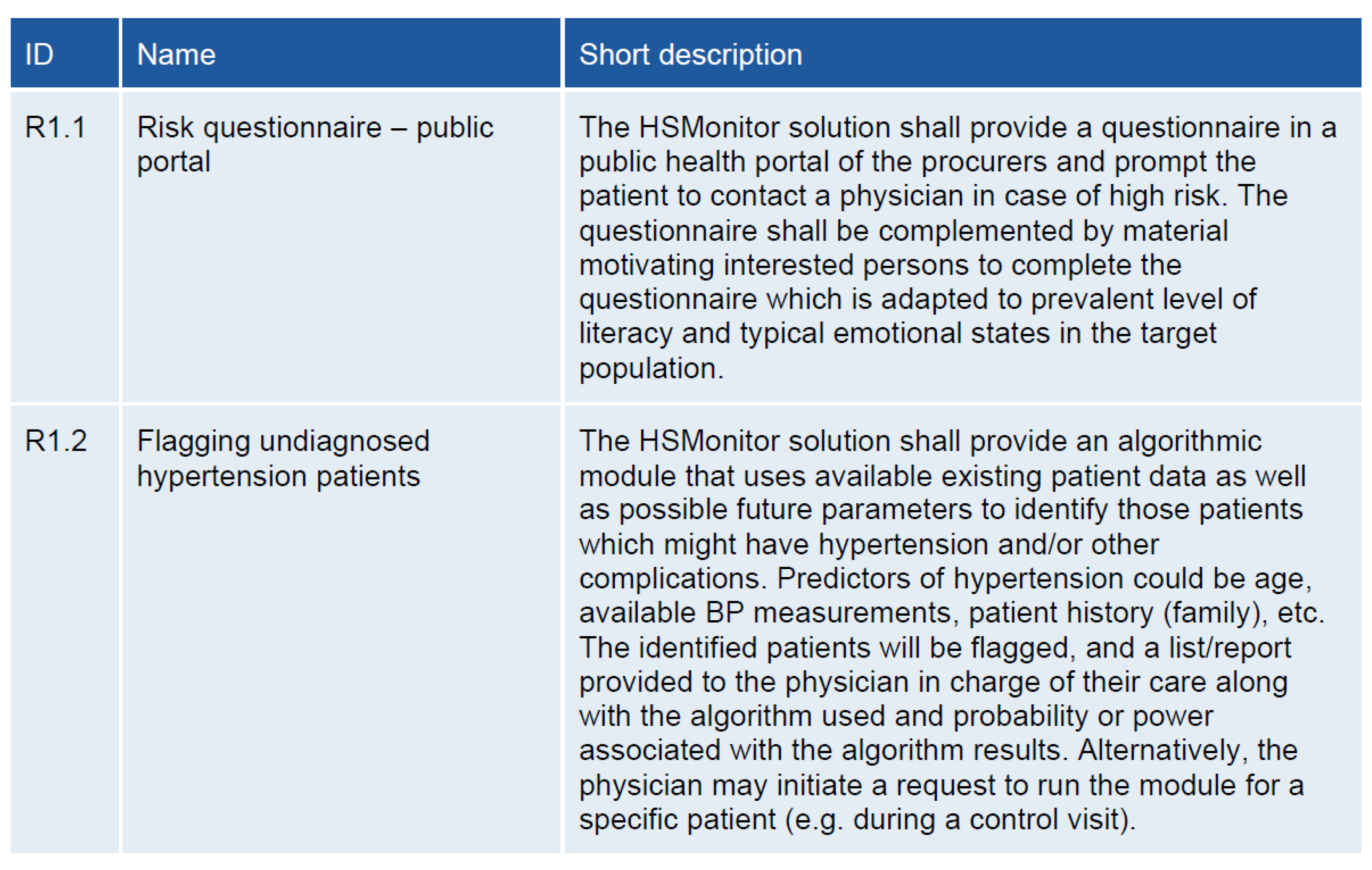
3.3. Functional Requirements
3.3.1. Early Detection and Prevention–R1
3.3.2. Healthier Lifestyle, Nutrition and Supplementation–R2
3.3.3. Optimizing Drug Therapy and Improving Treatment Adherence–R3
3.3.4. Devices and Remote Monitoring–R4
3.3.5. Personalized Decision Support–R5
3.3.6. Interoperability and Integration–R6
3.3.7. Quality and Outcome Reporting–R7
3.3.8. Patient-Professional Collaboration and Co-Ordination–R8
3.3.9. Training and Education–R9
3.4. Non-Functional Requirements
3.4.1. Service Organization and Staff
- ⚬
- General practitioner (GP);
- ⚬
- Specialist (cardiologist, nephrologist, internal medicine);
- ⚬
- Nurse;
- ⚬
- Pharmacist;
- ⚬
- Nutritionist;
- ⚬
- Physical trainer.
3.4.2. Existing IT Systems
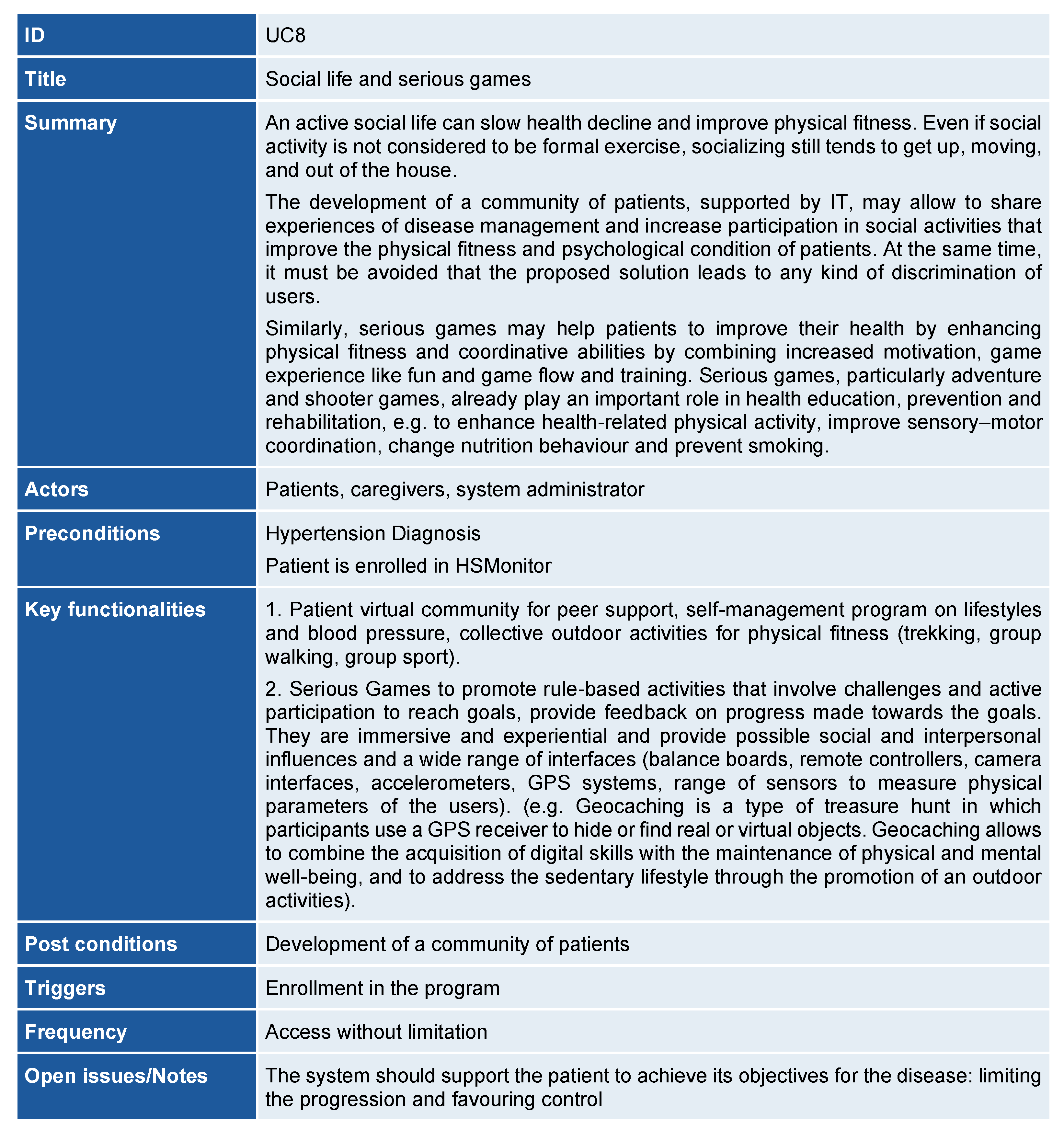
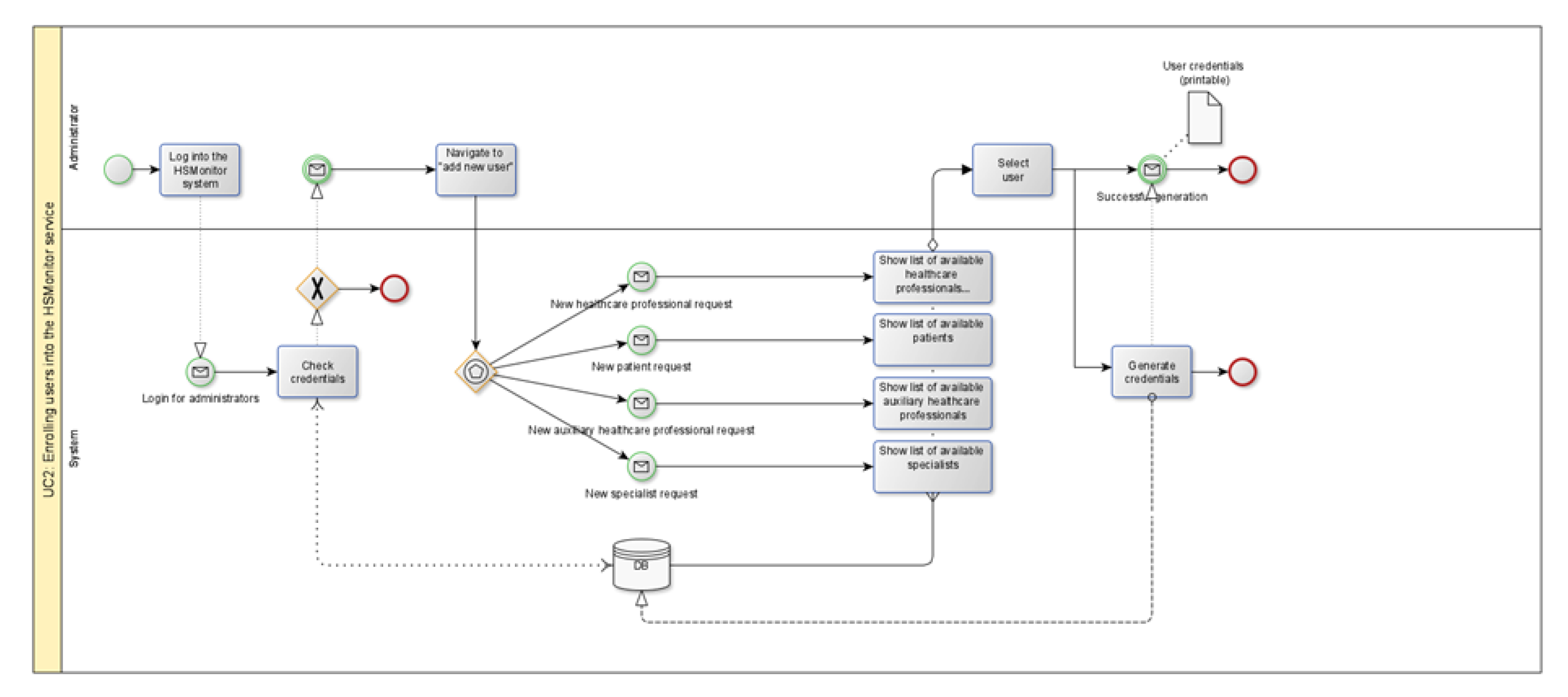
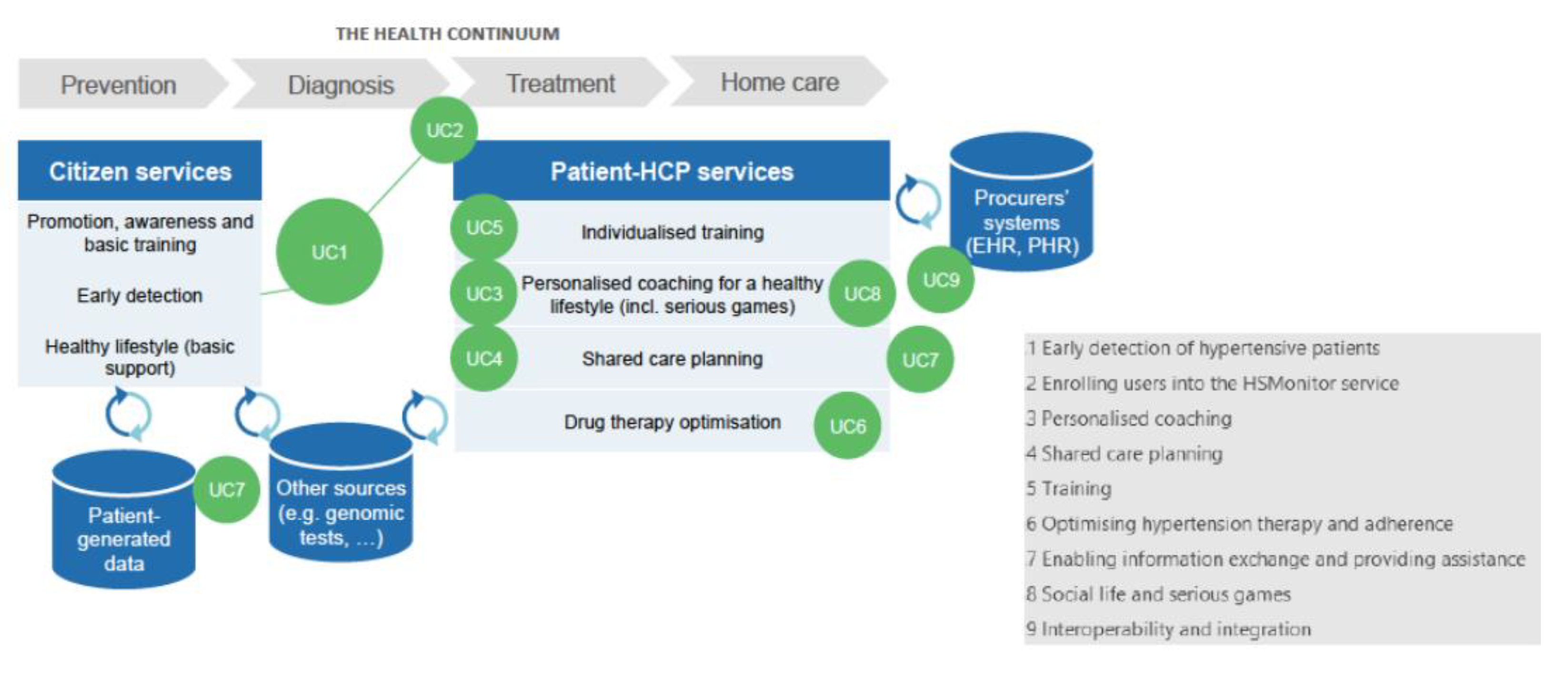
3.5. The UCs and Process Models
- ⚬
- UC1-Early identification of hypertensive citizens;
- ⚬
- UC2-Enrolment of diagnosed patients and professionals in the HSMonitor service;
- ⚬
- UC3-Personalized coaching;
- ⚬
- UC4-Shared care planning;
- ⚬
- UC5-Hypertension education;
- ⚬
- UC6-Optimization of hypertension treatment and adherence;
- ⚬
- UC7-Big data and information exchange;
- ⚬
- UC8-Social life and serious gaming;
- ⚬
- UC9-Interoperability and integration.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. HSMonitor Patients’ Questionnaire

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scores (%) | ||
|---|---|---|
| Q1. What age group are you in? | ||
| 18–39 | 1 (3.6) | |
| 40–59 | 11 (39.3) | |
| 60–79 | 15 (53.5) | |
| 80 or older | 1 (3.6) | |
| Q2. What statement best describes your current life with hypertension? | ||
| I am diagnosed with hypertension, but I feel no restrictions. | 18 (64.3) | |
| I have early symptoms of complications due to hypertension, but my quality of life still is very good. | 2 (7.1) | |
| My hypertension causes minor restrictions in my life. | 3 (10.7) | |
| My daily life activities are impaired due to my hypertension or its complications. | 5 (17.9) | |
| I am not able to work because of my hypertension or its complications. | 0 (0.0) | |
| Q3. How do you feel about your hypertension? * | ||
| I have hypertension, but feel confident that I can live a close-to-normal life in the future | 13 (46.4) | |
| I am worried about the negative effect hypertension may have on my life expectancy | 7 (25.0) | |
| I am worried about the reduced quality of life my hypertension may cause in the future | 4 (14.3) | |
| I feel well cared for | 9 (32.1) | |
| Other | 1 (3.6) | |
| Q4. Please tick which communication devices you have. * | ||
| Landline at home | 15 (53.6) | |
| Mobile phone or smartphone with access to the internet | 20 (71.4) | |
| Mobile phone or smartphone without access to the internet | 1 (3.6) | |
| PC with access to the internet (modem, through cable operator, satellite, etc.) | 16 (57.1) | |
| PC without access to the internet | 0 (0.0) | |
| Tablet with access to the internet | 7 (25.0) | |
| Q5. Do you have access to a hypertension plan, such as a document (online, paper) that contains relevant understandable information and can be used by your doctor and yourself to discuss your care? | ||
| Yes, I have access to such a plan online | 4 (14.3) | |
| Yes, I have access to a such a plan as paper document(s) | 4 (14.3) | |
| No | 16 (57.1) | |
| I do not know | 4 (14.3) | |
| Q6. If you do not have access to such a plan, would you like to in the future? | ||
| Yes | 18 (90.0) | |
| No | 2 (10.0) | |
| Q7. What kind of information would you like for such a plan to contain? * | ||
| Information and alerts about when I should visit my doctor | 21 (75.0) | |
| Setting lifestyle goals in the plan (e.g., exercise goals, diet goals) | 16 (57.1) | |
| Managing the drugs that I am taking and receiving reminders | 16 (57.1) | |
| Information about what I can do to contribute to a good therapy | 15 (53.6) | |
| The most relevant issues I should work on together with my doctor in the next three months | 16 (57.1) | |
| Information about situations in which I should get into contact with my doctor | 15 (53.6) | |
| Other | 0 (0.0) | |
| Q8. What is most important to you in order to use such a plan? * | ||
| My personal data is secure and protected | 13 (46.4) | |
| I can access the plan online (Internet connection required) | 17 (60.7) | |
| I can update the information in the plan | 7 (25.0) | |
| I can share the document with my doctor and others (other doctors, family members) | 10 (35.7) | |
| I can understand the plan because it uses language which is easy to understand | 11 (39.3) | |
| I can see my progress against the goals that have been set together with my doctor | 10 (35.7) | |
| I can see the progression of my disease (e.g., systolic/diastolic blood pressure) | 15 (53.6) | |
| I can review my medication and dosage | 11 (39.3) | |
| Other | 0 (0.0) | |
| Q9. Please provide up to three ideas and suggestions for what a shared hypertension document between you and your doctor should be able to do. Use sentences such as “I would like to be able to...” and “I wish there were...”. (Free text) | ||
| Q10. With regard to the training that hypertension patients typically receive, please tick which topics are relevant to you at some point in your life with hypertension. * | ||
| I want to know which foods are good and which I should avoid in order to to stay healthy | 17 (60.7) | |
| I want to know what physical activity and exercise help me maintain a healthy life with hypertension | 17 (60.7) | |
| I want to know what goals I should set in my plan to manage my blood pressure well | 9 (32.1) | |
| I want to learn about the best ways to handle stress | 10 (35.7) | |
| I want to know what the medication I am taking is for and what to do if I forget to take it | 12 (42.9) | |
| I want to know about technology and what medical equipment I can use to help me manage my hypertension | 9 (32.1) | |
| I want to know about all the different parameters that need to be monitored to keep the hypertension in control | 10 (35.7) | |
| I want to know what the appropriate actions are, in order to manage my disease on my own | 15 (53.6) | |
| I want to know what complications can occur with hypertension patients and how to react | 18 (64.3) | |
| Other | 0 (0.0) | |
| Q11. Have you received training for managing your hypertension yet? | ||
| Yes | 9 (32.1) | |
| No, I have not been offered any training by my doctor | 19 (67.9) | |
| No, I have declined to attend training offers by my doctor | 0 (0.0) | |
| Q12. If you have attended any hypertension management training courses, how personalised were they? * | ||
| The training took into account my age (minimum: child, adult, elderly) | 3 (33.3) | |
| The training took into account my medication | 4 (44.4) | |
| The training was available in other languages than my own | 0 (0.0) | |
| The training ensured that my personal questions were answered | 3 (33.3) | |
| Other | 3 (33.3) | |
| Q13. Which one of the following forms of training would you prefer to receive? | ||
| Online training (online materials, messages, videos) | 6 (21.4) | |
| Face-to-face training/physical presence | 8 (28.6) | |
| Mixed online and face-to-face training | 14 (50.0) | |
| Q14. With time, the care process needs may have to be adjusted, e.g., new medication, change in diet. Which method would you prefer in order to master such changes? * | ||
| Face-to-face training with a doctor or nurse | Personalized 11 (39.3) | lecture-style 6 (21.4) |
| Paper materials relating to the change | specifically put together and printed for me 5 (17.9) | general (e.g., leaflets) 3 (10.7) |
| Online hypertension knowledge base (e.g., website, platform) which I use myself | which I can use to read and add content 9 (32.1) | that I can use to read content 7 (25.0) |
| Messages delivered on my mobile devices that are personalised for me | Personalized 14 (50.0) | General 1 (3.6) |
| Q15. If you have attended hypertension management training course(s), how satisfied were you overall with them | ||
| very satisfied | 4 (14.3) | |
| somewhat satisfied | 4 (14.3) | |
| neither satisfied nor dissatisfied | 1 (3.6) | |
| somewhat dissatisfied | 0 (0.0) | |
| very dissatisfied | 0 (0.0) | |
| Q16: Have you felt at some point the need to re-visit certain aspects of the training courses? | ||
| Yes | 4 (14.3) | |
| No | 2 (7.1) | |
| Q17. Based on your experience with receiving training for hypertension, please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to see more...” and “I wish there were...”. (Free text) | ||
| Q18. What parameters do you currently monitor or are aware of that relate to managing your hypertension? * | ||
| Blood pressure | 25 (89.3) | |
| Pulse frequency | 23 (82.1) | |
| Weight | 16 (57.1) | |
| Blood cholesterol | 15 (53.6) | |
| Body fat | 7 (25.0) | |
| Body muscle | 0 (0.0) | |
| Blood sugar (glucose levels) | 13 (46.4) | |
| Physical activity (steps walked, stairs climbed) | 12 (42.9) | |
| Alcohol intake | 5 (17.9) | |
| Tobacco use | 5 (17.9) | |
| Other | 1 (3.6) | |
| Q19. Do you have and/or use any tools or devices to monitor such data or to generally inform yourself about your disease? * | Have | Use |
| Blood pressure monitor | 16 (57.1) | 7 (25.0) |
| Electronic scale | 5 (17.9) | 6 (21.4) |
| Notebook/PC | 8 (28.6) | 3 (10.7) |
| Tablet | 4 (14.3) | 0 (0.0) |
| Smartphone | 8 (28.6) | 4 (14.3) |
| Other | 1 (3.6) | 1 (3.6) |
| Q20. How do you currently communicate with your doctor regarding your disease? * | ||
| Via visitation, which the doctor initiates | 17 (60.7) | |
| Via visitation, which I have initiated | 12 (42.9) | |
| Via visitation, which the nurse has initiated | 4 (14.3) | |
| Via phone calls | 6 (21.4) | |
| Via phone messages (SMS, WhatsApp, etc.) | 2 (7.1) | |
| Via VoIP (e.g., Skype) and/or video conferencing | 0 (0.0) | |
| Via social media (e.g., Facebook, twitter) | 0 (0.0) | |
| Other | 3 (10.7) | |
| Q21. Do you wish for a more flexible communication than the current situation? | ||
| Yes | 14 (50.0) | |
| No, I am satisfied with the current way of communication | 11 (39.3) | |
| Q22. About what would you like to communicate with your doctor additionally? (Free text) | ||
| Q23. Which method or combination of methods do you think would be the most efficient for you to communicate with your doctor in the future? * | ||
| Via visitation, which the doctor initiates | 23 (82.1) | |
| Via visitation, which I have initiated | 11 (39.3) | |
| Via phone calls | 6 (21.4) | |
| Via phone messages (SMS, WhatsApp, etc.) | 11 (39.3) | |
| Via VoIP (e.g., Skype) and/or video conferencing | 9 (32.1) | |
| Via social media (e.g., Facebook, twitter) | 3 (10.7) | |
| Other | 2 (7.1) | |
| Q24. Based on your experience with communicating with your doctor, please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to...” and “I wish I could...”. (Free text) | ||
| Q25. Are you currently part of a community that deals with the aspect of hypertension? | ||
| Yes, a community specialised in hypertension only | 0 (0.0) | |
| Yes, a community which deals with hypertension among other topics | 0 (0.0) | |
| Yes, an informal community (e.g., friends group) | 0 (0.0) | |
| No | 26 (92.9) | |
| Q26. What topics would you consult the community about? * | ||
| I want to know which foods are good and which I should avoid to stay healthy | 14 (50.0) | |
| I want to know what physical activity and exercise helps me to maintain a healthy life with hypertension | 11 (39.3) | |
| I want to know what goals I should set in my plan to manage my hypertension well | 13 (46.4) | |
| I want to learn about best ways to handling stress | 9 (32.1) | |
| I want to know what the medication I am taking is for and what to do if I forget to take it | 9 (32.1) | |
| I want to know about technology and medical equipment I can use to help me manage my hypertension | 9 (32.1) | |
| I want to know about all the different parameters that need to be monitored to keep the hypertension in control | 7 (25.0) | |
| I want to post information and exchange ideas with others | 12 (42.9) | |
| I want to know what are appropriate actions to take in order to manage my disease on my own | 8 (28.6) | |
| I want to know what complications can occur with hypertension patients and how to react | 9 (32.1) | |
| Other | 9 (32.1) | |
| Q27. What do you expect from a community around hypertension? Please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to...” and “I wish I could...”. (Free text) | ||
| Q28 If you have some other ideas on what you would want to see added to the solution we will create, please write here: (Free text) | ||
Appendix B. HSMonitor Professionals Questionnaire
| Scores (%) | ||
|---|---|---|
| Q1. Do you have access to a hypertension plan, such as a document (online, paper) that contains relevant information and can be used by yourself or the patient to agree on the best care plan for them (including personalised goals)? | ||
| Yes, I have access to such a plan online | 5 (19.2) | |
| Yes, I have access to a such a plan as paper document(s) | 2 (7.7) | |
| No | 17 (65.4) | |
| I do not know | 2 (7.7) | |
| Q2. If you do not have access to such a plan, would you like to in the future? | ||
| Yes | 24 (92.3) | |
| No | 2 (7.7) | |
| Q3. What kind of information and functionality would you prefer for such a plan to contain? * | ||
| Information and alerts about when the patient should visit me or I should contact him/her | 17 (65.4) | |
| Setting goals in the plan together with the patient (e.g., exercise goals, diet goals) | 21 (80.8) | |
| Easy selection of information that can be printed and given together with a referral | 7 (26.9) | |
| Presentation of patient data according to my needs (e.g., show all blood pressure measurements in the last six months) | 19 (73.1) | |
| Information about what the patient can do to contribute to a good therapy | 19 (73.1) | |
| The most relevant issues the patient should work on together with me in the next three months | 9 (34.6) | |
| Other | 1 (3.8) | |
| Q4. What is most important to you in order to use such a plan? * | ||
| The personal data of the patient is secure and protected | 4 (15.4) | |
| I can access the plan online (Internet connection required) | 14 (53.8) | |
| I can update the information in the plan | 10 (38.5) | |
| I can rely on alerts to inform me when necessary (e.g., to schedule a check-up, re-do a test, etc.) | 11 (42.3) | |
| I can share the document with other colleagues | 7 (26.9) | |
| I can see the patient’s progress against the goals we have set together | 16 (61.5) | |
| I can see the progression of the patient’s disease (e.g., systolic/diastolic blood pressure) | 17 (65.4) | |
| I can review the patient’s medication and dosage | 18 (69.2) | |
| Other | 2 (7.7) | |
| Q5. Please provide up to three ideas and suggestions for what a shared hypertension document between you and your patient should be able to do. Use sentences such as “I would like to be able to...” and “I wish there were...”. (Free text) | ||
| Q6. Have you performed or been present at training(s) offered to patients for managing their hypertension? | ||
| Yes | 8 (30.8) | |
| No | 17 (65.4) | |
| Q7. If yes how personalised were the trainings? * | ||
| The training took into account the patient’s age (minimum: child, adult, elderly). | 12 (46.2) | |
| The training took into account the patient’s medication. | 10 (38.5) | |
| The training was available in more than one language | 1 (3.8) | |
| The training ensured that patients’ personal questions are answered | 6 (23.1) | |
| Other | 0 (0.0) | |
| Q8. Which one of the following forms of training would you prefer to prescribe to patients? | ||
| Online training (online materials, messages, videos) | 4 (15.4) | |
| Face-to-face training/physical presence | 2 (7.7) | |
| Mixed online and face-to-face training | 20 (76.9) | |
| Q9. Based on your experience with providing training for hypertension, please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to see more...” and “I wish there were...”. (Free text) | ||
| Q10. What parameters do you currently record or think the system should collect to help when treating your patients’ hypertension? * | Currently recorded | Should be recorded |
| Blood pressure | 21 (80.8) | 11 (42.3) |
| Pulse frequency | 20 (76.9) | 11 (42.3) |
| Weight | 18 (69.2) | 10 (38.5) |
| Blood cholesterol | 18 (69.2) | 12 (46.2) |
| Body fat | 5 (19.2) | 10 (38.5) |
| Body muscle | 2 (7.7) | 8 (30.8) |
| Blood sugar (glucose levels) | 16 (61.5) | 12 (46.2) |
| Physical activity (steps walked, stairs climbed) | 7 (26.9) | 15 (57.7) |
| Alcohol intake | 7 (26.9) | 11 (42.3) |
| Tobacco use | 17 (65.4) | 11 (42.3) |
| Other | 2 (7.7) | 2 (7.7) |
| Q11. Do you know if your patients adhere to the prescribed treatment (i.e., take the drugs as prescribed, do physical activity? | ||
| Yes | 8 (30.8) | |
| No | 18 (69.2) | |
| Q12. How do you currently communicate with your patients regarding their hypertension? * | ||
| Via visitation, which I initiate | 18 (69.2) | |
| Via visitation, which the patient has initiated | 18 (69.2) | |
| Via visitation, which a nurse has initiated | 10 (38.5) | |
| Via phone calls | 14 (53.8) | |
| Via phone messages (SMS, WhatsApp, etc.) | 3 (11.5) | |
| Via VoIP (e.g., Skype) and/or video conferencing | 0 (0.0) | |
| Via social media (e.g., Facebook, twitter) | 0 (0.0) | |
| Other | 6 (23.1) | |
| Q13. Do you wish for a more flexible communication than the current case? | ||
| Yes | 17 (65.4) | |
| No, I am satisfied with the current way of communication | 7 (26.9) | |
| Q14. Which method or combination of methods do you think would be most efficient for you to communicate with your patient in the future? * | ||
| Via visitation, which I initiate | 14 (53.8) | |
| Via visitation, which the patient has initiated | 11 (42.3) | |
| Via visitation, which a nurse has initiated | 11 (42.3) | |
| Via phone calls | 5 (19.2) | |
| Via phone messages (SMS, WhatsApp, etc.) | 9 (34.6) | |
| Via VOIP (e.g., Skype) and/or video conferencing | 9 (34.6) | |
| Via social media (e.g., Facebook, twitter) Other | 0 (0.0) 7 | |
| Q15. Based on your experience with communicating with your patients, please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to...” and “I wish I could...”. (Free text) | ||
| Q16. Hypertension treatment sometimes requires a combination of drugs at lower doses. However, some studies show that finding the right combination that works best for a specific patient can take time (sometimes years) as patients do not visit their doctors so often as being able to provide feedback and adjust the combination. From your experience, how many months on average are required to find the optimal combination of drugs for your hypertensive patient? | ||
| Average: | 6.4 months | |
| Q17. Are you currently part of a community that deals with the aspect of hypertension? | ||
| Yes, a community specialised in hypertension only | 4 (15.4) | |
| Yes, a community which deals with hypertension among other topics | 2 (7.7) | |
| Yes, an informal community (e.g., occasional meetings with other colleagues) | 4 (15.4) | |
| No | 16 (61.5) | |
| Q18. What topics would you consult the community about? * | ||
| Dietary recommendations for hypertension patients | 10 (38.5) | |
| Recommendations for physical activity and exercise suitable for hypertension patients | 15 (57.7) | |
| Suitable goals doctors should set with their hypertension patients | 12 (46.2) | |
| Appropriate recommendations to hypertension patients regarding handling stress | 13 (50.0) | |
| Newest medicine and medicinal products for hypertension | 10 (38.5) | |
| Newest technology and medical equipment that help patients manage their hypertension | 9 (34.6) | |
| Newest information about parameters that need to be monitored to keep the hypertension under control | 11 (42.3) | |
| I want to post information and exchange ideas with other colleagues | 11 (42.3) | |
| Information about complications with hypertension patients and appropriate management | 9 (34.6) | |
| Other | 2 (7.7) | |
| Q19. What do you expect from a community around hypertension? Please provide up to three ideas and suggestions for improvement. Use sentences such as “I would like to...” and “I wish I could...”. (Free text) | ||
| Q20. If you have some other ideas on what you would want to see added to the solution we will create, please write here: (Free text) | ||
References
- England, K.; Azzopardi-Muscat, N. Demographic trends and public health in Europe. Eur. J. Public Health 2017, 27 (Suppl. 4), 9–13. [Google Scholar] [CrossRef]
- Iaccarino, G.; Grassi, G.; Borghi, C.; Ferri, C.; Salvetti, M.; Volpe, M. SARS-RAS Investigators. Age and Multimorbidity Predict Death Among COVID-19 Patients: Results of the SARS-RAS Study of the Italian Society of Hypertension. Hypertension 2020, 76, 366–372. [Google Scholar] [CrossRef]
- Marois, G.; Muttarak, R.; Scherbov, S. Assessing the potential impact of COVID-19 on life expectancy. PLoS ONE 2020, 15, e0238678. [Google Scholar] [CrossRef]
- European Commission. Communication COM(2007)799: Pre-Commercial Procurement: Driving Innovation to Ensure Sustainable High Quality Public Services in Europe. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=COM:2007:0799:FIN:EN:PDF (accessed on 19 October 2021).
- European Commission. Decision C(2019)4575. COMMISSION IMPLEMENTING DECISION Amending Implementing Decision C(2017)7124 as Regards the Work Programme for 2018–2020 within the Framework of the Specific Programme Implementing Horizon 2020—The Framework Programme for Research and Innovation (2014–2020) and on the Financing of the Work Programme for 2020. Available online: https://ec.europa.eu/transparency/documents-register/detail?ref=C(2019)4575&lang=en (accessed on 19 October 2021).
- OECD. Public Procurement for Innovation: Good Practices and Strategies; OECD Public Governance Reviews; OECD Publishing: Paris, France, 2017. [Google Scholar] [CrossRef]
- Brogaard, L. Innovation and value in pre-commercial procurement: A systematic evaluation of national experiences. J. Strateg. Contracting Negot. 2017, 3, 137–156. [Google Scholar] [CrossRef]
- García-Esquinas, E.; Ortolá, R.; Prina, M.; Stefler, D.; Rodríguez-Artalejo, F.; Pastor-Barriuso, R. Trajectories of Accumulation of Health Deficits in Older Adults: Are There Variations According to Health Domains? J. Am. Med. Dir. Assoc. 2019, 20, 710–717.e6. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Du, Z.; Bian, W.; Wu, S.; Gao, B.; Sun, Y.; Kang, Z.; Zhang, X. Effects of blood pressure goals on cardiovascular outcomes in hypertensive patients. Arch. Med. Sci. 2019, 15, 1381–1387. [Google Scholar] [CrossRef]
- Visco, V.; Finelli, R.; Pascale, A.V.; Mazzeo, P.; Ragosa, N.; Trimarco, V.; Illario, M.; Ciccarelli, M.; Iaccarino, G. Difficult-to-control hypertension: Identification of clinical predictors and use of ICT519 based integrated care to facilitate blood pressure control. J. Hum. Hypertens. 2018, 32, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Carey, R.M.; Muntner, P.; Bosworth, H.B.; Whelton, P.K. Prevention and Control of Hypertension: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1278–1293. [Google Scholar] [CrossRef]
- Alleyne, G.; Stuckler, D.; Alwan, A. The hope and the promise of the UN Resolution on non-communicable diseases. Global Health 2010, 6, 15. [Google Scholar] [CrossRef][Green Version]
- Gee, P.M.; Greenwood, D.A.; Paterniti, D.A.; Ward, D.; Miller, L.M. The eHealth enhanced chronic care model: A theory derivation approach. J. Med. Internet Res. 2015, 17, e86. [Google Scholar] [CrossRef] [PubMed]
- Communication from the Commission to the European Parliament, the European Council, the Council, the European Economic and Social Committee and the Committee of the Regions on Enabling the Digital Transformation of Health and Care in the Digital Single Market; Empowering Citizens and Building a Healthier Society. Available online: https://digital-strategy.ec.europa.eu/en/library/communication-enabling-digital-transformation-health-and-care-digital-single-market-empowering (accessed on 19 October 2021).
- Roller-Wirnsberger, R.; Liotta, G.; Lindner, S.; Iaccarino, G.; De Luca, V.; Geurden, B.; Maggio, M.; Longobucco, Y.; Vollenbroek-Hutten, M.; Cano, A.; et al. Public health and clinical approach to proactive management of frailty in multidimensional arena. Ann. Ig. 2021, 33, 543–554. [Google Scholar] [CrossRef]
- Bevilacqua, R.; Casaccia, S.; Cortellessa, G.; Astell, A.; Lattanzio, F.; Corsonello, A.; D’Ascoli, P.; Paolini, S.; Di Rosa, M.; Rossi, L.; et al. Coaching Through Technology: A Systematic Review into Efficacy and Effectiveness for the Ageing Population. Int. J. Environ. Res. Public Health 2020, 17, 5930. [Google Scholar] [CrossRef]
- De Luca, V.; Tramontano, G.; Riccio, L.; Trama, U.; Buono, P.; Losasso, M.; Bracale, U.M.; Annuzzi, G.; Zampetti, R.; Cacciatore, F.; et al. "One Health" Approach for Health Innovation and Active Aging in Campania (Italy). Front. Public Health 2021, 9, 658959. [Google Scholar] [CrossRef] [PubMed]
- Blueprint Digital Transformation of Health and Care for the Ageing Society. Available online: https://futurium.ec.europa.eu/en/active-and-healthy-living-digital-world/library/eip-aha-blueprint?language=sv (accessed on 19 October 2021).
- Vincent, C.J.; Blandford, A. The challenges of delivering validated personas for medical equipment design. Appl. Ergon. 2014, 45, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Stellefson, M.; Dipnarine, K.; Stopka, C. The Chronic Care Model and diabetes management in US primary care settings: A systematic review. Prev. Chronic Dis. 2013, 10, E26. [Google Scholar] [CrossRef]
- Wagner, E.H.; Austin, B.T.; Von Korff, M. Organizing care for patients with chronic illness. Milbank Q. 1996, 74, 511–544. [Google Scholar] [CrossRef]
- Bodenheimer, T.; Wagner, E.H.; Grumbach, K. Improving primary care for patients with chronic illness. JAMA 2002, 288, 1775–1779. [Google Scholar] [CrossRef]
- Carter, B.L.; Bosworth, H.B.; Green, B.B. The hypertension team: The role of the pharmacist, nurse, and teamwork in hypertension therapy. J. Clin. Hypertens. (Greenwich) 2012, 14, 51–65. [Google Scholar] [CrossRef]
- Lewanczuk, R. Innovations in primary care: Implication for hypertension detection and treatment. Can. J. Cardiol. 2006, 22, 614–616. [Google Scholar] [CrossRef]
- Jacobson, I.; Christerson, M.; Johnsson, P.; Overgaards, G. Object-Oriented Software Engineering: A Use CaseDriven Approach; Addison-Wesley Professional: Boston, MA, USA, 1992. [Google Scholar]
- De Luca, V.; Birov, S.; Beyhan, O.; Robinson, S.; Sanchez-Nanclares, G.; Acuña, M.D.; Fernandes, A.; Hammerschmidt, R.; Annuzzi, G.; Iaccarino, G.; et al. European Specifications for Value-Based Pre-Commercial Procurement Ofinnovative ICT for Empowerment and Self-Management of Diabetes Mellituspatients. In Proceedings of the 5th International Conference on Informationand Communication Technologies for Ageing Well and e-Health (ICT4AWE), Heraklion, Greece, 2–4 May 2019; Volume 1, pp. 19–27. [Google Scholar] [CrossRef]
- White, S.A.; Bock, C. BPMN 2.0 Handbook Second Edition: Methods, Concepts, Case Studies and Standards in Business Process Management Notation; Future Strategies Inc.: Lighthouse Point, FL, USA, 2011; ISBN 978-0-9849764-0-9. Available online: https://www.conradbock.org/white-bpmn2-process-bookmark-web.pdf (accessed on 19 October 2021).
- Khoong, E.C.; Olazo, K.; Rivadeneira, N.A.; Thatipelli, S.; Barr-Walker, J.; Fontil, V.; Lyles, C.R.; Sarkar, U. Mobile health strategies for blood pressure self-management in urban populations with digital barriers: Systematic review and meta-analyses. NPJ Digit. Med. 2021, 4, 114. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Luca, V.; Lazic, V.; Birov, S.; Piesche, K.; Beyhan, O.; Pengo, M.F.; Melgara, M.; Sherman, M.H.; Lilja, M.; Balenovic, A.; et al. Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process. Int. J. Environ. Res. Public Health 2021, 18, 12442. https://doi.org/10.3390/ijerph182312442
De Luca V, Lazic V, Birov S, Piesche K, Beyhan O, Pengo MF, Melgara M, Sherman MH, Lilja M, Balenovic A, et al. Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process. International Journal of Environmental Research and Public Health. 2021; 18(23):12442. https://doi.org/10.3390/ijerph182312442
Chicago/Turabian StyleDe Luca, Vincenzo, Vanja Lazic, Strahil Birov, Klaus Piesche, Ozan Beyhan, Martino Francesco Pengo, Marcello Melgara, Marie Holm Sherman, Mikael Lilja, Antonija Balenovic, and et al. 2021. "Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process" International Journal of Environmental Research and Public Health 18, no. 23: 12442. https://doi.org/10.3390/ijerph182312442
APA StyleDe Luca, V., Lazic, V., Birov, S., Piesche, K., Beyhan, O., Pengo, M. F., Melgara, M., Sherman, M. H., Lilja, M., Balenovic, A., Parati, G., Triassi, M., Izzo, R., Iaccarino, G., & Illario, M. (2021). Digitally Enabled Health Service for the Integrated Management of Hypertension: A Participatory User-Centred Design Process. International Journal of Environmental Research and Public Health, 18(23), 12442. https://doi.org/10.3390/ijerph182312442