
Institutional Determinants of Informal Payments for Health Services: An Exploratory Analysis across 117 Countries




Abstract
1. Introduction
Tackling Informal Payments for Healthcare: What Role for Institutions?
2. Materials and Methods
3. Results
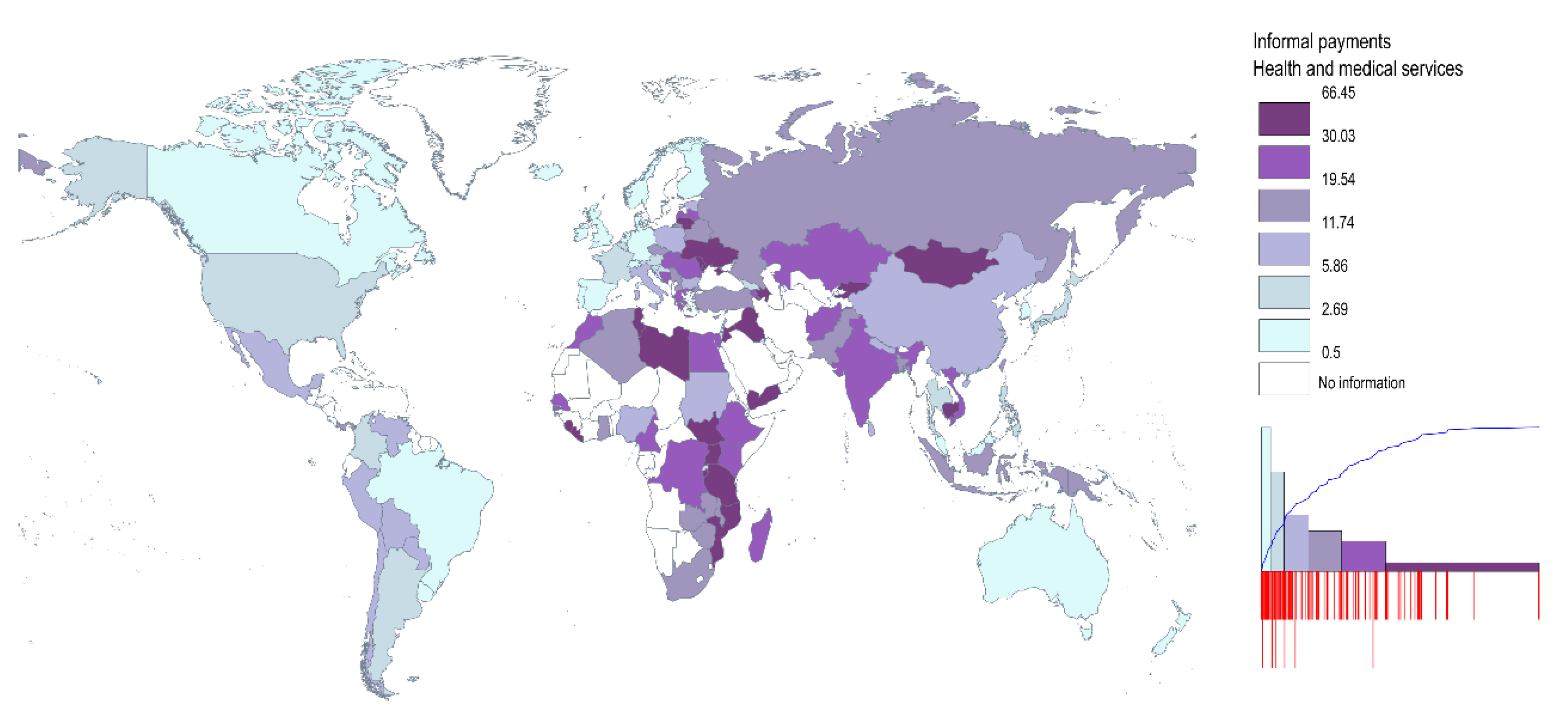
3.1. Data Description
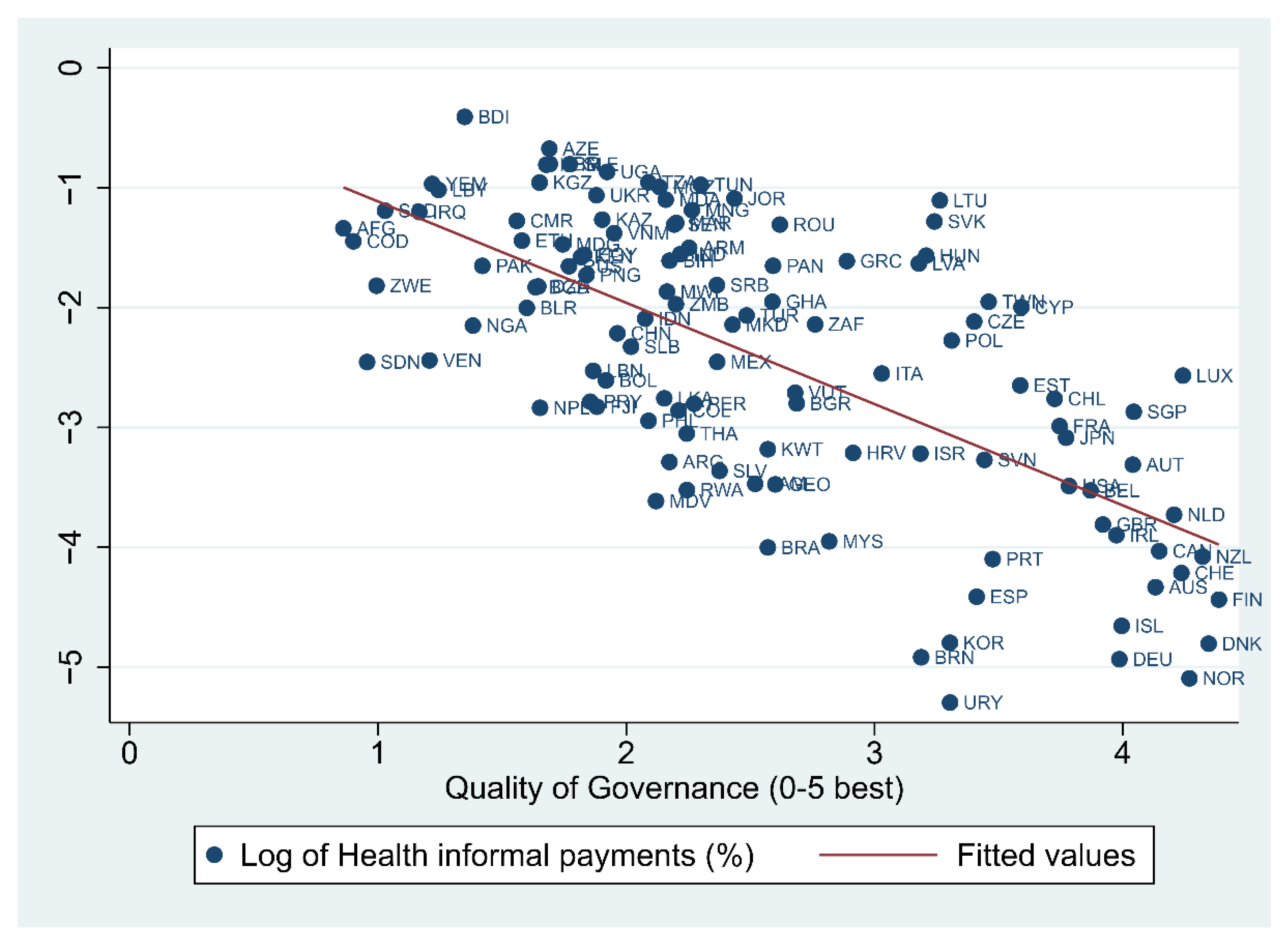
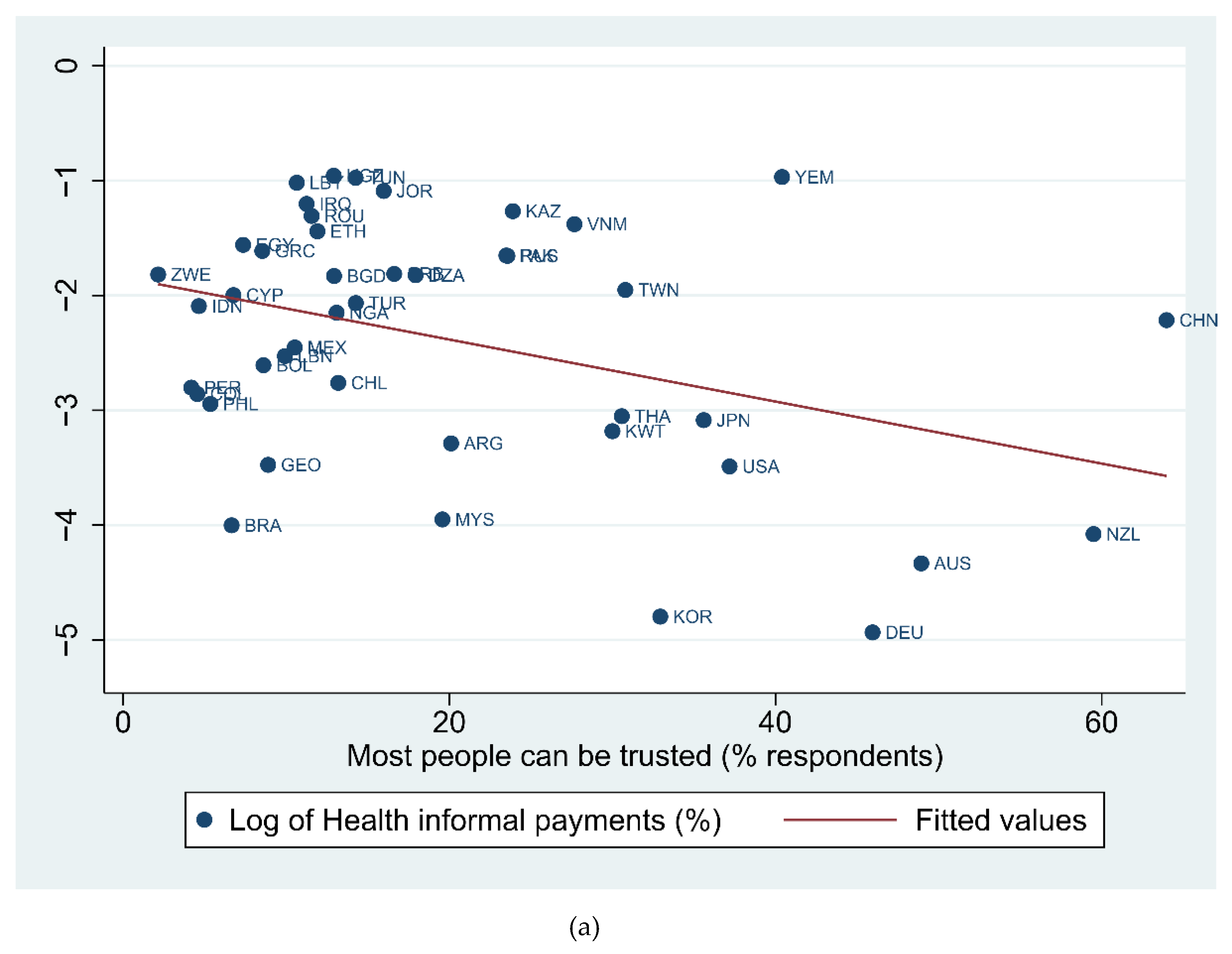
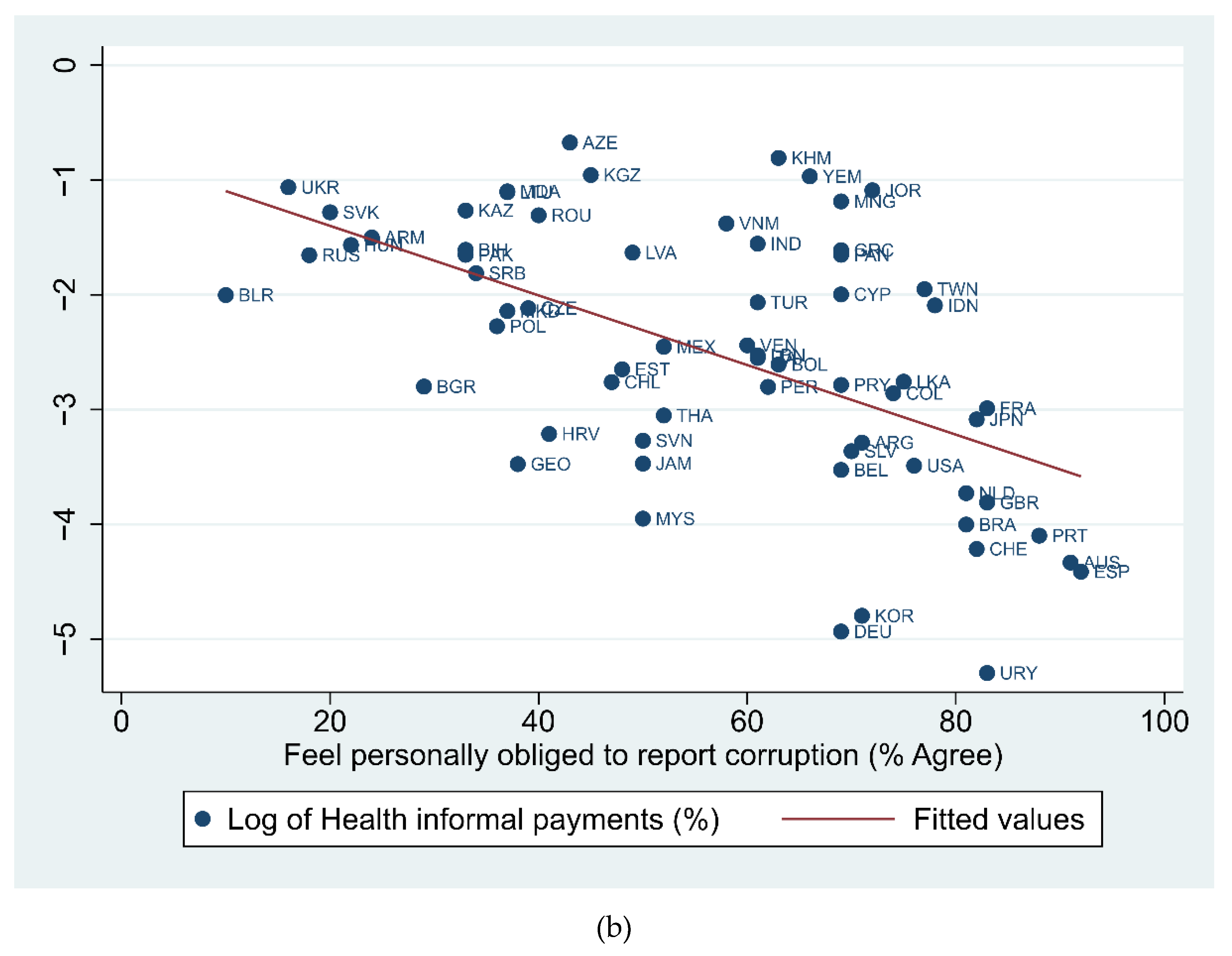
3.2. Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description | Source |
|---|---|---|
| Informal payments | ||
| Informal payments in health sector | Share of population responding ‘Yes’ when it comes to ‘Medical and health services’ to the following question: ‘In your contact or contacts with the institutions have your or anyone living in your household paid a bribe in any form in the past 12 months?’ | The Global Corruption Barometer, Transparency InternationalDownloaded from QoG Standard dataset [40] |
| Formal institutions | ||
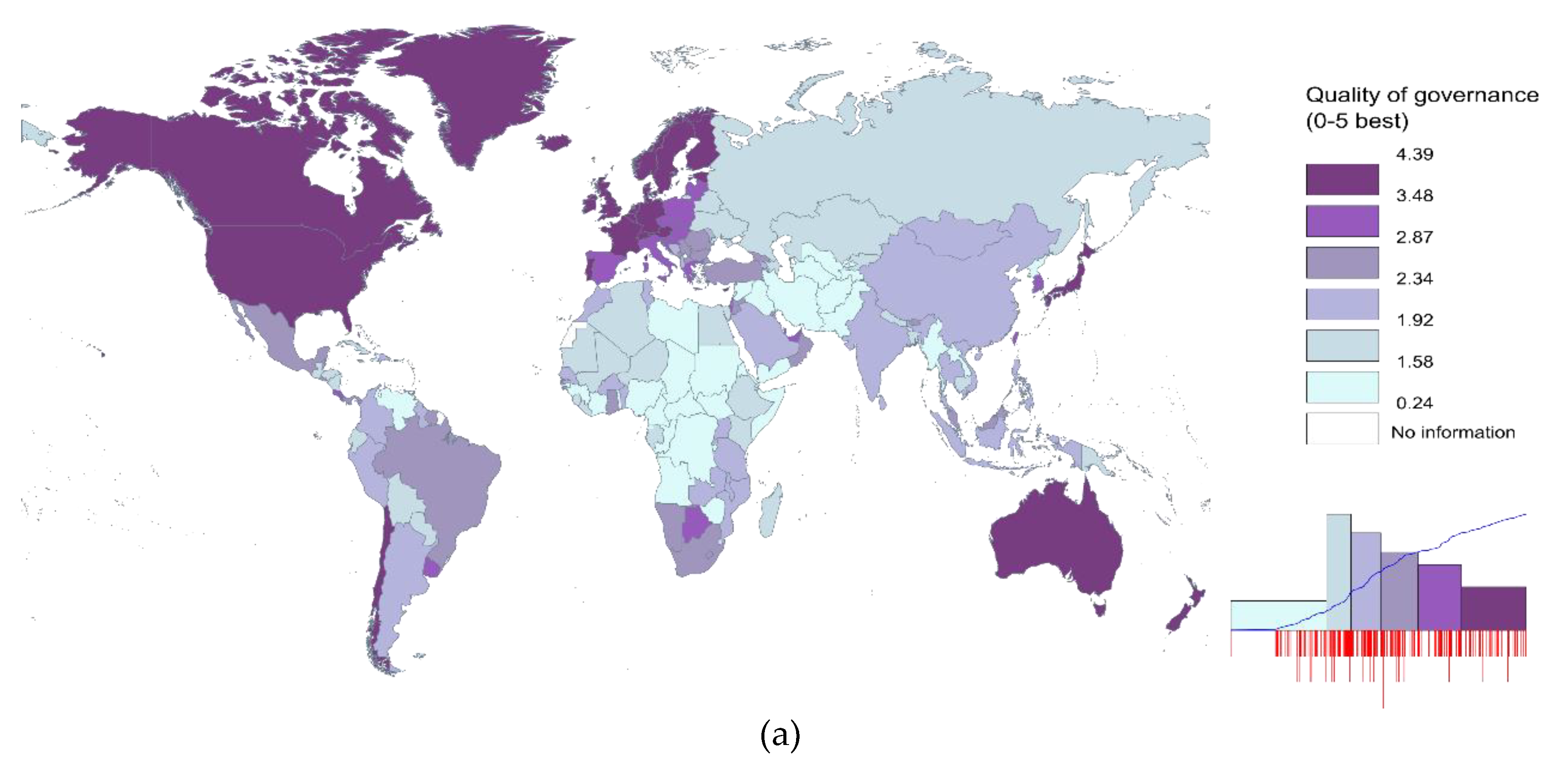
| Quality of governance | The Quality of Governance Index (estimate). The index was rescaled to 0–5 (best) values. The six dimensions of the index were aggregated using a factorial analysis. | Worldwide Governance indicators database of World Bank [39] |
| Health expenditures | Current Health Expenditure (CHE) as % Gross Domestic Product (GDP), Percentage | World Health Organization |
| Out-of-pocket expenditure | Out-of-pocket (OOPS) as % of Current Health Expenditure (CHE), Percentage | World Health Organization |
| Private health expenditure | Domestic Private Health Expenditure (PVT-D) as % Current Health Expenditure (CHE), Percentage | World Health Organization |
| Doctor ratio | Medical doctors (per 10,000) | World Health Organization |
| Informal institutions | ||
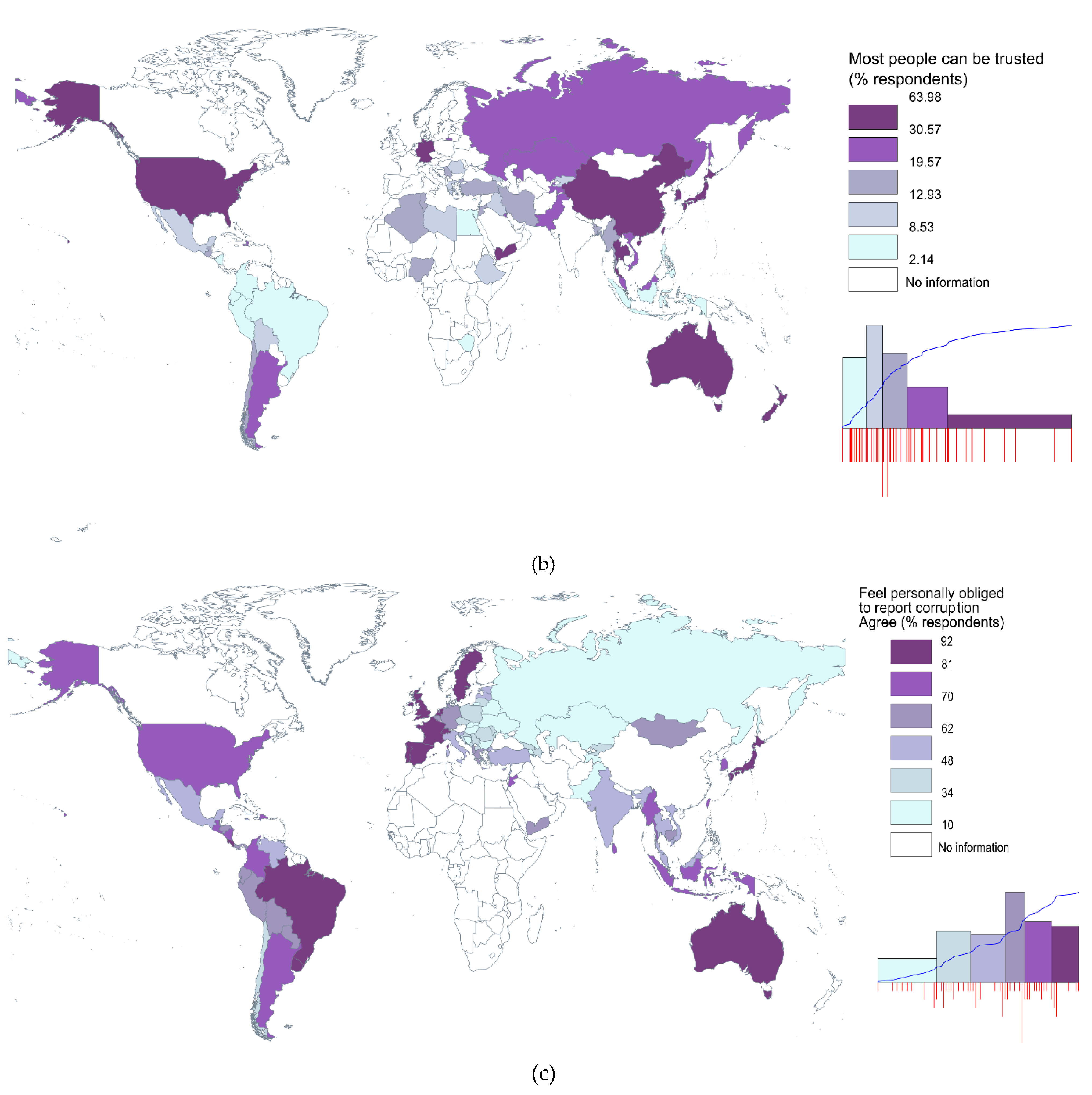
| Feel personally obliged to report corruption | Share of people agreeing with the following statement: ‘Feel personally obliged to report corruption’. The values are from and around 2017, with a ± 3 years margin interval. | The Global Corruption Barometer, Transparency InternationalDownloaded from QoG Standard dataset [40] |
| Trust | Share of people responding that ‘Most people can be trusted’ to the following question: ‘Generally speaking, would you say that most people can be trusted or that you need to be very careful in dealing with people?’ The values are from and around 2017, with a ± 3 years margin interval. | World Values SurveyDownloaded from QoG Standard dataset [40] |
| Other variables | ||
| Age dependency | Age dependency ratio (% of working-age population) | World Bank |
| Education | Educational attainment (population weighted education per capita, age 25+, mean years) | Institute for Health Metrics and Evaluation [71] |
| Employment | Employment to population ratio, 15+, total (%) (modelled ILO estimate) | World Bank |
| GDP per capita | Real GDP per capita, PPP | PWT version 9.1 [72] |
| GDP per capita growth | Real GDP growth | |
| Life expectancy | Life expectancy at birth, total (years) | World Bank |
| Urban | Urban population (% of total population) | World Bank |
| Variable | Obs. | Mean | Std. Dev. | Min | Max |
|---|---|---|---|---|---|
| Panel data | |||||
| Informal Payments | |||||
| Informal payments in health sector | 354 | 13.39 | 14.02 | 0.00 | 66.45 |
| High income | 138 | 5.75 | 7.87 | 0.00 | 35.85 |
| Upper-middle income | 102 | 12.92 | 13.24 | 0.36 | 64.91 |
| Lower-middle income | 90 | 20.03 | 13.06 | 0.97 | 60.34 |
| Low income | 30 | 31.72 | 15.70 | 1.75 | 66.45 |
| Formal institutions | |||||
| Quality of governance | 354 | 2.66 | 0.94 | 0.79 | 4.43 |
| Health expenditures | 354 | 6.81 | 2.60 | 1.78 | 16.35 |
| Out-of-pocket expenditure | 354 | 33.20 | 18.62 | 1.20 | 82.88 |
| Private health expenditure | 354 | 41.19 | 19.00 | 1.20 | 84.60 |
| Doctor ratio | 264 | 25.77 | 18.00 | 0.13 | 78.09 |
| Other variables | |||||
| Age dependency | 354 | 56.60 | 15.91 | 26.99 | 104.70 |
| Education | 354 | 9.13 | 3.44 | 1.69 | 14.69 |
| Employment | 354 | 56.95 | 11.12 | 31.64 | 87.02 |
| GDP per capita | 346 | 21,318.13 | 18,789.94 | 746.30 | 91,533.16 |
| GDP per capita growth | 346 | 4.48 | 7.34 | −27.87 | 36.08 |
| Life expectancy | 354 | 72.40 | 7.93 | 48.47 | 83.33 |
| Urban | 354 | 61.57 | 21.22 | 10.92 | 100.00 |
| Cross-sectional data | |||||
| Informal payments | |||||
| Informal payments in health sector | 113 | 15.00 | 13.68 | 0.50 | 66.45 |
| High income | 40 | 6.70 | 8.01 | 0.50 | 33.07 |
| Upper-middle income | 32 | 13.84 | 11.85 | 1.83 | 50.95 |
| Lower-middle income | 27 | 20.43 | 11.17 | 3.46 | 44.56 |
| Low income | 14 | 30.86 | 17.00 | 2.95 | 66.45 |
| Formal institutions | |||||
| Quality of governance | 113 | 2.55 | 0.93 | 0.86 | 4.39 |
| Health expenditures | 113 | 6.76 | 2.60 | 2.06 | 16.28 |
| Private health expenditure | 113 | 40.18 | 18.41 | 1.64 | 79.07 |
| Informal institutions | |||||
| Feel personally obliged to report corruption | 64 | 56.17 | 20.69 | 10.00 | 92.00 |
| Trust | 42 | 19.71 | 15.12 | 2.14 | 63.98 |
| Other variables | |||||
| Age dependency | 113 | 57.64 | 17.35 | 27.46 | 103.19 |
| Education | 113 | 8.88 | 3.60 | 1.73 | 14.46 |
| Employment | 113 | 57.61 | 12.18 | 33.49 | 86.46 |
| Life expectancy | 113 | 72.08 | 7.98 | 50.17 | 82.96 |




References
- World Health Organization. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov (accessed on 10 September 2021).
- World Bank. Ensuring Integrity in Governments’ Response to COVID-19; World Bank: Washington, DC, USA, 2020. [Google Scholar]
- Levin-Scherz, J.; Parson, T.; The Paradox of Medical Costs during the Pandemic. EconoFact. 2020. Available online: https://econofact.org/the-paradox-of-medical-costs-during-the-pandemic (accessed on 10 September 2021).
- Hellowell, M.; Okafor, Y. Understanding the Impact of COVID-19 on the Private Health Sector in Africa. 2021. Blog—BMJ Global Health. Available online: https://blogs.bmj.com/bmjgh/2021/03/09/understanding-the-impact-of-covid-19-on-the-private-health-sector-in-africa/?fbclid=IwAR2Z9FBrxxBvC_-is7IvY8S_xi1NHl7_NugH3WsnFMV6GicMchatCHU_hRc (accessed on 1 October 2021).
- Cepeda Cuadrado, D. The Ignored Pandemic behind COVID-19: The Impact of Corruption on Healthcare Service Delivery; Transparency International: Brussels, Belgium, 2020. [Google Scholar]
- Transparency International. Global Corruption Barometer (GCB)—EU. 2021. Available online: https://www.transparency.org/en/gcb/eu/european-union-2021/press-and-downloads (accessed on 15 September 2021).
- Cohen, N. Informal Payments for Health Care—The Phenomenon and Its Context. Health Econ. Policy Law 2012, 7, 285–308. [Google Scholar] [CrossRef] [PubMed]
- Tomini, S.; Groot, W.; Pavlova, M. Paying Informally in the Albanian Health Care Sector: A Two-Tiered Stochastic Frontier Model. Eur. J. Health Econ. 2012, 13, 777–788. [Google Scholar] [CrossRef]
- Williams, C.C.; Horodnic, A.V. Evaluating the Prevalence of Informal Payments for Health Services in Southeast Europe: An Institutional Approach. Southeast Eur. Black Sea Stud. 2018, 18, 345–365. [Google Scholar] [CrossRef]
- Gaal, P.; McKee, M. Fee-for-Service or Donation? Hungarian Perspectives on Informal Payment for Health Care. Soc. Sci. Med. 2005, 60, 1445–1457. [Google Scholar] [CrossRef]
- Ensor, T. Informal Payments for Health Care in Transition Economies. Soc. Sci. Med. 2004, 58, 237–246. [Google Scholar] [CrossRef]
- Atanasova, E.; Pavlova, M.; Groot, W. Out-of-Pocket Patient Payments for Public Health Care Services in Bulgaria. Front. Public Health 2015, 3, 175. [Google Scholar] [CrossRef] [PubMed]
- Liaropoulos, L.; Siskou, O.; Kaitelidou, D.; Theodorou, M.; Katostaras, T. Informal Payments in Public Hospitals in Greece. Health Policy 2008, 87, 72–81. [Google Scholar] [CrossRef]
- Williams, C.C.; Horodnic, A.V. Rethinking Informal Payments in Europe: An Institutional Approach. Health Policy 2017, 121, 1053–1062. [Google Scholar] [CrossRef]
- North, D.C. Institutional Change and Economic Performance; Cambridge University Press: Cambridge, UK, 1990. [Google Scholar]
- Baumol, W.J.; Blinder, A. Macroeconomics: Principles and Policy; South-Western Publishing: Cincinnati, OH, USA, 2008. [Google Scholar]
- Helmke, G.; Levitsky, S. Informal Institutions and Comparative Politics: A Research Agenda. Perspect. Politics 2004, 2, 725–740. [Google Scholar] [CrossRef]
- García, P.J. Corruption in Global Health: The Open Secret. Lancet 2019, 394, 2119–2124. [Google Scholar] [CrossRef]
- Stepurko, T.; Pavlova, M.; Gryga, I.; Murauskiene, L.; Groot, W. Informal Payments for Health Care Services: The Case of Lithuania, Poland and Ukraine. J. Eurasian Stud. 2015, 6, 46–58. [Google Scholar] [CrossRef]
- Lewis, M.; Pettersson, G. Governance in Health Care Delivery: Raising Performance; World Bank Institute Working Paper No. 5074; World Bank: Washington, DC, USA, 2009. [Google Scholar]
- Tomini, S.M.; Groot, W. Paying Informally for Public Health Care in Albania: Scarce Resources or Governance Failure? Appl. Econ. 2013, 45, 5119–5130. [Google Scholar] [CrossRef]
- Kankeu, H.T.; Ventelou, B. Socioeconomic Inequalities in Informal Payments for Health Care: An Assessment of the ‘Robin Hood’ Hypothesis in 33 African Countries. Soc. Sci. Med. 2016, 151, 173–186. [Google Scholar] [CrossRef]
- Stringhini, S.; Thomas, S.; Bidwell, P.; Mtui, T.; Mwisongo, A. Understanding Informal Payments in Health care: Motivation of Health Workers in Tanzania. Hum. Resour. Health 2009, 7, 53. [Google Scholar] [CrossRef]
- Balabanova, D.; McKee, M. Understanding Informal Payments for Health Care: The Example of Bulgaria. Health Policy 2002, 62, 243–273. [Google Scholar] [CrossRef]
- Correia, T.; Dussault, G.; Pontes, C. The Impact of the Financial Crisis on Human Resources for Health Policies in Three Southern-Europe Countries. Health Policy 2015, 119, 1600–1605. [Google Scholar] [CrossRef]
- Kerasidou, A.; Kingori, P.; Legido-Quigley, H. “You Have to Keep Fighting”: Maintaining Healthcare Services and Professionalism on the Frontline of Austerity in Greece. Int. J. Equity Health 2016, 15, 118. [Google Scholar] [CrossRef]
- Kolasa, K.; Kowalczyk, M. Does Cost Sharing Do More Harm or More Good?—A Systematic Literature Review. BMC Public Health 2016, 16, 992. [Google Scholar] [CrossRef]
- Baji, P.; Pavlova, M.; Gulácsi, L.; Zsófia, H.C.; Groot, W. Informal Payments for Healthcare Services and Short-Term Effects of the Introduction of Visit Fee on These Payments in Hungary. Int. J. Health Plan. Manag. 2012, 27, 63–79. [Google Scholar] [CrossRef]
- Lewis, M. Informal Payments and the Financing of Health Care in Developing and Transition Countries. Health Aff. 2007, 26, 984–997. [Google Scholar] [CrossRef]
- WHO. State of the World’s Nursing 2020: Investing in Education, Jobs and Leadership; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Botezat, A.; Ramos, R. Physicians’ Brain Drain—A Gravity Model of Migration Flows. Glob. Health 2020, 16, 7. [Google Scholar] [CrossRef]
- Scheffler, R.M.; Cometto, G.; Tulenko, K.; Bruckner, T.; Liu, J.; Keuffel, E.L. Health Workforce Requirements for Universal Health Coverageand the Sustainable Development Goals. In Human Resources for Health Observer; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Piroozi, B.; Rashidian, A.; Moradi, G.; Takian, A.; Ghasri, H.; Ghadimi, T. Out-of Pocket and Informal Payment before and after the Health Transformation Plan in Iran: Evidence from Hospitals Located in Kurdistan, Iran. Int. J. Health Policy Manag. 2017, 6, 573–586. [Google Scholar] [CrossRef]
- Habibov, N.; Cheung, A. Revisiting Informal Payments in 29 Transitional Countries: The Scale and Socio-Economic Correlates. Soc. Sci. Med. 2017, 178, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Nekoeimoghadam, M.; Esfandiari, A.; Ramezani, F.; Amiresmaili, M. Informal Payments in Healthcare: A Case Study of Kerman Province in Iran. Int. J. Health Policy Manag. 2013, 1, 157–162. [Google Scholar] [CrossRef]
- Najar, A.V.; Ebrahimipour, H.; Pourtaleb, A.; Esmaily, H.; Jafari, M.; Nejatzadegan, Z.; Taleghani, Y.M. At First Glance, Informal Payments Experience on Track: Why Accept or Refuse? BMC Health Serv. Res. 2017, 17, 205. [Google Scholar]
- Stepurko, T.; Pavlova, M.; Gryga, I.; Groot, W. Informal Payments for Health Care Services—Corruption or Gratitude? A Study on Public Attitudes, Perceptions and Opinions in Six Central and Eastern European Countries. Communist Post-Communist Stud. 2013, 46, 419–431. [Google Scholar] [CrossRef]
- Evans, R. Unhealthy Markets: Financial Crisis, Fiscal Crisis… Health Care Crisis? J. Health Serv. Res. Policy 2009, 14, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, D.; Kraay, A.; Mastruzzi, M. The Worldwide Governance Indicators: Methodology and Analytical Issues. World Bank Policy Research Working Paper 5430. 2010. Available online: https://openknowledge.worldbank.org/handle/10986/3913 (accessed on 7 September 2021).
- Teorell, J.; Sundström, A.; Holmberg, S.; Rothstein, B.; Alvarado Pachon, N.; Dalli, C.M. The Quality of Government Standard Dataset, Version Jan21; University of Gothenburg, The Quality of Government Institute: Gothenburg, Sweden, 2021; Available online: http://www.qog.pol.gu.se (accessed on 2 June 2021). [CrossRef]
- Cruz-García, P.; Peiró-Palomino, J. Informal, Formal Institutions and Credit: Complements or Substitutes? J. Inst. Econ. 2019, 15, 649–671. [Google Scholar] [CrossRef]
- Williams, C.C.; Horodnic, I.A. Evaluating the Illegal Employer Practice of Under-Reporting Employees’ Salaries. Br. J. Ind. Relat. 2017, 55, 83–111. [Google Scholar] [CrossRef]
- Horodnic, I.A. Tax Morale and Institutional Theory: A Systematic Review. Int. J. Sociol. Soc. Policy 2018, 38, 868–886. [Google Scholar] [CrossRef]
- Greene, W.H. Econometric Analysis; Econometric Software: Upper Saddle River, NJ, USA, 2000. [Google Scholar]
- Wooldridge, J.M. Econometric Analysis of cross Section and Panel Data; MIT Press: Cambridge, MA, USA, 2002. [Google Scholar]
- Williams, C.C.; Horodnic, I.A. Extent and Distribution of Unregistered Employment in the Service Industries in Europe. Serv. Ind. J. 2018, 38, 645–649. [Google Scholar] [CrossRef]
- Horodnic, I.A.; Williams, C.C.; Manolica, A.; Roman, C.T.; Boldureanu, G. Employer Perspectives on Undeclared Work in the Service Sector: Impacts and Policy Responses. Serv. Ind. J. 2020. [Google Scholar] [CrossRef]
- Horodnic, I.A.; Williams, C.C.; Ianole-Călin, R. Does Higher Cash-in-Hand Income Motivate Young People to Engage in Under-Declared Employment? East. J. Eur. Stud. 2020, 11, 48–69. [Google Scholar]
- Horodnic, A.V.; Mazilu, S.; Oprea, L. Drivers behind Widespread Informal Payments in the Romanian Public Healthcare System: From Tolerance to Corruption to Socio-Economic and Spatial Patterns. Int. J. Health Plan. Manag. 2018, 33, e597–e611. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.C.; Martinez-Perez, A. Evaluating the Cash-In-Hand Consumer Culture in the European Union. J. Contemp. Eur. Stud. 2014, 22, 466–482. [Google Scholar] [CrossRef]
- Williams, C.C.; Horodnic, A.V. Explaining Informal Payments for Health Services in Central and Eastern Europe: An Institutional Asymmetry Perspective. Postcommunist Econ. 2018, 30, 440–458. [Google Scholar] [CrossRef]
- Tobin, J. Estimation of Relationships for Limited Dependent Variables. Econometrica 1958, 26, 24–36. [Google Scholar] [CrossRef]
- Honoré, B.E. Orthogonality Conditions for Tobit Models with Fixed Effects and Lagged Dependent Variables. J. Econom. 1993, 59, 35–61. [Google Scholar] [CrossRef]
- Papke, L.; Wooldridge, J. Econometric Methods for Fractional Response Variables with an Application to 401(k) Plan Participation Rates. J. Appl. Econ. 1996, 11, 619–632. [Google Scholar] [CrossRef]
- Papke, L.; Wooldridge, J. Panel Data Methods for Fractional Response Variables with an Application to Test Pass Rates. J. Econom. 2008, 145, 121–133. [Google Scholar] [CrossRef]
- Khodamoradi, A.; Rashidian, A.; Aghlmand, S.; Arab, M. Informal Payments and Its Related Factors in Urmia Hospitals. Hakim. Res. J. 2015, 17, 313–321. [Google Scholar]
- Meskarpour-Amiri, M.; Arani, A.A.; Sadeghi, H.; Agheli-Kohnehshahri, L. Socioeconomic Factors Affecting Informal Payments in the Health Sector. Transylv. Rev. Adm. Sci. 2016, 47, 116–128. [Google Scholar]
- Lewis, M. Governance and Corruption in Public Health Care Systems; Working Paper No. 78; Center for Global Development: Washington, DC, USA, 2006. [Google Scholar]
- Werner, D.; Sanders, D.; Weston, J. Questioning the Solution: The Politics of Primary Health Care and Child Survival with an In-Depth Critique of Oral Rehydration Therapy; HealthWrights: Palo Alto, CA, USA, 1997. [Google Scholar]
- Ensor, T.; Witter, S. Health Economics in Low Income Countries: Adapting to the Reality of the Unofficial Economy. Health Policy 2001, 57, 1–13. [Google Scholar] [CrossRef]
- Zandian, H.; Esfandiari, A.; Sakha, M.; Takian, A. Strategies to Reduce Informal Payments in Health Systems: A Systematic Review. East. Mediterr. Health J. 2019, 25, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Tomini, S.; Maarse, H. How Do Patient Characteristics Influence Informal Payments for Inpatient and Outpatient Health Care in Albania: Results of Logit and OLS Models Using Albanian LSMS 2005. BMC Public Health 2011, 11, 375. [Google Scholar] [CrossRef] [PubMed]
- Huntington, A.; Gilmour, J.; Tuckett, A.; Neville, S.; Wilson, D.; Turner, C. Is Anybody Listening? A Qualitative Study of Nurses’ Reflections on Practice. J. Clin. Nurs. 2012, 20, 1413–1422. [Google Scholar] [CrossRef] [PubMed]
- Rechel, B.; McKee, M. Health Reform in Central and Eastern Europe and the Former Soviet Union. Lancet 2009, 374, 1186–1195. [Google Scholar] [CrossRef]
- Humphries, N.; Mcaleese, S.; Matthews, A.; Brugha, R. ‘Emigration Is a Matter of Self-Preservation. The working Conditions Are Killing Us Slowly’: Qualitative Insights into Health Professional Emigration from Ireland. Hum. Resour. Health 2015, 13, 35. [Google Scholar] [CrossRef]
- Benson, A. Labor Market Trends among Registered Nurses: 2008–2011. Policy Polit. Nurs. Pract. 2012, 13, 205–213. [Google Scholar] [CrossRef] [PubMed]
- IRC. COVID19 and the International Supply of Nurses; International Council of Nurses: Geneva, Switzerland, 2020. [Google Scholar]
- Russo, G.; Silva, T.J.; Gassasse, Z.; Filippon, J.; Rotulo, A.; Kondilis, E. The Impact of Economic Recessions on Health Workers: A Systematic Review and Best-Fit Framework Synthesis of the Evidence from the Last 50 Years. Health Policy Plan 2021, 36, 542–551. [Google Scholar] [CrossRef]
- Liu, N.; Bao, G.; He, A.J. Does Health Insurance Coverage Reduce Informal Payments? Evidence from the “Red Envelopes” in China. BMC Health Serv. Res. 2020, 20, 95. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.C.; Horodnic, A.V. Informal Payments in the Health Services Sector: Prevalence and Determinants. Serv. Ind. J. 2018, 38, 841–855. [Google Scholar]
- Institute for Health Metrics and Evaluation (IHME). Global Educational Attainment 1970–2015; Institute for Health Metrics and Evaluation (IHME): Seattle, WA, USA, 2015. [Google Scholar]
- Feenstra, R.C.; Inklaar, R.; Timmer, M.P. The Next Generation of the Penn World Table. Am. Econ. Rev. 2015, 105, 3150–3182. [Google Scholar] [CrossRef]


| Two-Way Fixed Effects | Tobit | Fractional Probit | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | |
| Log of Education | −2.235 | −2.518 | −2.915 | −2.636 | −2.540 | 4.992 | −7.302 | −0.0183 | −0.0542 |
| (4.709) | (4.822) | (4.875) | (4.975) | (4.528) | (5.431) | (4.653) | (0.0337) | (0.142) | |
| Log of Age dependency | −1.282 | −1.543 | −1.596 | −1.511 | −1.569 | −2.169 | −2.402 | −0.0604 | −0.417 * |
| (1.964) | (1.911) | (1.912) | (1.951) | (2.177) | (1.980) | (1.905) | (0.0581) | (0.249) | |
| Log of Employment | 2.546 ** | 3.001 ** | 2.977 ** | 3.006 ** | 3.059 ** | 3.280 *** | 2.814 ** | −0.0231 | −0.256 |
| (1.280) | (1.225) | (1.214) | (1.229) | (1.171) | (1.240) | (1.138) | (0.0484) | (0.216) | |
| Life expectancy | 0.142 * | 0.142 ** | 0.147 * | 0.144 * | 0.142 * | 0.192 * | 0.142 ** | −0.00522 ** | −0.0299 *** |
| (0.0762) | (0.0687) | (0.0757) | (0.0764) | (0.0755) | (0.0991) | (0.0716) | (0.00233) | (0.0112) | |
| Log of Health expenditures | −0.255 | −0.180 | −0.203 | −0.0756 | −0.0730 | 1.134 * | −0.245 | 0.0279 | 0.127 |
| (0.418) | (0.404) | (0.424) | (0.494) | (0.514) | (0.627) | (0.416) | (0.0252) | (0.105) | |
| Log of Out-of-pocket expenditure | −0.660 ** | −0.704 ** | |||||||
| (0.287) | (0.272) | ||||||||
| Quality of governance | −0.978 * | −1.010 * | −1.024 * | −1.036 * | −0.499 | −0.947 * | −0.0608 *** | −0.324 *** | |
| (0.550) | (0.554) | (0.563) | (0.535) | (0.631) | (0.529) | (0.0182) | (0.0839) | ||
| Log of Private health expenditure | −0.643 ** | −0.696 ** | −0.685 ** | −1.126 ** | −0.574 * | −0.0153 | −0.0425 | ||
| (0.297) | (0.314) | (0.298) | (0.445) | (0.295) | (0.0178) | (0.0651) | |||
| GDP per capita growth | −0.00353 | ||||||||
| (0.00613) | |||||||||
| Log of GDP per capita | −0.0595 | ||||||||
| (0.699) | |||||||||
| Log of Doctors ratio | −0.257 | ||||||||
| (0.228) | |||||||||
| Urban | 0.118 * | ||||||||
| (0.0652) | |||||||||
| Obs./Countries | 353/117 | 353/117 | 353/117 | 345/113 | 345/113 | 263/97 | 353/117 | 354/117 | 354/117 |
| R-squared | 0.223 | 0.233 | 0.230 | 0.231 | 0.230 | 0.306 | 0.240 | - | - |
| BIC | 525.3 | 526.4 | 528.1 | 529.3 | 529.6 | 366.5 | 529.2 | −663.7 | - |
| OLS | Tobit | Fractional Probit | |||||||
|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | |
| Log of Education | 0.540 * | 0.563 | 0.478 | 0.833 | 0.901 * | 0.831 | 0.991 | 0.184 *** | 1.040 *** |
| (0.290) | (0.652) | (0.515) | (0.604) | (0.449) | (0.749) | (0.690) | (0.0608) | (0.306) | |
| Log of age dependency | −0.955 ** | 0.217 | −0.886 | 0.0143 | −0.334 | −0.0428 | 0.174 | −0.0315 | 0.191 |
| (0.474) | (0.962) | (0.770) | (0.975) | (0.710) | (1.241) | (1.209) | (0.0979) | (0.503) | |
| Log of employment | −1.666 *** | −1.481 * | −2.353 *** | −1.513 * | −1.891 *** | −1.997 * | −1.830 | −0.280 ** | −1.554 *** |
| (0.418) | (0.783) | (0.534) | (0.759) | (0.521) | (1.127) | (1.160) | (0.108) | (0.489) | |
| Life expectancy | −0.0510 *** | −0.0857 | −0.0442 | −0.0619 | 0.0140 | 0.0110 | 0.0208 | −0.00300 | 0.0238 |
| (0.0184) | (0.0660) | (0.0288) | (0.0604) | (0.0318) | (0.105) | (0.102) | (0.00856) | (0.0469) | |
| Log of Health expenditure | −0.0272 | −0.0786 | −0.0530 | −0.0594 | −0.0390 | −0.0348 | −0.0379 | −0.00811 | −0.0886 * |
| (0.0399) | (0.0688) | (0.0715) | (0.0633) | (0.0613) | (0.108) | (0.108) | (0.00653) | (0.0474) | |
| Log of Private health expenditure | −0.00742 | 0.0139 | −0.609 | −0.0243 | −0.491 | −0.886 | −0.807 | −0.0673 | −0.293 |
| (0.151) | (0.291) | (0.385) | (0.291) | (0.392) | (0.532) | (0.487) | (0.0404) | (0.192) | |
| Quality of governance | −0.646 *** | −0.842 *** | −0.950 *** | −0.805 | −0.0647 * | −0.404 ** | |||
| (0.186) | (0.298) | (0.337) | (0.500) | (0.0359) | (0.172) | ||||
| Feel personally obliged to report corruption | −0.0161 ** | −0.0108 | −0.0219 * | −0.0166 | −0.000390 | −0.00486 | |||
| (0.00775) | (0.00838) | (0.0118) | (0.0144) | (0.00121) | (0.00545) | ||||
| Trust | −0.0140 | −0.0103 | −0.0378 ** | −0.0324 * | −0.000807 | −0.00511 | |||
| (0.0131) | (0.0114) | (0.0168) | (0.0176) | (0.00124) | (0.00770) | ||||
| Observations | 113 | 63 | 42 | 63 | 42 | 28 | 28 | 29 | 29 |
| BIC | 296.6 | 178.0 | 118.9 | 173.5 | 114.2 | 85.46 | 85.45 | −37.88 | 57.91 |
| R-squared | 0.584 | 0.539 | 0.583 | 0.598 | 0.659 | 0.649 | 0.689 | - | - |
| Hypothesis | Result | ||
|---|---|---|---|
| Formal Institutions | H1. Quality of Governance: Informal payments in health are more likely to occur with ill-functioning formal institutions. | Confirmed | Significant negative impact of quality of governance on informal payments. |
| H2. Resource allocation: Higher shares of financial resources/private financing reduce informal payments in health. | Partially confirmed | ||
| H2a. The higher the share of health resources, the lower the prevalence of informal payments in health. | Not confirmed | Unsignificant impact of the share of health expenditures on informal payments in health. | |
| H2b. The higher the share of private financing, the lower the prevalence of informal payments in health. | Confirmed | Significant negative impact of out-of-pocket and domestic private health expenditure on informal payments in health. | |
| H3. Healthcare accessibility: higher accessibility rates reduce informal payments in health. | Not confirmed | Unsignificant impact of the ratio of physicians (per 10,000 inhabitants) on informal payments in health. | |
| Informal Institutions | H4. Patient’s norms and values: Informal payments in health are more likely to occur with ‘bad’ informal institutions. | Confirmed | Significant negative impact of trust, and feel personally obliged to report corruption on informal payments in health. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Incaltarau, C.; Horodnic, A.V.; Williams, C.C.; Oprea, L. Institutional Determinants of Informal Payments for Health Services: An Exploratory Analysis across 117 Countries. Int. J. Environ. Res. Public Health 2021, 18, 12421. https://doi.org/10.3390/ijerph182312421
Incaltarau C, Horodnic AV, Williams CC, Oprea L. Institutional Determinants of Informal Payments for Health Services: An Exploratory Analysis across 117 Countries. International Journal of Environmental Research and Public Health. 2021; 18(23):12421. https://doi.org/10.3390/ijerph182312421
Chicago/Turabian StyleIncaltarau, Cristian, Adrian V. Horodnic, Colin C. Williams, and Liviu Oprea. 2021. "Institutional Determinants of Informal Payments for Health Services: An Exploratory Analysis across 117 Countries" International Journal of Environmental Research and Public Health 18, no. 23: 12421. https://doi.org/10.3390/ijerph182312421
APA StyleIncaltarau, C., Horodnic, A. V., Williams, C. C., & Oprea, L. (2021). Institutional Determinants of Informal Payments for Health Services: An Exploratory Analysis across 117 Countries. International Journal of Environmental Research and Public Health, 18(23), 12421. https://doi.org/10.3390/ijerph182312421