
Decreased Emotional Dysregulation Following Multi-Modal Motion-Assisted Memory Desensitization and Reconsolidation Therapy (3MDR): Identifying Possible Driving Factors in Remediation of Treatment-Resistant PTSD

 ,
,  , , and
, , and 
Abstract
:1. Introduction
1.1. 3MDR Intervention
1.2. Emotional Regulation and Dysregulation
2. Materials and Methods
2.1. Study Design
2.2. Sample Eligibility and Size
2.3. Inclusion and Exclusion Criteria
2.4. Recruitment and Setting
2.5. Questionnaire
2.6. Data Collection
2.7. Data Analysis
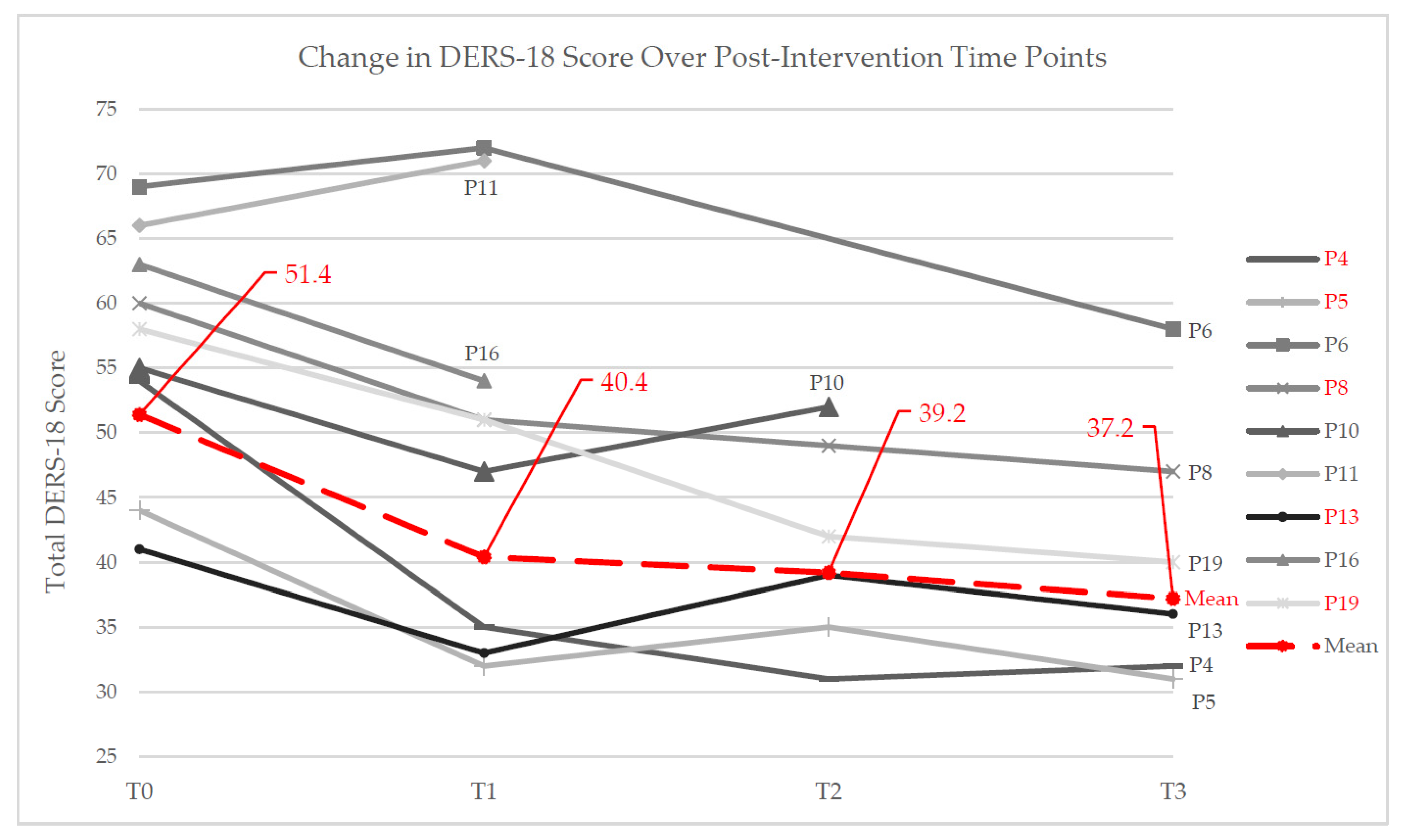
3. Results
3.1. DERS-18 Score 1 Week Postintervention (T0 vs. T1)
3.2. DERS-18 Score 1 Month Postintervention (T0 vs. T2)
3.3. DERS-18 Score 3 Month Postintervention (T0 vs. T3)
3.4. Qualitative Changes in Participant Emotional Regulation
4. Discussion
4.1. Cognitive–Motor Stimulation
4.2. Eye Movement Bilateral Stimulation
4.3. Comprehensive Treatment Addressing Emotional Regulation
4.4. Future Research
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Currier, J.M.; Holland, J.M.; Drescher, K.D. Residential treatment for combat-related posttraumatic stress disorder: Identifying trajectories of change and predictors of treatment response. PLoS ONE 2014, 9, e101741. [Google Scholar] [CrossRef]
- Zamorski, M.A.; Bennett, R.E.; Rusu, C.; Weeks, M.; Boulos, D.; Garber, B.G. Prevalence of Past-Year Mental Disorders in the Canadian Armed Forces, 2002–2013. Can. J. Psychiatry 2016, 61, 26S–35S. [Google Scholar] [CrossRef] [Green Version]
- Boulos, D.; Zamorski, M.A. Military Occupational Outcomes in Canadian Armed Forces Personnel with and without Deployment-Related Mental Disorders. Can. J. Psychiatry 2016, 61, 348–357. [Google Scholar] [CrossRef] [Green Version]
- Vermetten, E.; Ambaum, J. Exposure to combat and deployment; reviewing the military context in The Netherlands. Int. Rev. Psychiatry 2019, 31, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Bryant, R.A. Post-traumatic stress disorder: A state-of-the-art review of evidence and challenges. World Psychiatry 2019, 18, 259–269. [Google Scholar] [CrossRef] [Green Version]
- Vermetten, E.; Jetly, R. A Critical Outlook on Combat-Related PTSD: Review and Case Reports of Guilt and Shame as Drivers for Moral Injury. Mil. Behav. Health 2018, 6, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Nazarov, A.; Fikretoglu, D.; Liu, A.; Richardson, J.D.; Thompson, M. Help-seeking for mental health issues in deployed Canadian Armed Forces personnel at risk for moral injury. Eur. J. Psychotraumatol. 2020, 11, 1729032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijdam, M.J.; Vermetten, E. Moving forward in treatment of posttraumatic stress disorder: Innovations to exposure-based therapy. Eur. J. Psychotraumatol. 2018, 9, 1458568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gelderen, M.J.; Nijdam, M.J.; Vermetten, E. An Innovative Framework for Delivering Psychotherapy to Patients with Treatment-Resistant Posttraumatic Stress Disorder: Rationale for Interactive Motion-Assisted Therapy. Front. Psychiatry 2018, 9, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gelderen, M.J.; Nijdam, M.J.; Haagen, J.F.; Vermetten, E. Interactive Motion-Assisted Exposure Therapy for Veterans with Treatment-Resistant Posttraumatic Stress Disorder: A Randomized Controlled Trial. Psychother. Psychosom. 2020, 89, 215–227. [Google Scholar] [CrossRef]
- Vermetten, E.; Meijer, L.; van der Wurff, P.; Mert, A. The effect of military motion-assisted memory desensitization and reprocessing treatment on the symptoms of combat- related post traumatic stress disorder: First preliminary results. Annu. Rev. Cyberther. Telemed. 2013, 11, 125–128. [Google Scholar]
- Seidler, G.H.; Wagner, F.E. Comparing the efficacy of EMDR and trauma-focused cognitive-behavioral therapy in the treatment of PTSD: A meta-analytic study. Psychol. Med. 2006, 36, 1515–1522. [Google Scholar] [CrossRef]
- Bisson, J.; Van Deursen, R.; Hannigan, B.; Kitchiner, N.; Barawi, K.; Jones, K.; Pickles, T.; Skipper, J.; Young, C.; Abbott, L.; et al. Randomized controlled trial of multi-modular motion-assisted memory desensitization and reconsolidation (3MDR) for male military veterans with treatment-resistant post-traumatic stress disorder. Acta Psychiatr. Scand. 2020, 142, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Smith-MacDonald, L.; Miguel-Cruz, A.; Pike, A.; van Gelderen, M.; Lentz, L.; Shiu, M.Y.; Tang, E.; Sawalha, J.; Greenshaw, A.; et al. Virtual Reality–Based Treatment for Military Members and Veterans with Combat-Related Posttraumatic Stress Disorder: Protocol for a Multimodular Motion-Assisted Memory Desensitization and Reconsolidation Randomized Controlled Trial. JMIR Res. Protoc. 2020, 9, e20620. [Google Scholar] [CrossRef]
- Witte, K. Putting the fear back into fear appeals: The extended parallel process model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Gross, J.J. The Extended Process Model of Emotion Regulation: Elaborations, Applications, and Future Directions. Psychol. Inq. 2015, 26, 130–137. [Google Scholar] [CrossRef]
- Lanius, R.A.; Frewen, P.A.; Vermetten, E.; Yehuda, R. Fear conditioning and early life vulnerabilities: Two distinct pathways of emotional dysregulation and brain dysfunction in PTSD. Eur. J. Psychotraumatol. 2010, 1, 5467. [Google Scholar] [CrossRef] [PubMed]
- Yehuda, R.; Hoge, C.W.; McFarlane, A.C.; Vermetten, E.; Lanius, R.A.; Nievergelt, C.M.; Hobfoll, S.E.; Koenen, K.C.; Neylan, T.C.; Hyman, S.E. Post-traumatic stress disorder. Nat. Rev. Dis. Prim. 2015, 1, 15057. [Google Scholar] [CrossRef]
- Raudales, A.M.; Preston, T.J.; Albanese, B.J.; Schmidt, N.B. Emotion dysregulation as a maintenance factor for posttraumatic stress symptoms: The role of anxiety sensitivity. J. Clin. Psychol. 2020, 76, 2183–2197. [Google Scholar] [CrossRef] [PubMed]
- Spies, J.P.; Cwik, J.C.; Willmund, G.D.; Knaevelsrud, C.; Schumacher, S.; Niemeyer, H.; Engel, S.; Küster, A.; Muschalla, B.; Köhler, K.; et al. Associations Between Difficulties in Emotion Regulation and Post-Traumatic Stress Disorder in Deployed Service Members of the German Armed Forces. Front. Psychiatry 2020, 11, 1–15. [Google Scholar] [CrossRef]
- Christ, N.M.; Elhai, J.D.; Forbes, C.N.; Gratz, K.L.; Tull, M.T. A machine learning approach to modeling PTSD and difficulties in emotion regulation. Psychiatry Res. 2021, 297, 113712. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Lentz, L.; Smith-MacDonald, L.; Miguel-Cruz, A.; Brémault-Phillips, S. Tackling trauma with technology: Treating chronic combat-related PTSD in Canadian Armed Forces personnel and veterans with 3MDR. Annu. Rev. Cyberther. Telemed. 2021, 18, 235–239. [Google Scholar]
- Jones, C.; Smith-MacDonald, L.; Brown MR, G.; Pike, A.; Vermetten, E.; Brémault-Phillips, S. Quantitative changes in mental health measures with 3MDR treatment for Canadian military members and veterans with treatment-resistant posttraumatic stress disorder. Brain Behav. 2021. in review. [Google Scholar]
- Cohen, J. A power primer: Quantitative methods in psychology. Psychol. Bull 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Victor, S.E.; Klonsky, E.D. Validation of a Brief Version of the Difficulties in Emotion Regulation Scale (DERS-18) in Five Samples. J. Psychopathol. Behav. Assess. 2016, 38, 582–589. [Google Scholar] [CrossRef]
- Taheri, S.M.; Hesamian, G. A generalization of the Wilcoxon signed-rank test and its applications. Stat. Pap. 2013, 54, 457–470. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Nursing Research: Generating and Assessing Evidence for Nursing Practice; Wolters Kluwer, Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Neergaard, M.A.; Olesen, F.; Andersen, R.S.; Sondergaard, J. Qualitative description—The poor cousin of health research? BMC Med. Res. Methodol. 2009, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Schoonenboom, J.; Johnson, R.B. How to Construct a Mixed Methods Research Design. KZfSS Kölner Z. Soziologie Soz. 2017, 69, 107–131. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research; SAGE Publications: Thousand Oaks, CA, USA, 2011; pp. 58–88. [Google Scholar]
- Oppezzo, M.; Schwartz, D.L. Give your ideas some legs: The positive effect of walking on creative thinking. J. Exp. Psychol. Learn. Mem. Cogn. 2014, 40, 1142–1152. [Google Scholar] [CrossRef] [Green Version]
- Pietrzak, T.; Lohr, C.; Jahn, B.; Hauke, G. Embodied cognition and the direct induction of affect as a compliment to cognitive behavioural therapy. Behav. Sci. 2018, 8, 29. [Google Scholar] [CrossRef] [Green Version]
- Guell, X.; Gabrieli, J.D.; Schmahmann, J.D. Embodied cognition and the cerebellum: Perspectives from the Dysmetria of Thought and the Universal Cerebellar Transform theories. Cortex 2018, 100, 140–148. [Google Scholar] [CrossRef]
- Kitayama, S.; Chua, H.F.; Tompson, S.; Han, S. Neural mechanisms of dissonance: An fMRI investigation of choice justification. Neuroimage 2013, 69, 206–212. [Google Scholar] [CrossRef]
- Landin-Romero, R.; Moreno-Alcázar, A.; Pagani, M.; Amann, B.L. How Does Eye Movement Desensitization and Reprocessing Therapy Work? A Systematic Review on Suggested Mechanisms of Action. Front. Psychol. 2018, 9, 1395. [Google Scholar] [CrossRef]
- Herkt, D.; Tumani, V.; Grön, G.; Kammer, T.; Hofmann, A.; Abler, B. Facilitating Access to Emotions: Neural Signature of EMDR Stimulation. PLoS ONE 2014, 9, e106350. [Google Scholar] [CrossRef] [PubMed]
- Giotakos, O. Neurobiology of emotional trauma. Psychiatriki 2020, 31, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Sripada, R.K.; King, A.P.; Garfinkel, S.N.; Wang, X.; Sripada, C.S.; Welsh, R.C.; Liberzon, I. Altered resting-state amygdala functional connectivity in men with posttraumatic stress disorder. J Psychiatry Neurosci. 2012, 37, 241–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, M.A.; Romanski, L.M.; LeDoux, J.E. Extinction of emotional learning: Contribution of medial prefrontal cortex. Neurosci. Lett. 1993, 163, 109–113. [Google Scholar] [CrossRef]
- Milad, M.R.; Quirk, G.J. Neurons in medial prefrontal cortex signal memory for fear extinction. Nature 2002, 420, 70–74. [Google Scholar] [CrossRef]
- Shin, L.M.; Orr, S.P.; Carson, M.A.; Rauch, S.L.; Macklin, M.L.; Lasko, N.B.; Peters, P.M.; Metzger, L.J.; Dougherty, D.D.; Cannistraro, P.A.; et al. Regional cerebral blood flow in the amygdala and medial prefrontal cortex during traumatic imagery in male and female Vietnam veterans with PTSD. Arch. Gen. Psychiatry 2004, 61, 168–176. [Google Scholar] [CrossRef] [Green Version]
- Andrewes, D.G.; Jenkins, L.M. The Role of the Amygdala and the Ventromedial Prefrontal Cortex in Emotional Regulation: Implications for Post-traumatic Stress Disorder. Neuropsychol. Rev. 2019, 29, 220–243. [Google Scholar] [CrossRef]
- Ebneabbasi, A.; Mahdipour, M.; Nejati, V.; Li, M.; Liebe, T.; Colic, L.; Leutritz, A.L.; Vogel, M.; Zarei, M.; Walter, M.; et al. Emotion processing and regulation in major depressive disorder: A 7T resting-state fMRI study. Hum. Brain Mapp. 2021, 42, 797–810. [Google Scholar] [CrossRef] [PubMed]
- Protopopescu, A.; Boyd, J.E.; O’Connor, C.; Rhind, S.; Jetly, R.; Lanius, R.A.; McKinnon, M.C. Moral injury in Canadian military members and Veterans: Implications for military and healthcare sector response during the COVID-19 pandemic. J. Mil. Veteran Fam. Health 2020, 6. [Google Scholar] [CrossRef]


{kind=link}
| Post-Intervention Timepoint | 1 Week | 1 Month | 3 Months | |||
|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T2 | T0 | T3 | |
| Mean | 56.67 | 49.56 | 52.00 | 41.33 | 54.33 | 40.67 |
| df | 8 | 5 | 5 | |||
| p-value | 0.021 | 0.028 | 0.027 | |||
| Z score | −2.314 | −2.201 | −2.207 | |||
| Quotes | |
|---|---|
| Range and layers of emotions addressed by 3MDR | “[I]t’s a complete 180 in perspective, I am no longer focused on trying to deal with anger and whatever. I am focused on the guilt and shame that caused the anger to begin with. I have gotten to an underlying layer of things … helped me realize it was real, to look at it in a different manner. Shift from anger to shame and guilt which is actually what I had to face. And I had never faced it until now.” (P10) |
| Subsection of DERS-18 | |
| Awareness | “I have noticed [positive] differences. Just being more aware of how I feel. And being able to, you know, once I identify it, I’m able to change the way I–what I’m thinking about. And that’s progress for me because that’s always been a tough one … [to shift out of] an intrusive thought or negative state.” (P5)“My emotional range has improved. I don’t avoid stuff anymore, I kind of focus on it, try to deal with it.” (P2)“Being more patient. Knowing my reactions. My triggers. What triggers me off, and what sets me off easier. Noticing little things, I used to get so emotionally upset.” (P3) |
| Clarity | “I don’t think I’ve expanded my vocabulary. I think I’ve just learned to put words to feelings … I’m more connected to my emotions and my feelings and my thoughts.” (P5) |
| Goals | “My focus has improved, concentration has improved. Go to work and do paperwork. I still tire quickly when I have to pay attention to details; it does wear me out, but at least I can do it now. Where before I wouldn’t have been able to … improvement is there but it’s not 100%.” (P2) |
| Impulse | “I’m a lot calmer, I’m allowing things to happen without reacting, with the kids and stuff. Stomp, stomp, pound, smash. I’m not letting it get to me, 90% better. I still get irked. You get that twitch. Even my driving is getting better. [Less] reacting to the morons in front, behind and on the side of me.” (P13) |
| Nonacceptance | “In week three, and again in post-week five, was a little bit less of beating myself up, a little bit of saying ‘it’s okay to take care of yourself, it’s okay to put yourself in front sometimes’.” (P11)“I used to be very ashamed of [my PTSD]. Very … [Now] everybody I know knows that I suffer from it.” (P6) |
| Strategies | “Usually … I try to deal with [negative thoughts and emotions] in a healthy manner. Spend time with my cat or do photography or just do something different” (P5)“[Prior to 3MDR, arguments with wife] would carry on for at least an hour or two. And it would take me 2–3 h to calm down from that. And you know I still get some of those rushes, I guess. But not as bad as they used to be.” (P6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, E.; Jones, C.; Smith-MacDonald, L.; Brown, M.R.G.; Vermetten, E.H.G.J.M.; Brémault-Phillips, S. Decreased Emotional Dysregulation Following Multi-Modal Motion-Assisted Memory Desensitization and Reconsolidation Therapy (3MDR): Identifying Possible Driving Factors in Remediation of Treatment-Resistant PTSD. Int. J. Environ. Res. Public Health 2021, 18, 12243. https://doi.org/10.3390/ijerph182212243
Tang E, Jones C, Smith-MacDonald L, Brown MRG, Vermetten EHGJM, Brémault-Phillips S. Decreased Emotional Dysregulation Following Multi-Modal Motion-Assisted Memory Desensitization and Reconsolidation Therapy (3MDR): Identifying Possible Driving Factors in Remediation of Treatment-Resistant PTSD. International Journal of Environmental Research and Public Health. 2021; 18(22):12243. https://doi.org/10.3390/ijerph182212243
Chicago/Turabian StyleTang, Emily, Chelsea Jones, Lorraine Smith-MacDonald, Matthew R. G. Brown, Eric H. G. J. M. Vermetten, and Suzette Brémault-Phillips. 2021. "Decreased Emotional Dysregulation Following Multi-Modal Motion-Assisted Memory Desensitization and Reconsolidation Therapy (3MDR): Identifying Possible Driving Factors in Remediation of Treatment-Resistant PTSD" International Journal of Environmental Research and Public Health 18, no. 22: 12243. https://doi.org/10.3390/ijerph182212243
APA StyleTang, E., Jones, C., Smith-MacDonald, L., Brown, M. R. G., Vermetten, E. H. G. J. M., & Brémault-Phillips, S. (2021). Decreased Emotional Dysregulation Following Multi-Modal Motion-Assisted Memory Desensitization and Reconsolidation Therapy (3MDR): Identifying Possible Driving Factors in Remediation of Treatment-Resistant PTSD. International Journal of Environmental Research and Public Health, 18(22), 12243. https://doi.org/10.3390/ijerph182212243