
Negative Association between Acrylamide Exposure and Metabolic Syndrome Markers in Adult Population



Abstract
1. Introduction
2. Participants & Methods
2.1. Study Design and Participant Selection
2.2. Measurement of AA and GA
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
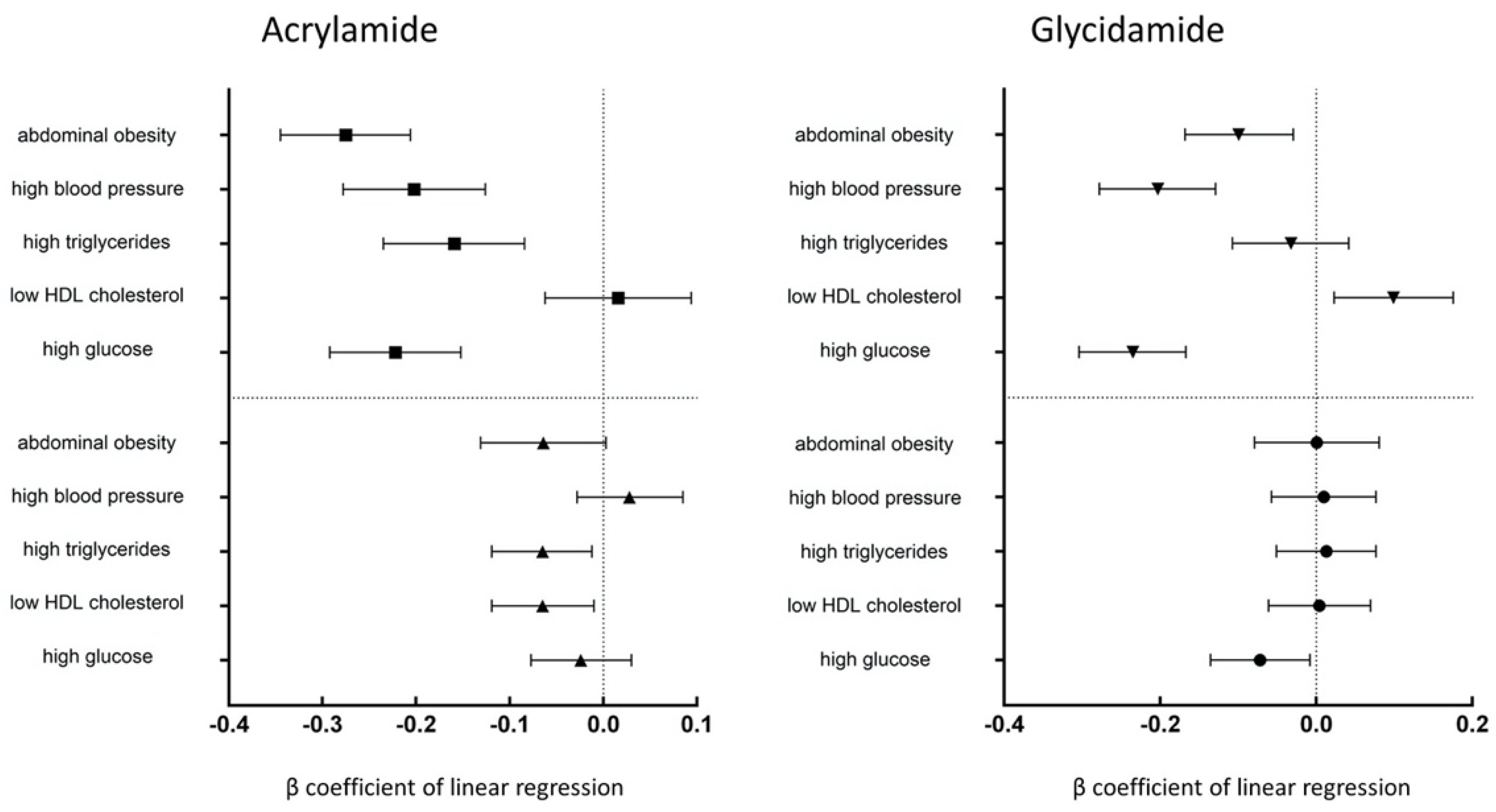
3.2. Correlations between the Concentrations of HbAA and HbGA and the Metabolic Syndrome Markers
4. Discussion
4.1. Acrylamide Exposure and Blood Glucose Regulation
4.2. Acrylamide Exposure and Lipid Metabolism
4.3. Acrylamide Exposure and Bodyweight
4.4. Acrylamide Exposure and Cardiovascular Disease
4.5. Acrylamide Exposure and Inflammation
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Hagmar, L.; Törnqvist, M.; Nordander, C.; Rosén, I.; Bruze, M.; Kautiainen, A.; Magnusson, A.-L.; Malmberg, B.; Aprea, P.; Granath, F.; et al. Health effects of occupational exposure to acrylamide using hemoglobin adducts as biomarkers of internal dose. Scand. J. Work Environ. Health 2001, 27, 219–226. [Google Scholar] [CrossRef]
- Kjuus, H.; Goffeng, L.O.; Heier, M.S.; Sjöholm, H.; Øvrebø, S.; Skaug, V.; Paulsson, B.; Tömqvist, M.; Brudal, S. Effects on the peripheral nervous system of tunnel workers exposed to acrylamide and N-methylolacrylamide. Scand. J. Work Environ. Health 2004, 30, 21–29. [Google Scholar] [CrossRef]
- Reynolds, T. Acrylamide and Cancer: Tunnel Leak in Sweden Prompted Studies. JNCI J. Natl. Cancer Inst. 2002, 94, 876–878. [Google Scholar] [CrossRef] [PubMed]
- FAO/WHO. Consultation on Health Implications of Acrylamide in Food. In Health Implications of Acrylamide in Food: Report of a Joint FAO/WHO Consultation; WHO Headquarters: Geneva, Switzerland, 2002. [Google Scholar]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Acrylamide. In The IARC Monographs Identify Environmental Factors That Are Carcinogenic Hazards to Humans; International Agency for Research on Cancer: Lyon, France, 1994; Volume 60, pp. 389–433. [Google Scholar]
- Schmidt, R.E.; Plurad, S.B.; Clark, H.B. Acrylamide-induced sympathetic autonomic neuropathy resulting in pineal denervation. Lab. Investig. 1987, 56, 505–517. [Google Scholar] [PubMed]
- Tyl, R.W.; Friedman, M.A. Effects of acrylamide on rodent reproductive performance. Reprod. Toxicol. 2003, 17, 1–13. [Google Scholar] [CrossRef]
- Friedman, M. Chemistry, biochemistry, and safety of acrylamide. A review. J. Agric. Food Chem. 2003, 51, 4504–4526. [Google Scholar] [CrossRef]
- Lee, T.; Manjanatha, M.G.; Aidoo, A.; Moland, C.L.; Branham, W.S.; Fuscoe, J.C.; Ali, A.A.; Desai, V.G. Expression Analysis of Hepatic Mitochondria-Related Genes in Mice Exposed to Acrylamide and Glycidamide. J. Toxicol. Environ. Health Part A 2012, 75, 324–339. [Google Scholar] [CrossRef]
- McCracken, E.; Monaghan, M.; Sreenivasan, S. Pathophysiology of the metabolic syndrome. Clin. Derm. 2018, 36, 14–20. [Google Scholar] [CrossRef]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the Metabolic Syndrome. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C.; et al. Diagnosis and Management of the Metabolic Syndrome. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Shim, Y.H.; Ock, J.W.; Kim, Y.-J.; Kim, Y.; Kim, S.Y.; Kang, D. Association between Heavy Metals, Bisphenol A, Volatile Organic Compounds and Phthalates and Metabolic Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 671. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lin, Y.C.; Kuo, H.K.; Hwang, J.J.; Lin, J.L.; Chen, P.C.; Lin, L.Y. Association among acrylamide, blood insulin, and insulin resistance in adults. Diabetes Care 2009, 32, 2206–2211. [Google Scholar] [CrossRef]
- Wang, B.; Qiu, W.; Yang, S.; Cao, L.; Zhu, C.; Ma, J.; Li, W.; Zhang, Z.; Xu, T.; Wang, X.; et al. Acrylamide Exposure and Oxidative DNA Damage, Lipid Peroxidation, and Fasting Plasma Glucose Alteration: Association and Mediation Analyses in Chinese Urban Adults. Diabetes Care 2020, 43, 1479–1486. [Google Scholar] [CrossRef]
- Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [CrossRef] [PubMed]
- Rönnemaa, T.; Rönnemaa, E.M.; Puukka, P.; Pyörälä, K.; Laakso, M. Smoking Is Independently Associated with High Plasma Insulin Levels in Nondiabetic Men. Diabetes Care 1996, 19, 1229. [Google Scholar] [CrossRef]
- Yue, Z.; Chen, Y.; Song, Y.; Zhang, J.; Yang, X.; Wang, J.; Li, L.; Sun, Z. Effect of acrylamide on glucose homeostasis in female rats and its mechanisms. Food Chem. Toxicol. 2020, 135, 110894. [Google Scholar] [CrossRef]
- Totani, N.; Yawata, M.; Ojiri, Y.; Fujioka, Y. Effects of trace acrylamide intake in Wistar rats. J. Oleo Sci. 2007, 56, 501–506. [Google Scholar] [CrossRef][Green Version]
- Bodin, J.; Stene, L.C.; Nygaard, U.C. Can Exposure to Environmental Chemicals Increase the Risk of Diabetes Type 1 Development? BioMed Res. Int. 2015, 2015, 208947. [Google Scholar] [CrossRef]
- Howard, S.G. Developmental Exposure to Endocrine Disrupting Chemicals and Type 1 Diabetes Mellitus. Front. Endocrinol. 2018, 9, 513. [Google Scholar] [CrossRef]
- Howard, S.G. Exposure to environmental chemicals and type 1 diabetes: An update. J. Epidemiol. Community Health 2019, 73, 483. [Google Scholar] [CrossRef] [PubMed]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Reamy, B.V. Dyslipidemias. In CURRENT Diagnosis & Treatment: Family Medicine, 5th ed.; South-Paul, J.E., Matheny, S.C., Lewis, E.L., Eds.; McGraw Hill: New York, NY, USA, 2020. [Google Scholar]
- Lee, H.-W.; Pyo, S. Acrylamide induces adipocyte differentiation and obesity in mice. Chem.-Biol. Interact. 2019, 298, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Alves-Bezerra, M.; Cohen, D.E. Triglyceride Metabolism in the Liver. Compr. Physiol. 2017, 8, 1–8. [Google Scholar] [CrossRef]
- Kim, S.M.; Baek, J.M.; Lim, S.M.; Kim, J.Y.; Kim, J.; Choi, I.; Cho, K.H. Modified Lipoproteins by Acrylamide Showed More Atherogenic Properties and Exposure of Acrylamide Induces Acute Hyperlipidemia and Fatty Liver Changes in Zebrafish. Cardiovasc. Toxicol. 2015, 15, 300–308. [Google Scholar] [CrossRef]
- El-Sayyad, H.I.; Abou-Egla, M.H.; El-Sayyad, F.I.; El-Ghawet, H.A.; Gaur, R.L.; Fernando, A.; Raj, M.H.G.; Ouhtit, A. Effects of fried potato chip supplementation on mouse pregnancy and fetal development. Nutrition 2011, 27, 343–350. [Google Scholar] [CrossRef]
- Vesper, H.W.; Slimani, N.; Hallmans, G.; Tjønneland, A.; Agudo, A.; Benetou, V.; Bingham, S.; Boeing, H.; Boutron-Ruault, M.-C.; Bueno-de-Mesquita, H.B.; et al. Cross-Sectional Study on Acrylamide Hemoglobin Adducts in Subpopulations from the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. J. Agric. Food Chem. 2008, 56, 6046–6053. [Google Scholar] [CrossRef]
- Ellberg, C.; Olsson, H.; Jernström, H. Current smoking is associated with a larger waist circumference and a more androgenic profile in young healthy women from high-risk breast cancer families. Cancer Causes Control 2018, 29, 243–251. [Google Scholar] [CrossRef]
- Swamy, M.V.; Subbaiah, K.; Suman, B.; Kamala, K.; Rao, K.J.; Raju, K.T. Toxic effect of acrylamide on body weight, antioxidants and histoarchitecture of heart in the developing chick embryo. Indian J. Appl. Res. 2013, 3, 27–30. [Google Scholar] [CrossRef]
- Pedersen, M.; von Stedingk, H.; Botsivali, M.; Agramunt, S.; Alexander, J.; Brunborg, G.; Chatzi, L.; Fleming, S.; Fthenou, E.; Granum, B.; et al. Birth weight, head circumference, and prenatal exposure to acrylamide from maternal diet: The European prospective mother-child study (NewGeneris). Environ. Health Perspect. 2012, 120, 1739–1745. [Google Scholar] [CrossRef]
- European Food Safety, A. Results on acrylamide levels in food from monitoring years 2007–2009 and Exposure assessment. EFSA J. 2011, 9, 2133. [Google Scholar] [CrossRef]
- Chu, P.L.; Lin, L.Y.; Chen, P.C.; Su, T.C.; Lin, C.Y. Negative association between acrylamide exposure and body composition in adults: NHANES, 2003–2004. Nutr. Diabetes 2017, 7, e246. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Huang, M.; Zhuang, P.; Jiao, J.; Chen, X.; Wang, J.; Wu, Y. Exposure to acrylamide and the risk of cardiovascular diseases in the National Health and Nutrition Examination Survey 2003–2006. Environ. Int. 2018, 117, 154–163. [Google Scholar] [CrossRef]
- Callera, G.E.; Montezano, A.C.; Yogi, A.; Tostes, R.C.; Touyz, R.M. Vascular signaling through cholesterol-rich domains: Implications in hypertension. Curr. Opin. Nephrol. Hypertens. 2007, 16, 90–104. [Google Scholar] [CrossRef] [PubMed]
- Kotchen, T.A. Hypertensive Vascular Disease. In Harrison’s Principles of Internal Medicine, 20th ed.; Jameson, J.L., Fauci, A.S., Kasper, D.L., Hauser, S.L., Longo, D.L., Loscalzo, J., Eds.; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Lai, S.-M.; Gu, Z.-T.; Zhao, M.-M.; Li, X.-X.; Ma, Y.-X.; Luo, L.; Liu, J. Toxic effect of acrylamide on the development of hippocampal neurons of weaning rats. Neural. Regen. Res. 2017, 12, 1648–1654. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.; Wu, X.; Yan, D.; Peng, C.; Rao, C.; Yan, H. Acrylamide-induced oxidative stress and inflammatory response are alleviated by N-acetylcysteine in PC12 cells: Involvement of the crosstalk between Nrf2 and NF-κB pathways regulated by MAPKs. Toxicol. Lett. 2018, 288, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Scherer, P.E. Adipokines as novel biomarkers and regulators of the metabolic syndrome. Ann. N. Y. Acad. Sci. 2010, 1212, E1–E19. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Kim, K. Effect of subchronic acrylamide exposure on the expression of neuronal and inducible nitric oxide synthase in rat brain. J. Biochem. Mol. Toxicol. 2005, 19, 162–168. [Google Scholar] [CrossRef]
- Hsu, C.N.; Hou, C.Y.; Lu, P.C.; Chang-Chien, G.P.; Lin, S.; Tain, Y.L. Association between Acrylamide Metabolites and Cardiovascular Risk in Children With Early Stages of Chronic Kidney Disease. Int. J. Mol. Sci. 2020, 21, 5855. [Google Scholar] [CrossRef]
- Zhao, M.; Wang, L.; Hu, X.; Chen, F.; Chan, L. Acrylamide-induced neurotoxicity in primary astrocytes and microglia: Roles of the Nrf2-ARE and NF-κB pathways. Food Chem. Toxicol. 2017, 106, 25–35. [Google Scholar] [CrossRef] [PubMed]
- de Luca, C.; Olefsky, J.M. Inflammation and insulin resistance. FEBS Lett. 2008, 582, 97–105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Abdominal Obesity | Waist Circumference (Men > 102 cm; Women > 88 cm) |
|---|---|
| High triglyceride (TG) level † | ≥1.69 mmol/L (≥150 mg/dL) |
| Low HDL cholesterol level | Men: <1.03 mmol/L (<40 mg/dL); Women: <1.29 mmol/L (<50 mg/dL) |
| High blood pressure † | Systolic ≥ 130 mm hg or diastolic ≥ 85 mm hg |
| Impaired FPG concentration † | ≥5.9 mmol/L (≥100 mg/dL) |
| Variables | N = 4813 | ||
|---|---|---|---|
| Non-Metabolic Syndrome N = 3749 | Metabolic Syndrome N = 1064 | p Value | |
| Continuous variables | |||
| Age (years) a | 33.97 (20.86) | 53.54 (19.20) | <0.001 |
| Acrylamide (pmol/g Hb) b | 54.70 (34.70) | 49.80 (34.80) | <0.001 |
| Glycidamide (pmol/g Hb) b | 51.40 (36.25) | 50.00 (36.88) | <0.001 |
| Serum creatinine (μmol/L) a | 74.26 (22.98) | 82.21 (25.64) | <0.001 |
| Serum AST (U/L) a | 24.56 (12.41) | 26.28 (11.77) | <0.001 |
| SBP (mmHg) a | 116.46 (16.48) | 134.36 (21.04) | <0.001 |
| DBP (mmHg) a | 64.23 (12.82) | 71.64 (15.82) | <0.001 |
| Waist circumference (cm) a | 88.84 (15.21) | 108.78 (13.66) | <0.001 |
| Serum TG (mmol/L) a | 2.36 (1.61) | 5.17 (4.32) | <0.001 |
| Serum HDL (mmol/L) a | 1.50 (0.39) | 1.18 (0.34) | <0.001 |
| FPG (mmol/L) a | 5.20 (1.06) | 6.69 (2.47) | <0.001 |
| Categorical variables, n (%) | |||
| Gender | |||
| Male | 2027 (50.5) | 573 (49.7) | 0.666 |
| Female | 1990 (49.5) | 579 (50.3) | |
| Race | |||
| Mexican American | 950 (23.6) | 277 (24.0) | <0.001 |
| Other Hispanic | 123 (3.1) | 29 (2.5) | |
| Non-Hispanic White | 1664 (41.4) | 622 (54.0) | |
| Non-Hispanic Black | 1091 (27.2) | 183 (15.9) | |
| Other Race—Including Multi-Racial | 189 (4.7) | 41 (3.6) | |
| Past history | |||
| Emphysema | 52 (2.1) | 30 (2.8) | 0.257 |
| Angina/angina pectoris | 54 (2.2) | 57 (5.3) | <0.001 |
| Smoke | 483 (41.1) | 195 (33.4) | <0.001 |
| Variables | Acrylamide (HbAA) | Glycidamide (HbGA) | ||||||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||
| β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | β (95% CI) | p Value | |
| Presence of metabolic syndrome | −0.214 (−0.228, −0.140) | <0.001 | −0.031 (−0.089, 0.027) | 0.298 | −0.119 (−0.193, −0.046) | 0.001 | −0.001 (−0.070, 0.068) | 0.977 |
| Number of metabolic syndrome markers | ||||||||
| 1 | −0.165 (−0.272, −0.058) | 0.002 | −0.011 (−0.088, 0.067) | 0.789 | −0.110 (−0.216, −0.003) | 0.044 | 0.005 (−0.087, 0.097) | 0.918 |
| 2 | −0.301 (−0.405, −0.198) | <0.001 | −0.082 (−0.163, −0.002) | 0.045 | −0.179 (−0.283, −0.075) | 0.001 | −0.036 (−0.132, 0.060) | 0.457 |
| 3 | −0.319 (−0.429, −0.209) | <0.001 | −0.051 (−0.141, −0.040) | 0.275 | −0.191 (−0.301, −0.081) | 0.001 | −0.017 (−0.125, 0.091) | 0.762 |
| 4–5 | −0.487 (−0.612, −0.363) | <0.001 | −0.127 (−0.229, −0.025) | 0.015 | −0.278 (−0.402, −0.154) | <0.001 | −0.023 (−0.145, 0.098) | 0.707 |
| P for trend | <0.001 | 0.013 | <0.001 | 0.570 | ||||
| HbAA | HbGA | |||
|---|---|---|---|---|
| OR (95% CI) | p Value | OR (95% CI) | p Value | |
| Model 1 | ||||
| Metabolic syndrome | 0.997 (0.995, 0.998) | <0.001 | 0.997 (0.995, 0.999) | 0.002 |
| Q2 vs. Q1 | 0.560 (0.398, 0.788) | 0.005 | 1.002 (0.724, 1.386) | 0.992 |
| Q3 vs. Q1 | 0.559 (0.403, 0.777) | 0.002 | 0.788 (0.577,1.076) | 0.134 |
| Q4 vs. Q1 | 0.462 (0.351, 0.608) | <0.001 | 0.674 (0.510, 0.890) | 0.005 |
| Model 2 | ||||
| Metabolic syndrome | 0.998 (0.996, 1.000) | 0.023 | 1.000 (0.997, 1.002) | 0.911 |
| Q2 vs. Q1 | 0.604 (0.424, 0.860) | 0.005 | 1.070 (0.763, 1.499) | 0.696 |
| Q3 vs. Q1 | 0.579 (0.410, 0.817) | 0.002 | 0.888 (0.637, 1.237) | 0.481 |
| Q4 vs. Q1 | 0.595 (0.404, 0.876) | 0.009 | 1.020 (0.717, 1.452) | 0.911 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, C.-C.; Cheng, Y.-W.; Chen, W.-L.; Fang, W.-H. Negative Association between Acrylamide Exposure and Metabolic Syndrome Markers in Adult Population. Int. J. Environ. Res. Public Health 2021, 18, 11949. https://doi.org/10.3390/ijerph182211949
Hung C-C, Cheng Y-W, Chen W-L, Fang W-H. Negative Association between Acrylamide Exposure and Metabolic Syndrome Markers in Adult Population. International Journal of Environmental Research and Public Health. 2021; 18(22):11949. https://doi.org/10.3390/ijerph182211949
Chicago/Turabian StyleHung, Chun-Chi, Yung-Wen Cheng, Wei-Liang Chen, and Wen-Hui Fang. 2021. "Negative Association between Acrylamide Exposure and Metabolic Syndrome Markers in Adult Population" International Journal of Environmental Research and Public Health 18, no. 22: 11949. https://doi.org/10.3390/ijerph182211949
APA StyleHung, C.-C., Cheng, Y.-W., Chen, W.-L., & Fang, W.-H. (2021). Negative Association between Acrylamide Exposure and Metabolic Syndrome Markers in Adult Population. International Journal of Environmental Research and Public Health, 18(22), 11949. https://doi.org/10.3390/ijerph182211949