
The Paradox of Conspiracy Theory: The Positive Impact of Beliefs in Conspiracy Theories on Preventive Actions and Vaccination Intentions during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Theory and Research Model
2.1. Dominant Views about Conspiracy Theories
2.2. Preventive Actions and Conspiracy Theories
2.3. Vaccination and Conpiracy Theories
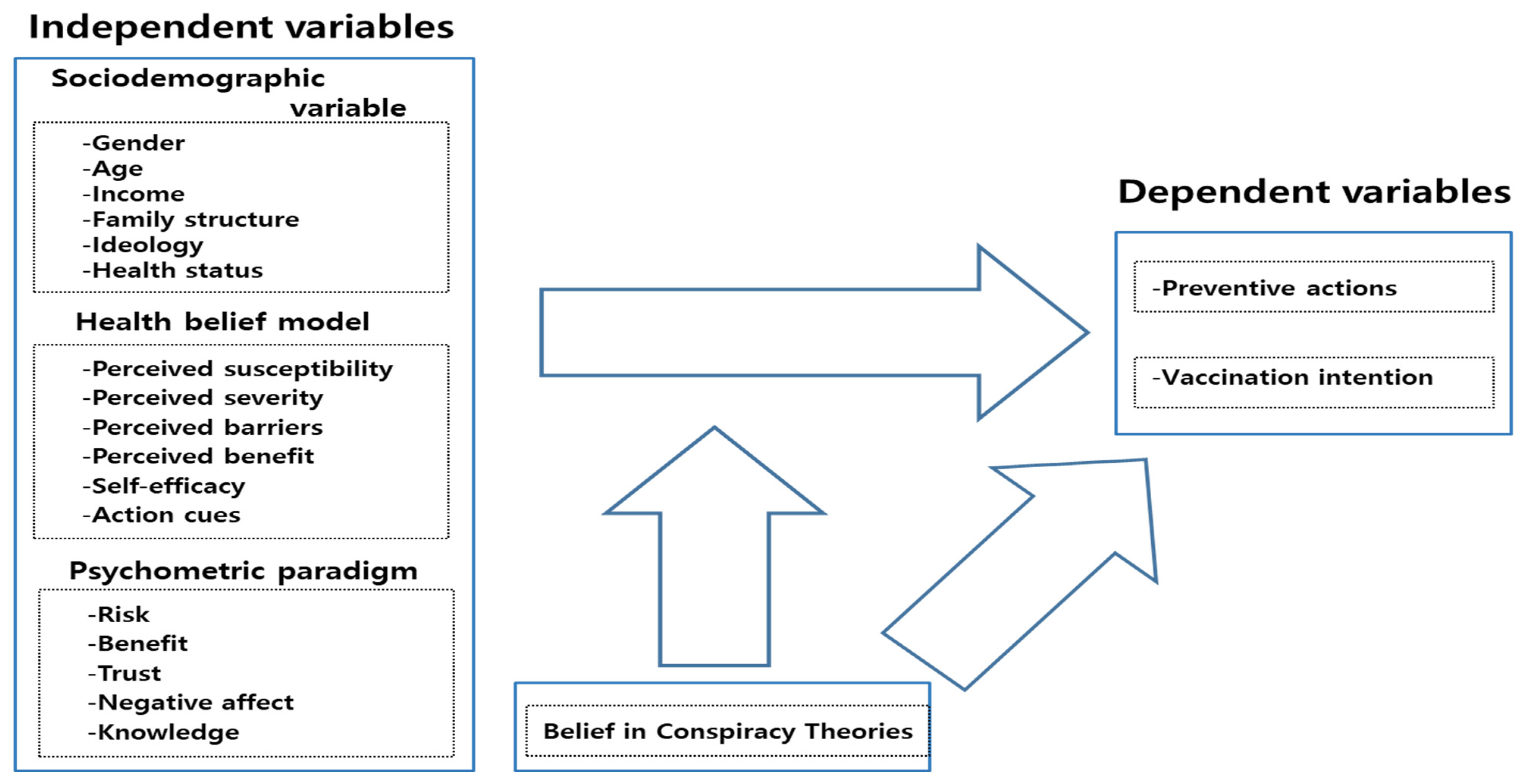
2.4. Research Model
3. Sample and Measures
4. Analysis and Findings
4.1. Descriptive Analysis
4.2. Correlation Analysis
4.3. Regression Analyses
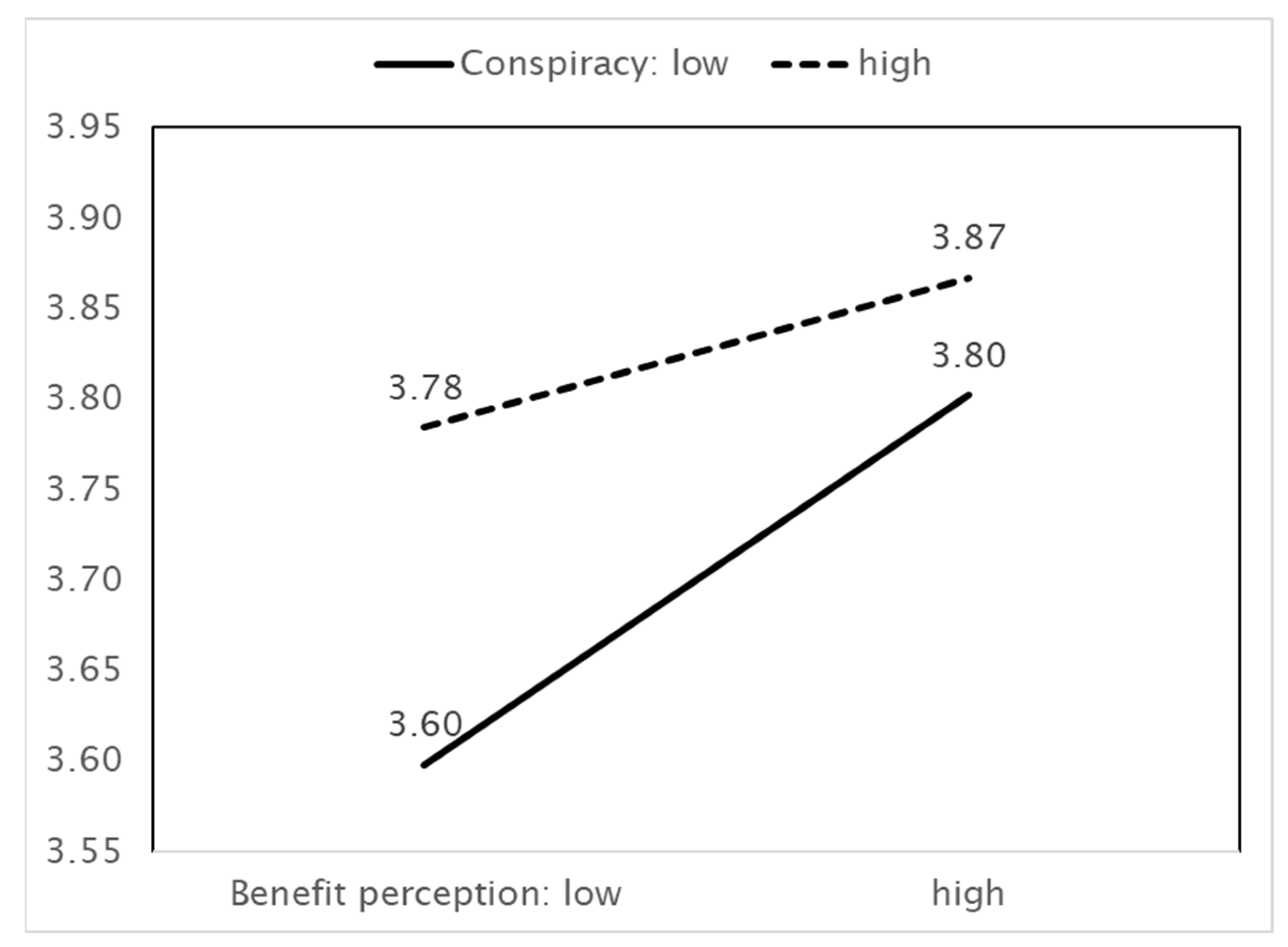
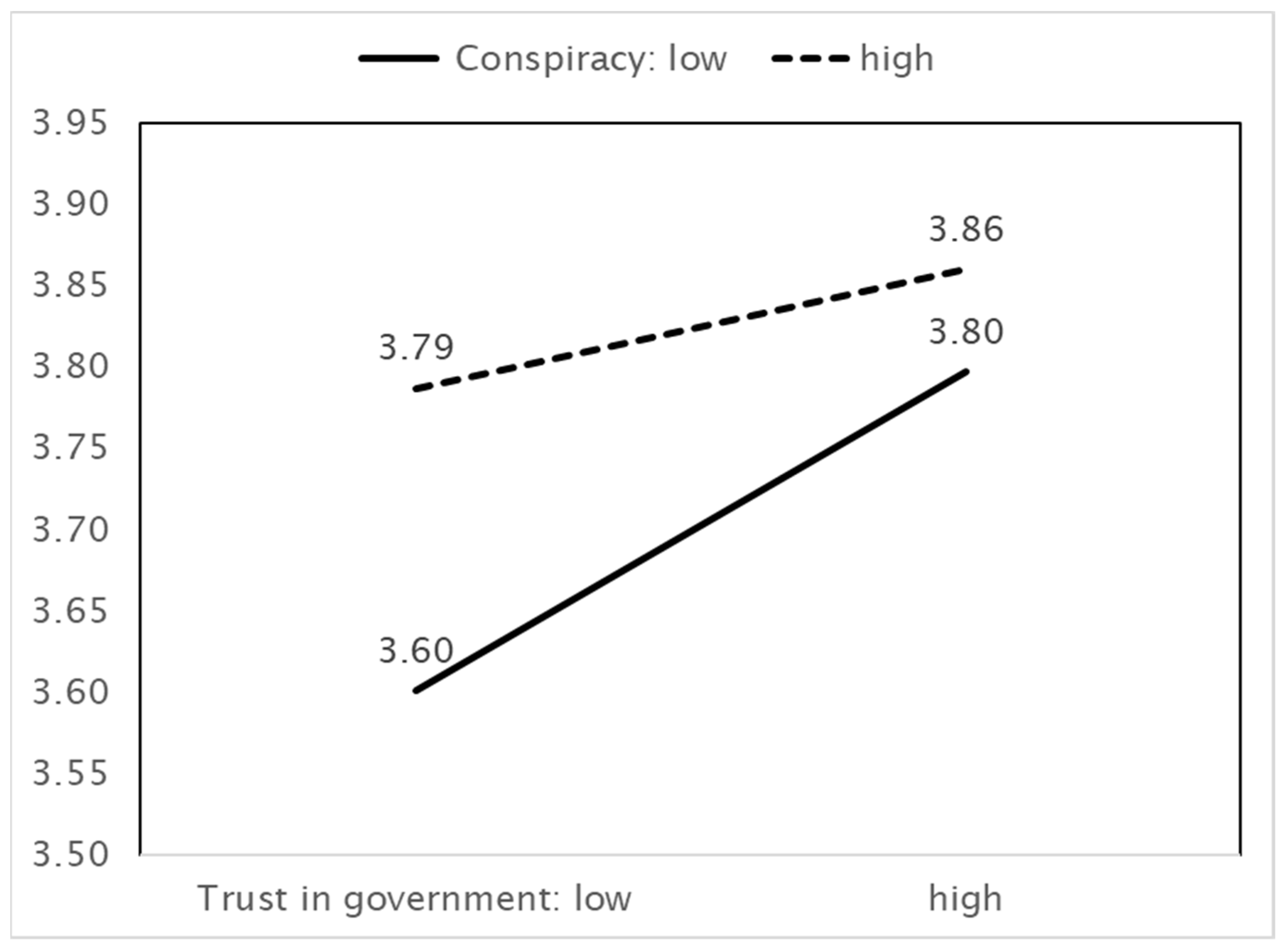
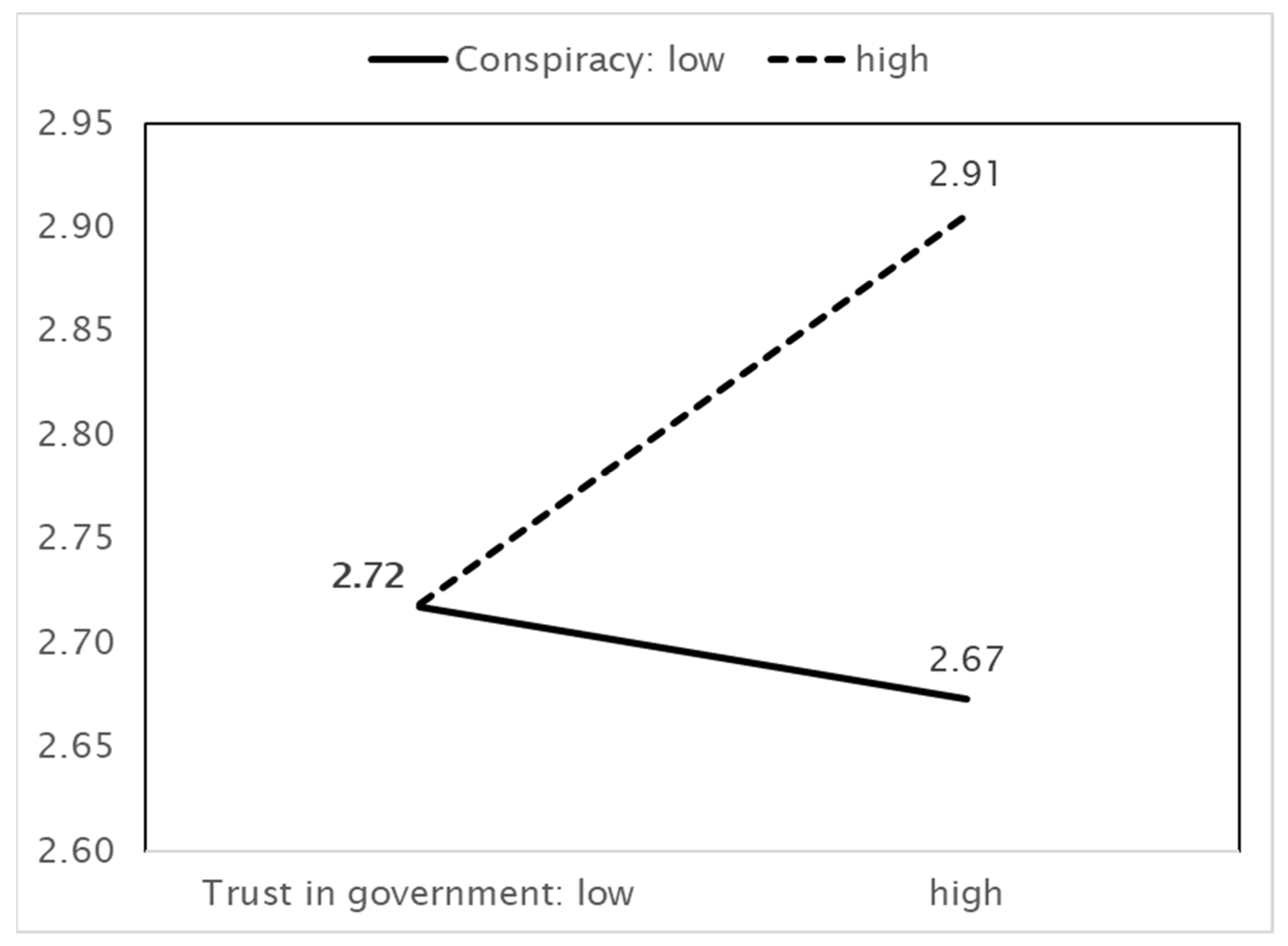
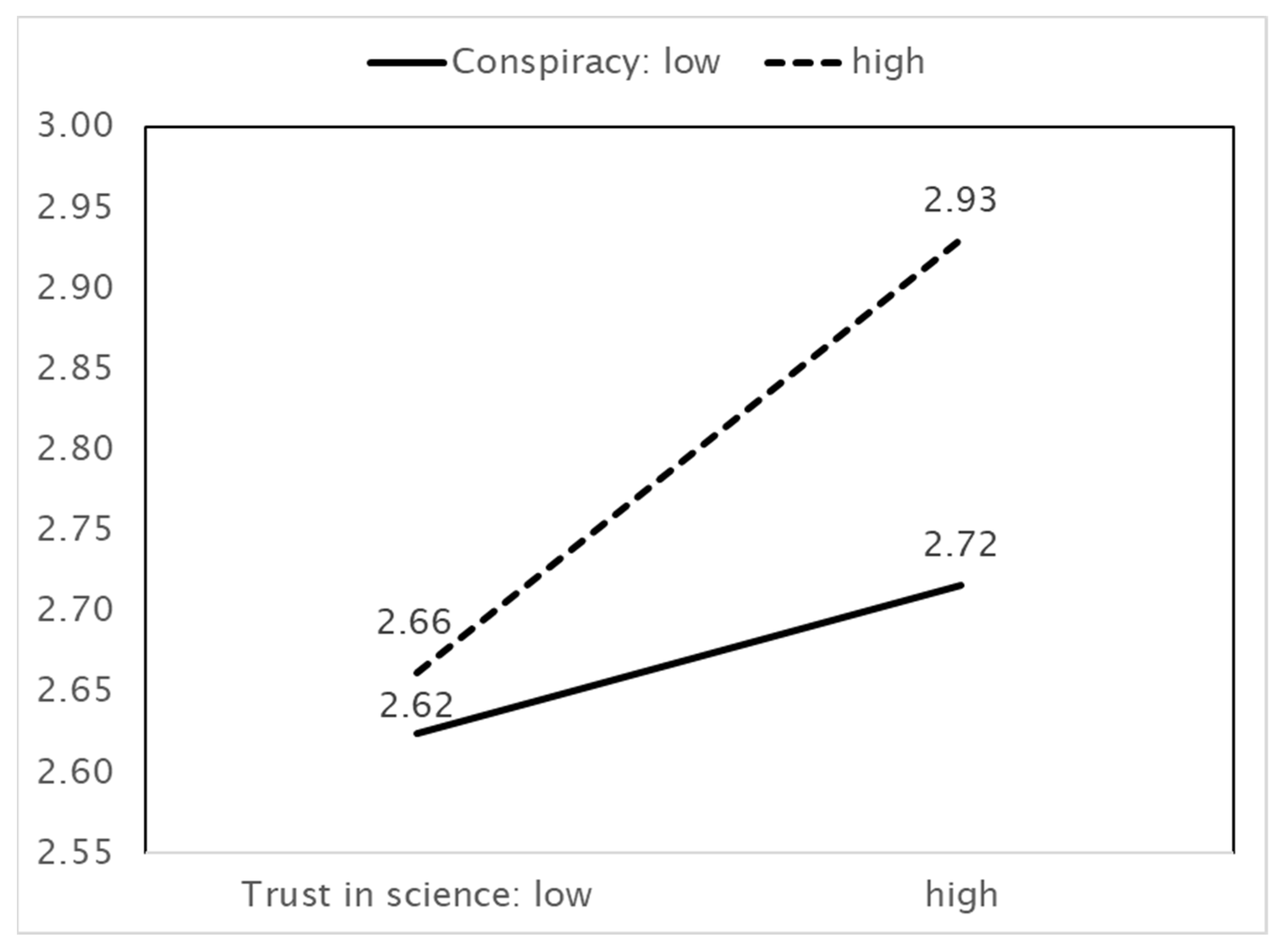
4.4. Moderation Analysis
5. Main Findings and Discussion
6. Conclusions and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| B | SE | Beta | B | SE | Beta | |
|---|---|---|---|---|---|---|
| Benefit perception | 0.081 *** | 0.017 | 0.122 | 0.084 *** | 0.017 | 0.127 |
| Conspiracy | 0.077 *** | 0.018 | 0.104 | 0.082 *** | 0.018 | 0.111 |
| Interaction term | − | −0.046 * | 0.018 | −0.055 | ||
| F-value | 30.586 *** | 29.683 *** | ||||
| R2 square | 0.320 | 0.323 | ||||
| R2 square change | 0.309 | 0.312 | ||||
| Simple slope test | Law | B = 0.118 *** se = 0.022 t = 5.306 | ||||
| Middle | B = 0.084 *** se = 0.017 t = 5.008 | |||||
| High | B = 0.050 ** se = 0.021 t = 2.421 | |||||
| Effect size | 0.005 | |||||
| B | SE | beta | B | SE | beta | |
| Trust in government | 0.067 *** | 0.016 | 0.107 | 0.077 *** | 0.016 | 0.123 |
| Conspiracy | 0.077 *** | 0.018 | 0.104 | 0.084 *** | 0.018 | 0.114 |
| Interaction term | - | −0.048 ** | 0.015 | −0.069 | ||
| F-value | 30.586 *** | 29.878 *** | ||||
| R2 square | 0.320 | 0.324 | ||||
| R2 square change | 0.309 | 0.313 | ||||
| Simple slope test | Law | B = 0.112 *** se = 0.022 t = 5.186 | ||||
| Middle | B = 0.077 *** se = 0.016 t = 4.719 | |||||
| High | B = 0.042 ** se = 0.018 t = 2.327 | |||||
| Effect size | 0.006 | |||||
| B | SE | Beta | B | SE | Beta | |
|---|---|---|---|---|---|---|
| Trust in government | 0.059 * | 0.025 | 0.066 | 0.041 | 0.026 | 0.046 |
| Conspiracy | 0.092 ** | 0.029 | 0.087 | 0.079 ** | 0.029 | 0.075 |
| Interaction term | - | 0.089 *** | 0.024 | 0.091 | ||
| F-value | 15.128 *** | 15.194 *** | ||||
| R² square | 0.189 | 0.199 | ||||
| R² square change | 0.176 | 0.183 | ||||
| Simple slope test | Law | B = −0.025 se = 0.034 t = −0.739 | ||||
| Middle | B = 0.041 se = 0.026 t = 1.605 | |||||
| High | B = 0.107 *** se = 0.028 t = 3.803 | |||||
| Effect size | 0.040 | |||||
| B | SE | beta | B | SE | beta | |
| Trust in science | 0.119 *** | 0.026 | 0.113 | 0.121 *** | 0.026 | 0.115 |
| Conspiracy | 0.092 ** | 0.029 | 0.087 | 0.085 ** | 0.029 | 0.08 |
| Interaction term | - | 0.08 ** | 0.029 | 0.066 | ||
| F-value | 15.128 *** | 14.877 *** | ||||
| R² square | 0.189 | 0.193 | ||||
| R² square change | 0.176 | 0.18 | ||||
| Simple slope test | Law | B = 0.062 se = 0.033 t = 1.853 | ||||
| Middle | B = 0.121 *** se = 0.026 t = 4.615 | |||||
| High | B = 0.179 *** se = 0.034 t = 5.248 | |||||
| Effect size | 0.016 | |||||
Appendix B
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Preventive action | 1 | |||||||
| 2. Vaccination | 0.121 *** | 1 | ||||||
| 3. The government makes important decisions related to coronavirus disease (COVID-19) without the public knowing. | 0.014 | 0.172 *** | 1 | |||||
| 4. Politicians do not honestly reveal their true intentions to the public regarding their decisions on coronavirus disease (COVID-19). | 0.049 * | 0.011 | 0.344 *** | 1 | ||||
| 5. The government is hiding something from the public. | −0.007 | 0.156 *** | 0.611 *** | 0.384 *** | 1 | |||
| 6. There is a secret organization that greatly influences political decisions. | −0.004 | 0.115 *** | 0.480 *** | 0.377 *** | 0.682 *** | 1 | ||
| 7. The government is always monitoring the public. | 0.004 | 0.175 *** | 0.544 *** | 0.351 *** | 0.665 *** | 0.642 *** | 1 | |
| 8. Certain powerful nations deliberately created the coronavirus (COVID-19) to dominate the world. | −0.026 | 0.146 *** | 0.389 *** | 0.204 *** | 0.416 *** | 0.455 *** | 0.508 *** | 1 |
| 9. Coronavirus disease (COVID-19) was deliberately created by pharmaceutical companies to make money. | −0.069 *** | 0.152 *** | 0.356 *** | 0.092 *** | 0.355 *** | 0.397 *** | 0.408 *** | 0.721 *** |
References
- Lynas, M. COVID: Top 10 Current Conspiracy Theories. 2020. Available online: https://allianceforscience.cornell.edu/blog/2020/04/covid-top-10-current-conspiracy-theories/ (accessed on 1 May 2019).
- Oliver, J.; Wood, T. Conspiracy theories and the paranoid style(s) of mass opinion. Am. J. Pol. Sci. 2014, 58, 952–966. Available online: http://www.jstor.org/stable/24363536 (accessed on 10 September 2020). [CrossRef]
- Mitchell, A.; Jurkowitz, M.; Oliphant, B.J.; Shearer, E. Most Americans Have Heard of the Conspiracy Theory that the COVID-19 Outbreak Was Planned, and about One-Third of Those Aware of it Say it Might Be True. 2020. Available online: https://www.pewresearch.org/journalism/2020/06/29/ (accessed on 10 September 2020).
- Allington, D.; Duffy, B.; Moxham-Hall, V.; McAndrew, S.; Murkin, G. Coronavirus Conspiracies and Views Of Vaccination. 2021. Available online: https://www.kcl.ac.uk/policy-institute/assets/coronavirus-conspiracies-and-views-of-vaccination.pdf (accessed on 21 June 2021).
- Duffy, B.; Allington, D. Covid Conspiracies and Confusions: The Impact on Compliance with the UK’s Lockdown Rules and the Link with Social Media Use. 2020. Available online: https://www.ipsos.com/sites/default/files/ct/news/documents/2020-06/covid-19-conspiracies-and-confusions.pdf (accessed on 21 July 2021).
- Pummerer, L.; Böhm, R.; Lilleholt, L.; Winter, K.; Zettler, I.; Sassenberg, K. Conspiracy Theories and Their Societal Effects During the COVID-19 Pandemic. Soc. Psychol. Pers. Sci. 2021. [Google Scholar] [CrossRef]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Soc. Sci. Med. 2020, 263, 113356. [Google Scholar] [CrossRef]
- Douglas, K.M. Are Conspiracy Theories Harmless? Span. J. Psychol. 2021, 24, e13. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Saunders, K.L.; Farhart, C.E. Conspiracy endorsement as motivated reasoning: The moderating roles of political knowledge and trust. Am. J. Pol. Sci. 2016, 60, 824–844. [Google Scholar] [CrossRef] [Green Version]
- Connolly, J.M.; Uscinski, J.E.; Klofstad, C.A.; West, J.P. Communicating to the public in the era of conspiracy theory. Public Integr. 2019, 21, 469–476. [Google Scholar] [CrossRef]
- Swami, V.; Furnham, A. Political Paranoia and Conspiracy Theories. In Power Politics, and Paranoia: Why People Are Suspicious of Their Leaders; van Prooijen, J.W., van Lange, P.A.M., Eds.; Cambridge University Press: Cambridge, MA, USA, 2014; pp. 218–236. [Google Scholar]
- Uscinski, J.E.; Klofstad, C.; Atkinson, M.D. What drives conspiratorial beliefs? The role of informational cues and predispositions. Polit. Res. Q. 2016, 69, 57–71. [Google Scholar] [CrossRef] [Green Version]
- Uscinski, J.E. The study of conspiracy theories. Argumenta 2017, 3, 233–245. [Google Scholar]
- Uscinski, J.E. The Conspiracy Theories: A Primer; Rowman & Littlefield: New York, NY, USA, 2020. [Google Scholar]
- Uscinski, J.E.; Parent, J.M. American Conspiracy Theories; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Uscinski, J.E. Conspiracy Theories and the People Who Believe Them; Uscinski, J.E., Ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Uscinski, J.; Klofstad, C.; Atkinson, M.D. Why do people believe in conspiracy theories? The role of informational cues and predispositions. SSRN 2013. [Google Scholar] [CrossRef]
- Uscinski, J.E.; Olivella, S. The conditional effect of conspiracy thinking on attitudes toward climate change. Res. Polit 2017, 4, 1–9. [Google Scholar] [CrossRef]
- Douglas, K.M.; Sutton, R.M.; Cichocka, A. The psychology of conspiracy theories. Curr. Dir. Psychol. Sci. 2017, 26, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M.; Uscinski, J.E.; Sutton, R.M.; Cichocka, A.; Nefes, T.; Ang, C.S.; Deravi, F. Understanding Conspiracy Theories. Polit. Psychol. 2019, 40, 3–35. [Google Scholar] [CrossRef] [Green Version]
- Earnshaw, V.A.; Bogart, L.M.; Klompas, M.; Katz, I.T. Medical mistrust in the context of Ebola: Implications for intended care-seeking and quarantine policy support in the United States. J. Health Psychol. 2019, 24, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Stempel, C.; Hargrove, S.; Stempel, G.H. Media use, social structure and belief in 9/11 conspiracy theories. J. Mass Commun. Q. 2007, 84, 353–373. [Google Scholar] [CrossRef]
- Kim, S.; Kim, S. Searching for General Model of Conspiracy Theories and Its Implication for Public Health Policy: Analysis of the Impacts of Political, Psychological, Structural Factors on Conspiracy Beliefs about the COVID-19 Pandemic. Int. J. Env. Res. Public Health 2021, 18, 266. [Google Scholar] [CrossRef]
- Swami, V.; Chamorro-Premuzic, T.; Furnham, A. Unanswered questions: A preliminary investigation of personality and individual difference predictors of 9/11 conspiracist beliefs. Appl. Cognit. Psychol. 2010, 24, 749–761. [Google Scholar] [CrossRef]
- De Coninck, D.; Frissen, T.; Matthijs, K.; D’Haenens, L.; Lits, G.; Champagne-Poirier, O.; Carignan, M.-E.; David, M.D.; Pignard-Cheynel, N.; Salerno, S.; et al. Beliefs in Conspiracy Theories and Misinformation About COVID-19: Comparative Perspectives on the Role of Anxiety, Depression and Exposure to and Trust in Information Sources. Front. Psychol. 2021, 12, 646394. [Google Scholar] [CrossRef]
- Swami, V.; Coles, R. The truth is out there: Belief in conspiracy theories. Psychologist 2010, 23, 560–563. [Google Scholar]
- Knight, P. ILOVEYOU: Viruses, paranoia, and the environment of risk. Sociol. Rev. Monogr. 2001, 48, 17–30. [Google Scholar] [CrossRef]
- Radnitz, S.; Underwood, P. Is belief in conspiracy theories pathological? A survey experiment on the cognitive roots of extreme suspicion. Br. J. Polit. Sci. 2015, 47, 113–129. [Google Scholar] [CrossRef] [Green Version]
- Franks, B.; Bangerter, A.; Bauer, M.W. Conspiracy theories as quasi-religious mentality: An integrated account from cognitive science, social representations theory, and frame theory. Front. Psychol. 2013, 4, 424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasson, T. African American Conspiracy Theories and the Social Construction of Crime. Sociol. Inq. 1995, 65, 265–285. [Google Scholar] [CrossRef]
- Miller, S. Conspiracy theories: Public arguments as coded social critiques. A rhetorical analysis of the TWA Flight 800 conspiracy theories. Argum. Advocacy 2002, 39, 40–56. [Google Scholar] [CrossRef]
- Basham, L. Malevolent global conspiracy. J Soc. Philos. 2003, 34, 91–103. [Google Scholar] [CrossRef]
- Imhoff, R.; Bruder, M. Speaking (Un–)Truth to Power: Conspiracy Mentality as A Generalised Political Attitude. Eur. J. Pers. 2014, 28, 25–43. [Google Scholar] [CrossRef]
- Mari, S.; Volpato, C.; Papastamou, S.; Chryssochoou, X.; Prodromitis, G.; Pavlopoulos, V. How Political Orientation and Vulnerability Shape Representations of the Economic Crisis in Greece and Italy. Int. Rev. Soc. Psychol. 2017, 30, 52–67. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, L.E. Conspiracy theory. In The SAGE Glossary of the Social and Behavioral Sciences; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2009; p. 104. [Google Scholar] [CrossRef]
- Clark, S. Conspiracy theories and conspiracy theorizing. Philos. Soc. Sci. 2002, 32, 131–150. [Google Scholar] [CrossRef]
- Moore, A. Conspiracy and Conspiracy Theories in Democratic Politics. Crit. Rev. 2016, 28, 1–23. [Google Scholar] [CrossRef]
- Bartlett, J.; Miller, C. The Power of Unreason: Conspiracy Theories, Extremism and Counter-Terrorism; Demos: London, UK, 2010. [Google Scholar]
- Einstein, K.L.; Glick, S. Do I think BLS data are BS? The consequences of conspiracy theories. Polit. Behav. 2015, 37, 679–701. [Google Scholar] [CrossRef]
- Abalakina-Paap, M.; Stephan, W.G.; Craig, T.; Gregory, W.L. Beliefs in conspiracies. Polit. Psychol. 1999, 20, 637–647. [Google Scholar] [CrossRef]
- Goertzel, T. Belief in conspiracy theories. Polit. Psychol. 1994, 15, 731–742. [Google Scholar] [CrossRef]
- Imhoff, R.; Lamberty, P.; Klein, O. Using power as a negative cue: How conspiracy mentality affects epistemic trust in sources of historical knowledge. Pers. Soc. Psychol. Bull. 2018, 44, 1364–1379. [Google Scholar] [CrossRef]
- Jolley, D.; Meleady, R.; Douglas, K.M. Exposure to intergroup conspiracy theories promotes prejudice which spreads across groups. Br. J. Psychol. 2020, 111, 17–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolley, D.; Douglas, K.M. The social consequences of conspiracism: Exposure to conspiracy theories decreases intentions to engage in politics and to reduce one’s carbon footprint. Br. J. Psychol. 2014, 105, 35–56. [Google Scholar] [CrossRef] [PubMed]
- Rottweiler, B.; Gill, P. Conspiracy Beliefs and Violent Extremist Intentions: The Contingent Effects of Self-efficacy, Self-control and Law-related Morality. Terror. Polit. Violence 2020, 1–20. [Google Scholar] [CrossRef]
- Faasse, K.; Newby, J. Public perceptions of COVID-19 in Australia: Perceived risk, knowledge, health-protective behaviors, and vaccine intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Chan, H.H.; Yi, Y.Y.; Tang, A.; Wei, W.I.; Wong, Y.S.J. Community responses during the early phase of the COVID-19 epidemic in Hong Kong: Risk perception, information exposure and preventive measures. MedRxiv 2020, 26, 200500. [Google Scholar]
- Prati, G.; Pietrantoni, L.; Zani, B. A social-cognitive model of pandemic influenza H1N1 risk perception and recommended behaviors in Italy. Risk Anal. 2010, 31, 645–656. [Google Scholar] [CrossRef]
- Jose, R.; Narendran, M.; Bindu, A.; Beevi, N.; Manju, L.; Benny, P.V. Public perception and preparedness for the pandemic COVID 19: A Health Belief Model approach. Clin. Epidemiol. Glob. Health 2020, 9, 41–46. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Hornik, R.; Kikut, A.; Jesch, E.; Woko, C.; Siegel, L.; Kim, K. Association of COVID-19 misinformation with face mask wearing and social distancing in a nationally representative US sample. Health Commun. 2021, 36, 6–14. [Google Scholar] [CrossRef]
- Allington, D.; Dhavan, N. The Relationship between Conspiracy Beliefs and Compliance with Public Health Guidance with Regard to COVID-19; Centre for Countering Digital Hate: London, UK, 2020. [Google Scholar]
- Freeman, D.; Bentall, R.P. The concomitants of conspiracy concerns. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 595–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biddlestone, M.; Green, R.; Douglas, K. Cultural orientation, powerlessness, belief in conspiracy theories, and intentions to reduce the spread of COVID-19. Br J Soc Psychol. 2020, 59, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Bierwiaczonek, K.; Kunst, J.R.; Pich, O. Belief in COVID-19 conspiracy theories reduces social distancing over time. Appl. Psychol. Health Well Being 2020, 12, 1270–1285. [Google Scholar] [CrossRef] [PubMed]
- Banai, P.I.; Banai, B.; Mikloušić, I. Beliefs in COVID-19 conspiracy theories, compliance with the preventive measures, and trust in government medical officials. Curr. Psychol. 2021, 26, 1–11. [Google Scholar] [CrossRef]
- Alper, S.; Bayrak, F.; Yilmaz, O. Psychological correlates of COVID-19 conspiracy beliefs and preventive measures: Evidence from Turkey. Curr. Psychol. 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Čavojová, V.; Šrol, J.; Mikušková, E.B. How scientific reasoning correlates with health-related beliefs and behaviors during the COVID-19 pandemic? J. Heal. Psychol. 2020, 1359105320962266. [Google Scholar] [CrossRef]
- Hussein, I.E.; Echams, N.; Echams, S.; Sayegh, S.E.; Badran, R.; Eraad, M.; Egerges-Geagea, A.; Eleone, A.; Ejurjus, A. Vaccines Through Centuries: Major Cornerstones of Global Health. Front. Public Health 2015, 3, 269. [Google Scholar] [CrossRef]
- Page, B. Attitudes to COVID-19 Vaccines. Presented at World Economic Forum. 2021. Available online: https://www.ipsos.com/sites/default/files/ct/news/documents/2021-01/attitudes-to-covid-19-vaccines-ipsos.pdf (accessed on 5 May 2021).
- Wang, Q.; Yang, L.; Jin, H.; Lin, L. Vaccination against COVID-19: A systematic review and meta-analysis of acceptability and its predictors. Prev. Med. 2021, 150, 106694. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Wang, W.; Wu, Q.; Yang, J.; Dong, K.; Chen, X.; Bai, X.; Chen, X.; Chen, Z.; Viboud, C.; Ajelli, M.; et al. Global, regional, and national estimates of target population sizes for covid-19 vaccination: Descriptive study. BMJ 2020, 371, m4704. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M. About One in Five Americans Remain Vaccine-Resistant. 2021. Available online: https://news.gallup.com/poll/353081/one-five-americans-remain-vaccine-resistant.aspx (accessed on 6 August 2021).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, I.; Kabir, R.; Rahman, M.A.; Alradie-Mohamed, A.; Vinnakota, D.; Al-Mohaimeed, A. The Health Belief Model Predicts Intention to Receive the COVID-19 Vaccine in Saudi Arabia: Results from a Cross-Sectional Survey. Vaccines 2021, 9, 864. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Wong, E.L.; Huang, J.; Cheung, A.W.; Law, K.; Chong, M.K.; Ng, R.W.; Lai, C.K.; Boon, S.S.; Lau, J.T.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef]
- Craciun, C.; Baban, A. Who will take the blame? Understanding the reasons why Romanian mothers decline HPV vaccination for their daughters. Vaccine 2012, 30, 6789–6793. [Google Scholar] [CrossRef]
- Gu, F.; Wu, Y.; Hu, X.; Guo, J.; Yang, X.; Zhao, X. The Role of Conspiracy Theories in the Spread of COVID-19 across the United States. Int. J. Environ. Res. Public Health 2021, 18, 3843. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, R.; Chen, B.; Chen, H.; Li, Y.; Chen, Z.; Zhu, H.; Wang, H. Knowledge, Perceived Beliefs, and Preventive Behaviors Related to COVID-19 Among Chinese Older Adults: Cross-Sectional Web-Based Survey. J. Med. Internet Res. 2020, 22, e23729. [Google Scholar] [CrossRef]
- Handebo, S.; Wolde, M.; Shitu, K.; Kassie, A. Determinant of intention to receive COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. PLoS ONE 2021, 16, e0253499. [Google Scholar] [CrossRef]
- Slovic, P.; Fischhoff, B.; Lichtentstein, S. The Psychometric study of risk perception. In Contemporary Issues in Risk Analysis: The Behavioral and Social Sciences; Menkes, J., Covello, V., Mumpower, J., Eds.; Plenum: New York, NY, USA, 1986. [Google Scholar]
- Shahin, M.A.H.; Hussien, R.M. Risk perception regarding the COVID-19 outbreak among the general population: A comparative Middle East survey. Middle East Curr. Psychiatry 2020, 27, 1–19. [Google Scholar] [CrossRef]
- Min, C.; Shen, F.; Yu, W.; Chu, Y. The relationship between government trust and preventive behaviors during the COVID-19 pandemic in China: Exploring the roles of knowledge and negative emotion. Prev Med. 2020, 141, 106288. [Google Scholar] [CrossRef] [PubMed]
- Savadori, L.; Lauriola, M. Risk Perception and Protective Behaviors During the Rise of the COVID-19 Outbreak in Italy. Front. Psychol. 2021, 11, 57733. [Google Scholar] [CrossRef] [PubMed]
- Mou, Y.; Lin, C.A. Communicating Food Safety via the Social Media: The Role of Knowledge and Emotions on Risk Perception and Prevention. Sci. Commun. 2014, 36, 593–616. [Google Scholar] [CrossRef]
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yang, J.Z. In the Wake of Scandals: How Media Use and Social Trust Influence Risk Perception and Vaccination Intention among Chinese Parents. Health Commun. 2020, 36, 1188–1199. [Google Scholar] [CrossRef]
- Muller, R. COVID-19 Brings a Pandemic of Conspiracy Theories. 2020. Available online: https://www.psychologytoday.com/us/blog/talking-about-trauma/202004/covid-19-brings-pandemic-conspiracy-theories (accessed on 11 July 2020).
- Earnshaw, E.V.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl. Behav. Med. 2020, 10, 850–856. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Butter, M.; Knight, P. Bridging the great divide: Conspiracy theory research for the 21st century. Diogenes 2015, 62, 1–13. [Google Scholar] [CrossRef]
- Adam-Troian, J.; Wagner-Egger, P.; Motyl, M.; Arciszewski, T.; Imhoff, R.; Zimmer, F.; Klein, O.; Babinska, M.; Bangerter, A.; Bilewicz, M.; et al. Investigating the links between cultural values and belief in conspiracy theories: The key roles of collectivism and masculinity. Political Psychol. 2021, 42, 597–618. [Google Scholar] [CrossRef]

| Categories | N | % | Categories | N | % | ||
|---|---|---|---|---|---|---|---|
| All respondents | 1525 | 100 | Education level | High school | 720 | 47.2 | |
| Gender | Men | 731 | 47.9 | College | 805 | 52.8 | |
| Women | 794 | 52.1 | No. of children | 0 | 1085 | 71.1 | |
| Age | 18–29 | 254 | 16.7 | 1 | 241 | 15.8 | |
| 30–39 | 248 | 16.3 | 2+ | 199 | 13.0 | ||
| 40–49 | 299 | 19.6 | No. of elderly people | 0 | 859 | 56.4 | |
| 50–59 | 310 | 20.3 | 1 | 279 | 18.3 | ||
| 60+ | 414 | 27.1 | 2+ | 386 | 25.3 | ||
| Household income | <299 MW | 499 | 32.7 | Ideology | Conservative | 714 | 46.8 |
| 300–499 MW | 577 | 37.8 | Progressive | 811 | 53.2 | ||
| >500 MW | 449 | 29.4 | Health status change after COVID-19 | Not worse | 668 | 43.8 | |
| Worse | 857 | 56.2 | |||||
| Factor | Variable | Measures | Reliability |
|---|---|---|---|
| Preventive actions | (1) wearing a mask; (2) covering one’s mouth with one’s sleeve when coughing; (3) washing one’s hands for at least 30 s; (4) refraining from traveling or going out; (5) ventilating rooms at least twice a day; (6) social distancing; (7) staying at home for three to four days if sick; (8) not going where there are many people; (9) using hand sanitizer to clean one’s hands; (10) refraining from visiting hospitals; (11) avoiding visiting public places; (12) not holding meetings with people; (13) keeping a distance of two arms’ length from people; (14) refraining from using public transportation; (15) staying two meters away from people in daily life; (16) eating health foods, such as vitamins; (17) periodically disinfecting things that one touches; (18) avoiding touching one’s eyes, nose, or mouth with one’s hands; (19) disinfecting cell phones | 0.926 | |
| Vaccination intentions | - If the COVID-19 vaccine is available, I will apply for vaccination first. - Even if there are side effects, I plan to use the COVID-19 vaccine early. | 0.649 | |
| Beliefs in conspiracy theories | - Politicians do not honestly reveal their true intentions to the public regarding their decisions on coronavirus disease (COVID-19). - There is a secret organization that greatly influences political decisions. - The government is hiding something from the public. - The government is always monitoring the public. - The government makes important decisions related to coronavirus disease (COVID-19) without the public knowing. - Certain powerful nations deliberately created the coronavirus (COVID-19) to dominate the world. - Coronavirus disease (COVID-19) was deliberately created by pharmaceutical companies to make money. | 0.852 | |
| Health belief factors | Perceived susceptibility | - I am more likely to be at risk for COVID-19 than others are. - I live in an environment where I can be exposed to COVID-19 infection. | 0.759 |
| Perceived severity | - Diseases caused by COVID-19 infection have very serious consequences. - Diseases caused by COVID-19 infection will have a major impact on my life. | 0.781 | |
| Perceived barriers | - Excessive efforts are necessary to comply with actions for COVID-19 prevention. - There are many obstacles to complying with actions for COVID-19 prevention. | 0.503 | |
| Perceived benefit | - The benefits of complying with actions for COVID-19 prevention outweigh the costs. - The benefits of taking actions for COVID-19 prevention outweigh the inconvenience. | 0.575 | |
| Self-efficacy | - If I try, I can fully practice preventive actions. - I am sufficiently able to take actions for COVID-19 prevention. | 0.865 | |
| Action cues 1: Exposure to media | How much COVID-19-related information do you obtain from the following sources: - offline media (broadcasting, paper newspapers, magazines, etc.) - online media (Internet newspapers, portal news, etc.) - Internet sources (personal blogs, social networks, cafes, and communities). → Response scale: (1) I did not get information at all; (2) I did not get much information; (3) I got information; (4) I got some information, (5) I got a lot of information. | 0.603 | |
| Action cues 2: Knowing confirmed cases | -Has anyone you know had a confirmed case of coronavirus? → Response scale: (1) No; (2) Yes. | - | |
| Psychometric Paradigm Factors | Risk perception | - The danger from coronavirus will be fatal to me. - Coronavirus is a serious threat to me and my family. | 0.859 |
| Benefit perception | - If the coronavirus problem is solved, it will greatly benefit our society. - Once the coronavirus is resolved, our society will develop greatly. | 0.812 | |
| Trust in government | - The government has the capacity to control the spread of the coronavirus. - The government has a well-prepared preventive system in place for the coronavirus problem. | 0.861 | |
| Trust in experts | How much trust do you have in information on the coronavirus from the following organizations and people? - the World Health Organization - doctors → Response scale: (1) extremely distrust; (2) slightly distrust; (3) usually trust; (4) slightly trust; (5) extremely trust. | 0.448 | |
| Trust in science | - Thanks to science and technology, the earth’s resources will not be depleted but will become abundant. - Science and technology solve many social problems rather than causing them. | 0.754 | |
| Negative affect | - When it comes to coronavirus, negative feelings come first. - Negative images immediately come to mind when I think of coronavirus. | 0.910 | |
| Knowledge | - I have good knowledge about the COVID-19 pandemic. - I know more about COVID-19 than others do. | 0.840 | |
| Preventive Actions | Vaccination Intentions | Beliefs in Conspiracies | |||||
|---|---|---|---|---|---|---|---|
| Mean | p-Value | Mean | p-Value | Mean | p-Value | ||
| All respondents | 3.771 | - | 2.736 | 2.691 | |||
| Gender | Male | 3.667 | 0.000 | 2.758 | 0.290 | 2.704 | 0.516 |
| Female | 3.867 | 2.715 | 2.680 | ||||
| Age | 18–29 | 3.643 | 0.000 | 2.646 | 0.014 | 2.704 | 0.596 |
| 30–39 | 3.745 | 2.702 | 2.712 | ||||
| 40–49 | 3.712 | 2.749 | 2.720 | ||||
| 50–59 | 3.810 | 2.685 | 2.631 | ||||
| 60+ | 3.879 | 2.839 | 2.696 | ||||
| Household income | <299 MW | 3.756 | 0.195 | 2.737 | 0.257 | 2.762 | 0.035 |
| 300–499 MW | 3.753 | 2.699 | 2.658 | ||||
| >500 MW | 3.810 | 2.781 | 2.656 | ||||
| Education level | High school | 3.749 | 0.145 | 2.797 | 0.004 | 2.711 | 0.337 |
| College | 3.790 | 2.681 | 2.674 | ||||
| No. of children | 0 | 3.772 | 0.845 | 2.712 | 0.130 | 2.652 | 0.004 |
| 1 | 3.756 | 2.763 | 2.778 | ||||
| 2+ | 3.786 | 2.829 | 2.800 | ||||
| No. of elderly people | 0 | 3.718 | 0.000 | 2.697 | 0.056 | 2.679 | 0.724 |
| 1 | 3.841 | 2.751 | 2.699 | ||||
| 2+ | 3.838 | 2.811 | 2.714 | ||||
| Ideology | Conservative | 3.753 | 0.226 | 2.744 | 0.686 | 2.816 | 0.000 |
| Progressive | 3.787 | 2.728 | 2.581 | ||||
| Health status change after COVID-19 | Not worse | 3.777 | 0.719 | 2.554 | 0.000 | 2.459 | 0.000 |
| Worse | 3.767 | 2.877 | 2.872 | ||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Preventive actions | 0.105 *** | −0.013 | −0.078 *** | 0.192 *** | −0.069 *** | 0.195 *** | 0.368 *** | 0.140 *** | −0.017 | 0.243 *** | 0.312 *** | 0.233 *** | 0.150 *** | 0.131 *** | 0.174 *** | 0.240 *** | ||
| 2. Vaccination intentions | 0.121 *** | 0.124 *** | 0.172 *** | 0.074 *** | 0.167 *** | 0.047 * | −0.054 ** | 0.102 *** | 0.012 | 0.164 *** | 0.061 ** | 0.062 ** | 0.120 *** | 0.163 *** | 0.025 | 0.155 *** | ||
| 3. Beliefs in conspiracy theories | −0.008 | 0.183 *** | 0.096 *** | −0.066 ** | 0.257 *** | −0.094 *** | −0.182 *** | 0.054 * | 0.023 | 0.050 * | −0.167 *** | −0.253 *** | −0.014 | 0.048 * | −0.066 ** | −0.069 *** | ||
| Health Belief Factors | 4. Perceived susceptibility | −0.056 * | 0.223 *** | 0.159 *** | 0.208 *** | 0.159 *** | 0.050 * | −0.104 *** | −0.024 | 0.054 ** | 0.152 *** | −0.075 ** | −0.034 | −0.046 * | −0.048 * | 0.079 *** | 0.079 *** | |
| 5. Perceived severity | 0.227 *** | 0.110 *** | −0.028 | 0.237 *** | −0.048 * | 0.165 *** | 0.256 *** | 0.038 | −0.028 | 0.458 *** | 0.192 *** | 0.024 | −0.068 *** | −0.033 | 0.592 *** | 0.164 *** | ||
| 6. Perceived barriers | −0.064 * | 0.223 *** | 0.317 *** | 0.224 *** | −0.008 | 0.028 | −0.129 | 0.036 | 0.009 | 0.029 | −0.107 | −0.098 | 0.031 | 0.100 *** | −0.053 | 0.014 | ||
| 7. Perceived benefits | 0.196 *** | 0.035 | −0.120 *** | 0.045 | 0.164 *** | 0.017 | 0.307 *** | 0.054 | 0.001 | 0.102 *** | 0.195 *** | 0.224 *** | 0.054 | 0.121 *** | 0.174 *** | 0.187 *** | ||
| 8. Self−efficacy | 0.364 *** | −0.090 *** | −0.239 *** | −141 *** | 0.236 *** | −0.175 *** | 0.321 *** | 0.086 | −0.026 | 0.179 *** | 0.310 | 0.240 | 0.067 | 0.104 | 0.278 *** | 0.140 | ||
| 9. Media exposure | 0.154 *** | 0.106 *** | 0.063 * | −0.007 | 0.056 * | 0.046 | 0.057 * | 0.083 ** | 0.033 | 0.090 *** | 0.096 *** | −0.019 | 0.337 *** | 0.141 *** | 0.031 | 0.107 *** | ||
| 10. Knowing a confirmed case | −0.018 | 0.011 | 0.019 | 0.052 * | −0.032 | 0.009 | 0.004 | −0.025 | 0.037 | −0.018 | −0.011 | −0.007 | −0.010 | −0.011 | −0.032 | 0.045 * | ||
| Psychometric Factors | 11. Risk perception | 0.266 *** | 0.218 *** | 0.109 *** | 0.210 *** | 0.487 *** | 0.096 *** | 0.096 *** | 0.134 *** | 0.107 *** | −0.018 | 0.251 *** | 0.074 * | 0.039 | 0.012 | 0.350 *** | 0.120 *** | |
| 12. Benefit perception | 0.309 *** | 0.031 | −0.214 *** | −0.094 *** | 0.177 *** | −0.134 *** | 0.219 *** | 0.337 *** | 0.101 *** | −0.002 | 0.221 *** | 0.348 *** | 0.091 *** | 0.156 *** | 0.177 *** | 0.173 *** | ||
| 13. Trust in government | 0.220 *** | 0.020 | −0.320 *** | −0.060 * | 0.024 | −0.133 *** | 0.251 *** | 0.280 *** | −0.012 | −0.001 | 0.051 * | 0.390 *** | 0.109 *** | 0.137 *** | 0.024 | 0.134 *** | ||
| 14. Trust in experts | 0.171 *** | 0.121 *** | −0.022 | −0.045 | −0.050 | 0.022 | 0.055 * | 0.077 ** | 0.335 *** | −0.012 | 0.049 | 0.094 *** | 0.108 *** | 0.198 *** | −0.034 | 0.069 *** | ||
| 15. Trust in science | 0.133 *** | 0.170 *** | 0.05 | −0.034 | −0.034 | 0.107 *** | 0.126 *** | 0.099 *** | 0.131 *** | −0.008 | 0.017 | 0.155 *** | 0.117 *** | 0.196 *** | 0.001 | 0.141 *** | ||
| 16. Negative affect | 0.194 *** | 0.041 | −0.031 | 0.099 *** | 0.595 *** | −0.029 | 0.167 *** | 0.256 *** | 0.057 * | −0.030 | 0.364 *** | 0.169 *** | 0.012 | −0.027 | −0.008 | 0.128 *** | ||
| 17. Knowledge | 0.254 *** | 0.169 *** | −0.065 * | 0.103 *** | 0.172 *** | 0.035 | 0.205 *** | 0.142 *** | 0.114 *** | 0.052 * | 0.143 *** | 0.198 *** | 0.155 *** | 0.070 ** | 0.162 *** | 0.128 *** | ||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Beta | B | SE | Beta | B | SE | Beta | B | SE | Beta | ||
| F1: Sociodemographic Factors | Constant | 2.821 | 0.105 | 1.401 | 0.158 | 1.087 | 0.138 | 0.779 | 0.162 | ||||
| Gender (female) | 0.200 *** | 0.027 | 0.183 | 0.155 *** | 0.025 | 0.142 | 0.195 **** | 0.025 | 0.178 | 0.174 *** | 0.024 | 0.159 | |
| Age | 0.006 *** | 0.001 | 0.153 | 0.004 *** | 0.001 | 0.099 | 0.004 *** | 0.001 | 0.113 | 0.003 ** | 0.001 | 0.086 | |
| Household income | 0.058 * | 0.030 | 0.049 | 0.043 | 0.028 | 0.036 | 0.024 | 0.028 | 0.020 | 0.021 | 0.026 | 0.017 | |
| Education level | 0.109 *** | 0.029 | 0.100 | 0.073 *** | 0.027 | 0.066 | 0.060 ** | 0.027 | 0.055 | 0.520 * | 0.026 | 0.047 | |
| No. of children | 0.047 | 0.032 | 0.039 | 0.048 | 0.029 | 0.040 | 0.035 | 0.029 | 0.029 | 0.037 | 0.028 | 0.031 | |
| No. of elderly people | 0.097 *** | 0.033 | 0.088 | 0.128 *** | 0.030 | 0.116 | 0.080 *** | 0.030 | 0.073 | 0.100 ** | 0.029 | 0.091 | |
| Ideology (progressive) | 0.025 *** | 0.008 | 0.082 | 0.014 ** | 0.007 | 0.047 | −0.006 | 0.007 | −0.019 | −0.005 | 0.007 | −0.017 | |
| Health status change after COVID-19 | 0.047 *** | 0.017 | 0.073 | 0.070 *** | 0.016 | 0.108 | 0.022 | 0.016 | 0.034 | 0.057 *** | 0.016 | 0.087 | |
| F2: Health Belief Factors | Perceived susceptibility | −0.048 *** | 0.016 | −0.072 | 0.052 ** | 0.016 | −0.078 | ||||||
| Perceived severity | 0.077 *** | 0.017 | 0.112 | 0.030 | 0.021 | 0.044 | |||||||
| Perceived barriers | −0.028 | 0.019 | −0.037 | −0.030 * | 0.018 | −0.039 | |||||||
| Perceived benefit | 0.065 *** | 0.018 | 0.086 | 0.025 | 0.018 | 0.033 | |||||||
| Self-efficacy | 0.228 *** | 0.020 | 0.300 | 0.175 *** | 0.019 | 0.230 | |||||||
| Media exposure | 0.069 *** | 0.016 | 0.098 | 0.031 * | 0.016 | 0.044 | |||||||
| Knowing a confirmed case | −0.019 | 0.072 | −0.006 | −0.030 | 0.068 | −0.009 | |||||||
| F3: Psychometric Factors | Risk perception | 0.081 *** | 0.016 | 0.132 | 0.074 *** | 0.016 | 0.120 | ||||||
| Benefit perception | 0.121 *** | 0.017 | 0.182 | 0.081 *** | 0.017 | 0.122 | |||||||
| Trust in government | 0.086 *** | 0.016 | 0.138 | 0.067 *** | 0.016 | 0.107 | |||||||
| Trust in experts | 0.062 *** | 0.015 | 0.094 | 0.049 ** | 0.015 | 0.094 | |||||||
| Trust in science | 0.027 | 0.017 | 0.037 | 0.016 | 0.017 | 0.022 | |||||||
| Negative affect | 0.050 *** | 0.016 | 0.076 | 0.002 | 0.018 | 0.003 | |||||||
| Knowledge | 0.129 *** | 0.020 | 0.154 | 0.119 *** | 0.019 | 0.142 | |||||||
| Beliefs in conspiracy theories | −0.009 | 0.019 | −0.012 | 0.052 *** | 0.019 | 0.071 | 0.047 ** | 0.018 | 0.063 | 0.077 *** | 0.018 | 0.104 | |
| F-value | 15.300 *** | 30.065 *** | 32.696 *** | 30.586 *** | |||||||||
| R2/Adjusted R2 | 0.083/0.078 | 0.242/0.234 | 0.258/0.250 | 0.320/0.309 | |||||||||
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | Beta | B | SE | Beta | B | SE | Beta | B | SE | Beta | ||
| F1: Sociodemographic Factors | Constant | 1.728 | 0.151 | 0.908 | 0.242 | 0.481 | 0.212 | 0.212 | 0.255 | ||||
| Gender (female) | −0.064 * | 0.039 | −0.041 | −0.051 | 0.038 | −0.033 | −0.047 | 0.038 | −0.030 | −0.023 | 0.038 | −0.014 | |
| Age | 0.003 * | 0.002 | 0.056 | 0.003 * | 0.002 | 0.052 | 0.001 | 0.002 | 0.026 | 0.002 | 0.002 | 0.035 | |
| Household income | 0.110 ** | 0.043 | 0.064 | 0.097 ** | 0.043 | 0.056 | 0.068 | 0.042 | 0.040 | 0.063 | 0.042 | 0.036 | |
| Education level | −0.094 ** | 0.042 | −0.060 | −0.092 ** | 0.041 | −0.059 | −0.118 *** | 0.041 | −0.075 | −0.108 *** | 0.040 | −0.069 | |
| No. of children | 0.087 ** | 0.046 | 0.051 | 0.098 ** | 0.045 | 0.057 | 0.085 * | 0.044 | 0.049 | 0.092 ** | 0.044 | 0.053 | |
| No. of elderly people | 0.061 * | 0.047 | 0.038 | 0.077 * | 0.046 | 0.049 | 0.026 | 0.046 | 0.017 | 0.033 | 0.046 | 0.021 | |
| Ideology (progressive) | 0.013 | 0.011 | 0.030 | 0.006 | 0.011 | 0.014 | −0.006 | 0.011 | −0.013 | −0.010 | 0.011 | −0.023 | |
| Health status change after COVID-19 | 0.175 *** | 0.024 | 0.188 | 0.104 *** | 0.025 | 0.111 | 0.134 *** | 0.024 | 0.144 | 0.082 *** | 0.025 | 0.088 | |
| F2: Health Belief Factors | Perceived susceptibility | 0.122 *** | 0.025 | 0.129 | 0.116 *** | 0.025 | 0.122 | ||||||
| Perceived severity | 0.059 ** | 0.026 | 0.059 | 0.025 | 0.032 | 0.026 | |||||||
| Perceived barriers | 0.132 *** | 0.029 | 0.121 | 0.113 *** | 0.028 | 0.104 | |||||||
| Perceived benefit | 0.047 * | 0.028 | 0.043 | 0.004 | 0.028 | 0.003 | |||||||
| Self-efficacy | −0.053 * | 0.030 | −0.049 | −0.102 *** | 0.030 | −0.093 | |||||||
| Media exposure | 0.095 *** | 0.025 | 0.094 | 0.040 | 0.026 | 0.039 | |||||||
| Knowing a confirmed case | 0.000 | 0.110 | 0.000 | −0.004 | 0.107 | −0.001 | |||||||
| F3: Psychometric Factors | Risk perception | 0.131 *** | 0.024 | 0.149 | 0.106 *** | 0.025 | 0.120 | ||||||
| Benefit perception | −0.012 | 0.026 | −0.013 | 0.022 | 0.026 | 0.023 | |||||||
| Trust in government | 0.043 * | 0.025 | 0.048 | 0.059 ** | 0.025 | 0.066 | |||||||
| Trust in experts | 0.072 *** | 0.023 | 0.077 | 0.067 *** | 0.024 | 0.071 | |||||||
| Trust in science | 0.121 *** | 0.026 | 0.116 | 0.119 *** | 0.026 | 0.113 | |||||||
| Negative affect | −0.028 | 0.025 | −0.030 | −0.022 | 0.029 | −0.023 | |||||||
| Knowledge | 0.148 *** | 0.030 | 0.123 | 0.130 *** | 0.030 | 0.107 | |||||||
| Beliefs in conspiracy theories | 0.136 *** | 0.028 | 0.128 | 0.082 *** | 0.029 | 0.077 | 0.141 *** | 0.028 | 0.133 | 0.092 *** | 0.029 | 0.087 | |
| F-value | 15.265 | 14.636 | 16.842 | 15.128 *** | |||||||||
| R2/Adjusted R2 | 0.083/0.078 | 0.135/0.125 | 0.152/0.143 | 0.189/0.176 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.; Kim, S. The Paradox of Conspiracy Theory: The Positive Impact of Beliefs in Conspiracy Theories on Preventive Actions and Vaccination Intentions during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11825. https://doi.org/10.3390/ijerph182211825
Wang J, Kim S. The Paradox of Conspiracy Theory: The Positive Impact of Beliefs in Conspiracy Theories on Preventive Actions and Vaccination Intentions during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(22):11825. https://doi.org/10.3390/ijerph182211825
Chicago/Turabian StyleWang, Jaesun, and Seoyong Kim. 2021. "The Paradox of Conspiracy Theory: The Positive Impact of Beliefs in Conspiracy Theories on Preventive Actions and Vaccination Intentions during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 22: 11825. https://doi.org/10.3390/ijerph182211825
APA StyleWang, J., & Kim, S. (2021). The Paradox of Conspiracy Theory: The Positive Impact of Beliefs in Conspiracy Theories on Preventive Actions and Vaccination Intentions during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(22), 11825. https://doi.org/10.3390/ijerph182211825