
Performance of Professional Soccer Players before and after COVID-19 Infection; Observational Study with an Emphasis on Graduated Return to Play

 ,
,  ,
,  ,
, 
 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
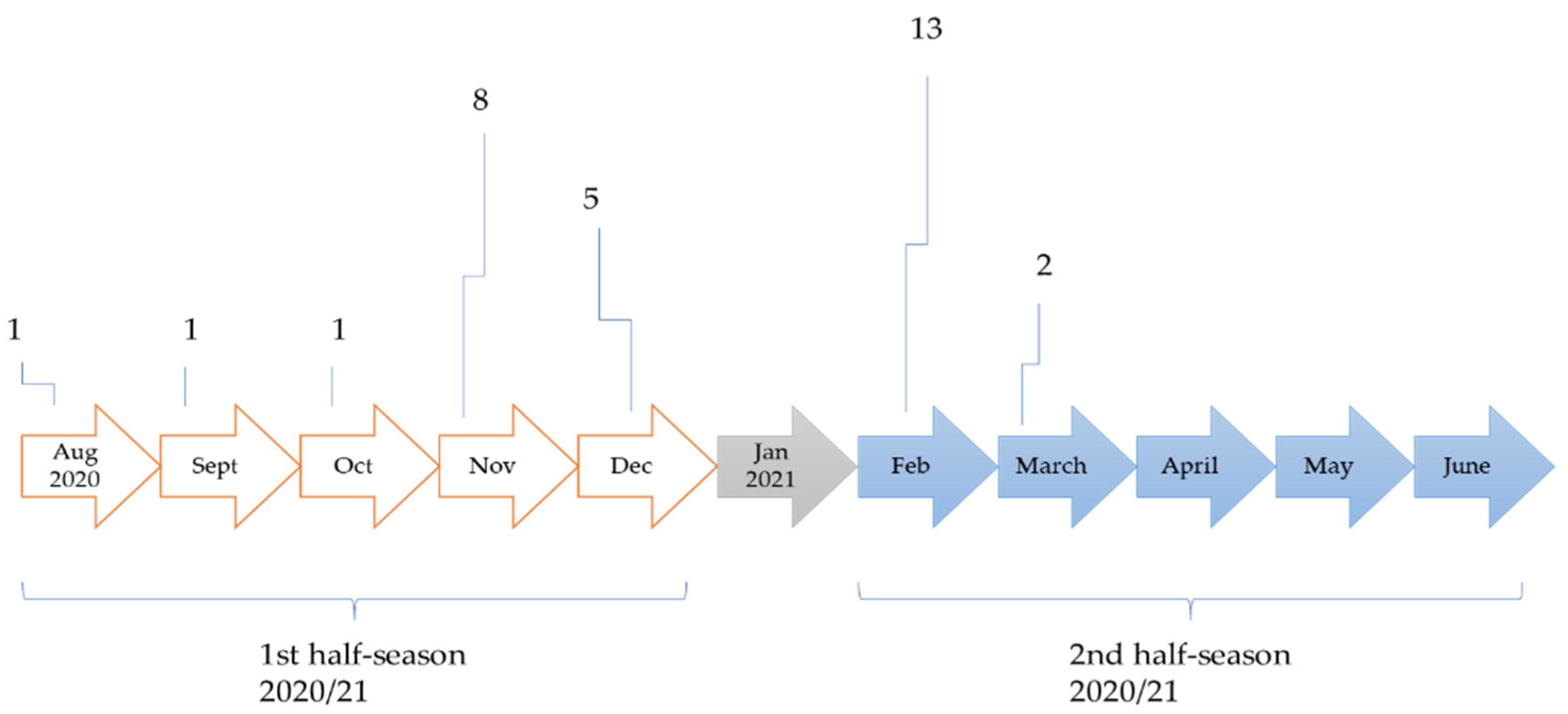
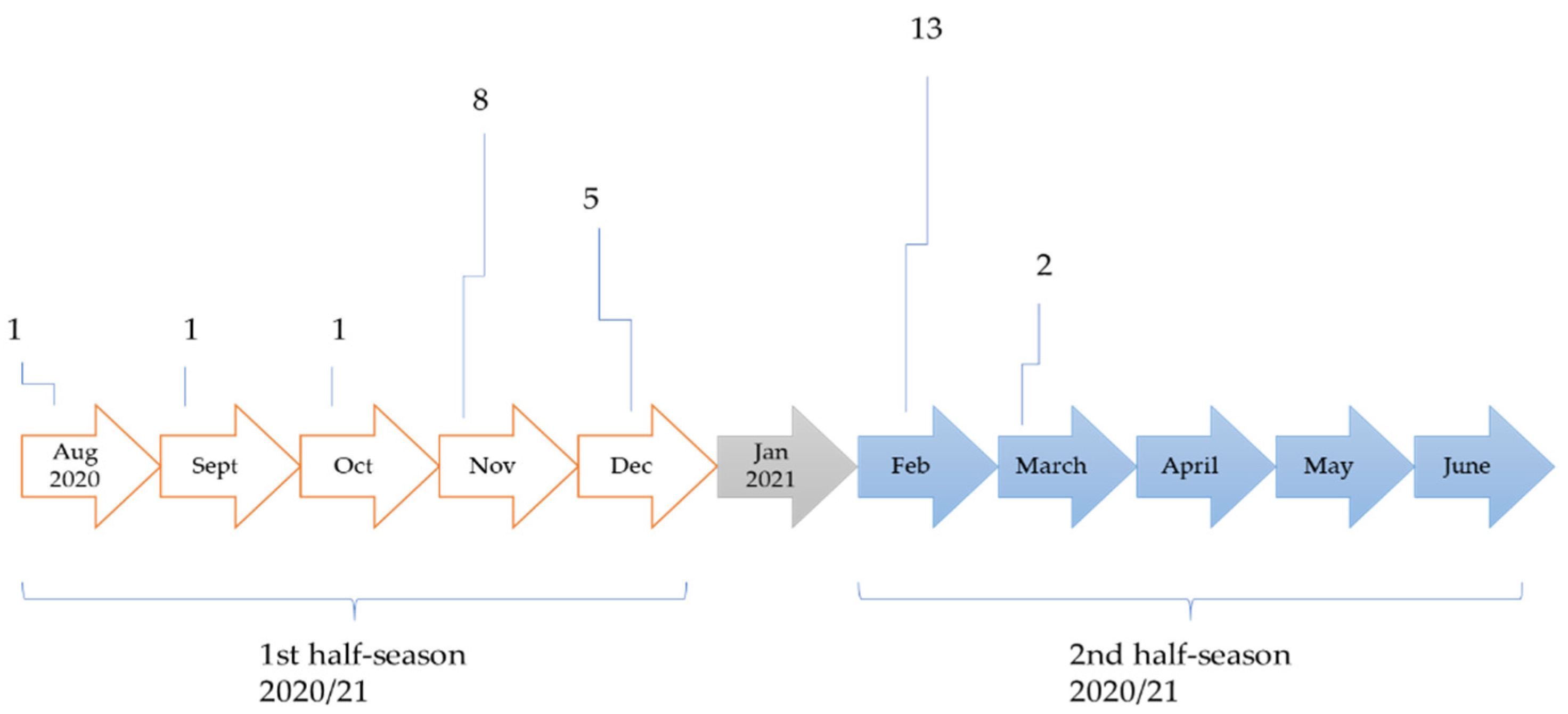
4.1. COVID Prevalence
4.2. Return to Play
4.3. Match Running Performance in Pre-COVID and Post-COVID Period
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blandenier, E.; Habibi, Z.; Kousi, T.; Sestito, P.; Flahault, A.; Rozanova, L. Initial COVID-19 Outbreak: An Epidemiological and Socioeconomic Case Review of Iran. Int. J. Environ. Res. Public Health 2020, 17, 9593. [Google Scholar] [CrossRef]
- Lemenager, T.; Neissner, M.; Koopmann, A.; Reinhard, I.; Georgiadou, E.; Muller, A.; Kiefer, F.; Hillemacher, T. COVID-19 Lockdown Restrictions and Online Media Consumption in Germany. Int. J. Environ. Res. Public Health 2020, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Turcu-Stiolica, A.; Bogdan, M.; Subtirelu, M.-S.; Meca, A.-D.; Taerel, A.-E.; Iaru, I.; Kamusheva, M.; Petrova, G. Influence of COVID-19 on Health-Related Quality of Life and the Perception of Being Vaccinated to Prevent COVID-19: An Approach for Community Pharmacists from Romania and Bulgaria. J. Clin. Med. 2021, 10, 864. [Google Scholar] [CrossRef]
- Rueckel, J.; Fink, N.; Kaestle, S.; Stüber, T.; Schwarze, V.; Gresser, E.; Hoppe, B.F.; Rudolph, J.; Kunz, W.G.; Ricke, J. COVID-19 Pandemic and Upcoming Influenza Season—Does an Expert’s Computed Tomography Assessment Differentially Identify COVID-19, Influenza and Pneumonias of Other Origin? J. Clin. Med. 2021, 10, 84. [Google Scholar] [CrossRef]
- Tayech, A.; Mejri, M.A.; Makhlouf, I.; Mathlouthi, A.; Behm, D.G.; Chaouachi, A. Second Wave of COVID-19 Global Pandemic and Athletes’ Confinement: Recommendations to Better Manage and Optimize the Modified Lifestyle. Int. J. Environ. Res. Public Health 2020, 17, 8385. [Google Scholar] [CrossRef] [PubMed]
- Hauer, R.; Tessitore, A.; Knaus, R.; Tschan, H. Lacrosse Athletes Load and Recovery Monitoring: Comparison between Objective and Subjective Methods. Int. J. Environ. Res. Public Health 2020, 17, 3329. [Google Scholar] [CrossRef] [PubMed]
- Krzywański, J.; Mikulski, T.; Krysztofiak, H.; Pokrywka, A.; Młyńczak, M.; Małek, Ł.A.; Kwiatkowska, D.; Kuchar, E. Elite athletes with COVID-19—Predictors of the course of disease. J. Sci. Med. Sport 2021. [Google Scholar] [CrossRef]
- Khan, Z.; Na, J.S.; Jerome, S. Review of COVID-19 Myocarditis in Competitive Athletes: Legitimate Concern or Fake News? Front. Cardiovasc. Med. 2021, 8, 689. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Alvarez, K.N.; Weissfeld, L.A.; Angus, D.C.; Chirinos, J.A.; Chang, C.-C.H.; Newman, A.; Loehr, L.; Folsom, A.R.; Elkind, M.S. Association between hospitalization for pneumonia and subsequent risk of cardiovascular disease. JAMA 2015, 313, 264–274. [Google Scholar] [CrossRef]
- Martinez, M.W.; Tucker, A.M.; Bloom, O.J.; Green, G.; DiFiori, J.P.; Solomon, G.; Phelan, D.; Kim, J.H.; Meeuwisse, W.; Sills, A.K. Prevalence of inflammatory heart disease among professional athletes with prior COVID-19 infection who received systematic return-to-play cardiac screening. JAMA Cardiol. 2021, 6, 745–752. [Google Scholar] [CrossRef]
- Moulson, N.; Petek, B.J.; Drezner, J.A.; Harmon, K.G.; Kliethermes, S.A.; Patel, M.R.; Baggish, A.L. SARS-CoV-2 cardiac involvement in young competitive athletes. Circulation 2021, 144, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Schwellnus, M.; Sewry, N.; Snyders, C.; Kaulback, K.; Wood, P.S.; Seocharan, I.; Derman, W.; Hull, J.H.; Valtonen, M.; Jordaan, E. Symptom cluster is associated with prolonged return-to-play in symptomatic athletes with acute respiratory illness (including COVID-19): A cross-sectional study—AWARE study I. Br. J. Sports Med. 2021, 55, 1144–1152. [Google Scholar] [CrossRef]
- García-Aliaga, A.; Marquina, M.; Cordón-Carmona, A.; Sillero-Quintana, M.; de la Rubia, A.; Refoyo Román, I. Comparative Analysis of Soccer Performance Intensity of the Pre-Post-Lockdown COVID-19 in LaLiga™. Int. J. Environ. Res. Public Health 2021, 18, 3685. [Google Scholar] [CrossRef] [PubMed]
- Radzimiński, Ł.; Padrón-Cabo, A.; Konefał, M.; Chmura, P.; Szwarc, A.; Jastrzębski, Z. The Influence of COVID-19 Pandemic Lockdown on the Physical Performance of Professional Soccer Players: An Example of German and Polish Leagues. Int. J. Environ. Res. Public Health 2021, 18, 8796. [Google Scholar] [CrossRef]
- Małek, Ł.A.; Marczak, M.; Miłosz-Wieczorek, B.; Konopka, M.; Braksator, W.; Drygas, W.; Krzywański, J. Cardiac involvement in consecutive elite athletes recovered from COVID-19: A magnetic resonance study. J. Magn. Reson. Imaging 2021, 53, 1723–1729. [Google Scholar] [CrossRef]
- Milovancev, A.; Avakumovic, J.; Lakicevic, N.; Stajer, V.; Korovljev, D.; Todorovic, N.; Bianco, A.; Maksimovic, N.; Ostojic, S.; Drid, P. Cardiorespiratory Fitness in Volleyball Athletes Following a COVID-19 Infection: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4059. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Levine, B.D.; Phelan, D.; Emery, M.S.; Martinez, M.W.; Chung, E.H.; Thompson, P.D.; Baggish, A.L. Coronavirus disease 2019 and the athletic heart: Emerging perspectives on pathology, risks, and return to play. JAMA Cardiol. 2021, 6, 219–227. [Google Scholar] [CrossRef]
- McKinney, J.; Connelly, K.A.; Dorian, P.; Fournier, A.; Goodman, J.M.; Grubic, N.; Isserow, S.; Moulson, N.; Philippon, F.; Pipe, A. COVID-19—Myocarditis and Return to Play: Reflections and Recommendations From a Canadian Working Group. Can. J. Cardiol. 2020, 37, 1165–1174. [Google Scholar] [CrossRef]
- Bhatia, R.T.; Marwaha, S.; Malhotra, A.; Iqbal, Z.; Hughes, C.; Börjesson, M.; Niebauer, J.; Pelliccia, A.; Schmied, C.; Serratosa, L. Exercise in the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) era: A question and answer session with the experts endorsed by the section of Sports Cardiology & Exercise of the European Association of Preventive Cardiology (EAPC). Eur. J. Prev. Cardiol. 2020, 27, 1242–1251. [Google Scholar]
- Wilson, M.G.; Hull, J.H.; Rogers, J.; Pollock, N.; Dodd, M.; Haines, J.; Harris, S.; Loosemore, M.; Malhotra, A.; Pieles, G. Cardiorespiratory considerations for return-to-play in elite athletes after COVID-19 infection: A practical guide for sport and exercise medicine physicians. Br. J. Sports Med. 2020, 54, 1157–1161. [Google Scholar] [CrossRef]
- Elliott, N.; Martin, R.; Heron, N.; Elliott, J.; Grimstead, D.; Biswas, A. Infographic. Graduated return to play guidance following COVID-19 infection. Br. J. Sports Med. 2020, 54, 1174–1175. [Google Scholar] [CrossRef]
- Schellhorn, P.; Klingel, K.; Burgstahler, C. Return to sports after COVID-19 infection. Eur. Heart J. 2020, 41, 4382–4384. [Google Scholar] [CrossRef]
- Mohr, M.; Nassis, G.P.; Brito, J.; Randers, M.B.; Castagna, C.; Parnell, D.; Krustrup, P. Return to elite football after the COVID-19 lockdown. Manag. Sport Leis. 2020, 25, 1–9. [Google Scholar] [CrossRef]
- Lolli, L.; Batterham, A.M.; Hawkins, R.; Kelly, D.M.; Strudwick, A.J.; Thorpe, R.T.; Gregson, W.; Atkinson, G. The Acute-to-Chronic Workload Ratio: An Inaccurate Scaling Index for An Unnecessary Normalisation Process? Br. J. Sports Med. 2019, 53, 1510–1512. [Google Scholar] [CrossRef] [PubMed]
- Castellano, J.; Casamichana, D.; Calleja-González, J.; San Román, J.; Ostojic, S.M. Reliability and accuracy of 10 Hz GPS devices for short-distance exercise. J. Sports Sci. Med. 2011, 10, 233. [Google Scholar] [PubMed]
- Johnston, R.J.; Watsford, M.L.; Kelly, S.J.; Pine, M.J.; Spurrs, R.W. Validity and interunit reliability of 10 Hz and 15 Hz GPS units for assessing athlete movement demands. J. Strength Cond. Res. 2014, 28, 1649–1655. [Google Scholar] [CrossRef]
- Stevens, T.G.; de Ruiter, C.J.; Twisk, J.W.; Savelsbergh, G.J.; Beek, P.J. Quantification of in-season training load relative to match load in professional Dutch Eredivisie football players. Sci. Med. Footb. 2017, 1, 117–125. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Available online: https://www.koronavirus.hr/en (accessed on 15 October 2021).
- Mack, D.; Gärtner, B.C.; Rössler, A.; Kimpel, J.; Donde, K.; Harzer, O.; Krutsch, W.; von Laer, D.; Meyer, T. Prevalence of SARS-CoV-2 IgG antibodies in a large prospective cohort study of elite football players in Germany (May–June 2020): Implications for a testing protocol in asymptomatic individuals and estimation of the rate of undetected cases. Clin. Microbiol. Infect. 2021, 27, e471–e473. [Google Scholar] [CrossRef]
- Pedersen, L.; Lindberg, J.; Lind, R.R.; Rasmusen, H. Reopening elite sport during the COVID-19 pandemic: Experiences from a controlled return to elite football in Denmark. Scand. J. Med. Sci. Sports 2021, 31, 936–939. [Google Scholar] [CrossRef]
- Schumacher, Y.O.; Tabben, M.; Hassoun, K.; Al Marwani, A.; Al Hussein, I.; Coyle, P.; Abbassi, A.K.; Ballan, H.T.; Al-Kuwari, A.; Chamari, K. Resuming professional football (soccer) during the COVID-19 pandemic in a country with high infection rates: A prospective cohort study. Br. J. Sports Med. 2021, 55, 1092–1098. [Google Scholar] [CrossRef]
- Ibarrola, M.; Dávolos, I. Myocarditis in athletes after COVID-19 infection: The heart is not the only place to screen. Sports Med. Health Sci. 2020, 2, 172–173. [Google Scholar] [CrossRef] [PubMed]
- Van Hattum, J.C.; Spies, J.L.; Verwijs, S.M.; Verwoert, G.C.; Planken, R.N.; Boekholdt, S.M.; Groenink, M.; Malekzadeh, A.; Pinto, Y.M.; Wilde, A.A.M.; et al. Cardiac abnormalities in athletes after SARS-CoV-2 infection: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e001164. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, F.M.; Franchi, M.V.; Sarto, F.; Meyer, T.; Coutts, A.J. Sharing Information Is Probably More Helpful than Providing Generic Training Recommendations on Return to Play after COVID-19 Home Confinement; Taylor & Francis: Abingdon, UK, 2020. [Google Scholar]
- Modric, T.; Versic, S.; Sekulic, D. Does aerobic performance define match running performance among professional soccer players? A position-specific analysis. Res. Sports Med. 2021, 29, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.M.; Rabbani, A.; Conte, D.; Castillo, D.; Afonso, J.; Clark, T.; Craig, C.; Nikolaidis, P.T.; Rosemann, T.; Knechtle, B. Training/Match External Load Ratios in Professional Soccer Players: A Full-Season Study. Int. J. Environ. Res. Public Health 2019, 16, 3057. [Google Scholar] [CrossRef] [Green Version]
- Purdam, C.; Drew, M.; Blanch, P.; Champman, D.; Gabbett, T.; Gore, C.; Hugues, D.; Kelly, T.; Mitchell, J.; Rice, T. Prescription of Training Load in Relation to Loading and Unloading Phases of Training; Australian Sports Commission: Bruce, Australia, 2015.
- Modric, T.; Versic, S.; Sekulic, D. Relations of the Weekly External Training Load Indicators and Running Performances in Professional Soccer Matches. Sport Mont 2021, 19, 31–37. [Google Scholar]
- Modric, T.; Versic, S.; Sekulic, D. Playing position specifics of associations between running performance during the training and match in male soccer players. Acta Gymnica 2020, 50, 51–60. [Google Scholar] [CrossRef]
- Modric, T.; Versic, S.; Sekulic, D.; Liposek, S. Analysis of the Association between Running Performance and Game Performance Indicators in Professional Soccer Players. Int. J. Environ. Res. Public Health 2019, 16, 4032. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
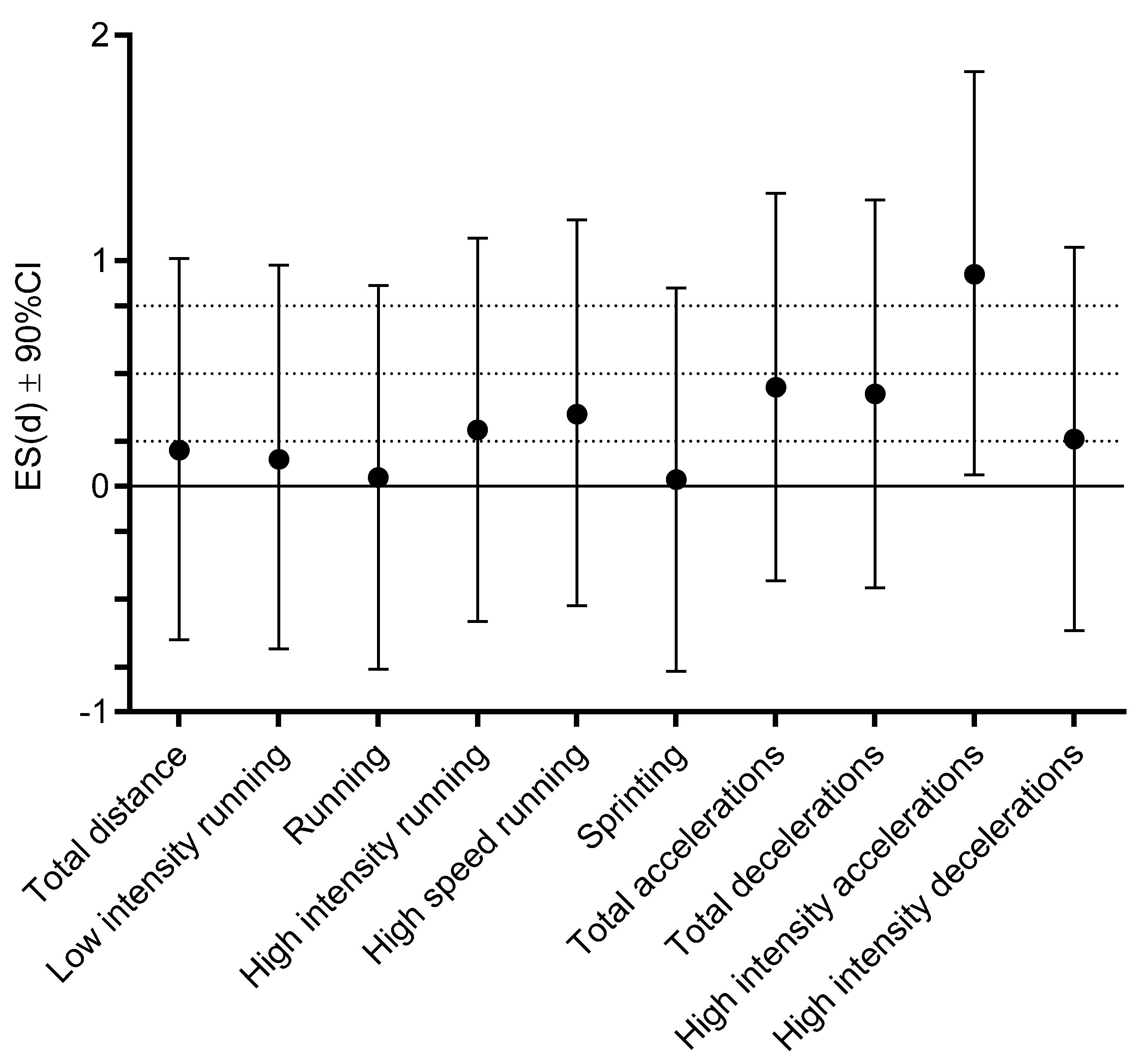
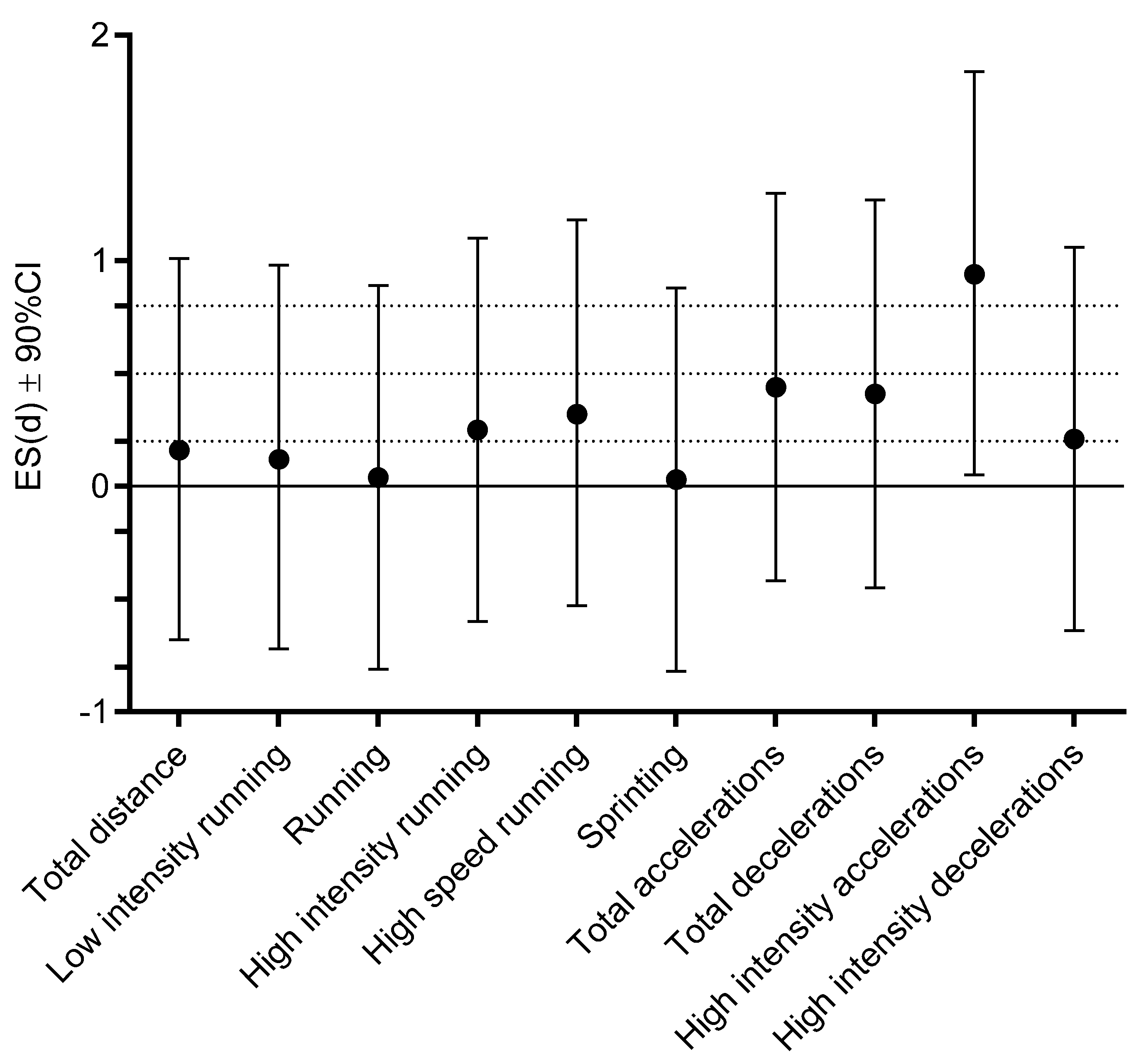
| NONINF | INF Pre-COVID | T-Test | ||||
|---|---|---|---|---|---|---|
| Mean | Std.Dev. | Mean | Std.Dev. | t-Test | p | |
| Total distance (m) | 10,776.08 | 566.27 | 10,651.16 | 918.15 | 0.41 | 0.69 |
| Low-intensity running (m) | 8518.35 | 421.05 | 8457.23 | 524.94 | 0.32 | 0.75 |
| Running (m) | 1562.42 | 280.76 | 1545.55 | 469.29 | 0.11 | 0.92 |
| High-intensity running (m) | 697.33 | 197.31 | 648.10 | 193.85 | 0.63 | 0.54 |
| High-speed running (m) | 572.44 | 160.10 | 524.16 | 135.83 | 0.82 | 0.42 |
| Sprinting (m) | 122.07 | 56.76 | 124.22 | 72.55 | −0.08 | 0.94 |
| Total accelerations (count) | 500.44 | 42.63 | 479.08 | 51.91 | 1.12 | 0.27 |
| Total decelerations (count) | 500.49 | 42.86 | 480.52 | 54.73 | 1.01 | 0.32 |
| High-intensity accelerations (count) | 18.87 | 8.55 | 28.68 | 11.56 | −2.39 | 0.03 |
| High-intensity decelerations (count) | 36.54 | 9.35 | 38.10 | 10.34 | −0.39 | 0.70 |
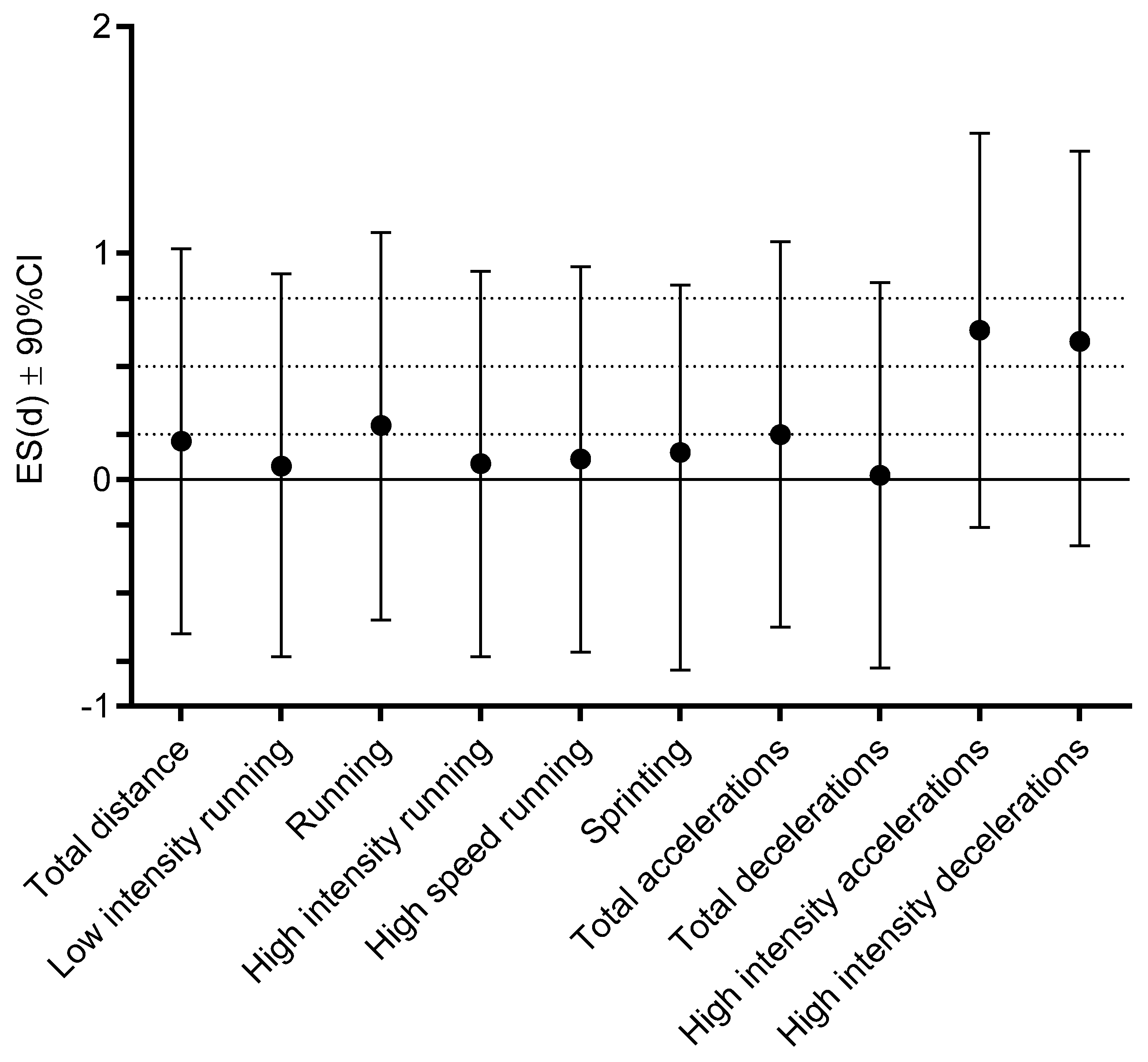
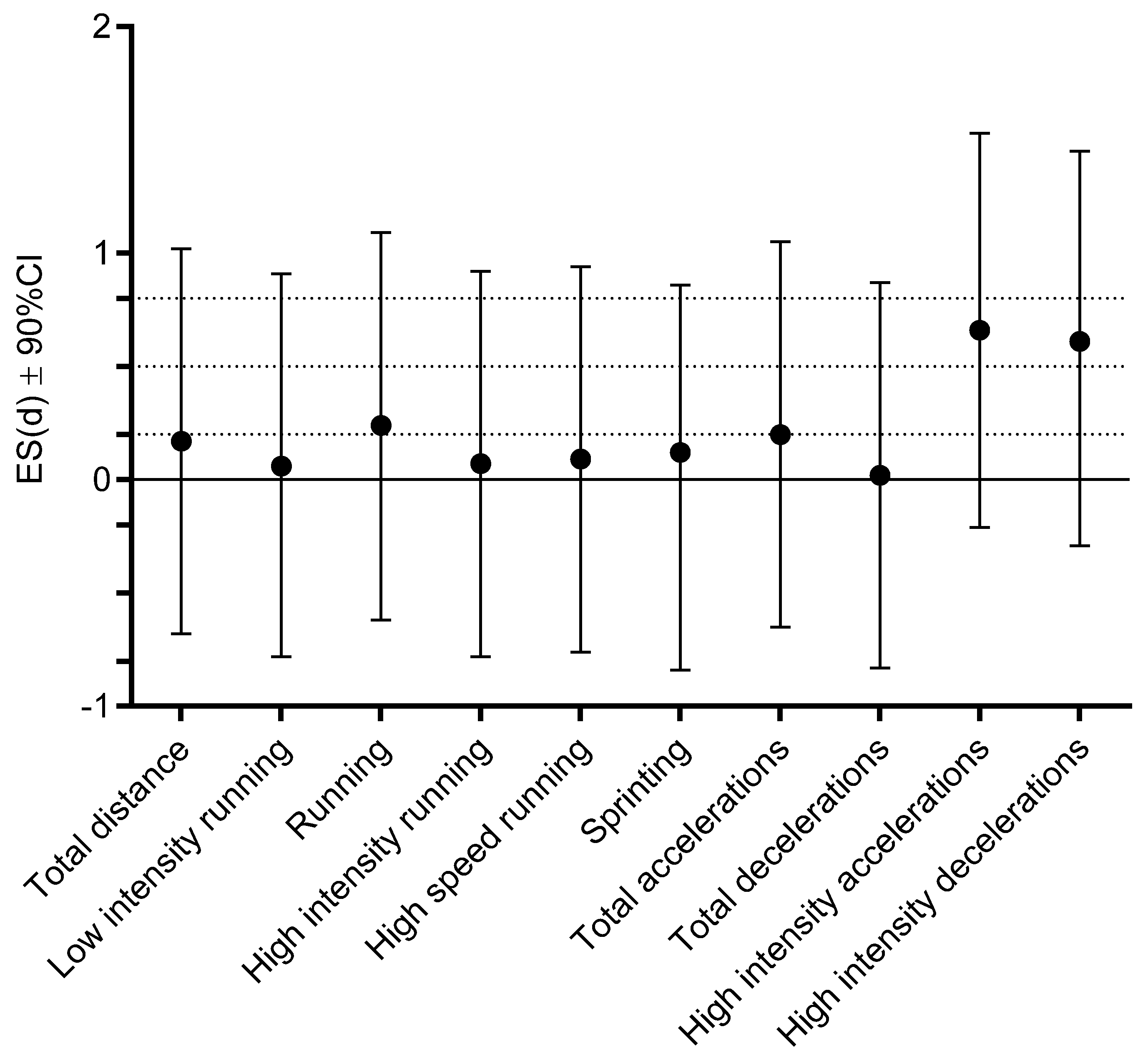
| Pre-COVID | Post-COVID | T-Test | ||||
|---|---|---|---|---|---|---|
| Mean | Std.Dev. | Mean | Std.Dev. | t-Test | p | |
| Total distance (m) | 10,651.16 | 918.15 | 10,799.96 | 765.13 | −1.02 | 0.32 |
| Low-intensity running (m) | 8457.23 | 524.94 | 8490.32 | 519.02 | −0.36 | 0.72 |
| Running (m) | 1545.55 | 469.29 | 1648.05 | 397.37 | −1.12 | 0.28 |
| High-intensity running (m) | 648.10 | 193.85 | 662.52 | 232.93 | −0.31 | 0.76 |
| High-speed running (m) | 524.16 | 135.83 | 538.72 | 161.38 | −0.42 | 0.68 |
| Sprinting (m) | 124.22 | 72.55 | 123.64 | 87.79 | 0.03 | 0.97 |
| Total accelerations (count) | 479.08 | 51.91 | 489.63 | 47.98 | −1.18 | 0.26 |
| Total decelerations (count) | 480.52 | 54.73 | 479.30 | 57.60 | 0.13 | 0.89 |
| High-intensity accelerations (count) | 28.68 | 11.56 | 21.22 | 10.83 | 2.11 | 0.04 |
| High-intensity decelerations (count) | 38.10 | 10.34 | 31.33 | 15.28 | 2.13 | 0.04 |
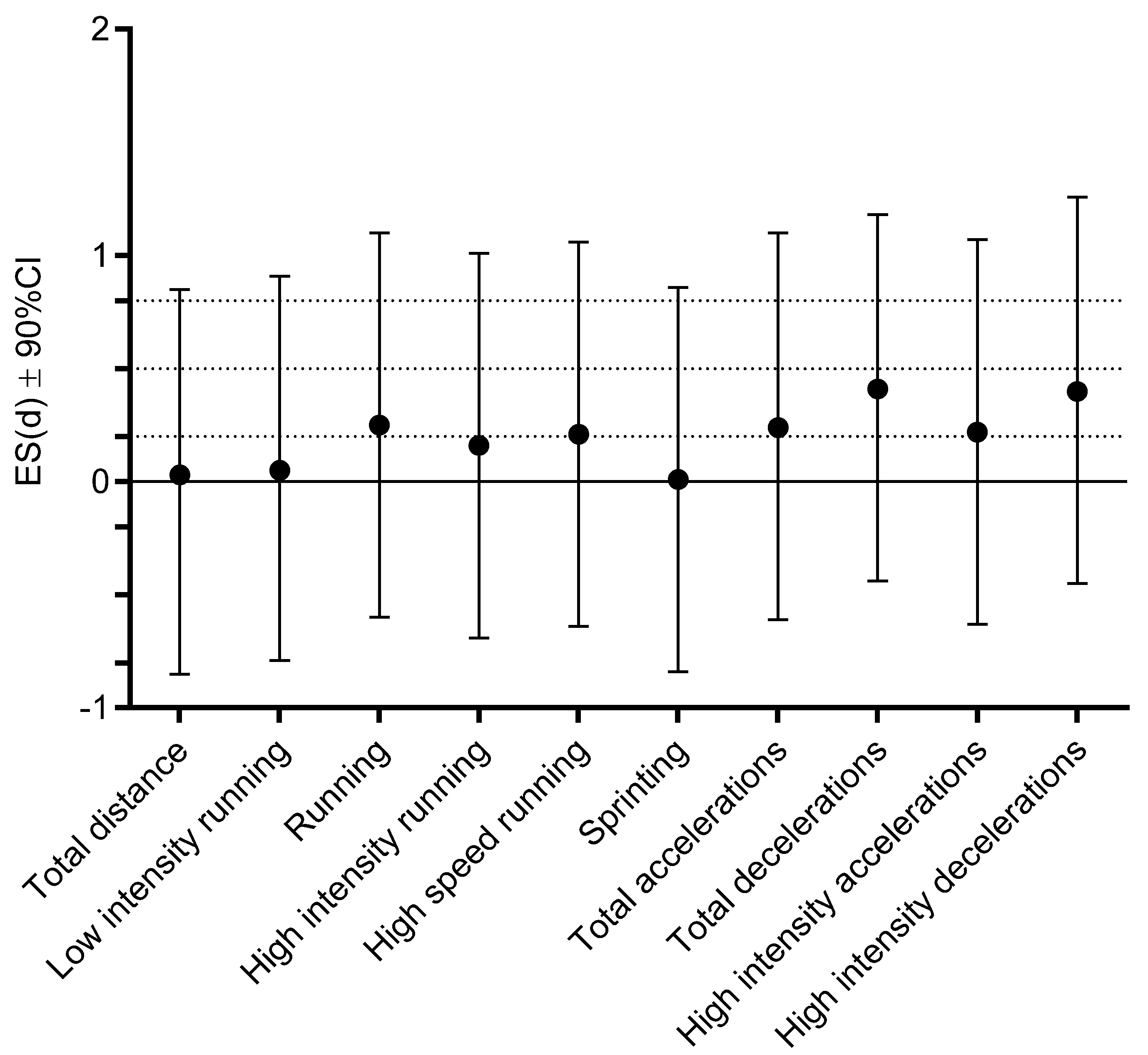
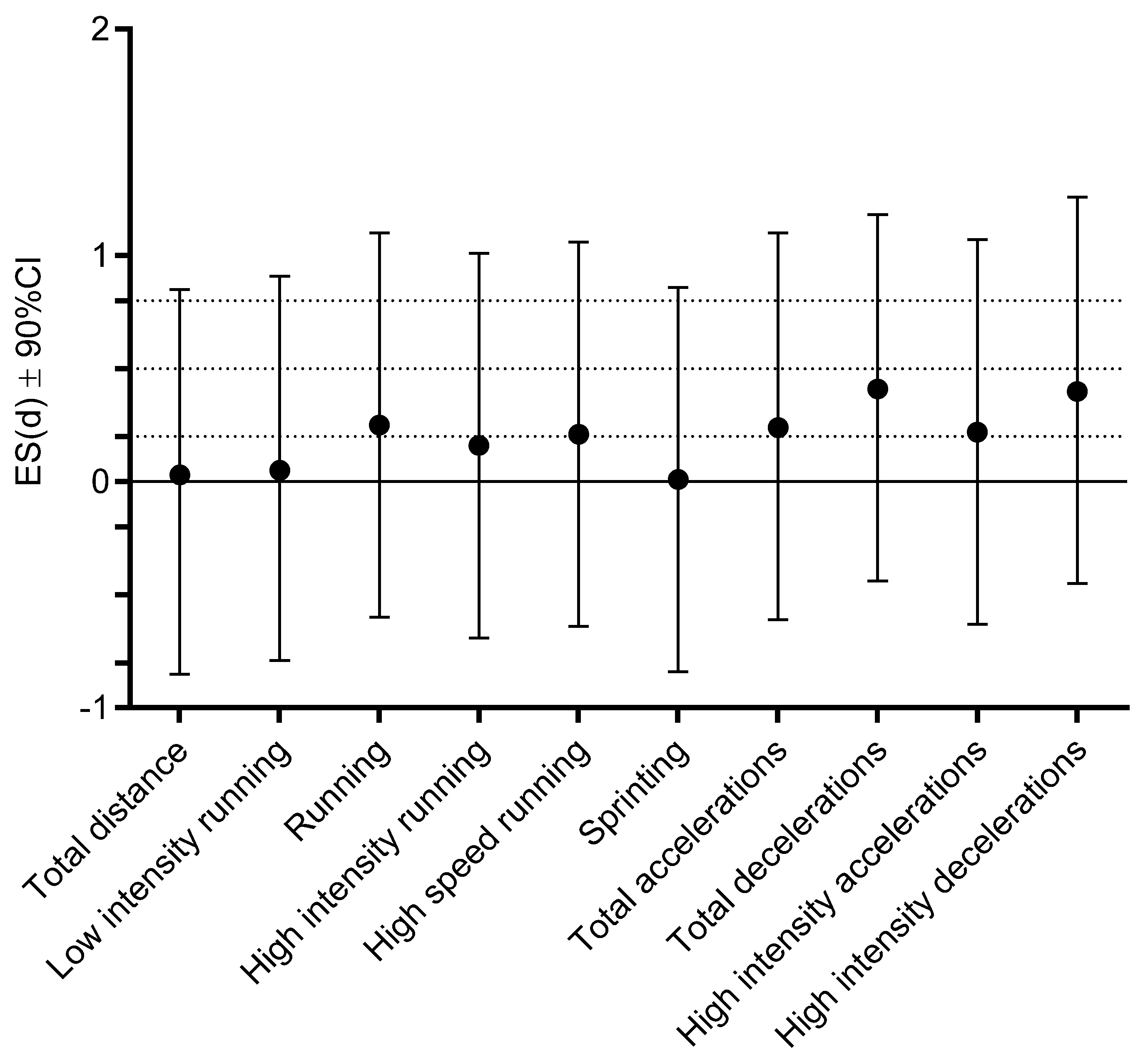
| NONINF | INF Post-COVID | T-Test | ||||
|---|---|---|---|---|---|---|
| Mean | Std.Dev. | Mean | Std.Dev. | t-Test | p | |
| Total distance (m) | 107,76.08 | 566.27 | 107,99.96 | 765.13 | −0.09 | 0.93 |
| Low-intensity running (m) | 8518.35 | 421.05 | 8490.32 | 519.02 | 0.15 | 0.88 |
| Running (m) | 1562.42 | 280.76 | 1648.05 | 397.37 | −0.62 | 0.54 |
| High-intensity running (m) | 697.33 | 197.31 | 662.52 | 232.93 | 0.40 | 0.69 |
| High-speed running (m) | 572.44 | 160.10 | 538.72 | 161.38 | 0.52 | 0.61 |
| Sprinting (m) | 122.07 | 56.76 | 123.64 | 87.79 | −0.05 | 0.96 |
| Total accelerations (count) | 500.44 | 42.63 | 489.63 | 47.98 | 0.59 | 0.56 |
| Total decelerations (count) | 500.49 | 42.86 | 479.30 | 57.60 | 1.04 | 0.31 |
| High-intensity accelerations (count) | 18.87 | 8.55 | 21.22 | 10.83 | −1.00 | 0.28 |
| High-intensity decelerations (count) | 36.54 | 9.35 | 31.33 | 15.28 | 0.62 | 0.54 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savicevic, A.J.; Nincevic, J.; Versic, S.; Cuschieri, S.; Bandalovic, A.; Turic, A.; Becir, B.; Modric, T.; Sekulic, D. Performance of Professional Soccer Players before and after COVID-19 Infection; Observational Study with an Emphasis on Graduated Return to Play. Int. J. Environ. Res. Public Health 2021, 18, 11688. https://doi.org/10.3390/ijerph182111688
Savicevic AJ, Nincevic J, Versic S, Cuschieri S, Bandalovic A, Turic A, Becir B, Modric T, Sekulic D. Performance of Professional Soccer Players before and after COVID-19 Infection; Observational Study with an Emphasis on Graduated Return to Play. International Journal of Environmental Research and Public Health. 2021; 18(21):11688. https://doi.org/10.3390/ijerph182111688
Chicago/Turabian StyleSavicevic, Anamarija Jurcev, Jasna Nincevic, Sime Versic, Sarah Cuschieri, Ante Bandalovic, Ante Turic, Boris Becir, Toni Modric, and Damir Sekulic. 2021. "Performance of Professional Soccer Players before and after COVID-19 Infection; Observational Study with an Emphasis on Graduated Return to Play" International Journal of Environmental Research and Public Health 18, no. 21: 11688. https://doi.org/10.3390/ijerph182111688
APA StyleSavicevic, A. J., Nincevic, J., Versic, S., Cuschieri, S., Bandalovic, A., Turic, A., Becir, B., Modric, T., & Sekulic, D. (2021). Performance of Professional Soccer Players before and after COVID-19 Infection; Observational Study with an Emphasis on Graduated Return to Play. International Journal of Environmental Research and Public Health, 18(21), 11688. https://doi.org/10.3390/ijerph182111688