
Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
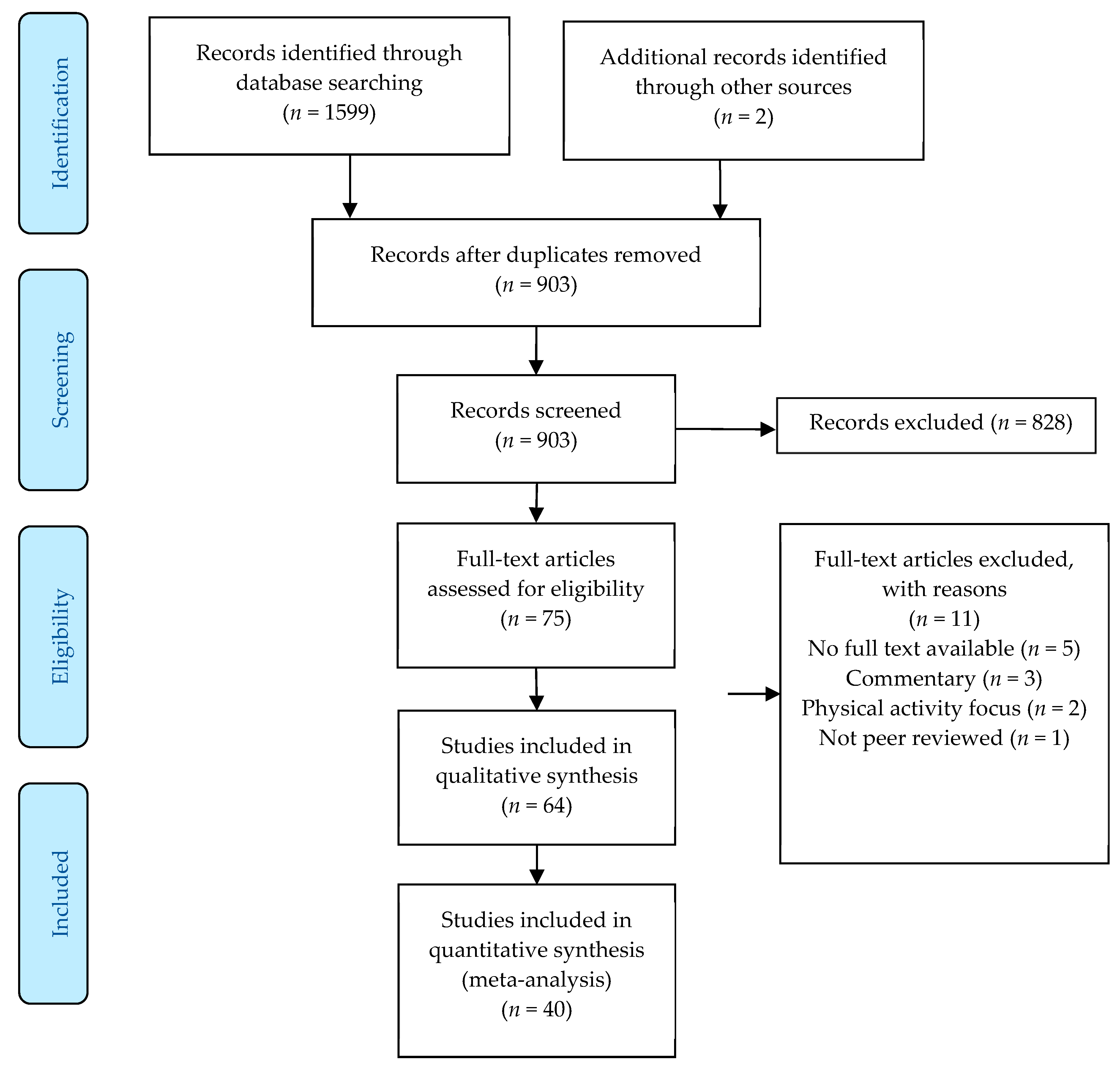
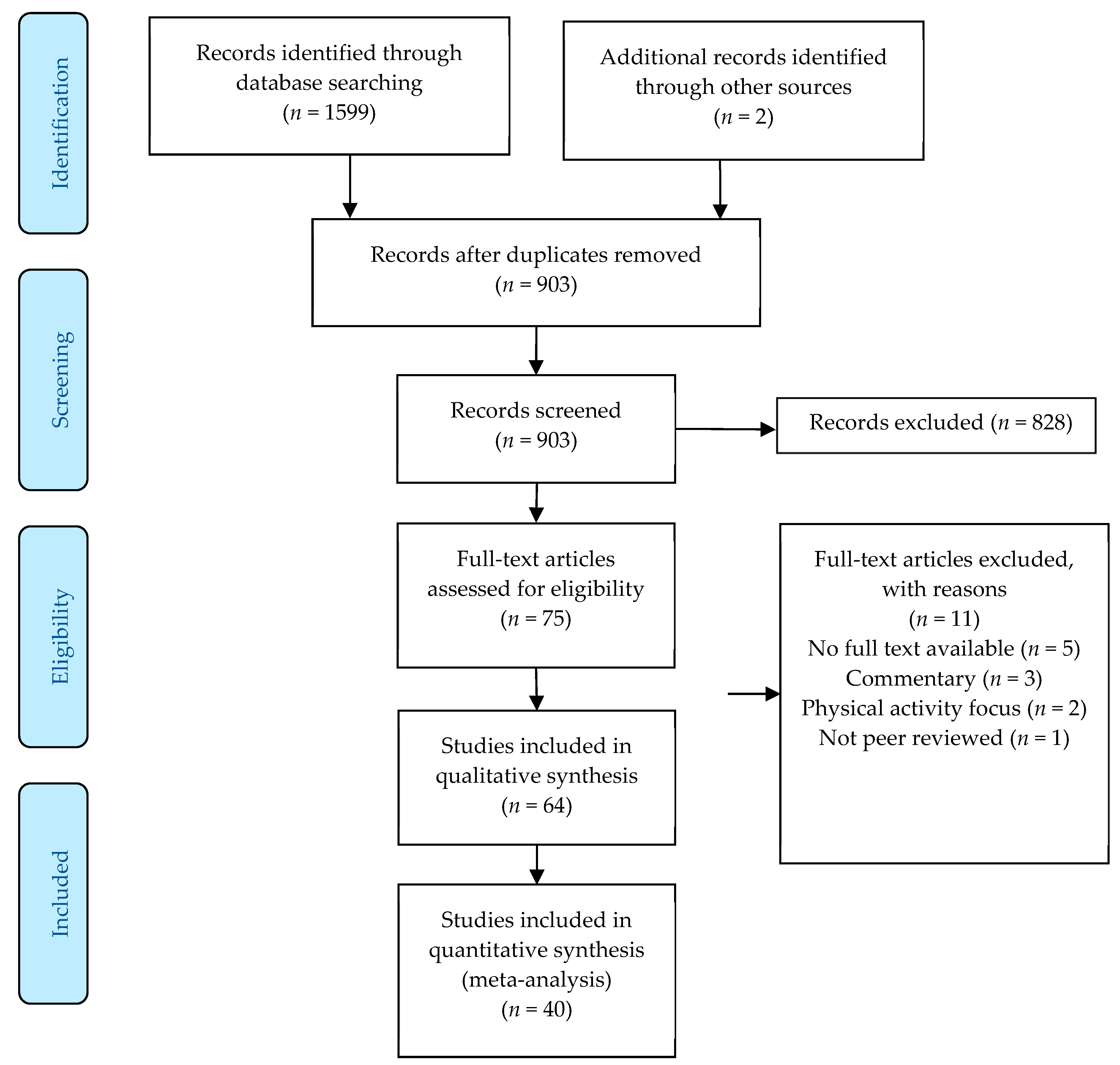
2. Methods
2.1. Search Strategy and Inclusion Criteria
2.2. Data Extraction, Quality Assessment, and Risk of Bias Appraisal
3. Results
4. Discussion
4.1. Children’s Sedentary Time
4.2. Adults and Older Adults
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saunders, T.J.; Chaput, J.P.; Tremblay, M.S. Sedentary behaviour as an emerging risk factor for cardiometabolic diseases in children and youth. Can. J. Diabetes 2014, 38, 53–61. [Google Scholar] [CrossRef] [Green Version]
- Väistö, J.; Haapala, E.; Viitasalo, A.; Schnurr, T.; Kilpeläinen, T.; Karjalainen, P.; Westgate, K.; Lakka, H.; Laaksonen, D.; Ekelund, U.; et al. Longitudinal associations of physical activity and sedentary time with cardiometabolic risk factors in children. Scand. J. Med. Sci. Sports 2019, 29, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Ku, P.; Steptoe, A.; Liao, Y.; Hsueh, M.; Chen, L. A cut-off of daily sedentary time and all cause mortality in adults: A meta-regression analysis involving more than one million participants. BMC Med. 2018, 16, 74. [Google Scholar] [CrossRef] [PubMed]
- Diaz, K.; Howard, V.; Hutto, B.; Colabianchi, N.; Vena, J.; Safford, M.; Blair, S.; Hooker, S. Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults: A National Cohort Study. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Leitzmann, M.F.; Jochem, C.; Schmid, D. (Eds.) Sedentary Behaviour Epidemiology; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Wilmot, E.; Edwardson, C.; Achana, F.; Davies, M.; Gorley, T.; Gray, L.; Khunti, K.; Yates, T.; Biddle, S. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.; Matthews, C.; Dunstan, D. Too much sitting: The population-health science of sedentary behaviour. Exerc. Sport Sci. Rev. 2010, 38, 105. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.; Fagerland, M.; Owen, N.; Powell, K.; Bauman, A.; Lee, I. Physical activity attenuates the detrimental association of sitting time with mortality: A harmonised meta-analysis of data from more than one million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Carson, V.; Tremblay, M.; Chaput, J.; McGregor, D.; Chastin, S. Compositional analyses of the associations between sedentary time, different intensities of physical activity, and cardiometaolic biomarkers among children and youth from the United States. PLoS ONE 2019, 14, e0220009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rideout, V.; Foehr, U.; Roberts, D. Generation M2: Media in the Lives of 8- to 18-Year-Olds. Available online: https://www.kff.org/other/event/generation-m2-media-in-the-lives-of/ (accessed on 1 December 2020).
- Leatherdale, S.; Ahmed, R. Screen-based sedentary behaviours among a nationally representative sample of youth: Are Canadian kids couch potatoes? Chronic Dis. Inj. Can. 2011, 31, 141–146. [Google Scholar] [CrossRef]
- Steene-Johannessen, J.; Hansen, B.; Dalene, K.; Kolle, E.; Northstone, K.; Møller, N.; Grøntved, A.; Wedderkopp, N.; Kriemler, S.; Page, A.; et al. Variations in accelerometry measured physical activity and sedentary time across Europe—Harmonized analyses of 47,497 children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Li, H.; Slapsinskaite, A.; Zhang, T.; Zhang, L.; Gui, C. Accelerometer-measured physical activity and sedentary behavior in Chinese children and adolescents: A systematic review and meta-analysis. Public Health 2020, 186, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.; Biddle, S.; Buman, M.; Chastin, S.; Ekelund, U.; Friedenreich, C.; Katzmarzyk, P.; Leitzmann, M.; Stamatakis, E.; van der Ploeg, H.; et al. New global guidelines on sedentary behaviour and health for adults: Broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Coronavirus Disease 2019 (COVID-19) Situation Report 51; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Dunford, D.; Dale, B.; Stylianou, N.; Lowther, E.; Ahmed, M.; de la Torre Areanas, I. Coronavirus: The World in Lockdown in Maps and Charts. Available online: https://www.bbc.com/news/world-52103747 (accessed on 6 April 2020).
- Caputo, E.; Reichert, F. Studies of Physical Activity and COVID-19 during the Pandemic: A Scoping Review. J. Phys. Act. Health 2020, 17, 1275–1284. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Ugbolue, U.; Duclos, M.; Urzeala, C.; Berthon, M.; Kulik, K.; Bota, A.; Thivel, D.; Bagheri, R.; Gu, Y.; Baker, J.; et al. An Assessment of the Novel COVISTRESS Questionnaire: COVID-19 Impact on Physical Activity, Sedentary Action and Psychological Emotion. J. Clin. Med. 2020, 9, 3352. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Sun, Y.; Zhang, X.; Sun, F.; Wang, B.; Zhu, W. Is Physical Activity Associated with Mental Health among Chinese Adolescents during Isolation in COVID-19 Pandemic? J. Epidemiol. Glob. Health 2020, 11, 26–33. [Google Scholar] [CrossRef]
- Lu, C.; Chi, X.; Liang, K.; Chen, S.; Huang, L.; Guo, T.; Jiao, C.; Yu, Q.; Veronese, N.; Soares, F.; et al. Moving More and Sitting Less as Healthy Lifestyle Behaviors are Protective Factors for Insomnia, Depression, and Anxiety among Adolescents during the COVID-19 Pandemic. Psychol. Res. Behav. Manag. 2020, 13, 1223–1233. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Green, S. Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: https://handbook-5-1.cochrane.org/ (accessed on 1 March 2011).
- Janssen, I.; Clarke, A.; Carson, V.; Chaput, J.; Giangregorio, L.; Kho, M.; Poitras, V.; Ross, R.; Saunders, T.; Ross-White, A.; et al. A systematic review of compositional data analysis studies examining associations between sleep, sedentary behaviour, and physical activity with health outcomes in adults. Appl. Physiol. Nutr. Metab. = Physiol. Appl. Nutr. Metab. 2020, 45, S248–S257. [Google Scholar] [CrossRef]
- Poitras, V.; Gray, C.; Janssen, X.; Aubert, S.; Carson, V.; Faulkner, G.; Goldfield, G.; Reilly, J.; Sampson, M.; Tremblay, M. Systematic review of the relationships between sedentary behaviour and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, J.; Lawrence, S.; Brazendale, K.; Leahy, N.; Fukuda, D. Brief report: The impact of the COVID-19 pandemic on health behaviors in adolescents with Autism Spectrum Disorder. Disabil. Health J. 2020, 14, 101021. [Google Scholar] [CrossRef]
- Sciberras, E.; Patel, P.; Stokes, M.; Coghill, D.; Middeldorp, C.; Bellgrove, M.; Becker, S.; Efron, D.; Stringaris, A.; Faraone, S.; et al. Physical Health, Media Use, and Mental Health in Children and Adolescents with ADHD during the COVID-19 Pandemic in Australia. J. Atten. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.; Heymsfield, S. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- López-Bueno, R.; López-Sánchez, G.; Casajús, J.; Calatayu, J.; Gil-Salmerón, A.; Grabovac, I.; Tully, M.; Smith, L. Health-Related Behaviors among School-Aged Children and Adolescents during the Spanish COVID-19 Confinement. Front. Pediatr. 2020, 8, 573. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2021, 16, e12731. [Google Scholar] [CrossRef]
- Palladino, F.; Merolla, E.; Solimeno, M.; de Leva, M.; Lenta, S.; Di Mita, O.; Bonadies, A.; Striano, P.; Tipo, V.; Varone, A. Is COVID-19 lockdown related to an increase of accesses for seizures in the emergency department? An observational analysis of a paediatric cohort in the Southern Italy. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2020, 41, 3475–3483. [Google Scholar] [CrossRef]
- Dutta, K.; Mukherjee, R.; Sen, D.; Sahu, S. Effect of COVID-19 lockdown on sleep behaviour and screen exposure time: An observational study among Indian school children. Biol. Rhythm Res. 2020. [Google Scholar] [CrossRef]
- Eyimaya, A.; Irmak, Y. Relationship between parenting practices and children’s screen time during the COVID-19 Pandemic in Turkey. J. Pediatr. Nurs. 2020, 56, 24–29. [Google Scholar] [CrossRef]
- Munasinghe, S.; Sperandei, S.; Freebairn, L.; Conroy, E.; Jani, H.; Marjanovic, S.; Page, A. The Impact of Physical Distancing Policies during the COVID-19 Pandemic on Health and Well-Being among Australian Adolescents. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2020, 67, 653–661. [Google Scholar] [CrossRef]
- Carroll, N.; Sadowski, A.; Laila, A.; Hruska, V.; Nixon, M.; Ma, D.; Haines, J.; On Behalf Of The Guelph Family Health Study. The Impact of COVID-19 on Health Behavior, Stress, Financial and Food Security among Middle to High Income Canadian Families with Young Children. Nutrients 2020, 12, 2352. [Google Scholar] [CrossRef]
- McCormack, G.; Doyle-Baker, P.; Petersen, J.; Ghoneim, D. Parent anxiety and perceptions of their child’s physical activity and sedentary behaviour during the COVID-19 pandemic in Canada. Prev. Med. Rep. 2020, 20, 101275. [Google Scholar] [CrossRef]
- Schmidt, S.; Anedda, B.; Burchartz, A.; Eichsteller, A.; Kolb, S.; Nigg, C.; Niessner, C.; Oriwol, D.; Worth, A.; Woll, A. Physical activity and screen time of children and adolescents before and during the COVID-19 lockdown in Germany: A natural experiment. Sci. Rep. 2020, 10, 21780. [Google Scholar] [CrossRef]
- Dunton, G.; Do, B.; Wang, S. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Mitra, R.; Moore, S.; Gillespie, M.; Faulkner, G.; Vanderloo, L.; Chulak-Bozzer, T.; Rhodes, R.; Brussoni, M.; Tremblay, M. Healthy movement behaviours in children and youth during the COVID-19 pandemic: Exploring the role of the neighbourhood environment. Health Place 2020, 65, 102418. [Google Scholar] [CrossRef]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the COVID-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Francisco, R.; Pedro, M.; Delvecchio, E.; Espada, J.; Morales, A.; Mazzeschi, C.; Orgilés, M. Psychological Symptoms and Behavioral Changes in Children and Adolescents during the Early Phase of COVID-19 Quarantine in Three European Countries. Front. Psychiatry 2020, 11, 1329. [Google Scholar] [CrossRef]
- Zinner, C.; Matzka, M.; Leppich, R.; Kounev, S.; Holmberg, H.; Sperlich, B. The Impact of the German Strategy for Containment of Coronavirus SARS-CoV-2 on Training Characteristics, Physical Activity and Sleep of Highly Trained Kayakers and Canoeists: A Retrospective Observational Study. Front. Sports Act. Living 2020, 2, 579830. [Google Scholar] [CrossRef]
- Rezende, D.; Pinto, A.; Goessler, K.; Nicoletti, C.; Sieczkowska, S.; Meireles, K.; Esteves, G.; Genario, R.; Oliveira Júnior, G.; Santo, M.; et al. Influence of Adherence to Social Distancing Due to the COVID-19 Pandemic on Physical Activity Level in Post-bariatric Patients. Obes. Surg. 2021, 31, 1372–1375. [Google Scholar] [CrossRef]
- Biviá-Roig, G.; La-Rosa, V.; Gómez-Tébar, M.; Serrano-Raya, L.; Amer-Cuenca, J.; Caruso, S.; Commodari, E.; Barrasa-Shaw, A.; Lisón, J. Analysis of the Impact of the Confinement Resulting from COVID-19 on the Lifestyle and Psychological Wellbeing of Spanish Pregnant Women: An Internet-Based Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 5933. [Google Scholar] [CrossRef] [PubMed]
- Werneck, A.; Silva, D.; Malta, D.; Souza-Júnior, P.; Azevedo, L.; Barros, M.; Szwarcwald, C. Physical inactivity and elevated TV-viewing reported changes during the COVID-19 pandemic are associated with mental health: A survey with 43,995 Brazilian adults. J. Psychosom. Res. 2021, 140, 110292. [Google Scholar] [CrossRef] [PubMed]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef] [PubMed]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2021, 39, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Colivicchi, F.; Di Fusco, S.; Magnanti, M.; Cipriani, M.; Imperoli, G. The Impact of the Coronavirus Disease-2019 Pandemic and Italian Lockdown Measures on Clinical Presentation and Management of Acute Heart Failure. J. Card. Fail. 2020, 26, 464. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.; Ferracuti, S.; De Giglio, O.; Caggiano, G.; Protano, C.; Valeriani, F.; Parisi, E.; Valerio, G.; Liguori, G.; et al. Sedentary Behaviors and Physical Activity of Italian Undergraduate Students during Lockdown at the Time of CoViD-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6171. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.; Zielinska, M.; Hamułka, J. Dietary and Lifestyle Changes during COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef] [PubMed]
- Janssen, X.; Fleming, L.; Kirk, A.; Rollins, L.; Young, D.; Grealy, M.; MacDonald, B.; Flowers, P.; Williams, L. Changes in Physical Activity, Sitting and Sleep across the COVID-19 National Lockdown Period in Scotland. Int. J. Environ. Res. Public Health 2020, 17, 9362. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Casaña, J.; Casajús, J.; Smith, L.; Tully, M.; Andersen, L.; López-Sánchez, G. COVID-19 Confinement and Health Risk Behaviors in Spain. Front. Psychol. 2020, 11, 1426. [Google Scholar] [CrossRef]
- Luciano, F.; Cenacchi, V.; Vegro, V.; Pavei, G. COVID-19 lockdown: Physical activity, sedentary behaviour and sleep in Italian medicine students. Eur. J. Sport Sci. 2021, 21, 1459–1468. [Google Scholar] [CrossRef]
- Mon-López, D.; Bernardez-Vilaboa, R.; Fernandez-Balbuena, A.; Sillero-Quintana, M. The Influence of COVID-19 Isolation on Physical Activity Habits and Its Relationship with Convergence Insufficiency. Int. J. Environ. Res. Public Health 2020, 17, 7406. [Google Scholar] [CrossRef]
- Richardson, D.; Duncan, M.; Clarke, N.; Myers, T.; Tallis, J. The influence of COVID-19 measures in the United Kingdom on physical activity levels, perceived physical function and mood in older adults: A survey-based observational study. J. Sports Sci. 2021, 39, 887–899. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Larrad, A.; Mañas, A.; Labayen, I.; González-Gross, M.; Espin, A.; Aznar, S.; Serrano-Sánchez, J.A.; Vera-Garcia, F.J.; González-Lamuño, D.; Ara, I.; et al. Impact of COVID-19 Confinement on Physical Activity and Sedentary Behaviour in Spanish University Students: Role of Gender. Int. J. Environ. Res. Public Health 2021, 18, 369. [Google Scholar] [CrossRef] [PubMed]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global Changes and Factors of Increase in Caloric/Salty Food Intake, Screen Use, and Substance Use during the Early COVID-19 Containment Phase in the General Population in France: Survey Study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef] [PubMed]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.; Parra-Fernández, M.; Prado-Laguna, M.; Hernández-Martínez, A. Physical Activity and Sedentary Lifestyle in University Students: Changes during Confinement Due to the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Sanudo, B.; Fennell, C.; Sanchez-Oliver, A. Objectively-assessed physical activity, sedentary behaviour, smart phone use, and sleep patterns pre-and during-COVID-19 quarantine in young adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Savage, M.; James, R.; Magistro, D.; Donaldson, D.; Healy, L.; Nevill, M.; Hennis, P. Mental health and movement behaviours during the COVID-19 pandemic in UK university students: Prospective cohort study. Ment. Health Phys. Act. 2020, 19, 100357. [Google Scholar] [CrossRef]
- Stieger, S.; Lewetz, D.; Swami, V. Emotional Well-Being under Conditions of Lockdown: An Experience Sampling Study in Austria during the COVID-19 Pandemic. J. Happiness Stud. 2021, 22, 2703–2720. [Google Scholar] [CrossRef]
- Alomari, M.; Khabour, O.; Alzoubi, K. Changes in Physical Activity and Sedentary Behavior Amid Confinement: The BKSQ-COVID-19 Project. Risk Manag. Healthc. Policy 2020, 13, 1757–1764. [Google Scholar] [CrossRef]
- Chawla, B.; Chawla, S.; Singh, H.; Jain, R.; Arora, I. Is coronavirus lockdown taking a toll on mental health of medical students? A study using WHOQOL-BREF questionnaire. J. Fam. Med. Prim. Care 2020, 9, 5261. [Google Scholar] [CrossRef]
- Husain, W.; Ashkanani, F. Does COVID-19 change dietary habits and lifestyle behaviours in Kuwait: A community-based cross-sectional study. Environ. Health Prev. Med. 2020, 25, 61. [Google Scholar] [CrossRef]
- Ismail, C.; Osaili, T.; Mohamad, M.; Al Marzouqi, A.; Jarrar, A.; Abu Jamous, D.; Magriplis, E.; Ali, H.; Al Sabbah, H.; Hasan, H.; et al. Eating Habits and Lifestyle during COVID-19 Lockdown in the United Arab Emirates: A Cross-Sectional Study. Nutrients 2020, 12, 3314. [Google Scholar] [CrossRef]
- Ismail, C.; Osaili, T.; Mohamad, M.; Al Marzouqi, A.; Jarrar, A.; Zampelas, A.; Habib-Mourad, C.; Jamous, O.; Ali, H.; Al Sabbah, H.; et al. Assessment of eating habits and lifestyle during the coronavirus 2019 pandemic in the Middle East and North Africa region: A cross-sectional study. Br. J. Nutr. 2021, 126, 757–766. [Google Scholar] [CrossRef]
- Qi, M.; Li, P.; Moyle, W.; Weeks, B.; Jones, C. Physical Activity, Health-Related Quality of Life, and Stress among the Chinese Adult Population during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6494. [Google Scholar] [CrossRef] [PubMed]
- Qin, F.; Song, Y.; Nassis, G.; Zhao, L.; Dong, Y.; Zhao, C.; Feng, Y.; Zhao, J. Physical Activity, Screen Time, and Emotional Well-Being during the 2019 Novel Coronavirus Outbreak in China. Int. J. Environ. Res. Public Health 2020, 17, 5170. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.; Islam, M.; Bishwas, M.; Moonajilin, M.; Gozal, D. Physical inactivity and sedentary behaviors in the Bangladeshi population during the COVID-19 pandemic: An online cross-sectional survey. Heliyon 2020, 6, e05392. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lei, S.; Le, S.; Yang, Y.; Zhang, B.; Yao, W.; Gao, Z.; Cheng, S. Bidirectional Influence of the COVID-19 Pandemic Lockdowns on Health Behaviors and Quality of Life among Chinese Adults. Int. J. Environ. Res. Public Health 2020, 17, 5575. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Guo, B.; Ao, L.; Yang, C.; Zhang, L.; Zhou, J.; Jia, P. Obesity and activity patterns before and during COVID-19 lockdown among youths in China. Clin. Obes. 2020, 10, e12416. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, S.; Eskici, G. Evaluation of emotional (depression) and behavioural (nutritional, physical activity and sleep) status of Turkish adults during the COVID-19 pandemic period. Public Health Nutr. 2021, 24, 942–949. [Google Scholar] [CrossRef]
- Zheng, C.; Huang, W.; Sheridan, S.; Sit, C.; Chen, X.; Wong, S. COVID-19 Pandemic Brings a Sedentary Lifestyle in Young Adults: A Cross-Sectional and Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 6035. [Google Scholar] [CrossRef] [PubMed]
- Barkley, J.; Lepp, A.; Glickman, E.; Farnell, G.; Beiting, J.; Wiet, R.; Dowdell, B. The Acute Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in University Students and Employees. Int. J. Exerc. Sci. 2020, 13, 1326. [Google Scholar]
- McDowell, C.; Herring, M.; Lansing, J.; Brower, C.; Meyer, J. Working From Home and Job Loss Due to the COVID-19 Pandemic Are Associated with Greater Time in Sedentary Behaviors. Front. Public Health 2020, 8, 750. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.; Herring, M.; McDowell, C.; Lansing, J.; Brower, C.; Schuch, F.; Smith, L.; Tully, M.; Martin, J.; Caswell, S.; et al. Joint prevalence of physical activity and sitting time during COVID-19 among US adults in April 2020. Prev. Med. Rep. 2020, 20, 101256. [Google Scholar] [CrossRef]
- Stephan, Y.; Terracciano, A.; Luchetti, M.; Aschwanden, D.; Lee, J.; Sesker, A.; Strickhouser, J.; Sutin, A. Physical Activity and Sedentary Behaviour during COVID-19: Trajectory and Moderation by Personality. Soc. Psychol. Personal. Sci. 2021, 12. [Google Scholar] [CrossRef]
- Zajacova, A.; Jehn, A.; Stackhouse, M.; Denice, P.; Ramos, H. Changes in health behaviours during early COVID-19 and socio-demographic disparities: A cross-sectional analysis. Can. J. Public Health = Rev. Can. Sante Publique 2020, 111, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Browne, R.; Macêdo, G.; Cabral, L.; Oliveira, G.; Vivas, A.; Fontes, E.; Elsangedy, H.; Costa, E. Initial impact of the COVID-19 pandemic on physical activity and sedentary behavior in hypertensive older adults: An accelerometer-based analysis. Exp. Gerontol. 2020, 142, 111121. [Google Scholar] [CrossRef] [PubMed]
- Malta, D.; Szwarcwald, C.; Barros, M.; Gomes, C.; Machado, Í.; Souza Júnior, P.; Romero, D.; Lima, M.; Damacena, G.; Pina, M.; et al. The COVID-19 Pandemic and changes in adult Brazilian lifestyles: A cross-sectional study, 2020. Epidemiol. Serv. Saude Rev. Sist. Unico Saude Bras. 2020, 29. [Google Scholar] [CrossRef]
- Werneck, A.O.; da Silva, D.R.; Malta, D.C.; de Souza, P.R.B.; Azevedo, L.O.; Barros, M.B.D.; Szwarcwald, C.L. Lifestyle behaviors changes during the COVID-19 pandemic quarantine among 6881 Brazilian adults with depression and 35,143 without depression. Cienc. Saude Coletiva 2020, 25, 4151–4156. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Olavarría, D.; Latorre-Román, P.; Guzmán-Guzmán, I.; Jerez-Mayorga, D.; Caamaño-Navarrete, F.; Delgado-Floody, P. Positive and Negative Changes in Food Habits, Physical Activity Patterns, and Weight Status during COVID-19 Confinement: Associated Factors in the Chilean Population. Int. J. Environ. Res. Public Health 2020, 17, 5431. [Google Scholar] [CrossRef]
- Asiamah, N.; Opuni, F.; Mends-Brew, E.; Mensah, S.; Mensah, H.; Quansah, F. Short-Term Changes in Behaviors Resulting from COVID-19-Related Social Isolation and Their Influences on Mental Health in Ghana. Community Ment. Health J. 2021, 57, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Werneck, A.; Silva, D.; Malta, D.; Souza-Júnior, P.; Azevedo, L.; Barros, M.; Szwarcwald, C. Changes in the clustering of unhealthy movement behaviors during the COVID-19 quarantine and the association with mental health indicators among Brazilian adults. Transl. Behav. Med. 2021, 11, 323–331. [Google Scholar] [CrossRef]
- Sá, C.; Pombo, A.; Luz, C.; Rodrigues, L.; Cordovil, R. COVID-19 Social Isolation in Brazil: Effects on the Physical Activity Routine of Families with Children. Rev. Paul. Pediatr. Orgao Of. Soc. Pediatr. Sao Paulo 2020, 39. [Google Scholar] [CrossRef]
- Gray, C.; Gibbons, R.; Larouche, R.; Sandseter, E.; Bienenstock, A.; Brussoni, M.; Chabot, G.; Herrington, S.; Janssen, I.; Pickett, W.; et al. What Is the Relationship between Outdoor Time and Physical Activity, Sedentary Behaviour, and Physical Fitness in Children? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 6455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Love, R.; Adams, J.; Atkin, A.; van Sluijs, E. Socioeconomic and ethnic differences in children’s vigorous intensity physical activity: A cross-sectional analysis of the UK Millennium Cohort Study. BMJ Open 2019, 9, e027627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akpinar, A. Urban green spaces for children: A cross-sectional study of associations with distance, physical activity, screen time, general health, and overweight status. Urban For. Urban Green. 2017, 25, 66–73. [Google Scholar] [CrossRef]
- Saunders, T.; Tremblay, M.; Mathieu, M.; Henderson, M.; O’Loughlin, J.; Tremblay, A.; Chaput, J. Associations of sedentary behavior, sedentary bouts and breaks in sedentary time with cardiometabolic risk in children with a family history of obesity. PLoS ONE 2013, 8, e79143. [Google Scholar] [CrossRef] [Green Version]
- Egan, C.; Webster, C.; Beets, M.; Weaver, R.; Russ, L.; Michael, D.; Nesbitt, D.; Orendorff, K. Sedentary time and Behaviour during School: A systematic Review and Meta-Analysis. Am. J. Health Educ. 2019, 50, 283–290. [Google Scholar] [CrossRef]
- Abbott, R.; Straker, L.; Mathiassen, S. Patterning of children’s sedentary time at and away from school. Obesity (Silver Spring Md.) 2013, 21, E131–E133. [Google Scholar] [CrossRef]
- Lubans, D.; Hesketh, K.; Cliff, D.; Barnett, L.; Salmon, J.; Dollman, J.; Morgan, P.; Hills, A.; Hardy, L. A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, 781–799. [Google Scholar] [CrossRef]
- Ottevaere, C.; Huybrechts, I.; De Bourdeaudhuij, I.; Sjostrom, M.; Ruiz, J.R.; Ortega, F.B.; Hagstromer, M.; Widhalm, K.; Molnar, D.; Moreno, L.A.; et al. Comparison of the IPAQ-A and ActiGraph in relation to VO2 max among European adolescents: The HELENA study. Sci. Med. Sport 2011, 14, 317–324. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S.; Leblanc, A.G.; Janssen, I.; Kho, M.E.; Hicks, A.; Murumets, K.; Colley, R.C.; Duggan, M. Canadian sedentary behaviour guidelines for children and youth. Appl. Physiol. Nutr. Metab. 2011, 36, 65–71. [Google Scholar] [CrossRef]
- Colley, R.; Garriguet, D.; Janssen, I.; Wong, S.; Saunders, T.; Carson, V.; Tremblay, M. The association between accelerometer-measured patterns of sedentary time and health risk in children and youth: Results from the Canadian Health Measures Survey. BMC Public Health 2013, 13, 200. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Luan, J.; Sherar, L.; Esliger, D.; Griew, P.; Cooper, A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012, 307, 704–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carson, V.; Tremblay, M.; Chaput, J.; Chastin, S. Associations between Sleep Duration, Sedentary Time, Physical Activity, and Health Indicators among Canadian Children and Youth Using Compositional Analyses. Appl. Physiol. Nutr. Metab. 2016, 41, S294–S302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, S.; Roberts, K.; Melvin, A.; Butler, G.; Thompson, W. Gender and education differences in sedentary behaviour in Canada: An analysis of national cross-sectional surveys. BMC Public Health 2020, 20, 1170. [Google Scholar] [CrossRef]
- Kallio, J.; Hakonen, H.; Syväoja, H.; Kulmala, J.; Kankaanpää, A.; Ekelund, U.; Tammelin, T. Changes in physical activity and sedentary time during adolescence: Gender differences during weekdays and weekend days. Scand. J. Med. Sci. Sports 2020, 30, 1265–1275. [Google Scholar] [CrossRef] [Green Version]
- Hidding, L.; Chinapaw, M.; van Poppel, M.; Mokkink, L.; Altenburg, T. An Updated Systematic Review of Childhood Physical Activity Questionnaires. Sports Med. 2018, 48, 2797–2842. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.; Anderson, L.; Bull, F.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress. pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Arigo, D.; Pasko, K.; Mogle, J. Daily relations between social perceptions and physical activity among college women. Psychol. Sport Exerc. 2020, 47, 101528. [Google Scholar] [CrossRef]
- Balish, S.; Deaner, R.; Rainham, D.; Blanchard, C. Sex Differences in Sport Remain When Accounting for Countries’ Gender Inequality. Cross-Cult. Res. 2016, 50, 395–414. [Google Scholar] [CrossRef]
- Copeland, J.L.; Eslinger, D.W. Accelerometer assessment of physical activity in active, healthy older adults. J. Ageing Phys. Act. 2009, 17, 17–30. [Google Scholar] [CrossRef] [Green Version]
- Burki, T. China’s successful control of COVID-19. Lancet. Infect. Dis. 2020, 20, 1240–1241. [Google Scholar] [CrossRef]
- Schmid, D.; Ricci, C.; Leitzmann, M.F. Associations of objectively assessed physical activity and sedentary time with all-cause mortality in US adults: The NHANES study. PLoS ONE 2015, 10, e0119591. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; Coombs, N.; Stamatakis, E. Associations between objectively assessed and self-reported sedentary time with mental health in adults: An analysis of data from the Health Survey for England. BMJ Open 2014, 4, e004580. [Google Scholar] [CrossRef]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef]
- Gradidge, P.J.L.; Kruger, H.S. Physical activity, diet and quality of life during mandatory (COVID-19) quarantine following repatriation. SAGE Open Med. Case Rep. 2020, 8, 2050313x20972508. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Author | Population | Country | Restrictions | Sedentary Behaviour Measurement | Health Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|
| Kang et al. [20] | 4898 adolescents 16.3 ± 1.3 years | China | School closures and social distancing | IPAQ-Short Form | Mood (Anger, Tension, Fatigue, Depression, Confusion, Self-esteem and Vigor) | Sedentary time totaled 363.6 ± 148.4 min day−1 No sig. correlation between sedentary time and any mood during COVID restrictions |
| Lu et al. [21] | 965 adolescents 15.3 ± 0.5 years | China | Social distancing and lockdown/homestay requirements | IPAQ-Short Form | Mental Health outcomes including Insomnia, Depression and Anxiety | 54% adolescents sedentary for ≥ 4 h day−1 Sedentary time associated with higher odds of experiencing insomnia (OR: 1.60), depression (OR: 1.57) and anxiety (OR: 1.35) during lockdown |
| Garcia et al. [27] | 11 adolescents with Autism 16.9 ± 1.4 years | Florida, USA | Lockdown/Homestay requirements | IPAQ Short Form | - | Number of days where participants met the PA guidelines ↓ from 4.2 ± 1.5 days to 2.3 ± 2.2 days Screen time ↑ by 2.6 h⋅day−1 during the week and +1.4 h⋅day−1 on the weekend |
| Sciberras et al. [28] | 213 children with ADHD 11.0 ± 3.9 years | Australia | Social distancing and lockdown/homestay requirements | CoRonavIruS Health Impact Survey (CRISIS) | - | Number of children reporting watching TV, social media, and gaming for >1 h⋅day−1 increased by 10.2%, 10.8% and 16.9%, respectively |
| Pietrobelli et al. [29] | 44 obese children 13.0 ± 3.1 years | Italy | Lockdown/homestay requirements | Two different interview techniques | Screen time ↑ by 4.9 ± 2.4 h⋅day−1 during the lockdown to 7.6 ± 2.1 h⋅day−1 | |
| Lopez-Beuno et al. [30] | 860 children 9.6 ± 3.9 years | Spain | Social distancing, quarantine, and lockdown/homestay requirements | Adapted pre-existing questionnaires | - | Daily screen time ↑ 2.9 ± 2.3 h⋅day−1 No significant sex differences in screen time |
| Medrano et al. [31] | 291 children (113 longitudinal) 12.1 ± 2.6 years | Spain | Social distancing and lockdown/homestay requirements | Youth PA (YPA) questionnaire | - | Screen time ↑ 1.9 ± 2.6 h day−1 to 6.4 ± 2.4 h day−1 Screen time higher in families of non-Spanish origin and lower education level |
| Palladino et al. [32] | 57 children 8.0 ± 1.6 years | Italy | Lockdown/stay at home orders | Questionnaires to assess total screen time | Likelihood of having a seizure | Daily screen time ↑ from 2.5–5.8 h day−1 from pre-COVID to circa-COVID Sig. correlation between screen time and seizures for epileptic patients (r2 = 0.52) and those with no prior history of seizures (r2 = 0.57) |
| Dutta et al. [33] | 153 participants No overall demographics reported | India | Lockdown/homestay requirements | Parenting practice scale (PPS) | - | Number of youth reporting using phones, watching TV, Laptops and Tablets from 4–8 h⋅day−1 increased by 8.7%, 5.7%, 2.8% and 0%, respectively |
| Eyimaya and Irmak [34] | 1115 participants 9.0 ± 2.0 years | Turkey | Lockdown/homestay requirements | IPAQ long-form | 71.7% parents reported an ↑ screen time of approximately 6.4 ± 3.0 h⋅day−1 | |
| Munasinghe et al. [35] | 582 adolescents 17.0 ± 1.0 years | Australia | Social distancing, school closures and lockdown/homestay requirements | PACE + Adolescent Physical Activity Measures | - | 41.5% were on social media for ≥ 4 h day−1 55.1% watched TV for ≥ 1 h⋅day−1 |
| Carroll et al. [36] | 310 participants 5.7 ± 2.0 years | Canada | School closures, closure of parks, and social distancing | IPAQ Short Form | - | Screen time = 2.4 ± 1.6 h⋅day−1 |
| McCormack et al. [37] | 345 parents 10.8 ± 4.0 years | Canada | Social distancing and quarantine measures | Parental recall of child’s PA and sedentary time | Parental COVID anxiety | Majority of children spent ≥ 2 h day−1 watching TV (74.1%), using a computer (63.7%), and using screen-based devices (60.7%) Children of highly anxious parents more likely to be sedentary (OR: 1.78; 1.02–3.11) |
| Schmidt et al. [38] | 1174 children No overall demographics reported | Germany | Social distancing and lockdown/homestay requirements | Subjective recall questions | - | 4–5 year olds screen time ↑ 41.1 min day−1 6–10 year olds screen time ↑ 67.5 min day−1 11–13 year olds screen time ↑ 60.7 min day−1 14–17 year olds screen time ↑ 67.8 min day−1 |
| Dunton et al. [39] | 211 children 8.7 ± 2.6 years | United States | Closure of schools, parks, and sports cancelled Social Distancing | Recall questionnaires used to estimate screen time | - | Boys TV time 95.7 ± 68.7 min day−1 vs. girls 113.0 ± 79.6 min day−1 Media time for leisure use: boys 30.2 ± 53.4 min day−1 vs. girls 46.4 ± 68.0 min day−1 Children engaged in > 8 h⋅day−1 in leisure-related sitting |
| Mitra et al. [40] | 1472 participants No overall demographics reported | Canada | Social distancing and lockdown/homestay requirements | Online questionnaires—limited details on specifics | - | 78.8% of children reported an increase in screen time 44.6% reported an increase in social media use 48.6% reported an increase in ‘non-screen based’ sedentary behaviour |
| Moore et al. [41] | 1472 children and adolescents Children: 8.1 ± 2.0 years Youth: 14.9 ± 1.7 years | Canada | Social distancing and lockdown/homestay requirements | participACTION survey | - | Screen time (children)—4.1 h day−1 Screen time (youth)—5.0 h day−1 |
| Francisco et al. [42] | 1480 children 9.1 ± 4.3 years | Multinational (Italy, Spain and Portugal) | Social distancing and lockdown/homestay requirements | IPAQ and the adult sedentary behaviour questionnaire (ASBQ) | - | Number of children reported to engage in >180 min⋅day−1 of screen time ↑ 26.6% |
| Author | Population | Country | Restrictions | Sedentary Behaviour Measurement | Health Outcome Measures | Key Findings |
|---|---|---|---|---|---|---|
| Meyer et al. [18] | 3052 participants No overall descriptives available | United States | Social distancing, quarantine, and lockdown/homestay requirements | Online questionnaires—no details on specific ones used | Depressive, anxiety, loneliness, and stress symptoms Social network and positive mental health all assessed | Those who maintained a screen time of <8 h day−1 had sig less depressive symptoms (b = 1.9, p < 0.01), loneliness (b = 0.3, p < 0.01), stress (b = 0.6, p < 0.01) and had a more positive outlook (b = 0.92, p < 0.01) Sitting time was not associated with any mental health outcome |
| Carroll et al. [36] | 351 participants 38.5 ± 5.2 years | Canada | School closures, closure of parks, and social distancing | IPAQ Short Form | - | Adult sitting time 6.3 ± 3.0 h day−1 Screen time 2.8 ± 1.7 h day−1 |
| Zinner et al. [43] | 14 professional kayakers 22.9 ± 1.4 years | Germany | Social distancing and Lockdown/homestay requirements | Heart rate monitoring | - | Sitting time ↑ from 623.0 ± 63.0 min day−1 to 729 ± 21 min day−1 during COVID) |
| Rezende et al. [44] | 37 post-bariatric patients 48.1 ± 4.0 years | Brazil | Social distancing and lockdown/homestay requirements | GT3X accelerometers and subjective recall questionnaires | - | Mean sedentary time was 9.5 ± 0.5 h day−1 Participants who adhered to social distancing measures spent more time sedentary (+1.1 ± 1.0 h day−1) |
| Bivia-Roig et al. [45] | 90 pregnant women 33.1 ± 4.6 years | Spain | Lockdown/homestay requirements | Adapted questionnaires for SB and EuroQol-5D for mental health | Health-Related QoL | ↓ in HRQoL 50% ↑ in sitting time (4 h day−1–8 h day−1) |
| Werneck et al. [46] | 43,995 participants 43.0 ± 0.5 years | Brazil | Social distancing and quarantine measures | No specific details on questionnaires used | Depression | ↑ TV viewing time associated with ↓ mental health |
| Castaneda-Babarro et al. [47] | 3800 participants 42.7 ± 10.4 | Spain | Lockdown/homestay requirements | Internally validated questionnaire | - | Overall sitting time ↑ 23.8% to 480.0 ± 306.0 min day−1 Women less of an increase in sedentary time than men (↑ 25.3% and 35.0%, resp.) |
| Cheval et al. [48] | 110 participants No overall demographics available | France and Switzerland | Limit to 1 h per day exercise Social distancing Home working | Newly designed questionnaire | Global physical and mental health Depressive symptoms Subjective vitality | ↑ 75 min day−1 sedentary time ↑ sedentary time led to ↓ physical and mental health and subjective vitality |
| Colivicchi et al. [49] | 124 participants 71.0 ± 14.0 years | France | Lockdown/homestay requirements | Telephone interviews | - | 41.9% reported ↓ physical activity 50% reported ↑ screen time |
| Gallé et al. [50] | 1430 participants 22.9 ± 3.5 years | Italy | Lockdown/homestay requirements | PLifeCOVID-19 questionnaire | - | Sedentary time doubled during lockdown (240 ± 240 to 480 ± 300 min day−1) Biggest increase in specific behaviours was electronic devices (+52.4 min day−1) |
| Gornicka et al. [51] | 2381 participants No overall demographics reported | Poland | Social distancing and lockdown/homestay requirements | Canadian Health Measures Survey | - | 49.1% of participants ↑ screen time 35.9% screen time ≥8 h day−1 on weekdays—dropping to 11.5% on weekends |
| Janssen et al. [52] | 3241 participants 46.2 ± 15.3 years | Scotland | Social distancing and lockdown/homestay requirements | IPAQ on three occasions to track changes in sedentary behaviour | - | Sitting time ↑ 396.9 ± 188.0 min day−1 pre-COVID to 427.4 ± 210.9 min day−1 during COVID |
| Lopez-Bueno et al. [53] | 2741 participants 34.2 ± 13.0 years | Spain | Social distancing, quarantine and lockdown/homestay requirements | Physical activity vital sign questionnaire | - | 2.3% of respondents reported spending >2 h day−1 using screens |
| Luciano et al. [54] | 1470 participants (394 of which assessed longitudinally) 23 ± 2 years | Italy | Social distancing and lockdown/homestay requirements | IPAQ-Short Form with additional questions added | - | Sitting time per day ↑ from 8 h day−1 pre-COVID to 10 h day−1 circa-COVID |
| Mon-Lopez et al. [55] | 120 participants 39.6 ± 13.6 years | Spain | Social distancing and lockdown/homestay requirements | IPAQ-Short Form | - | Screen time ↑ 403.0 ± 203.4 min day−1 to 615.6 ± 331.6 min day−1 |
| Richardson et al. [56] | 117 participants 75.0 ± 4.0 years | United Kingdom | Social distancing and lockdown/homestay requirements | IPAQ-E | - | Sitting time ↑ from 426.0 ± 27.0 min day−1 pre-COVID to 490.0 ± 25.0 min day−1 during COVID |
| Rodrìguez-Larrad et al. [57] | 13,754 university students 22.8 ± 5.3 years | Spain | Lockdown/homestay requirements | Combination of IPAQ and modified SB questions | - | Sedentary time ↑ by 52.7% from 357 ± 178 min day−1 (pre) to 545 ± 200 min day−1 (follow-up) Screen time ↑ 71.9% (217 min day−1–373 min day−1) |
| Rolland et al. [58] | 11,391 participants 47.5 ± 17.3 years | France | Lockdown/homestay requirements | Newly developed unvalidated questionnaire | - | 64.6% of people reported ↑ screen time Predictive factors included: being female (OR: 1.31) under 29 years, being single (OR: 1.15) and being employed. |
| Romero-Blanco et al. [59] | 213 participants 20.5 ± 4.6 years | Spain | Lockdown/homestay requirements | IPAQ-Short Form | - | Sitting time ↑ 141.8 (95%CI: 71.9–141.8) min day−1 to 525.4 ± 194.6 min day−1 Normal/underweight participants sig. increased sitting time compared to overweight/obese participants Smokers sitting time did not sig. change during lockdown |
| Sañudo et al. [60] | 20 adults 22.6 ± 3.4 years | Spain | Quarantine | Smart phone data and IPAQ-Short Form | - | Sitting time ↑ from 6.4 h day−1 to 9.7 h day−1 |
| Savage et al. [61] | 214 participants No overall demographics reported | United Kingdom | Social distancing and lockdown/homestay requirements | Exercise vital sign (EVS) questionnaireWarwick-Edinburgh Mental Well-Being Scale Perceived Stress Scale | Mental health | Sedentary time ↑ by 20 h week−1 during COVID restrictions Change in sedentary time was positively associated with perceived stress but not overall well-being |
| Stieger et al. [62] | 286 participants 31.0 ± 14.5 years | Austria | Social distancing and lockdown/homestay requirements | Adapted survey questions to assess total screen time | Well-Being | ↑ screen time associated with a poorer sense of well-being |
| Alomari et al. [63] | 1844 participants 33.7 ± 1.3 years | Jordan | Social distancing and school closures | Newly developed unvalidated questionnaire | - | 72.3% of participants ↑ TV time 82.7% of participants ↑ in technology usage 81.9% of participants ↑ social media |
| Chawla et al. [64] | 231 participants No overall demographics available | India | Social distancing and lockdown/homestay requirements | IPAQ and sitting focused questions (for SB measure) | Quality of Life | 33.3% reported spending ≥6 h day−1 screen time ≥ 6 h day−1 screen time associated with ↓ psychological and social well-being |
| Hussain and Ashkanani [65] | 415 participants 38.5 ± 12.7 years | Kuwait | Lockdown/homestay requirements | Adapted questionnaires | - | % of people watching >6 h day−1 increased by 27.5% |
| Ismail et al. [66] | 1012 participants No overall demographics available | United Arab Emirates | Social distancing and quarantine measures | IPAQ-Short Form with a screen time question added | - | Number of people using screen time >5 h day−1 for work ↑ 15.6% >5 h day−1 screen time for leisure-time ↑ 23.7% |
| Ismail et al. [67] | 2970 participants No overall demographics available | Multinational | Social distancing, quarantines and lockdown/homestay requirements | IPAQ-Short Form with a screen time question added | - | Number of people using screen time >5 h day−1 for work ↑ 15.6% >5 h day−1 screen time for leisure-time ↑ 22.9% |
| Qi et al. [68] | 645 participants 31.8 ± 8.6 years | China | Social distancing and lockdown/homestay requirements | IPAQ-Short Form and the SF-8 to assess health related quality of life | HRQoL | Sedentary time ↑ 0.4 h day−1 to 5.8 ± 4.6 h day−1 Significant negative correlation between sedentary time and perceived physical health (r2 = −0.10, p < 0.05) |
| Qin et al. [69] | 12,107 participants No overall demographics reported | China | Lockdown/homestay requirements | IPAQ-Short Form and the positive and negative affect schedule (PANAS) | - | 261.3 ± 189.8 min day−1 screen time |
| Rahman et al. [70] | 2028 participants 25.9 ± 8.1 years | Bangladesh | Lockdown/homestay requirements | IPAQ-Short Form | - | 20.9% of participants >8 h day−1 in sedentary behaviours |
| Wang et al. [71] | 2289 participants 27.8 ± 12.0 years | China | Social distancing and lockdown/homestay requirements | New questionnaire–but good detail of measures throughout | Quality of Life Score | Average sitting time 7.4 ± 3.4 h day−1 SB negatively correlated to QoL (r2 = −0.05, p < 0.01) |
| Yang et al. [72] | 10,082 participants 19.8 ± 2.3 years | China | Social distancing and school closures | IPAQ-Short Form | - | Sedentary time ↑ from 4.0 to 4.5 h day−1 |
| Yilmaz et al. [73] | 1120 participants 33.0 ± 11.0 years | Turkey | Social distancing and quarantine measures | New questionnaire—but good detail of measures throughout | - | Sitting time was 5.4 ± 2.6 h day−1 |
| Zheng et al. [74] | 631 participants 21.1 ± 2.9 years | Hong Kong | Quarantine, closure of schools and work at home orders | IPAQ Sedentary Behaviour Questionnaire (SBQ) | - | Daily SB during COVID 9.4 ± 3.0 h day−1 compared to 7.8 ± 3.2 h day−1 pre-COVID |
| Barkley et al. [75] | 398 participants No overall demographics provided | United States | Social distancing and lockdown/homestay requirements | IPAQ | - | All university staff members reported ↑ sedentary time—average of +467 min week−1 Average sedentary time during COVID 481.0 ± 207.0 min day−1 |
| McDowell et al. [76] | 2303 participants No overall demographics provided | United States | Social distancing and lockdown/homestay requirements | Online questionnaire—limited details available | - | Mean sedentary time 533.0 ± 208.5 min day−1 People who began working from home, or lost their jobs, were most likely to ↑ sedentary time |
| Meyer et al. [77] | 5036 participants No overall descriptives available | United States | Social distancing, quarantine, and lockdown/homestay requirements | IPAQ-Short Form and adapted COVID specific survey questions | - | 42.6% (95% CI: 41.2–44.0%) of participants sat for >8 h day−1 |
| Stephan et al. [78] | 2230 participants 46.7 ± 17.8 years | United States | Social distancing and lockdown / homestay requirements | Recall questionnaires to assess sedentary behaviour | - | Time spent sedentary ↑ by 40 min day−1 to 7.3 ± 3.8 h day−1 |
| Zajacova et al. [79] | 4319 participants No overall demographics reported | Canada | Social distancing and lockdown/homestay requirements | Canadian Perspectives Survey Series 1 (CPSS-COVID) | - | 66% increased TV viewing time |
| Browne et al. [80] | 35 participants 65.6 ± 3.8 years | Brazil | Social distancing and lockdown/homestay requirements | GT3X accelerometer | - | Sedentary time ↑ 29.8 min day−1 to 682.6 (95%CI: 657.3–707.9) mins day−1 SB pattern more negative (more bouts ≥10 and 30 min, broken up less often) |
| Malta et al. [81] | 45,161 participants No overall demographics provided | Brazil | Social distancing and lockdown/homestay requirements | Internally validated questionnaire | - | Time spent using computers/tablets ↑ 1.5 ± 0.1 h day−1 to 5.3 ± 0.1 h day−1 Time spent watching TV ↑ 1.5 ± 0.1 h day−1 to 3.3 ± 0.1 h day−1 |
| Werneck et al. [82] | 6881 participants with depression–35,143 participants with depression No overall demographics reported | Brazil | Social distancing and quarantine measures | IPAQ Long-Form | Depression | Depressed participants had significantly higher % engaging in >4 h day−1 TV viewing (39.6% vs. 37.4%) |
| Reyes-Olavarria et al. [83] | 700 participants No overall demographics available | Chile | Social distancing | Recall questions to assess sedentary time | - | 54.4% of participants reported spending ≥6 h day−1 sedentary |
| Asiamah et al. [84] | 621 participants No overall demographics reported | Ghana | Social distancing | Newly developed questionnaire which they piloted and validated | Mental health | 19.3% of participants ↑ sedentary time by ≥6 h day−1 Sedentary time negatively correlated with mental health |
| Werneck et al. [85] | 38,353 participants No overall demographics reported | Brazil | Social distancing and quarantine measures | New questionnaire–but good detail of measures throughout | Mental Health (Loneliness, Sadness and Anxiety) | 25% spend more than 8 h day sedentary. ↑ in the clustering of SB and physical inactivity ↑ in SB was associated with all mental health measures |
| Country (n of Papers) | Participants (n) and Age (Years) | Sedentary Time (Mins⋅Day−1) |
|---|---|---|
| Canada (n = 4) | 3295 participants 11.2 ± 2.5 years | 170.0 ± 96.0 |
| China (n = 2) | 4898 participants 16.3 ± 1.3 years | 363.6 ± 148.4 |
| Germany (n = 1) | 1174 participants No overall demographics available | 194.5 ± 141.3 |
| Italy (n = 2) | 112 participants 12.7 ± 2.0 years | 320.0 ± 144.0 |
| Spain (n = 2) | 1151 participants 10.9 ± 3.3 years | 330.0 ± 141.0 |
| United States (n = 1) | 211 participants 8.7 ± 2.6 years | 480.0 ± 123.0 |
| Country (n = Number of Papers) | Participants (n) and Age (Years) | Sedentary Time (Mins⋅Day−1) |
|---|---|---|
| Brazil (n = 3) | 45,233 participants 56.9 ± 3.9 years | 529.5 ± 20.4 |
| Canada (n = 1) | 351 participants 39.0 ± 5.0 years | 546.0 ± 78.0 |
| China (n = 4) | 25,754 participants 25.1 ± 6.7 years | 377.5 ± 212.5 |
| Germany (n = 1) | 14 participants (elite kayakers) 22.9 ± 1.4 years | 729.0 ± 21.0 |
| Italy (n = 2) | 2900 participants 23.0 ± 2.0 years | 540.0 ± 300.0 |
| Spain (n = 6) | 20,738 participants 30.8 ± 4.3 years | 538.0 ± 258.1 |
| Turkey (n = 1) | 1120 participants 33.0 ± 11.0 years | 324.0 ± 156.0 |
| United Kingdom (n = 3) | 3358 participants 60.6 ± 8.0 years | 458.7 ± 118.0 |
| United States (n = 3) | 5031 participants 46.7 ± 17.8 years | 484.0 ± 214.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. https://doi.org/10.3390/ijerph182111286
Runacres A, Mackintosh KA, Knight RL, Sheeran L, Thatcher R, Shelley J, McNarry MA. Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(21):11286. https://doi.org/10.3390/ijerph182111286
Chicago/Turabian StyleRunacres, Adam, Kelly A. Mackintosh, Rachel L. Knight, Liba Sheeran, Rhys Thatcher, James Shelley, and Melitta A. McNarry. 2021. "Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 21: 11286. https://doi.org/10.3390/ijerph182111286
APA StyleRunacres, A., Mackintosh, K. A., Knight, R. L., Sheeran, L., Thatcher, R., Shelley, J., & McNarry, M. A. (2021). Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(21), 11286. https://doi.org/10.3390/ijerph182111286